A 20-Year Post-traumatic Presentation of a Horizontal Root Fracture Accompanied by Bone Resorption and Sinus Tract: A Case Report
Pedram Hosseinzadehfard, Paulina Bernote, Greta Lodiene

TL;DR
A 56-year-old man had a 20-year-old tooth fracture treated successfully with a combination of endodontic and surgical methods to preserve the tooth.
Contribution
The paper presents a rare long-term case of a horizontal root fracture managed conservatively with combined endodontic and surgical techniques.
Findings
Selective endodontic treatment of the coronal fragment and surgical removal of the apical fragment resolved the persistent sinus tract.
The patient showed uneventful healing and stability of the treated tooth over 12 months.
Late-onset pulp necrosis can occur decades after trauma in horizontal root fractures.
Abstract
Horizontal root fractures present unique diagnostic and treatment challenges, particularly in cases with delayed presentation. This report describes the management of a 20‑year‑old untreated horizontal root fracture of the maxillary left central incisor, complicated by the presence of a persistent sinus tract. A 56‑year‑old male patient was referred due to mild anterior maxillary pain accompanied by purulent discharge. Clinical examination revealed Grade II mobility and tenderness upon percussion of tooth 21. Fistulogram traced the sinus tract to a displaced apical fragment of tooth 21. Endodontic treatment was conducted on the coronal fragment under magnification, including canal shaping, calcium hydroxide dressing, and final obturation with Biodentine (Septodont, Saint-Maur-des-Fosses, France). The persistence of the sinus tract during follow‑up indicated necrosis of the apical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
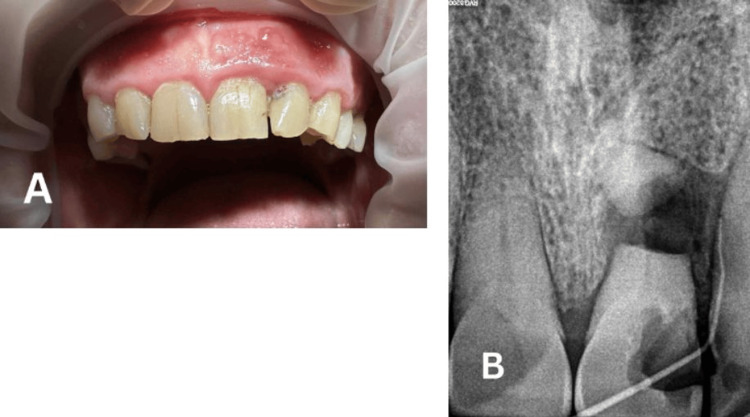 Figure 1
Figure 1 Figure 2
Figure 2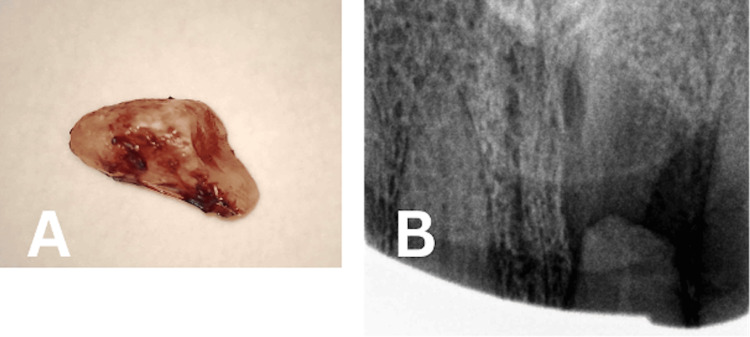 Figure 3
Figure 3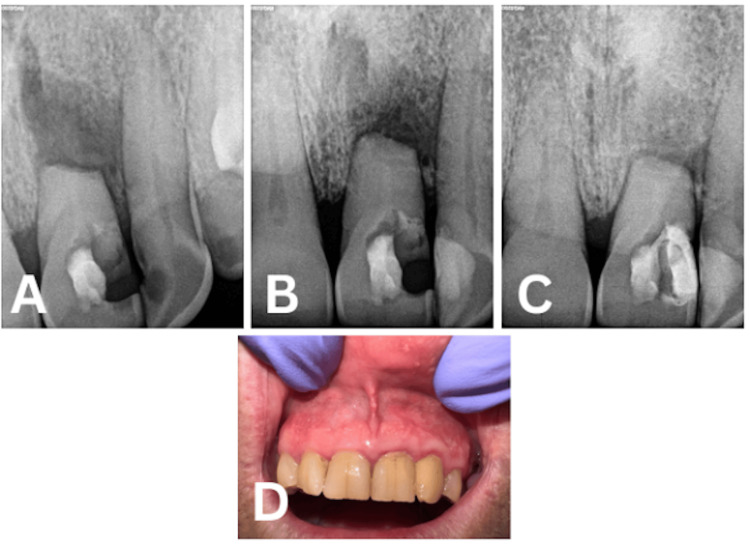 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Trauma and Treatments · Endodontics and Root Canal Treatments · Facial Trauma and Fracture Management
Introduction
Healing following a root fracture initiates locally, encompassing the pulp and periodontal tissues. In the absence of infection, a fracture may undergo healing through the formation of hard tissue or via the interposition of connective tissue between the fractured fragments [1].
