Low-density asymptomatic parasitemia in southern Zambia does not lead to clinical malaria and is not associated with household transmission: results from a two-year cohort study
Jessica L. Schue, Anne C. Martin, Japhet Matoba, Caison Sing’anga, Mukuma Lubinda, Ben Katowa, Michael Musonda, Sophie Berube, Timothy Shields, Tamaki Kobayashi, Harry Hamapumbu, Edgar Simulundu, Douglas E. Norris, Amy Wesolowksi, William J. Moss

TL;DR
A study in Zambia found that low-level asymptomatic malaria infections do not lead to clinical malaria or household transmission, suggesting they may not need treatment for elimination.
Contribution
Demonstrates that asymptomatic low-density parasitemia does not contribute to clinical malaria or household transmission in low-transmission settings.
Findings
Low-density asymptomatic parasitemia was common but not linked to clinical malaria.
No evidence of household transmission from asymptomatic parasitemia beyond one month.
Parasite prevalence remained low with median density of four parasites/μL.
Abstract
In low malaria transmission settings targeting elimination, the World Health Organization recommends a combination of mass (e.g., mass test-and-treat), targeted (e.g., chemoprophylaxis or treatment for travelers), and reactive (e.g., reactive drug administration) strategies. Most of these strategies would not identify and treat individuals with asymptomatic parasitemia. This study was conducted in a pre-elimination setting in Southern Province, Zambia to examine risk factors for asymptomatic parasitemia, its epidemiologic relationship to incident clinical malaria, and evidence of its contribution to ongoing transmission to inform policy on whether these parasitemic individuals need to be identified and treated to achieve malaria elimination. An intensive longitudinal cohort study of 197 households within the catchment area of a single health center was designed to capture all clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
