Utilizing the NIMHD Framework to Explore Barriers and Facilitators to Lung Cancer Screening Among Black Adults in NYC
Wynta Alexander, Mei Maeda, Jaime L. Gilliland, Jamie S. Ostroff, Lisa Carter-Bawa, Lina Jandorf, Victoria Frederico, Lesia M. Ruglass

TL;DR
This study explores why Black adults in NYC have low lung cancer screening rates and suggests ways to improve access and awareness.
Contribution
The study applies the NIMHD framework to identify multilevel barriers and facilitators to lung cancer screening in Black communities.
Findings
Four key themes—preparation, partnership, prioritization, and placement—were identified from interviews.
Community mistrust and lack of knowledge are major barriers to screening uptake.
Culturally tailored strategies like mobile units and community engagement are recommended.
Abstract
Lung cancer is the leading cause of cancer-related death in the United States, with Black individuals experiencing the highest incidence and mortality rates. Despite the benefits of early detection through low-dose computed tomography (LDCT), lung cancer screening rates remain disproportionately low among Black adults. This study explores barriers and facilitators to inform culturally tailored interventions that promote equitable screening uptake. Guided by the National Institute on Minority Health and Health Disparities (NIMHD) research framework, we conducted semi-structured interviews with screening-eligible Black adults in New York City (NYC). Participants were recruited through community canvassing and stakeholder partnerships. Transcripts were analyzed using thematic content analysis to identify key themes across individual, interpersonal, community, and societal levels.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
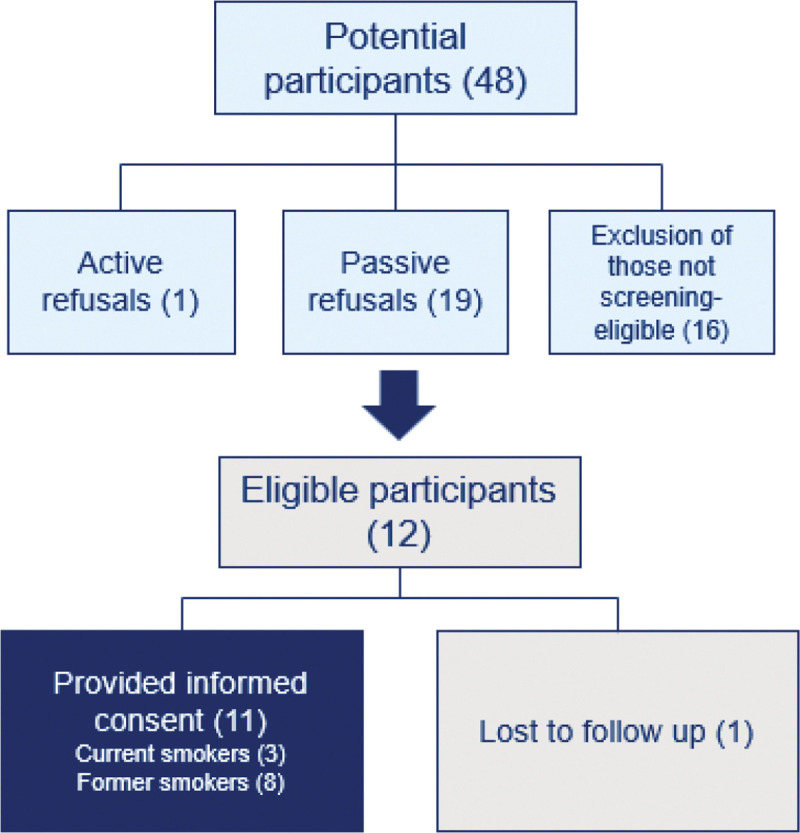 Figure 1
Figure 1- —National Cancer Institute
- —National Institute on Drug Abuse
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Diagnosis and Treatment · Global Cancer Incidence and Screening · Lung Cancer Treatments and Mutations
Introduction
In the United States, lung cancer is the leading cause of cancer death [1] and is the second most common cancer [2–3] in both men and women. Smoking cigarettes remains the primary risk factor [4] contributing to 80–90% of lung cancers [5–6]. Despite overall advances in prevention and early detection, persistent racial and ethnic disparities in lung cancer outcomes remain a pressing public health concern [7]. Specifically, Non-Hispanic (NH) Black or African American (hereafter referred to as Black) males have the highest rates of age-adjusted lung cancer incidence between 2004 and 2014 among all racial and ethnic groups [8]. Black individuals are also more likely to present at advanced lung cancer stage [9–10], further contributing to poor outcomes.
