Contextual variability in under-diagnosed cardiometabolic disease and cognitive vulnerability among populations at high risk for Alzheimer’s disease and related dementias
Nwanyieze Jiakponnah, Joseph Curran, Tamlyn Watermeyer, Jasmit Shah, Litha Musili, Stanley Onyango, Benard Aliwa, Andy Mackelfresh, Omonigho Michael Bubu, Chiadi Onyike, Ozioma Okonkwo, Zul Merali, Rufus Akinyemi, Timothy Hughes, Mansoor Saleh, Melissa Petersen, Karen Blackmon

TL;DR
This study explores how underdiagnosed heart and metabolic conditions may contribute to dementia risk in African and diaspora populations.
Contribution
The study identifies context-specific diagnostic gaps in cardiometabolic risk factors among high-risk populations for dementia.
Findings
Underdiagnosis of hypertension and abnormal glycaemia was common in African cohorts.
Elevated glucose was linked to cognitive impairment in Kenya and North Texas.
Severe hypertension and diabetes were associated with Alzheimer’s biomarkers in North Texas.
Abstract
Underdiagnosis of cardiometabolic risk factors (CMRFs) may represent an unrecognised biological pathway contributing to dementia risk; yet remains poorly characterised in African and African diaspora populations. We quantified the prevalence and determinants of underdiagnosed hypertension and abnormal glycaemia across four cohorts comprising up to 7,000 adults aged ≥ 40 years from Nigeria, Kenya, and The United States: Indianapolis, and North Texas. Underdiagnosis was defined as absence of self-reported diagnosis despite elevated systolic blood pressure (≥ 130 mmHg) or fasting blood glucose (≥ 100 mg/dL). Cohort-stratified analyses examined demographic, socioeconomic, cognitive, Alzheimer’s genetic, and blood-based biomarker correlates. Underdiagnosis was pervasive in African cohorts. Elevated fasting glucose was associated with cognitive impairment in Kenya and North Texas, while…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
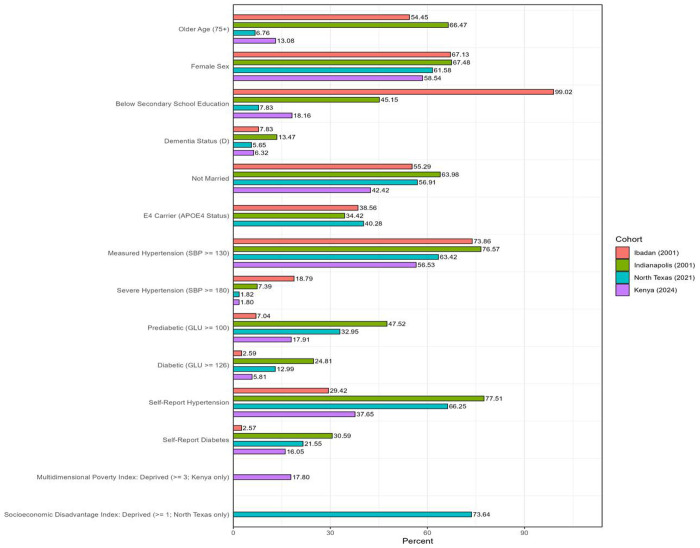 Figure 1
Figure 1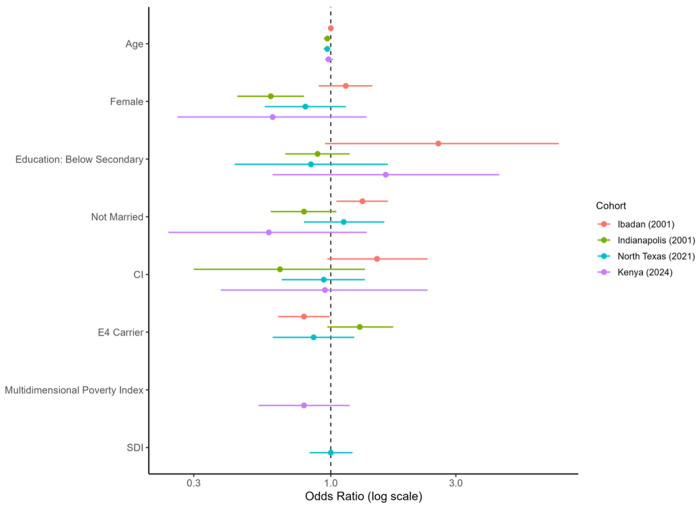 Figure 2
Figure 2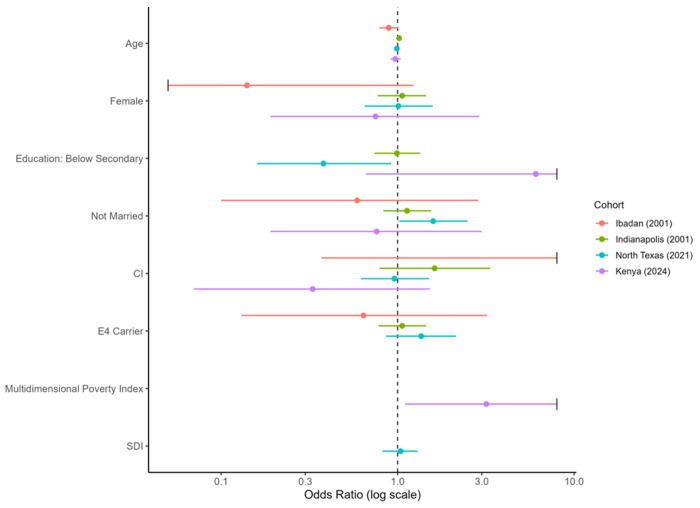 Figure 3
Figure 3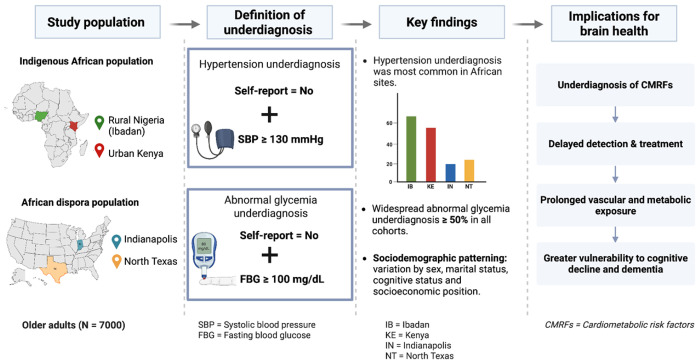 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDementia and Cognitive Impairment Research · Alzheimer's disease research and treatments · Neurological Disease Mechanisms and Treatments
INTRODUCTION
Dementia is a growing global health challenge, with prevalence projected to rise significantly among individuals of African descent^1,2^. This trajectory parallels the increasing burden of cardiometabolic risk factors (CMRFs), including hypertension, diabetes, and hyperlipidemia, which contribute to dementia through vascular and metabolic pathways that impair cerebrovascular integrity and accelerate neurodegeneration^3–5^. The 2024 Lancet Commission on dementia identified CMRFs as central components of the 14 modifiable risk factors that together account for approximately 45% of global dementia cases, indicating the substantial contribution of cardiometabolic pathways to dementia risk worldwide^6^. These cardiometabolic contributors are also increasingly recognized as dominant drivers of the expanding dementia burden in many parts of Africa^1^.