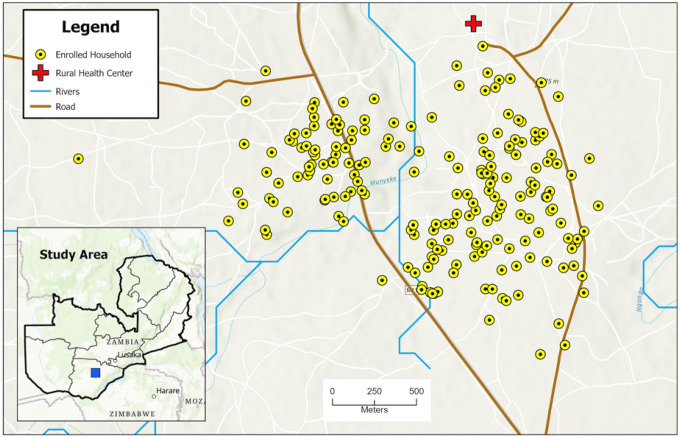 Figure 1
Figure 1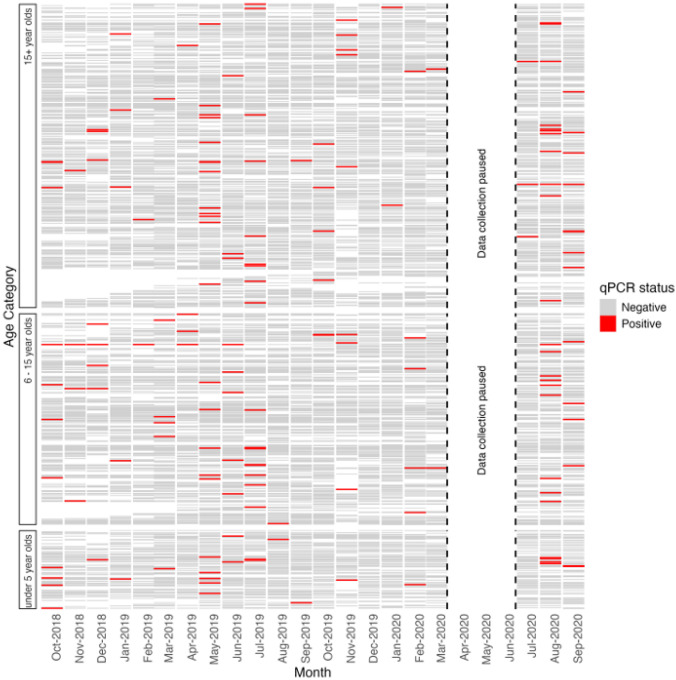 Figure 2
Figure 2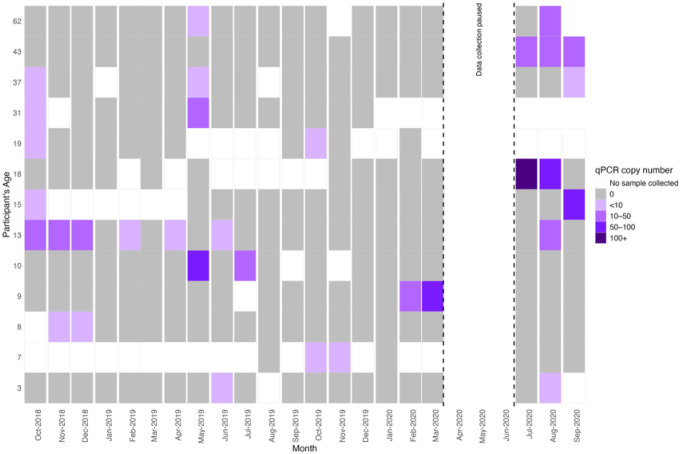 Figure 3
Figure 3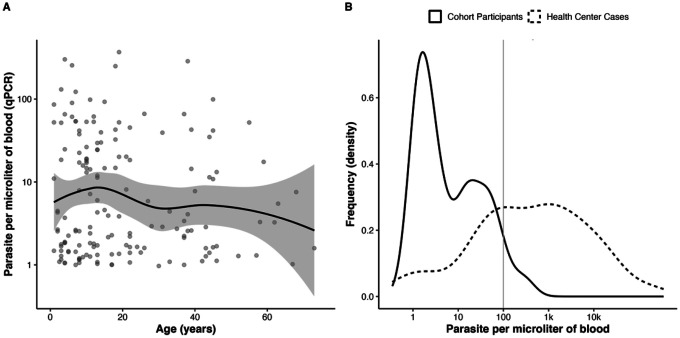 Figure 4
Figure 4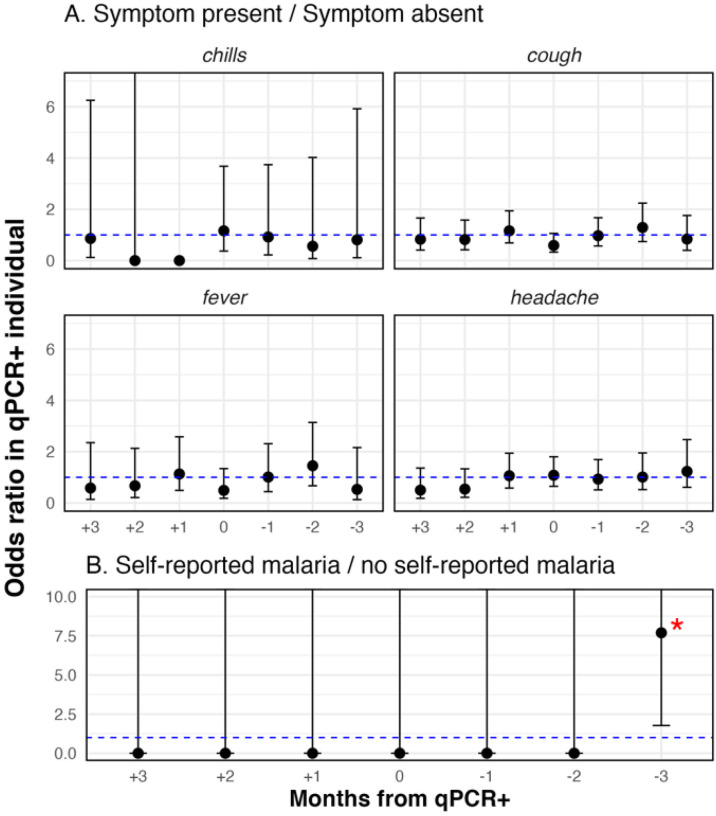 Figure 5
Figure 5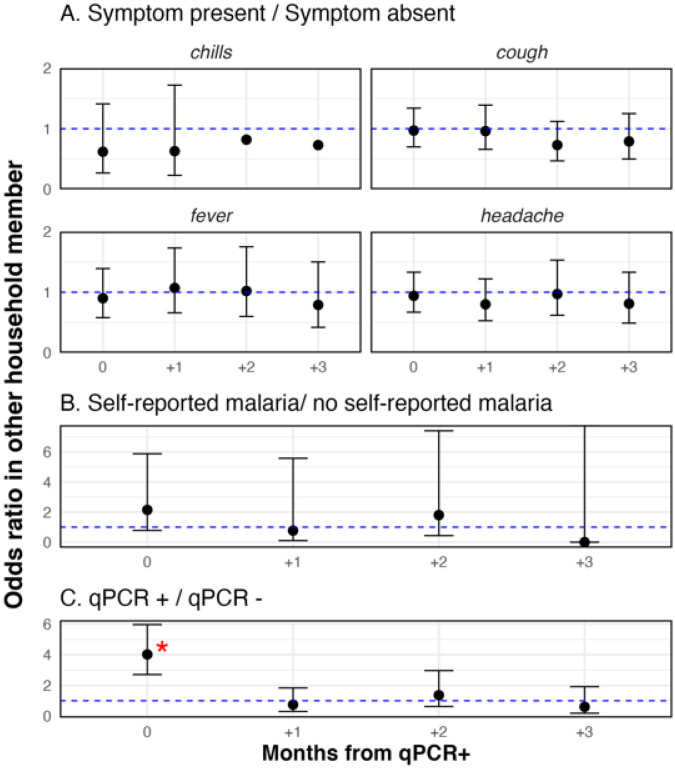 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · Parasites and Host Interactions · Parasitic Diseases Research and Treatment
Background
As of 2025, 47 countries achieved malaria elimination through a combination of mass, targeted, and reactive interventions (1). Understanding the causes of residual transmission in an area approaching elimination is necessary to deliver appropriate interventions and ultimately achieve malaria elimination. Residual transmission may be due to repeated parasite introductions via imported cases or ongoing low-level transmission from symptomatic infections prior to their treatment and/or untreated chronic, asymptomatic infections (2). These drivers are countered most effectively with different interventions. For example, reactive test-and-treat can curb transmission introduced from imported cases and symptomatic infections, whereas mass drug administration (MDA) can clear infections that may not result in clinical symptoms or be detected by available diagnostics and thus act as reservoirs for transmission (3–5).
Asymptomatic infections with moderate levels of parasitemia are major gametocyte reservoirs in high and moderate transmission settings and contribute disproportionately to onward transmission (6–8). In low transmission settings, where individuals have less protective immunity against clinical disease, asymptomatic parasitemias are typically low-density (9), undetectable by point-of-care