To detect lung tumors at earlier, more treatable stages, the U.S. Preventive Services Task Force (USPSTF) recommends low-dose computed tomography (LDCT) of the chest for high-risk individuals [11–12]. However, overall uptake remains alarmingly low, with only 16% of those at high risk receiving annual screening [13]. Among eligible Black individuals, screening rates are even lower, at only 1.7% [14–15]. Poulson et al. (2022) observed a 44% lower likelihood of undergoing screening among Black individuals compared to their White counterparts [16]. These disparities are rooted in multi-level barriers, including systemic racism, healthcare mistrust, limited access to care, and exclusion from clinical trials [17].
To enhance our understanding of the multi-level factors contributing to lung cancer screening disparities, this study applied the National Institute on Minority Health and Health Disparities (NIMHD) Research Framework [18] which emphasizes the role of structural factors, such as discrimination, socioeconomic inequality, and policy-level barriers in influencing health disparities among Black populations. The NIMHD framework offers a valuable lens through which the current study explores how individuals make sense of the complex factors surrounding lung cancer screening.
Methods
Study Design
This qualitative study explored multi-level influences from individual to societal across biological, behavioral, built environment, sociocultural, and healthcare system domains on lung cancer screening. We conducted semi-structured interviews with Black, screening-eligible adults to explore barriers and facilitators to lung cancer screening. The NIMHD Framework [18] guided our thematic analysis to situate participants’ experiences within the broader social and structural contexts shaping screening behavior. All study procedures were approved by the Institutional Review Boards at Memorial Sloan Kettering (protocol #X21–060) and the City University of New York (protocol #2022 − 0357).
Participants and Recruitment
The study included individuals who met eligibility criteria for lung cancer screening: aged 50–80, with a 20-pack year history or more of smoking who either currently smoke or have quit smoking within the past 15 years [19], and who self-identified as Black and resided in the NYC area. Participant characteristics can be found in Table 1. Members of the study team (WA, MM) conducted in-person community canvassing in the NYC metropolitan area for potential participants. Employing purposive and snowball sampling, eligible participants were asked to participate in an interview and to recommend others for participation. A recruitment flyer was posted on community center boards, handed out during in-person canvassing, and given to participants to share with their communities. The study team also collaborated with community stakeholders in the Harlem, NYC area. Individuals interested in the study reached out to the study team. Of 48 potential participants, 11 were consented to the study, as seen in Fig. 1.
Qualitative Data Collection & Analysis
A semi-structured interview guide was created to explore knowledge, barriers, and facilitators of lung cancer screening within participants’ communities. Based upon previous community-engaged work conducted by the Witness Project^®^ [20] to promote lung cancer screening, open-ended questions allowed participants to share knowledge and attitudes towards lung cancer screening (e.g. “Who is eligible for lung cancer screening?”), community-specific factors related to lung cancer screening uptake and implementation (e.g. “What factors are important to implementing lung cancer screening in the Black community?”), facilitators of lung cancer screening (e.g. “What things would help Black individuals who are eligible get screened?”), and barriers to lung cancer screening (e.g. “What things do you see stand in the way of eligible Black individuals getting screened?”)
Facilitated by two trained and supervised graduate-level research fellows (WA and MM), 11 semi-structured interviews were conducted via Zoom video conferencing platform (Zoom Video Communications, Inc, San Jose, CA) lasting approximately 45 minutes between October 2022 and June 2023 and were conducted according to established methodologic guidelines [21]. Thematic saturation was achieved by conducting enough interviews until no new themes emerged during analysis [22].
Each interview was audio recorded and transcribed verbatim. All transcripts were analyzed using deductive and inductive thematic content analysis [23–25]. The coding team was led by a qualitative methods specialist (QMS) (JG) and included the graduate-level research fellows. First, the coding team individually reviewed a subset of transcripts to identify domains of interest and create codes. Once agreed upon, these codes were consolidated and used to code subsequent transcripts. The team then independently coded each transcript in NVivo 14, highlighting significant statements within each domain. This iterative process involved the coding team meeting regularly with the larger research team to reach consensus regarding code definitions, application, and discrepancies in coding, as well as to discuss primary themes as they emerged. In the final phase, the research team organized the coded data based on the NIMHD framework and identified key themes observed across transcripts.