By 2030, in Sub-Saharan Africa, CMRFs including hypertension, type 2 diabetes mellitus, obesity, and hyperlipidemia are projected to become leading causes of morbidity and mortality, surpassing infectious diseases as the primary causes of death in the region^7,8^. Similarly, among diasporic African populations, such as African Americans, CMRFs are more prevalent than in other racial groups^4^, emphasizing the relevance of cardiometabolic health to dementia risk across both indigenous and diaspora African populations. However, the true scale of this risk may be significantly underestimated due to critical gaps in subjective awareness and clinical diagnosis. Indeed, current evidence indicates that an estimated 73% of adults with hypertension and 62.5% of those with diabetes in Sub-Saharan Africa remain undiagnosed^9,10^. This suggests that the substantial yet often overlooked burden of undiagnosed cardiometabolic disease in the region could be a potential hidden driver of the emerging dementia crisis. In the United States, African American adults with hypertension and diabetes are also more likely to be unaware of their condition compared to other racial groups, reflecting persistent disparities in screening and diagnosis^11^. Collectively, these findings point to a widespread pattern of underdiagnosis across both indigenous and diaspora populations. This trend is driven largely by inequities in healthcare access, diagnostic practices, and wider social determinants of health^4,5,12^.
Despite this growing evidence base, little is known about how underdiagnosis of CMRFs varies across demographic and contextual settings. Factors such as age, sex, educational attainment, socioeconomic status, and geography influence awareness of disease symptoms, healthcare-seeking behavior, and adherence to prevention and treatment^9,13^. Cultural, structural and health-system barriers including limited screening resources, fragmented healthcare infrastructure, and competing public health priorities often lead to delayed or missed diagnoses, particularly among older adults^12^. It also remains unclear whether the prevalence of undiagnosed CMRFs differs by cognitive status, such that individuals with cognitive impairment or dementia may experience distinct patterns of underdiagnosis compared with cognitively unimpaired individuals. This under-recognition obscures the true burden of cardiometabolic disease, reduces opportunities for timely prevention, and increases vulnerability to cognitive decline in later life.
Using data from four cohorts enriched with African and African diaspora participants, we analyze differences between self-reported and objectively ascertained measures of dementia-related cardiometabolic factors: hypertension and diabetes, to present the first cross-continental investigation of diagnostic gaps across sociodemographic, cognitive, and geographic factors towards identifying subgroups prone to underdiagnosis. The findings will help guide targeted public health efforts to improve cardiometabolic risk detection and reduce brain health disparities.
METHODS
Study Design and Cohorts
This cross-sectional analysis included four cohorts of older adults (N = 7,000) to examine underdiagnosis of cardiometabolic risk factors (CMRFs) across Indigenous African and African diaspora populations. Participants were drawn from community-based studies conducted in Nigeria, the United States, and Kenya.