testing (10), and linked to persistent carriage across transmission seasons (11, 12), but are of unknown clinical and public health relevance. Asymptomatic parasitemia in low transmission settings could be important if they are a prelude to clinical malaria in the infected individual or a source of transmission to other individuals. However, few cohort studies have been conducted in pre-elimination settings to understand the relationships between asymptomatic parasitemia and subsequent clinical malaria or asymptomatic parasitemia and subsequent parasitemia in other household members.
This work describes a prospective longitudinal cohort study designed to capture all cases of clinical malaria and asymptomatic subpatent parasitemia in a geographically defined population in Southern Province, Zambia. Background prevalence of asymptomatic parasitemia with Plasmodium falciparum is 1–3% by quantitative PCR (qPCR) (13). Specifically, this study seeks to guide elimination strategies in low transmission settings through examination of asymptomatic parasitemia: its risk factors, its epidemiologic relationship to incident clinical malaria, and evidence of its linkage to ongoing transmission.
Methods
Study Site
A 24-month longitudinal cohort study was conducted from October 2018 through September 2020 in Choma District, Southern Province, Zambia, a low-transmission setting typical of southern Zambia. The region has a tropical savannah climate with a rainy season from December to April, followed by a cool dry season from May to August, and a hot dry season from September to November. The primary malaria vector is Anopheles arabiensis, which peaks during the rainy season (14, 15). The study site was a contiguous two-square-kilometer area, defined by natural borders of roads and footpaths, located within the catchment of Mapanza Rural Health Centre (RHC) (Fig. 1).