Results
Table 2 summarizes the qualitative findings organized by NIMHD levels of influence and illustrative quotations. Below, we describe thematic constructs identified including preparation, partnership, prioritization, and placement across levels of influence.
Preparation
When asked about their knowledge of lung cancer or lung cancer screening, participants expressed uncertainty regarding the screening process and availability in their communities, and shared concerns about the costs associated with screening. Questions were raised about insurance coverage and whether screenings are accessible for those without insurance. Participants also discussed a lack of knowledge regarding the causes of lung cancer (heritability, environmental causes, etc.) and how it is treated.
Participants highlighted a lack of education in their communities about lung cancer and screening, exacerbated by limited communication channels such as billboards, television, and the internet. Participants consistently underscored the significance of education and ensuring information regarding lung cancer risk and screening is readily available, accessible, and relevant. Emphasis was placed on the importance of targeted, local outreach efforts, frequent and widespread messaging, engagement of community members in educational initiatives, and innovative approaches to effectively communicate with individuals within the Black community who may be at higher risk for lung cancer. Various forms of outreach were proposed, such as canvassing, media advertisements, health fairs and mobile outreach, and offering incentives for engagement. Participants emphasized the significance of community sharing of information and suggested locations for outreach efforts including schools, churches, gyms, senior centers, and healthcare facilities, underscoring the importance of promoting awareness about lung cancer and screenings within the Black community.
Partnership
Participants conveyed perceptions of discrimination and mistrust toward healthcare professionals and researchers, especially from different racial or ethnic backgrounds. This mistrust extended to the medical system and the broader government, stemming from historical instances of systemic discrimination and exploitation. This lack of trust poses practical barriers, such as doubts about receiving adequate support after a cancer diagnosis. Concerns were expressed about a perceived lack of urgency, attention, or support from health care providers. Participants reported instances of dismissiveness or insufficient support when requesting lung cancer screening from their clinicians.
For some, stigma presents an obstacle to lung cancer screening. Intersectional stigmatizing factors such as gender, race, socioeconomic status, and smoking history were identified. Participants expressed how stigmatization of smoking may lead to avoidance of screening, especially among Black elders.
Participants highlighted the importance of social support in facilitating access to lung cancer screenings, recommending either a buddy system where individuals attend screenings with a trusted companion, or peer navigation to help people understand the testing process, navigate procedures, and interpret lab results. Participants recommended encouraging social support within families to support individuals who may feel fearful or apprehensive about undergoing screening.
Prioritization
Participants frequently associated “lung cancer” with death, evoking fears about mortality. This was often informed by family history of illness, such as witnessing family members facing cancer. The potential to receive a cancer diagnosis evoked fear and presented a barrier to pursuing screening, revealing uncertainty about how to manage the potential strain of a cancer diagnosis.
Community beliefs, norms, and perceptions of healthcare were cited as influencing engagement with screening. Participants described a complex relationship with smoking in the Black community, noting that observing others smoking in the community often influences individuals to begin smoking themselves, and that smoking frequently involves social gatherings among community members. Participants also observed that community members can be dismissive, disregarding how smoking affects air quality and its impact on others, and, particularly among young adults, a lack of concern about lung health overall.
Participants described a tendency towards delayed healthcare-seeking behavior, with individuals often seeking care only when symptoms reach a critical stage; a pattern greatly influenced by social determinants of health. Healthcare, especially preventive care, is often deprioritized due to more immediate concerns such as gun violence, economic instability, including challenges with rent and food affordability, and other health priorities.
Despite these fears, worries, and influential beliefs and community norms, participants generally agreed on the importance of lung cancer screening, emphasizing that it is equally important as other health awareness initiatives such as HIV/AIDS and Hepatitis C, and that all forms of cancer screening (i.e., breast, colorectal) hold equal significance. Participants emphasized the importance of increasing awareness about lung cancer and screenings within the Black community. Participants perceived higher risk of lung cancer and elevated tobacco-related illness among Black individuals compared to other racial and ethnic groups and raised concerns about exposure to pollutants stemming from poor air quality, environmental contaminants, and secondhand smoke. Participants reflected a collective belief in the importance of heightened personal health awareness, noting that education and knowledge are essential in empowering individuals to manage their health effectively and potentially save lives. Factors identified as influencing lung cancer screening included familial encouragement, family health history considerations, and observing illness effects and outcomes of inadequate prevention or care via the media or lived experience.