In most cases, the pulp survives the trauma, remaining healthy and preserving normal functionality [2]. Pulp necrosis is relatively uncommon in the apical fragment; however, it occurs with greater prevalence in the coronal fragment. Endodontic treatment of the coronal fragment is indicated when the fracture line fails to demonstrate signs of healing [3]. Nevertheless, delayed pulp necrosis and infection may manifest many years subsequent to the initial injury. This phenomenon suggests that the pulp remained functional until a subsequent event, such as periodontal disease, dentin-involving infraction, or additional dental trauma - facilitated the ingress of bacteria into the root canal system [4].
When necrosis affects pulp tissue from both coronal and apical fragments, treatment becomes significantly more complex and presents additional clinical challenges. Endodontic intervention across the fracture line may compromise the integrity of the surrounding periodontal tissues. Alternatively, surgical removal of the apical fragment may be considered, contingent upon the coronal fragment maintaining adequate support and periodontal attachment [5].
Several factors can influence the long-term prognosis of a tooth subjected to a transverse root fracture, including the location of the fracture line, patient age, distance between the fractured segments, exposure of the fracture site to the oral cavity, and any pre-existing conservative, endodontic, or periodontal conditions [6]. Delayed treatment may result in significant long-term consequences. Teeth that experience trauma and receive late or no treatment are more susceptible to developing pulp canal obliteration, pulp necrosis, root resorption, and loss of marginal bone support [7].
This case report details the management of a horizontal root fracture associated with a sinus tract in a 56‑year‑old patient, presenting 20 years after the original traumatic incident.
Case presentation
The present case report followed the guidelines of Preferred Reporting Items for Case Reports in Endodontics 2020 (PRICE) [8]. Written informed consent was obtained from the patient for reporting this case. A 56-year-old male patient was referred to the Department of Dental and Oral Pathology of the Lithuanian University of Health Sciences, Kaunas, Lithuania, complaining of mild pain in the anterior maxilla. The patient’s medical history revealed facial trauma approximately 20 years prior, which resulted in a horizontal root fracture of tooth 21. No treatment was initiated at that time, and due to the absence of symptoms in subsequent years, the patient did not seek further follow-up.
Initial clinical examination revealed Grade II mobility according to the Miller classification, in addition to tenderness to percussion and a persistent sinus tract exhibiting purulent exudate (Figure 1A). The initial radiographic examination (fistulogram) demonstrated a horizontal root fracture with segment displacement, and the sinus tract was traced using gutta-percha #20 (Figure 1B).
(A) Initial Clinical Picture and (B) Initial Radiograph (Fistulogram)
During the initial visit, the tooth was isolated using a rubber dam system, and endodontic treatment was initiated. The endodontic access cavity was prepared under a surgical microscope (Leica Microsystem GmbH, Wetzlar, Germany) with a high-speed diamond bur under water coolant. A K-file size #10 was used to explore the canal, with the coronal portion of the working length determined to be 20 mm from the incisal edge to the fracture. The coronal segment of the root canal was shaped using hand instruments in a crown-down technique up to K-file #60. Subsequently, a calcium hydroxide medication (Ultracal, Ultradent Products Inc., South Jordan, UT, USA) was applied to the coronal fragment, and a follow-up appointment was scheduled two weeks later (Figure 2A).