The Ibadan sample was drawn from the Indianapolis–Ibadan Dementia Project (IIDP) and comprised Yoruba-speaking older adults residing in a predominantly rural community in Ibadan, Nigeria. Initial recruitment began in 1992 and was followed by a second wave of recruitment in 2001 from the same community, including survivors from the first wave. The Indianapolis sample was also drawn from the IIDP and comprised African American older adults residing in an urban community in Indianapolis, Indiana. Recruitment and assessment procedures in Indianapolis paralleled those used in Ibadan, with cohort-specific adaptations for the U.S. setting. A total of 5,336 IIDP participants across the two sites were included in the present study. The IIDP is conducted by investigators at Indiana University, USA and the University of Ibadan, Nigeria^14–16^.
The North Texas cohort comprised African American adults aged 50 years and older enrolled in the Health and Aging Brain Study–Health Disparities (HABS-HD), a community-based observational study of the long-term factors driving health disparities and progression from mild cognitive impairment to dementia, conducted in the Dallas-Fort Worth metropolitan area in Texas, United States. Enrollment of African American participants began in 2020, and a total of 1,213 participants were included in the present study. HABS-HD is conducted by investigators at the University of North Texas Health Science Center^17^.
The Kenyan sample was drawn from two community-based studies: Brain Resilience Kenya (BRK) and AD-DETECT Kenya, which recruited participants residing in Nairobi and surrounding urban areas. BRK enrolled adults aged 35 years and older and focuses on the physical, social, and psychological determinants of resilient aging^18,19^. AD-DETECT recruited older adults across the cognitive spectrum and focuses on developing and validating diagnostic biomarkers for dementia research in Kenya^20^. Both studies are conducted by investigators at the Brain and Mind Institute at Aga Khan University, Kenya, and share common assessment and data collection protocols. A total of 443 participants were included from the two Kenyan studies.
Ethics Approval, Consent and Data Use.
All studies obtained informed consent from participants and adhered to local ethical guidelines. Ethical approval for the AD-DETECT and BRK studies were obtained from the Aga Khan University Institutional Scientific and Ethics Review Committee (AD-DETECT: 2023/ISERC-135; BRK: 2023/ISERC-125) and the National Commission for Science, Technology, and Innovation (AD-DETECT: NACOSTI/P/24/33491; BRK License #: NACOSTI/P/25/418163). The HABS-HD study is conducted at The University of North Texas Health Science Center, Fort Worth, USA, under the approval of the North Texas Regional Institutional Review Board (NTR-IRB) approved protocol #2012-083. The Ibadan/Indianapolis Dementia Project was approved by the Ethics Committee of the University of Ibadan/University College Hospital, Ibadan, Nigeria as well as by the Indiana University-Purdue University of Indianapolis Institutional Review Board.
A data use agreement was established between each study host institution and the Wake Forest University Department of Epidemiology to permit access to de-identified and anonymised data analyzed in this study. Detailed descriptions of study design, clinical assessments, biomarker collection, and cardiometabolic measurements for each cohort have been published previously and are cited here for completeness^14–20^. Brief summaries of the measures relevant to the present analyses are provided below.
Harmonization of Study Measures
Objective CMRF Measurements
Objective blood pressure measurements were obtained using appropriately sized cuffs in accordance with each study’s standardized protocol, with participants seated or supine as specified by the cohort. Systolic (SBP) and diastolic blood pressure (DBP) were recorded and averaged when multiple readings were available. For our primary analyses, hypertension was defined using SBP ≥130 mmHg or DBP ≥90 mmHg, in accordance with American Heart Association criteria for stage 1 hypertension^21^. In secondary analyses, a more stringent definition of clinically overt hypertension was applied using SBP ≥180 mmHg and DBP ≥90 mmHg to examine associations at more severe thresholds.
Similarly, blood glucose measurements across individual study cohorts were obtained following an overnight fast and have been described in each study’s protocol. For our primary analyses, abnormal glycaemia was defined as fasting blood glucose (FBG) ≥100 mg/dL, encompassing prediabetes (100–125 mg/dL) and diabetes (≥126 mg/dL).
Self-Reported CMRFs Diagnosis
In each cohort, participants were asked whether a doctor or health professional had ever told them they had hypertension or diabetes. Responses were recorded as binary indicators for each condition (yes or no). Participants reporting a prior diagnosis or current use of medication for either hypertension and/or diabetes were classified as diagnosed and considered aware of that condition. Those reporting no prior diagnosis for either condition and not receiving disease-relevant medications were classified as undiagnosed.
Operationalization of CMRFs Underdiagnosis
The primary outcomes were underdiagnosed hypertension and underdiagnosed hyperglycemia, defined as unrecognized cardiometabolic risk. Underdiagnosed hypertension was defined as objectively elevated blood pressure (i.e., SBP ≥130 mmHg) in the absence of a self-reported hypertension diagnosis. Underdiagnosed abnormal glycaemia was defined as fasting blood glucose (FBG) ≥100 mg/dL without a self-reported diabetes diagnosis.