Household and participant selection
All households within the study site were enumerated using satellite imagery and were invited to participate. Geocoordinates of consenting households were captured by global positioning system (GPS) devices. Throughout the study period, newly constructed and newly occupied households in the study area also were invited to participate. Enrolled households were visited monthly for a minimum of one year. If a household agreed, the study visits continued into a second year.
All household residents and overnight visitors older than three months of age were invited to participate. Participants were classified as either a permanent resident, temporary resident (household resident for 2 months or more), or visitor (household resident for fewer than 2 months). Individuals younger than three months or with severe illness other than malaria were excluded. Written informed consent was obtained from each participant 16 years of age or older. Parental or guardian permission was obtained for all children younger than 16 years of age, and assent was obtained from children 13 to 15 years old.
Cohort data collection
Household and individual surveys were administered monthly, except between April and July 2020 when community data collection was paused in compliance with the Government of the Republic of Zambia’s COVID-19 prevention measures. The household survey recorded household size, amenities, net ownership, and history of indoor residual spraying. Each visit captured the number and condition of nets in the household, where household members slept, and any visitors to the household. House construction variables such as roof and wall material were collected for each sleeping structure within a household complex. Individual surveys captured demographic characteristics, socio-economic indicators, use of nets, times spent indoors versus outdoors, travel history, recent illnesses, and health care seeking behavior. Travel history included the location, purpose, and duration of up to four trips during the previous month. Each participant also had their tympanic temperature taken, and those with a temperature at 38° Celsius or higher were administered a malaria rapid diagnostic test (RDT) (SD Bioline Malaria AG P.f., Abbott, Abbott Park, Illinois, USA). Participants who tested positive were offered treatment with artemether-lumefantrine (16). Pregnant women and children under 5 kilograms who tested positive were to be offered transportation to the health center treatment. Dried blood spots (DBS) were collected monthly for detection of P. falciparum parasitemia by qPCR.
Health center symptomatic surveillance
Passive case detection was established at Mapanza RHC, the catchment area of which included the cohort households, and its aflliated health posts. Individuals older than three months of age who tested positive for malaria by RDT were asked to participate in the study by the health center staff. Those who provided written consent were administered a brief questionnaire, including basic demographic information, recent travel, bed net use, recent illnesses, and whether or not they were participants in the cohort study. DBS were collected from all consenting patients for the detection of P. falciparum by qPCR.
Laboratory Testing
DNA was extracted from the DBS using a standard saponin and Chelex-100 extraction procedure, and qPCR targeting the P. falciparum cytochrome-b gene was done using SYBR Green PCR Master Mix (Applied Biosystems, Thermo Fischer Scientific Inc, Waltham, MA) (10). All samples were run in duplicate. Parasite density was estimated based on the cycle threshold, and samples were considered positive if at least one of the two wells had a parasite density above one parasite/μL and a melting point within ± 0.5° Celsius of the melting point of the 3D7 g-DNA control. Positive samples were run on gel electrophoresis to confirm the DNA product size.
Data Analysis
Parasite prevalence by qPCR and the incidence of clinical malaria using health center surveillance were calculated across the study period. Monthly parasite prevalence (the proportion of participants parasitemic in a given month) and period prevalence (the proportion of participants ever-parasitemic) were calculated. Annual incidence of clinical malaria was calculated using the cohort cases captured in health facility surveillance and by self-reported confirmed malaria diagnoses at locations other than Mapanza RHC. These were summed and divided by the person-months of the study period (excluding the months the study was paused) and multiplied by twelve to estimate the annual incidence.
Descriptive and statistical analysis evaluated risk factors for asymptomatic parasitemia and evidence of the clinical and public health relevance of asymptomatic parasitemia as a prelude to clinical malaria or a source of transmission to other household members. To explore risk factors for asymptomatic parasitemia, multiple analyses were performed. First, summary statistics were stratified by participants who were ever versus never positive by qPCR to examine univariate risk factors associated with being ever positive. Differences were compared using Fisher’s exact test for proportions and the Kruskal-Wallis test for continuous data. Second, univariate regression was used to test for associations between qPCR positivity and age group, travel, and net usage. Finally, to assess if parasitemia occurred randomly across the population, a random forest model was constructed, maximizing predictive power for qPCR using available covariates, and the model fit was compared between the true study population (covariates and associated qPCR outcomes) and an alternate population where the covariates and associated qPCR outcomes were unlinked and qPCR outcomes were randomly assigned.