(A) Coronal Part Filled With (CaOH)2 and (B) Coronal Canal Obturated With Biodentine
During the second dental appointment, a persistent sinus tract was observed, which confirmed the diagnosis of pulp necrosis of the apical fragment. The tooth was isolated using a rubber dam, and the access cavity was re-entered. The calcium hydroxide dressing was meticulously removed, with irrigation of the canal performed following each instrument change. Subsequently, the root canal was irrigated with 5 mL of 0.5% sodium hypochlorite (NaOCl), and a final rinse was carried out using sterile water. Following this, the coronal fragment was thoroughly irrigated with 5 mL of 17% ethylenediaminetetraacetic acid (EDTA) solution, irrigated with sterile water, dried, and then obturated with Biodentine (Septodont, Saint-Maur-des-Fosses, France) (Figure 2B). The endodontic access cavity was sealed with glass ionomer cement (Riva, Victoria, Australia).
At the third appointment, the patient was admitted for the surgical extraction of the apical fragment. Local anesthesia, comprising 2% lidocaine with 1:100,000 epinephrine (Xylestesin-A 2%, 3M ESPE, Seefeld, Germany), was administered via a nasopalatine nerve block with concomitant (labial) buccal infiltration at the mucolabial fold. Additionally, one cartridge was administered as a supplemental buccal infiltration.
A full mucoperiosteal flap utilizing a papilla-based incision technique was selected to preserve the interdental papilla, maintain optimal esthetics in the anterior region, and minimize the risk of postoperative recession compared to conventional flap designs. Gingiva and mucosa were incised using a 15C blade. A partial-thickness flap was elevated at the sulcus and base of the papilla, followed by the elevation of a full mucoperiosteal flap extending to the mucosa. A flap with one vertical incision was created, extending from the distal surface of tooth 11 to the distal surface of tooth 22. Granulation tissue was subsequently excised, and the apical fragment was extracted (Figure 3A).
(A) Removed Apical Fragment and (B) Postoperative Radiograph After Apical Fragment Removal
Subsequently, the surgical site was meticulously irrigated with saline, and the flap was fixated and sutured using a 5-0 suture. The entire endodontic surgical procedure was performed under a dental operating microscope (Leica Microsystem GmbH, Wetzlar, Germany). A postoperative two-dimensional radiograph was obtained (Figure 3B). Postoperative instructions concerning oral hygiene practices for the surgical site and dietary intake were provided. Non-steroidal anti-inflammatory drugs (NSAIDs) were recommended for postoperative pain management if required. Follow-up appointments were scheduled for suture removal at two weeks as well as at three months, six months, and one year postoperatively (Figure 4). At the two-week visit, complete resolution of the sinus tract was observed. Mobility of the coronal segment progressively decreased at the three- and six-month evaluations. Radiographic assessment at six months and one year demonstrated evidence of bone healing, indicating a favorable clinical and radiographic outcome.
Follow-Ups (A) After Three Months, (B) After Six Months, (C) After One Year, and (D) Clinical Picture After One Year
Discussion
Although pulp necrosis may occur following horizontal root fractures, immediate endodontic intervention is generally not recommended. Instead, periodic clinical and radiographic monitoring is advised in the absence of clinical or pathological signs. Frequent follow-up visits are necessary to assess the need for endodontic treatment [9]. In the present case, the existence of a persistent sinus tract indicated the presence of infection and necrosis, thereby necessitating endodontic treatment of the coronal fragment 20 years post-trauma.
In cases of pulp necrosis associated with horizontal root fractures, it is frequently noted that the apical fragment maintains vitality; consequently, endodontic therapy is typically limited to the coronal segment [10]. However, case reports over the last years have noted that even apical third fractures can demonstrate delayed pathological changes when long intervals occur between trauma and treatment, although these reports are relatively uncommon compared with middle third fractures [11]. In the current case study, despite the execution of adequate chemomechanical preparation, the application of intracanal medication, and the obturation of the coronal portion, the persistence of a sinus tract suggested the possible existence of necrosis or infection within the apical fragment. Therefore, a surgical intervention for the removal of the apical segment was deemed necessary. The extraction of the apical fragment was conducted under magnification to facilitate thorough debridement while preserving the surrounding bone and soft tissues. Recent literature supports this approach, demonstrating that apical fragment removal can promote healing when chronic infection persists, while maintaining periodontal support and function of the coronal fragment [12].