Participants with objective SBP or FBG values below the specified risk thresholds, or those reporting a prior diagnosis, were not classified as underdiagnosed. Individuals receiving treatment for hypertension or diabetes were considered diagnosed, even if their current measurements were within the normal range, ensuring that underdiagnosis reflected lack of awareness of the diagnosis rather than treatment effects.
Cognitive Status
Cognitive diagnoses in each cohort were assigned using established diagnostic criteria and cohort-specific adjudication procedures^14–20^. In the Indianapolis-Ibadan Dementia Project, dementia diagnoses required concordance across diagnostic frameworks, with final classification determined through clinical review by experienced clinicians familiar with the local cultural context.
In HABS-HD, cognitive diagnosis was determined through a structured algorithm followed by expert review, with cases meeting criteria for cognitive impairment or dementia and a subset of cognitively unimpaired participants undergoing detailed chart review and consensus adjudication. Diagnoses incorporated neuropsychological performance, clinical information, and functional status, and were assigned based on established criteria for dementia.
In the Kenyan studies, cognitive status was assigned using neuropsychological testing and clinical evaluation according to locally implemented protocols aligned with international diagnostic standards.
For the present analyses, cohort-specific diagnoses were first mapped into three harmonized categories: cognitively normal (N), cognitively impaired but not demented (CI), and dementia (D). To increase sample size and statistical power for selected analyses, we created a second cognitive variable by collapsing CI and D into a single category (cognitive impairment, CI) and contrasting it with no cognitive impairment (NCI).
Plasma Alzheimer’s disease-related biomarkers
In the North Texas cohort, plasma biomarkers were assayed using single molecule array (Simoa) technology on the Quanterix HD-X platform following the study’s standard laboratory procedures. Analytes included plasma amyloid beta (Aβ) 40 and 42, the Aβ42/Aβ40 ratio, glial fibrillary acidic protein (GFAP), neurofilament light chain (NfL), and phosphorylated tau (pTau181 and pTau217). All biomarker values were log_10-_transformed and then standardized to reduce skewness and place analytes on a common scale prior to downstream analyses.
Covariates
Demographic covariates were harmonized across cohorts. Age was treated as a continuous variable in years. Sex was coded as female or male. Education was dichotomized as below secondary school education (i.e., <12 years of schooling) versus secondary school or higher (≥13 years of schooling) to account for differences in educational systems and distributions across sites. Marital status was categorized as married versus not married.
APOE ε4 status was included as a genetic covariate and categorized as carrier (one or more ε4 alleles) versus non-carrier. APOE genotyping was conducted using cohort-specific protocols, and ε4 status was harmonized across studies for pooled analyses.
Socioeconomic position was operationalized using cohort-specific indicators. In the North Texas cohort, socioeconomic disadvantage was captured using a Social Disadvantage Index (SDI) derived from five indicators: low income (<$49,999), insurance vulnerability (Medicaid or uninsured), recent medical hardship (inability to afford or access healthcare in the past 12 months), housing vulnerability (renting or housing other than home ownership), and educational vulnerability (below high school education). Each indicator contributed one point, with SDI scores ranging from 0 to 5 and higher scores indicating greater disadvantage.
In the Kenya cohort, socioeconomic deprivation was characterized using a Multidimensional Poverty Index (MPI)–based measure derived from household and individual deprivation indicators, including lack of formal education, low income, and limited access to basic utilities or sanitation^22^. The MPI was treated as a continuous variable, with higher values indicating greater deprivation. In the Ibadan and Indianapolis cohorts, sufficient information to derive composite socioeconomic measures was not available, and education was therefore used as a proxy for socioeconomic position. Data from all cohorts were cleaned and harmonized prior to analysis. Variables were recoded to ensure comparability across studies, and cohort-specific cognitive diagnoses were mapped into shared analytic categories. Variables unavailable in specific cohorts (SDI, MPI, or APOE ε4 status) were excluded from those cohort-specific analyses.
Participants missing key measures were excluded from condition-specific analyses. No statistical imputation was performed. Blood pressure and self-reported diagnosis data were available for all included participants, while fasting glucose in the Ibadan cohort was collected in a predefined subset and analyses of glycaemia were restricted to that subset.
Statistical Analysis
All analyses were conducted using R (version 4.0 or later). Descriptive statistics were generated separately for each cohort, with continuous variables summarized using means and standard deviations and categorical variables using proportions.
Cross-sectional associations between cardiometabolic risk factors (hypertension and abnormal glycaemia) and cognitive status were examined using cohort-stratified logistic regression models. The primary cognitive outcome was any cognitive impairment, defined by collapsing cognitively impaired but not demented (CI) and dementia (D) into a single category and contrasting it with cognitively normal (N). Odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Supplementary analyses modelled dementia as dementia (D) versus cognitively normal (N), excluding CI.