The possible clinical relevance of asymptomatic parasitemia as an indicator of subsequent or prior clinical malaria in the parasitemic individual was explored by examining the association between qPCR positivity and two individual-level outcomes in the six months surrounding the positive event: symptoms reported and self-reported malaria diagnosis. Logistic regression was used to examine the odds ratio of each outcome in those parasitemic by qPCR compared to those who were qPCR negative in each of the three months preceding and following the month in which the outcome was measured. All analyses adjusted p-values for multiple comparisons using a Bonferroni approach.
To explore the possible public health importance of asymptomatic parasitemia as a source of transmission to other individuals, associations were examined between individual qPCR positivity and three outcomes in other household members during the three months following the positive event, including symptoms reported, self-reported malaria diagnosis, and qPCR positivity, using the same statistical approach as described above for associations with clinical malaria.
To account for potential false positive qPCR results, a sensitivity analysis was conducted for which qPCR positivity was defined as any qPCR positive test with a parasite density of at least 10 parasites/μL. All analyses were done using R version 4.2.3.
Results
A total of 201 households, some comprised of multiple structures, were identified during the two years of the study, 197 were enrolled, and complete monthly data were obtained for 167 (83%) households. Over the 24 months of the study, 1198 persons were screened and 1071 (89%) were enrolled. Median participant age was 16 years (IQR: 8–28), and 58% of participants were female (Table 1). Median household size was 5 people (IQR: 3–7, range: 1–18).
Incidence of clinical malaria was low
The incidence of clinical malaria in the cohort was 46.7 cases per 1000 person-years, with an incidence of 24.9, 27.1, and 50.7 cases per 1000 person-years in individuals younger than 5 years old, 6 to 15 years, and 15 years and older, respectively. Mapanza RHC recorded 206 confirmed cases of malaria by RDT, of which only four were participants in the cohort study. These four cases occurred during the COVID-19 pandemic when data collection was paused (Table S1). An additional forty cohort members reported a malaria diagnosis at a different health care facility, most commonly, nearby Macha Hospital. None of these forty were qPCR positive in the month of, the month preceding, or the month following their self-reported diagnosis of malaria, although most (n = 34) reported taking Coartem^®^ (artemisinin-lumefantrine), which rapidly clears parasitemia. Three reported finishing their course of medication the day prior to the study visit, ten reported having finished their treatment course within the prior week, and 21 completed their treatment more than one week prior to the study visit. An additional four adult cohort participants reported taking antimalarial medications from a traditional healer, friend, family member, or local chemist and were not included in the case count.
Parasite prevalence and density were low in those with asymptomatic parasitemia
There were 164 episodes of parasitemia identified by qPCR in 144 individuals (Table 1, 13.3% of individuals). No RDT positive participants were identified in the cohort despite testing those who were febrile at the time of the study visit (n = 43). Monthly mean parasite prevalence was 1.5% and highest in May 2019 (4.2%), July 2019 (3.5%), and August 2020 (4.4%) (Figure S1). Most (89%) individuals who were ever parasitemic were only positive once (Figure 2). Fifteen individuals were parasitemic on more than one study visit, for an average of 2.4 monthly visits (Range: 2 – 7) (Figure 3), although none of these individuals self-reported having clinical malaria during the study period.
The median parasite density was only four parasites/μL (IQR: 2 – 23) (Figure 4, Panel B), much lower than the parasite density for clinical cases at Mapanza RHC (393 parasites/μL, IQR: 41 – 3340). Most (96%) qPCR positive individuals had parasitemia levels below 100 parasites/μL. There was a decreasing trend but no statistical correlation between age and level of parasitemia (Figure 4, Panel A) (Pearson correlation coeflcient, r = −0.13).
While travel, household visitors, and bed net use varied, none were risk factors for parasitemia
The odds of parasitemia by qPCR were not different among those who reported travel (odds ratio: 0.82, p-value= 0.45), nor among individuals living in households with others who had travelled (odds ratio: 1.0, p-value= 0.77). The odds of parasitemia by qPCR were not higher in visitors (odds ratio: 1.3, p-value= 0.59) nor in individuals living in households that had a visitor (odds ratio: 1.2, p-value= 0.46). Using a net was not associated with parasitemia by qPCR (odds ratio: 1.0, p-value= 0.34).