In addition to individual and community-level factors impacting prioritization of lung cancer screening, participants shared perspectives that lung cancer screening is viewed as a lower priority within their healthcare system. Perceptions of greater emphasis on smoking cessation over screening, and more attention given to screening for cancers like breast or colorectal, were commonly cited. Participants reported that healthcare providers rarely initiated discussions about screening during appointments, contributing to the perception that it is not prioritized. Integrating discussions about lung cancer screening into routine check-ups with primary care physicians and following consistent monitoring schedules were proposed as potential solutions. Participants likened this approach to existing practices for other cancer screenings, such as those for colorectal or breast cancer, with doctors initiating conversations and reminders for screening. Another suggestion was to adopt a similar screening approach as seen with other health concerns like COVID-19 and HIV, ensuring accessibility to lung cancer screening comparable to these tests, and increasing outreach and awareness within communities.
Placement
Participants highlighted that their community experience disparities in information about and access to local lung cancer screening services compared to more affluent neighborhoods. One participant noted that they never see literature or outreach on this topic, and that lung screening services are not advertised. Another shared a perception that there is likely more outreach for screening in upscale areas and noted a lack of care and concern for low-income communities. Participants stressed the importance of locating screening services within local communities for maximum accessibility and convenience, noting that many community members do not frequently travel outside their neighborhoods. .
Discussion
The study objective was to explore multi-level barriers to, and facilitators of, lung cancer screening among screening-eligible Black community members in NYC. Guided by the NIMHD Research Framework [18], we identified key constructs: preparation, partnership, prioritization, and placement that intersect across individual, interpersonal, community, and societal levels. These findings help contextualize structural inequities and inform strategies for promoting equitable lung cancer screening.
Preparation
Participants frequently described a lack of awareness about lung cancer screening guidelines, eligibility, and availability, findings that echo prior research demonstrating low screening-related health literacy among Black adults [26]. Such informational gaps likely reflect broader systemic failures in health education and outreach to minoritized communities. These findings underscore the critical role of community-level interventions in disseminating relevant information about lung cancer risk and screening. Culturally relevant education materials and communication approaches can help address the social determinants of health that shape health behaviors and improve engagement among screening-eligible Black individuals.
Participants recommended using diverse outreach channels, such as flyers, social media, and mobile services to effectively reach Black communities. Incentives were seen as helpful in reducing practical barriers like transportation. Suggested locations for outreach included schools, churches, gyms, and healthcare facilities, reflecting where community members naturally gather. Strategically placing educational materials in these spaces can improve accessibility [27], and messaging should be free of stigma to build trust and engagement.
Partnership
Trusting relationships with health care providers were central to participants’ decisions about lung cancer screening. Mistrust toward healthcare professionals and researchers, particularly from different racial or ethnic backgrounds, extended beyond individual providers to the broader medical system and government institutions, rooted in historical injustices and lived experiences of discrimination and neglect. For example, a study of 34 lung screening-eligible individuals, half of whom identified as Black, found that mistrust of providers contributed to reduced engagement with preventive care, including screening participation [28].
Patient–provider communication played a crucial role in shaping screening decisions. Our findings align with prior research showing that Black patients often report feeling dismissed or inadequately supported in clinical encounters, and experience disparities in communication, such as shorter visits, less patient-centered dialogue, and greater provider verbal dominance compared to White patients [29–31]. These results underscore the need for empathic, trust-building communication that validates patient concerns and promotes psychological safety. Training in implicit bias, cultural competence, and empathic communication may help strengthen patient–provider relationships. Future research should assess whether such efforts improve engagement and reduce screening barriers.
Stigma also emerged as a prominent barrier, consistent with prior research [32]. Participants described how stigma related to gender, socioeconomic status, and smoking history discouraged screening due to fears of judgment or discrimination. Addressing stigma is particularly critical among Black individuals due to their disproportionate burden of lung cancer [8–10]. Community-based health outreach could be adapted to explicitly address stigma and normalize screening discussions [30]. Studies could explore innovative approaches to destigmatize lung cancer screening through public awareness campaigns that amplify survivor voices and normalize the screening process.
Prioritization
Competing life demands and social determinants of health, such as housing instability, financial insecurity and caregiving responsibilities often led participants to delay their own health needs, including preventive care. Participants also described a perceived lack of prioritization of lung cancer screening within the healthcare system. This reinforced the perception that lung cancer screening is less important. Uncertainty about screening costs and insurance coverage may further discourage care-seeking.