In the North Texas cohort, we additionally examined associations between cardiometabolic disease severity and plasma AD-related biomarkers. Separate models were fitted for early-stage disease (SBP ≥130 mmHg; FBG ≥100 mg/dL) and clinically overt disease (SBP ≥180 mmHg; FBG ≥126 mg/dL). Each biomarker was modelled as a continuous outcome with adjustment for age, sex, APOE ε4 status, and cognitive status (CI vs NCI), to assess whether associations with cardiometabolic disease were present independent of clinical cognitive status. Analyses were restricted to participants with available biomarker and cardiometabolic data.
Primary analyses focused on the underdiagnosis of hypertension and abnormal glycaemia. Underdiagnosis prevalence was quantified within each cohort by comparing objectively measured cardiometabolic risk status with self-reported diagnosis. Differences in underdiagnosis rates across cohorts were assessed using chi-squared tests. To identify predictors of underdiagnosis, cohort-specific multivariable logistic regression models were fitted separately for hypertension and abnormal glycaemia. Underdiagnosis was modeled as a binary outcome, with age, sex, education, marital status, APOE ε4 status, and cognitive status included as covariates. Models were stratified by cohort to allow associations to vary across social and healthcare contexts. In the North Texas and Kenya models, SDI and MPI were included, respectively, as additional covariates.
All statistical tests were two-sided with a significance threshold of α = 0.05. Given the exploratory nature of some analyses, interpretation emphasized consistency and substantive relevance rather than isolated marginal findings.
RESULTS
Cohort Characteristics
Participant demographic, cardiometabolic, and cognitive characteristics by cohort are presented in Table 1 and Supplementary Table S1. Cohorts differed significantly in age, education, cardiometabolic profiles, and cognitive status distributions (all overall p < 0.001). Mean age was highest in the Indianapolis (78.2 ± 5.8 years) and Ibadan (76.9 ± 5.8 years) cohorts and lower in the North Texas and Kenya cohorts. Women comprised the majority of participants across all cohorts (58.5%–67.5%). Educational attainment varied markedly, with the lowest levels observed in Ibadan, where over 95% of participants had less than secondary school education, compared with 2% in North Texas.
Cognitive status distributions also differed across cohorts, with dementia prevalence highest in Indianapolis (13.5%) and lowest in Kenya (6.3%). Mean SBP and FBG levels differed significantly across cohorts. Ibadan had the highest mean SBP (151.6 ± 31.4 mmHg), while mean FBG levels were highest in the U.S. cohorts (Indianapolis: 113.6 ± 51.4 mg/dL; North Texas: 102.3 ± 39.6 mg/dL). The Kenyan cohort showed intermediate cardiometabolic values.
Cardiometabolic Risk Factors and Cognitive Status
Cross-sectional associations between hypertension, abnormal glycemia, and cognitive status are shown in Table 2 and Table 3 and Supplementary Tables S2–S3 (for dementia models). SBP ≥130 mmHg was not significantly associated with cognitive impairment (p > 0.5; Table 2) or dementia (p > 0.5; Supplementary Table S2). In a sensitivity analysis, SBP ≥180 mmHg was likewise not significantly associated with increased odds of cognitive impairment or dementia diagnosis (p > 0.5).
FBG ≥100 mg/dL was associated with increased odds of cognitive impairment in the Kenya cohort (OR = 2.47, 95% CI 1.16–5.27, p < 0.05) and the North Texas cohort (OR = 1.44, 95% CI 1.11–1.88, p < 0.01; Table 3). In supplementary analysis, FBG ≥100 mg/dL was associated with increased odds of dementia only in the North Texas cohort (OR = 2.85, 95% CI 1.05–7.79, p < 0.05), which was also observed for FBG ≥126 mg/dL (OR = 1.85, 95% CI 1.13–2.32, p < 0.01).
Cardiometabolic Risk Factors and Alzheimer’s Disease-Related Plasma Biomarkers
Associations between CMRFs and AD plasma biomarkers were examined in the North Texas cohort, where biomarker data were available. Supplementary Table S4 shows the distribution of plasma biomarkers and association models are presented in Supplementary Table S5. Severe hypertension (SBP ≥180 mmHg) was associated with higher plasma pTau217 (β = 0.63, SE = 0.27, p = 0.02), pTau181 (β = 0.60, SE = 0.30, p = 0.04), and NfL (β = 0.62, SE = 0.27, p = 0.02). Diabetes defined by FBG ≥126 mg/dL was associated with higher NfL (β = 0.37, SE = 0.09, p < 0.001) and was inversely associated with the Aβ42/40 (β = −0.27, SE = 0.14, p = 0.06).
Hypertension Underdiagnosis Across Cohorts
The prevalence of hypertension underdiagnosis differed substantially across cohorts (Table 4; Figure 1). Among participants with objectively measured hypertension, underdiagnosis was highest in Ibadan (67%) and Kenya (53%), and lower in Indianapolis (21%) and North Texas (28%) (overall p < 0.001).
