Factors associated with and patterns of alcohol intake in late survivorship for breast cancer survivors
Sanjna Rajput, Robert A. Vierkant, Kayleigh N. Olson, Nicole L. Larson, Daniela L. Stan, Dawn M. Mussallem, Stacy D. D’Andre, Fergus J. Couch, Janet E. Olson, Ciara C. O’Sullivan, Kathryn J. Ruddy

TL;DR
This study examines alcohol consumption patterns and factors influencing alcohol intake among breast cancer survivors four years after diagnosis.
Contribution
The study identifies demographic and lifestyle factors associated with alcohol intake in late survivorship of breast cancer patients.
Findings
Alcohol intake remained stable in late survivorship, with 30.2% abstaining and 48.8% consuming 1–4 drinks weekly.
Younger age and current smoking were strongly associated with higher alcohol intake at Year 4.
Mild exercise was linked to increased alcohol intake over time, though physical health was not significant in adjusted models.
Abstract
To evaluate alcohol intake trends and identify demographic, clinical, lifestyle and socioeconomic factors associated with alcohol consumption in late survivorship among breast cancer survivors. Individuals diagnosed with stage 0–3 breast cancer enrolled in the Mayo Clinic Breast Disease registry between 2014 to 2022 reported their average weekly alcohol intake at baseline (time of diagnosis) and at approximately four years post-diagnosis. Alcohol intake was divided into four categories and cross-sectional associations with demographic, clinical, and lifestyle factors were examined using Monte Carlo-based Fisher exact tests and multivariable multinomial logistic regression. Changes in alcohol consumption from baseline to Year 4 were evaluated using Bowker’s test of symmetry and multinomial models. Among 719 participants, alcohol intake 4 years post diagnosis closely resembled baseline…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
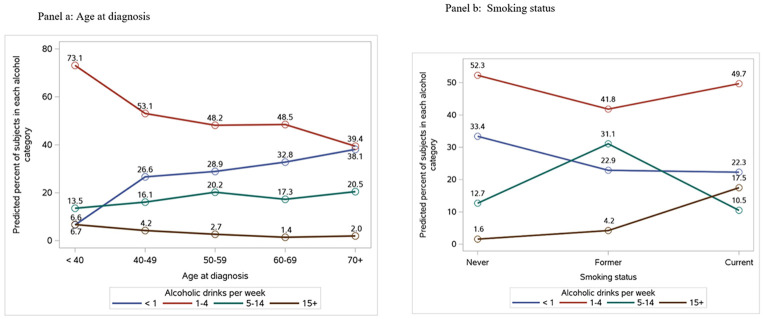 Figure 1
Figure 1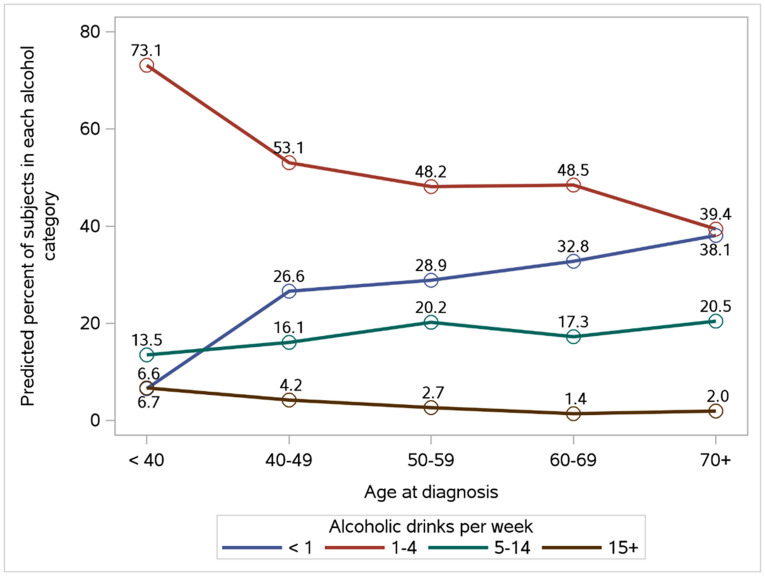 Figure 2
Figure 2- —National Cancer Institute and the Breast Cancer Research Foundation
- —National Institutes of Health or the Breast Cancer Research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAlcohol Consumption and Health Effects · Cancer survivorship and care · Cancer Risks and Factors
INTRODUCTION
Breast cancer (BC) is the most common cancer diagnosis among women in the United States,^1^ and in 2020, the worldwide BC incidence surpassed lung cancer for the first time.^2^ In recent decades, the overall incidence rates of BC in females have increased, specifically by 1% annually since 2012.^1^ With advances in systemic and local treatments as well as earlier detection through improved screening, death rates due to BC have decreased 44% since 1989, preventing over 500,000 estimated deaths.^1^ Given high rates of survival, with the five-year survival rate for BC exceeding 90%, it is anticipated that an ever-increasing population will be living with, or be in remission from BC.^1^ Thus, evaluating and addressing factors which negatively influence BC outcomes is of the utmost importance.