Common symptoms of malaria were prevalent but not associated with parasitemia
There was no statistical association with current or lagged parasitemia and fever, cough or headache (Figure 5, Panel A). The prevalence of fever was 7.5% in children younger than 5 years, 3.2% in children 5–15 years, and 5.1% in those older than 15 years. There were 43 instances of fever at the time of the study visit among 40 household residents, but only one febrile individual was parasitemic by qPCR.
Univariate analysis examined associations between parasitemia by qPCR and clinical outcomes to assess evidence of the clinical relevance of qPCR positivity. The alpha for the significance threshold was adjusted for multiple comparisons. A) qPCR positivity and symptoms of malaria B) qPCR positivity and self-reported malaria. Participants were asked to self-report malaria diagnoses received at a health facility.
There was no evidence that those with parasitemia progressed to clinical malaria
Most (97%) of the 147 individuals ever parasitemic by qPCR did not report any episodes of clinical malaria during the 24-month study period. Specifically, no qPCR infected individuals reported clinical malaria in the three months prior or two months following their episode of parasitemia. Three months after individuals self-reported a diagnosis of clinical malaria, their odds of having parasitemia by qPCR were higher than the odds of parasitemia by qPCR in individuals with no history of clinical malaria (univariate odds 7.6, CI [1.8, 33.5] p-value = 0.0066) (Figure 5, Panel B), but there was no association in the months preceding the diagnosis of clinical malaria nor during the first or second month following diagnosis.
There was no evidence that parasitemia was associated with subsequent clinical malaria in other household members
There was no statistical association between parasitemia by qPCR and symptoms of malaria or self-reported malaria in other household members in the three months following the qPCR positive test result (Figure 6, Panels A, B). Individuals with parasitemia by qPCR clustered at the household level, where in a households with a qPCR positive individual, the odds of having other positive members in the same month were four times the odds of having no positive household members that month (Odds ratio: 4.0, 95% CI: 2.7, 6.0). However, there were no higher odds of household members being parasitemic by qPCR in the three months following parasitemia in the index case, suggesting no association with household transmission.
Univariate analyses examined associations between qPCR positivity and outcomes in other household members to examine whether parasitemia led to onward transmission: A) individual qPCR positivity and symptoms of malaria in household members; B) individual qPCR positivity and self-reported malaria; and C) individual qPCR positivity and qPCR positivity in household members.
The results of the sensitivity analysis were consistent with the main results, although, as expected, there were fewer episodes of parasitemia. When restricting the definition of qPCR positivity to those with parasite levels of at least 10 parasites/μL, only 66 episodes of parasitemia were identified in 57 individuals. Full results of the sensitivity analyses are shown in the supplementary materials.
Discussion
In a two-year longitudinal cohort study in a low transmission setting in southern Zambia, the prevalence of parasitemia was low but persistent throughout the study period and across a wide age range. Parasite density was quite low and most episodes of parasitemia were transient, subsequently either cleared by the immune system or below the limit of detection. There was no evidence to support the hypothesis that low-density parasitemia led to symptomatic malaria. Despite the fact that asymptomatic parasitemia clustered in households within the same month, consistent with the idea of shared household risk factors and consistent with prior research demonstrating spatial clustering of asymptomatic parisitemia. there was no association with an increased risk of parasitemia or reported clinical malaria among household members in subsequent months that would be consistent with onward transmission (13,17). These findings suggest that, in this low transmission setting in southern Zambia, programmatic efforts to identify and treat low level parasitemia of this magnitude are not needed to prevent clinical malaria or achieve malaria elimination.
Asymptomatic parasitemia was not associated with typical malaria risk factors of sex, travel, or net usage. In low transmission settings, older individuals are expected to have premunition and thus higher odds of asymptomatic parasitemia of lower density, whereas younger children are assumed to be relatively immunologically naive and to have symptomatic disease when parasitemia (18). Instead, there were no significant decreases in parasite density by age and asymptomatic parasitemia was prevalent in children younger than five years.
Other studies have shown that any level of parasitemia carries a risk of onward transmission (19,20). Currently, Southern Province, Zambia deploys a reactive test-and-treat strategy following focal investigations, in which a malaria case at a health center triggers a reactive response around the case’s residence. RDTs are used for screening, which would have missed nearly all the parasitemic individuals identifiedin this cohort. To detect these low-level parasitemias, more sensitive tools are needed (21), but even newer ultra-sensitive RDTs would not have detected the level of parasitemia identified in this study (22).