Cohort-specific predictors of hypertension underdiagnosis are shown in Supplementary Tables S6–S9, with summary effect estimates displayed in Figure 2. In Ibadan, being unmarried was associated with higher odds of underdiagnosis (OR = 1.32, 95% CI 1.05–1.65, p = 0.017). Cognitive impairment showed a borderline association (OR = 1.50, 95% CI 0.97–2.34, p = 0.071), while APOE ε4 carriage was associated with lower odds of underdiagnosis (OR = 0.79, 95% CI 0.63–0.99, p = 0.043).
In Indianapolis, female sex (OR = 0.59, 95% CI 0.44–0.79, p< 0.001) and age (OR = 0.97, 95% CI 0.94–1.00, p = 0.025) were associated with lower odds of underdiagnosis, whereas APOE ε4 carriage showed a trend towards higher odds (OR = 1.42, 95% CI 1.03–1.97, p = 0.04). No predictors reached statistical significance in the North Texas or Kenya cohorts.
Abnormal Glycemia Underdiagnosis Across Cohorts
Underdiagnosis of abnormal glycaemia (FBG ≥100 mg/dL) was common across all cohorts (Table 5), with the highest prevalence observed in Ibadan (93%) and Kenya (61%), and substantial underdiagnosis in Indianapolis (54%) and North Texas (56%) (overall p < 0.001). Similar patterns were observed using the stricter diabetes threshold (FBG ≥126 mg/dL).
Cohort-specific predictors of abnormal glycaemia underdiagnosis are shown in Supplementary Tables S10–S13, with summary effect estimates presented in Figure 3. In Ibadan, increasing age showed a suggestive association with lower odds of underdiagnosis (OR = 0.89, 95% CI 0.78–1.01, p= 0.07), while in Indianapolis age showed a trend toward higher odds of underdiagnosis (OR = 1.03, 95% CI 1.00–1.06, p = 0.09). In Kenya, higher Multidimensional Poverty Index scores were associated with increased odds of underdiagnosis (OR = 3.18, 95% CI 1.10–9.21, p = 0.03).
In North Texas, below secondary school education (OR = 0.38, 95% CI 0.16–0,92, p = 0.03) was associated with lower odds whereas, being unmarried (OR = 1.59, 95% CI 1.02–2.49, p = 0.04) were associated with higher odds of abnormal glycaemia underdiagnosis. In a sensitivity model including only cognitive status, APOE ε4 status, and a cognitive status × APOE ε4 interaction term, the interaction term was associated with increased odds of underdiagnosis (OR = 3.22, 95% CI 1.24–8.35, p = 0.02). Figure 4 summarizes the observed prevalence patterns and sociodemographic predictors of underdiagnosis of CMRFs across cohorts, together with a conceptual link to downstream brain health vulnerability.
In North Texas, having at least a high school education (OR = 2.63, 95% CI 1.09–6.36, p = 0.03) and not being married (OR = 1.59, 95% CI 1.02–2.49, p = 0.04) were associated with higher odds of abnormal glycaemia underdiagnosis. In a sensitivity model including only cognitive status, APOE ε4 status, and a cognitive status × APOE ε4 interaction term, the interaction term was associated with increased odds of underdiagnosis (OR = 3.22, 95% CI 1.24–8.35, p = 0.02). Figure 4 summarizes the observed prevalence patterns and sociodemographic correlates of underdiagnosis of CMRFs across cohorts, together with a conceptual link to downstream brain health vulnerability.
DISCUSSION
In this multi-cohort study of older adults from indigenous African and African diaspora populations, we identified substantial underdiagnosis of hypertension and abnormal glycaemia across all settings, with marked variation by cohort and sociodemographic context. Underdiagnosis was most pronounced in the African cohorts, particularly Ibadan and Kenya, but remained common in U.S. cohorts, indicating that gaps in cardiometabolic disease awareness persist even within health systems with greater clinical infrastructure. Our results suggest that underdiagnosis constitutes a critical and underappreciated barrier beyond what prevalence estimates alone capture for dementia risk reduction across diverse African populations.
Hypertension and diabetes are well-established modifiable risk factors for dementia, particularly when exposure is prolonged or inadequately treated^6,23–26^. Contemporary dementia prevention frameworks, including the 2024 Lancet Commission on dementia, place cardiometabolic health at the center of risk reduction strategies, estimating that a substantial proportion of dementia cases globally are attributable to such modifiable factors^6^. Midlife hypertension and diabetes are robust predictors of late-life cognitive decline and dementia^6,23–26^, and cumulative vascular burden accelerate neurodegeneration and cognitive decline^27^. Evidence further suggests that blood pressure control may reduce the risk of cognitive impairment ^27–30^, pointing to the importance of early detection. The present study adds an important dimension to this literature by demonstrating that, in many indigenous African and African diaspora populations, cardiometabolic risk frequently remains undetected. Underdiagnosis thus represents a major missed opportunity for prevention and limits the effectiveness of strategies targeting modifiable risk factors such as blood pressure and glycemic control. In the North Texas cohort, clinically overt cardiometabolic disease (SBP ≥ 180 mmHg and FBG ≥ 126 mg/dL) was associated with AD-related plasma biomarkers (Aβ42/40, pTau, and NfL), indicating that biological markers of brain vulnerability may already be present once disease is established. This suggests that variation in these biomarkers may, in part, reflect downstream effects of uncontrolled cardiometabolic disease rather than primary neurodegenerative processes alone, with important implications for how blood-based biomarkers are interpreted in population studies, particularly in settings where cardiometabolic disease is common and frequently underdiagnosed. This is especially relevant in African settings, where both cardiometabolic disease and dementia are frequently undetected because of diagnostic limitations and structural and health-system constraints, which may complicate the interpretation of biomarker signals in these populations ^31,32^.