Although conservative management and retention of both fragments are generally preferred, the extraction of the apical fragment may be warranted in instances of persistent pathology, particularly when the coronal segment remains stable and functional [13]. In the current case, this approach facilitated the resolution of the sinus tract while preserving the coronal portion of the tooth, thereby illustrating that the selective removal of the necrotic apical fragment can serve as an effective and conservative alternative to complete extraction in chronic cases of root-fractured teeth exhibiting persistent periapical pathology. Furthermore, the long-standing periapical lesion in this case may suggest that the inflammatory process has extended to the apical fragment, potentially leading to its loss of vitality [14].
In similar cases detected shortly after trauma, prompt diagnosis, appropriate stabilization, and close monitoring of pulp vitality are essential to guide timely intervention and avoid progression of pathology. Early, targeted management can prevent the need for complete extraction and help preserve the remaining periodontal support, thereby maintaining both function and esthetics.
Conclusions
Late pulp necrosis can manifest decades following a horizontal root fracture, underscoring the importance of long-term follow-up for traumatized teeth. Targeted removal of the infection source, in conjunction with endodontic treatment of the coronal segment, presents a conservative and functional alternative to complete extraction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical management and subsequent healing of teeth with horizontal root fractures Dent Traumatol Versiani MA de Sousa CJ Cruz-Filho AM Perez DE Sousa-Neto MD 136139242008 https://doi.org/10.1111/j.1600-9657.2006.00507.x 1817368610.1111/j.1600-9657.2006.00507.x · doi ↗ · pubmed ↗
- 2Healing after horizontal root fracture of maxillary central incisor: a case report with 24-month follow-up Cureus Mane NA Shetty P Borkar AC Mujumdar SV Mujawar A 0152023 https://doi.org/10.7759/cureus.4337310.7759/cureus.43373 PMC 1049487237700969 · doi ↗ · pubmed ↗
- 3Apexification and repair of root fracture with mineral trioxide aggregate - a case report with 5-year follow-up J Pharm Bioallied Sci Annamalai S Hariharavel VP Ramar K Samuel V 05132021 https://doi.org/10.4103/jpbs.JPBS_789_2010.4103/jpbs.JPBS_789_20PMC 837585234447222 · doi ↗ · pubmed ↗
- 4Diagnosis and management of transverse root fractures Dent Traumatol Abbott PV 333347352019 https://doi.org/10.1111/edt.124823111236710.1111/edt.12482 · doi ↗ · pubmed ↗
- 5Long-term outcome of horizontal root fractures in permanent teeth: a retrospective cohort study J Endod Sheikhnezami M Shahmohammadi R Jafarzadeh H Azarpazhooh A 579589502024 https://doi.org/10.1016/j.joen.2024.02.0023835490610.1016/j.joen.2024.02.002 · doi ↗ · pubmed ↗
- 6Management of horizontal root fracture: a four-year follow-up case report Int J Oral Health Tagliatesta L Pappalardo F Porcheddu L Rovelli G Abdelazim Ibrahim RSI 1422022 https://skeenapublishers.com/journal/ijoh/IJOH-02-00016.pdf
- 7Delayed management of concurrent coronal extrusions and root fractures in two traumatized maxillary immature permanent central incisors: a case study J Clin Med Vo TT Do TN 3605142025 https://doi.org/10.3390/jcm 141036054042959910.3390/jcm 14103605 PMC 12112395 · doi ↗ · pubmed ↗
- 8PRICE 2020 guidelines for reporting case reports in endodontics: a consensus-based development Int Endod J Nagendrababu V Chong BS Mc Cabe P 619626532020 https://doi.org/10.1111/iej.132853209034210.1111/iej.13285 · doi ↗ · pubmed ↗