Inherent in interview-based surveys are biases that may come with self-reporting. For example, net usage may be somewhat overestimated due to social desirability bias. However, this is an unavoidable limitation in this context, and the seasonal trends observed in net usage are unlikely to be differentially impacted. A more significant limitation is that most clinical cases were self-reported by individuals who sought care at a health facility not included in the study. However, because these individuals were followed monthly in this cohort, their recall for malaria diagnosis is expected to be relatively accurate. Under the assumption that these self-reported cases are wholly misclassified, the null finding that there is no relationship between clinical and asymptomatic infection may be incorrect, although the absence of clinical malaria in cohort members during the study period supports this conclusion – that these low level parasitemias have no clinical significance. Overall, the repeated longitudinal measurements in this cohort study minimize recall bias and the design is an overall strength.
Low-level parasitemia was prevalent in this low transmission setting in southern Zambia. There was no evidence that low-level asymptomatic parasitemia led to clinical malaria or transmission to other household members. Thus, programmatic efforts to identify and treat individuals with low level parasitemia of this magnitude is not warranted to minimize the disease burden or achieve malaria elimination.
Supplementary Material
Supplementary Files
This is a list of supplementary files associated with this preprint. Click to download.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Countries and territories certified malaria-free by WHO [Internet]. [cited 2025 July 9]. Available from: https://www.who.int/teams/global-malaria-programme/elimination/countries-and-territories-certified-malaria-free-by-who
- 2Ahmed S, Reithinger R, Kaptoge SK, Ngondi JM. Travel Is a Key Risk Factor for Malaria Transmission in Pre-Elimination Settings in Sub-Saharan Africa: A Review of the Literature and Meta-Analysis. Am J Trop Med Hyg. 2020 Oct;103(4):1380–7.32815497 10.4269/ajtmh.18-0456 PMC 7543864 · doi ↗ · pubmed ↗
- 3Deutsch-Feldman M, Hamapumbu H, Lubinda J, Musonda M, Katowa B, Searle KM, Eflciency of a Malaria Reactive Test-and-Treat Program in Southern Zambia: A Prospective, Observational Study. Am J Trop Med Hyg. 2018 May;98(5):1382–8.29557330 10.4269/ajtmh.17-0865 PMC 5953385 · doi ↗ · pubmed ↗
- 4Nguyen TD, Tran TNA, Parker DM, White NJ, Boni MF. Antimalarial mass drug administration in large populations and the evolution of drug resistance. PLOS Glob Public Health. 2023 July 26;3(7):e 0002200.37494337 10.1371/journal.pgph.0002200 PMC 10370688 · doi ↗ · pubmed ↗
- 5Pinchoff J, Hamapumbu H, Kobayashi T, Simubali L, Stevenson JC, Norris DE, Factors Associated with Sustained Use of Long-Lasting Insecticide-Treated Nets Following a Reduction in Malaria Transmission in Southern Zambia. Am J Trop Med Hyg. 2015 Nov 4;93(5):954–60.26324729 10.4269/ajtmh.15-0093 PMC 4703265 · doi ↗ · pubmed ↗
- 6Rek J, Blanken SL, Okoth J, Ayo D, Onyige I, Musasizi E, Asymptomatic School-Aged Children Are Important Drivers of Malaria Transmission in a High Endemicity Setting in Uganda. The Journal of Infectious Diseases. 2022 Aug 15;226(4):708–13.35578987 10.1093/infdis/jiac 169PMC 9441202 · doi ↗ · pubmed ↗
- 7Sumari D, Mwingira F, Selemani M, Mugasa J, Mugittu K, Gwakisa P. Malaria prevalence in asymptomatic and symptomatic children in Kiwangwa, Bagamoyo district, Tanzania. Malar J. 2017 Dec;16(1):1–7.
- 8Sumner KM, Freedman E, Abel L, Obala A, Pence BW, Wesolowski A, Genotyping cognate Plasmodium falciparum in humans and mosquitoes to estimate onward transmission of asymptomatic infections. Nat Commun. 2021 Feb 10;12(1):909.33568678 10.1038/s 41467-021-21269-2PMC 7875998 · doi ↗ · pubmed ↗