Patterns of underdiagnosis varied systematically across cohorts, reflecting differences in healthcare access, screening practices, and social context. In Ibadan and Kenya, the majority of participants with objectively measured hypertension or abnormal glycemia were unaware of their condition. These findings are consistent with population-based studies documenting limited screening coverage, low cardiometabolic disease awareness, and constrained diagnostic capacity in many Sub-Saharan African settings ^9,33–35^. Structural factors, including multidimensional poverty, limited primary care infrastructure, and competing health priorities, likely contribute to delayed or absent diagnosis in these contexts^22,36^.
Crucially, the observed underdiagnosis was not confined to low-resource settings. In both Indianapolis and North Texas, substantial proportions of participants with abnormal glycemia were unaware of their condition, indicating persistent diagnostic gaps within U.S. health systems. This aligns with prior work showing that African American populations experience disparities in cardiometabolic screening, disease awareness, and continuity of care despite overall healthcare availability^2,4^. These results indicate that underdiagnosis is not solely a function of national income but may reflect complex socio-cultural and health-system barriers shared across the African diaspora population.
Sociodemographic factors further shaped patterns of underdiagnosis of CMRFs in cohort-specific ways. In Ibadan, being unmarried was associated with higher odds of hypertension underdiagnosis. In the U.S. cohorts, older age and female sex were associated with lower odds of hypertension underdiagnosis in Indianapolis, and older age was similarly associated with lower odds in North Texas. For abnormal glycaemia underdiagnosis, a different pattern emerged. In Ibadan, older age and female sex showed non-significant trends toward higher odds of underdiagnosis, whereas in Indianapolis there was a trend toward higher odds with increasing age. In North Texas, lower educational attainment was associated with reduced odds of abnormal glycaemia underdiagnosis, while being unmarried was associated with higher odds. The age-related associations observed for hypertension underdiagnosis in the U.S. cohorts may partly reflect cohort structure and differential engagement with health services across the life course. This is consistent with evidence that older adults tend to have greater health needs and are therefore more likely to utilize healthcare services, leading to increased awareness of their health conditions^37^. The trend toward higher odds of hypertension underdiagnosis among women in rural Ibadan may plausibly reflect gender roles in indigenous African settings that favor patriarchal social structures. This is consistent with prior evidence that older women in rural African settings face distinct barriers to preventive care, including reduced access to screening and lower diagnostic awareness^1^. These observed differences indicate that age-related, gendered, and marital patterns in the underdiagnosis of CMRFs vary across settings and may reflect differences in healthcare access, screening practices, and health-seeking behaviors, reinforcing the need for context-specific approaches to chronic disease detection rather than uniform assumptions about risk or access.
Cognitive status was associated with underdiagnosis in selected cohorts, suggesting that early cognitive changes may complicate disease awareness or engagement with healthcare systems. In Ibadan, cognitive impairment showed a borderline association with hypertension underdiagnosis, while in North Texas, cognitive status interacted with APOE ε4 carriage in relation to abnormal glycemia underdiagnosis. This is consistent with prior studies indicating that cognitive impairment may interfere with symptom recognition, self-report accuracy, and chronic disease management in older adults^38,39^, particularly in settings with limited caregiver or health system support ^12,32,36^. This has important implications for dementia prevention. If individuals with early cognitive impairment are less likely to have CMRFs recognized and treated, they may experience prolonged exposure to vascular and metabolic insults during a critical window for risk modification. This could increase dementia vulnerability by delaying interventions that are most effective earlier in the disease course.
We also examined whether APOE ε4 genetic susceptibility modified patterns of cardiometabolic underdiagnosis. Associations varied by cohort and outcome, with no consistent pattern observed. This heterogeneity suggests that underdiagnosis of cardiometabolic risk factors is shaped more strongly by social, cognitive, and healthcare contexts than by genetic risk alone. This interpretation is consistent with prior evidence showing that awareness, diagnosis, and management of cardiometabolic conditions are strongly structured by social determinants and health system factors rather than by biological susceptibility^40,41^. APOE plays a role in lipid metabolism and cardiometabolic physiology^42^; however, our findings caution against over-emphasizing genetic explanations for diagnostic disparities and instead highlight the central role of structural determinants in shaping cardiometabolic underdiagnosis, with important implications for dementia risk stratification. While APOE ε4 is a strong genetic risk factor for dementia, our results further indicate that genetic susceptibility does not reliably translate into greater CMRF surveillance or earlier detection in clinical or community settings. Consequently, individuals at elevated genetic risk may remain exposed to unmanaged vascular and metabolic risk, which could limit the effectiveness of precision prevention strategies that rely on genetic profiling alone.