These findings highlight the need for healthcare systems to elevate lung cancer screening as a key component of preventive care. Proactive provider engagement, including initiating discussions, routine reminders, and integration of screening into primary care can help normalize the practice and improve uptake among screening-eligible Black individuals. At the policy level, expanding insurance coverage and eliminating cost-related barriers are essential to improving access.
Psychological barriers, particularly fear of a cancer diagnosis, shaped how participants prioritized lung cancer screening, often fueled by personal or family experiences and uncertainty about outcomes. This fear led to avoidance and fatalism, highlighting the need for outreach that frames screening as a safe and effective tool for early detection. Culturally tailored education, health literacy promotion, and peer-led efforts can help address fears and improve engagement. One study found that while informational leaflets may increase knowledge about lung cancer screening, they may not be sufficient on their own to overcome fear [33]. This underscores the importance of combining knowledge dissemination with trust-building and emotional support strategies to effectively promote screening uptake. Despite these concerns, participants emphasized the value of lung cancer screening, particularly for Black communities disproportionately affected by tobacco-related illness, environmental exposures, and structural barriers to care.
Placement
Our findings highlight the role of geographic access on lung cancer screening behaviors. Participants described a lack of nearby screening services and minimal visibility of outreach materials in their neighborhoods, contributing to the perception that screening was inaccessible. Many participants cited barriers to traveling outside their immediate neighborhood, including time, cost, and caregiving responsibilities. These barriers reflect broader patterns of resource inequity in cities like NYC, where historically underserved neighborhoods, often impacted by long-standing disinvestment, face persistent barriers to preventive healthcare access [34]. To address placement-related barriers, public health systems must ensure equitable allocation of screening resources across neighborhoods. Investing in infrastructure within historically underserved communities and prioritizing localized, convenient access to screening services can help bridge the gap between awareness and action, ultimately improving uptake and reducing disparities.
Although our study has important findings, it is not without limitations. While our sample allowed us to reach thematic saturation [22], we recognize that the Black community is diverse, and a larger sample could enable deeper stratification across important participant characteristics such as socioeconomic status, gender, ethnicity, and geographic location.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kratzer TB, Bandi P, Freedman ND, Smith RA, Travis WD, Jemal A, Siegel RL (2024) Lung cancer statistics, 2023. Cancer 130(8):1330–1348. 10.1002/cncr.3512838279776 · doi ↗ · pubmed ↗
- 2Siegel RL, Miller KD, Wagle NS, Jemal A (2023) Cancer statistics, 2023. Cancer J Clin 73(1):17–48. 10.3322/caac.21763 · doi ↗
- 3Dwyer LL, Vadagam P, Vanderpoel J, Cohen C, Lewing B, Tkacz J (2023) Disparities in Lung Cancer: A Targeted Literature Review Examining Lung Cancer Screening, Diagnosis, Treatment, and Survival Outcomes in the United States. J racial ethnic health disparities. 10.1007/s 40615-023-01625-2 Advance online publication · doi ↗
- 4Lortet-Tieulent J, KulhánováI, Jacobs EJ, Coebergh JW, Soerjomataram I, Jemal A (2017) Cigarette smoking-attributable burden of cancer by race and ethnicity in the United States. Cancer causes control: CCC 28(9):981–984. 10.1007/s 10552-017-0932-928748344 · doi ↗ · pubmed ↗
- 5Siegel RL, Miller KD, Jemal A, Cancer statistics (2018) CA Cancer J Clin. 2018;68 (1):7–3029313949 10.3322/caac.21442 · doi ↗ · pubmed ↗
- 6Tanner NT, Thomas NA, Ward R, Rojewski A, Gebregziabher M, Toll B, Silvestri GA (2019) Association of Cigarette Type With Lung Cancer Incidence and Mortality: Secondary Analysis of the National Lung Screening Trial. JAMA Intern Med 179(12):1710–1712. 10.1001/jamainternmed.2019.348731633739 PMC 6806424 · doi ↗ · pubmed ↗
- 7Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A (2025) Cancer statistics, 2025. Cancer J Clin 75(1):10–45. 10.3322/caac.21871 · doi ↗
- 8Annangi S, Nutalapati S, Foreman MG, Pillai R, Flenaugh EL (2019) Potential racial disparities using current lung cancer screening guidelines. J Racial Ethn Health Disparities 6:22–2629729002 10.1007/s 40615-018-0492-z · doi ↗ · pubmed ↗