From a policy perspective, our findings align with calls to strengthen cardiometabolic detection as a cornerstone of dementia prevention, particularly in African populations. Initiatives such as the AFRICA-FINGERS^43^, and FeMBER- AFRICA^44^ emphasize integrated approaches that combine early detection, community-based screening, and health system strengthening to address modifiable dementia risk factors across the life course.
Our results indicate that without addressing underdiagnosis, even well-established prevention frameworks may fail to reach populations at greatest risk. Improving screening coverage, diagnostic awareness, and follow-up care should therefore be considered essential components of dementia risk reduction strategies in both indigenous African and African diaspora contexts.
This study has several notable strengths. By combining data from three geographically and culturally distinct cohorts, it provides, to our knowledge, the first cross-continental analysis of cardiometabolic underdiagnosis, rather than prevalence, in relation to dementia risk across both indigenous African and African diaspora populations. Integration of objective cardiometabolic measures with self-reported diagnosis enables direct quantification of diagnostic gaps, revealing the extent of hidden morbidity often overlooked in surveillance studies. The sex-disaggregated and context-sensitive analyses further uncover distinct vulnerability profiles, highlighting the need for tailored prevention strategies. Although cross-sectional, the study establishes a foundation for longitudinal investigation within established cohorts to clarify how early detection of cardiometabolic disease may mitigate cognitive decline.
Limitations should be acknowledged. The cross-sectional design precludes causal inference, and differences in measurement protocols across cohorts may contribute to heterogeneity. Sample sizes in some of the cohorts had limited power for subgroup analyses. Nevertheless, the consistency of underdiagnosis across settings supports the robustness of the central findings. Future studies should extend these analyses longitudinally to determine whether underdiagnosed cardiometabolic risk predicts subsequent cognitive decline and incident dementia and whether improving detection alters dementia trajectories. Additionally, integration of neuroimaging, blood-based biomarkers, and digital cognitive assessments may help clarify mechanisms linking unrecognized cardiometabolic burden to neurodegeneration. Lastly, expanding cohort representation across African regions and diaspora contexts will further inform region-specific prevention strategies and embedding such work within emerging African brain health networks, including AFRICA-FINGERS^43^, FeMBER-AFRICA^44^, the African Dementia Consortium^45^, and the Global Brain Health Institute^46^, offers a pathway toward sustainable, equity-focused dementia prevention.
In conclusion, underdiagnosis of dementia-related CMRFs, specifically, hypertension and abnormal glycaemia is widespread across indigenous African and African diaspora populations and varies systematically by sociodemographic, geographic and healthcare contexts. These diagnostic gaps undermine dementia prevention strategies that depend on early identification and management of modifiable risk factors. Prioritizing the identification and management of cardiometabolic underdiagnosis through contextually tailored, gender-sensitive, and health system-oriented strategies is essential for promoting global brain health equity and mitigating the burden of dementia.
Supplementary Material
This is a list of supplementary files associated with this preprint. Click to download.
• UnderdiagnosisofCardiometabolicRiskFactorsinAfricansSupplementalDataforsubmission.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Akinyemi R. O. Dementia in Africa: Current evidence, knowledge gaps and future directions. Alzheimer’s Dement. J. Alzheimer’s Assoc. 18, 790–809 (2022).
- 2Chen C. & Zissimopoulos J. M. Racial and ethnic differences in trends in dementia prevalence and risk factors in the United States. Alzheimer’s Dement. Transl. Res. Clin. Interv. 4, 510–520 (2018).
- 3Alemayehu Z. G. Dementia in Sub-Saharan Africa: Risk factors, public perception, and management approaches. J. Med. Surg. Public Health 7, 100204 (2025).
- 4Chen S. Cardiometabolic Multimorbidity and Dementia Onset Among Middle-Aged and Older Adults: Differences by Race/Ethnicity. J. Gerontol. Ser. A 80, glaf 009 (2025).
- 5Patel V. & Edison P. Cardiometabolic risk factors and neurodegeneration: a review of the mechanisms underlying diabetes, obesity and hypertension in Alzheimer’s disease. J. Neurol. Neurosurg. Psychiatry 95, 581–589 (2024).38290839 10.1136/jnnp-2023-332661 PMC 11103343 · doi ↗ · pubmed ↗
- 6Livingston G. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. The Lancet 404, 572–628 (2024).
- 7Houle B. Cognitive function and cardiometabolic disease risk factors in rural South Africa: baseline evidence from the HAALSI study. BMC Public Health 19, 1579 (2019).31775713 10.1186/s 12889-019-7938-z PMC 6882146 · doi ↗ · pubmed ↗
- 8Noubiap J. J. Clustering of cardiometabolic risk factors in sub-Saharan Africans. Pan Afr. Med. J. 38, 112 (2021).33912282 10.11604/pamj.2021.38.112.28180 PMC 8051209 · doi ↗ · pubmed ↗