Alcohol is a known carcinogen and has been linked to an increased BC incidence.^3-7^ Patients with a history of certain cancers, including BC, significantly benefit from healthy lifestyle choices.^8^ Approximately 30% of BC cases can be attributed to modifiable lifestyle factors, including alcohol intake.^6^ Recurrence and mortality have been found to be impacted by both pre- and post-diagnosis alcohol consumption levels, with studies suggesting that higher alcohol consumption is associated with an increased risk of overall mortality, and postdiagnosis alcohol intake is positively associated with breast cancer recurrence.^4^ Some studies also suggest a higher risk of recurrence in postmenopausal but not premenopausal women who regularly consume ≥ 6 grams of alcohol daily post-diagnosis (HR, 1.19; 95% CI, 1.01–1.40).^9^
Most of the available evidence has focused on the relationship between alcohol intake and BC incidence, and the results are relatively consistent.^10^ Less has been published on post-diagnosis alcohol intake and the risk of BC recurrence. Additionally, there are little or no studies assessing alcohol intake in late BC survivorship (often defined as the period from 2 to 5 years post-diagnosis).^11-13^ Multiple studies show that, following a BC diagnosis, patients are likely to alter their dietary habits and alcohol intake (i.e., eating a more balanced diet and/or reducing alcohol intake).^14-15^ While cancer survivorship guidelines suggest limiting alcohol intake, if not avoiding it altogether,^16^ some cancer survivors continue to consume alcohol, and may even increase their intake post BC diagnosis. Studies suggest roughly 75% of cancer survivors drink alcohol post diagnosis, with many partaking in risky consumption patterns (consuming > 2 drinks per day, binge drinking i.e. consuming ≥ 6 drinks on a single occasion, hazardous drinking i.e. AUDIT-C scores ≥ 3).^14, 17-18^ Many studies do not monitor long-term alcohol intake in BC survivors, which is critical as these patients are now living longer than ever before.
Our group previously studied demographic, lifestyle, and clinical characteristics associated with changes in alcohol intake in a cohort of BC survivors in early survivorship, i.e., in the year following BC diagnosis.^19^ However, alcohol use is not static across survivorship; it is shaped by evolving clinical, psychological, and social factors. Our current study therefore aims to assess changes in and associations with alcohol intake in the same cohort of BC survivors later in survivorship, i.e. four years following BC diagnosis.
METHODS
Individuals aged 18 or older who were diagnosed with BC within the past year and had at least one clinical visit at the Mayo Clinic in Rochester, Minnesota, were prospectively enrolled in the Mayo Clinic Breast Disease Registry (MCBDR) upon providing informed consent. Participants diagnosed with BC between 2014 and 2022 were asked to provide information regarding their alcohol intake on the initial (baseline) survey and again at approximately four years after diagnosis.
Individuals who completed the alcohol intake question on both the baseline and four-year follow-up surveys were included in the analysis. Exclusion criteria included a diagnosis of stage IV BC, a documented BC recurrence prior to the completion of the Year 4 survey, or a baseline survey submitted more than one year after the initial diagnosis.
The baseline and Year 4 surveys assessed self-reported average number of alcoholic drinks consumed per week over the past 10 years, defining a standard drink as 5 ounces of wine, 12 ounces of beer, or 1 ounce of liquor. Reported alcohol use was categorized into four weekly intake levels: none, low (1–4 drinks), moderate (5–14 drinks), and high (15 or more drinks).
Participants provided clinical data and additional demographic information regarding their education level, the presence or absence of financial strain (e.g., difficulty paying bills or limited disposable income), their smoking behavior (never, former, current), exercise levels, menopausal status, and PROMIS-10 health scores. For exercise levels, participants reported the number of minutes per day and days per week of engagement in mild, moderate and strenuous exercise. Mild-intensity activity was defined as requiring “minimal effort”, moderate-intensity activity as “not exhausting” and strenuous activity as “heart beats rapidly”. The PROMIS Global-10 instrument consists of 10 items evaluating overall health, well-being, and distress, yielding scores for global physical health (GPH) and global mental health (GMH).^20^ These scores are presented as T-scores derived from raw totals, where a T-score of 50 represents the average of the U.S. general population, with a standard deviation of 10. Higher T-scores indicate better physical or mental health. T-scores were categorized based on approximate quartiles amongst all participants returning baseline questionnaires. Data was abstracted by trained nurses from electronic medical records—including patient race, gender, age at diagnosis, cancer stage and features, BRCA mutation status, and post-diagnosis treatments (such as surgery, radiation, chemotherapy, and/or endocrine therapy)—were incorporated into the analysis.
Statistical methods
Data were summarized using frequencies and percents for categorical variables and means and standard deviations for continuous variables. Associations of participant attributes with return of the Year 4 questionnaire, among all patients returning the baseline questionnaire, were assessed using chisquare tests.
Among participants returning the Year 4 questionnaire, univariable cross-sectional associations of Year 4 alcohol intake with demographic and clinical characteristics were carried out using Monte Carlo-based Fisher exact tests. In brief, for a given comparison, a cross-tabulated table was created using the observed data and the Fisher test statistic was calculated. Following this, 10,000 random samples of cross-tabulated tables were generated, conditional on the same total sample size, column totals, and row totals as the observed table. The Monte Carlo p-value was then determined as the proportion of the resulting 10,000 tables that yielded a test statistic at least as large as the one observed. We chose Monte Carlo-based tests rather than traditional Fisher exact tests because the number of permutations needed to calculate the exact tests was extremely large and memory intensive. Following these univariable associations, we fit a nominal, multivariable, multi-categorical logistic regression model to determine variables independently associated with Year 4 alcohol intake. Alcohol intake was fit as the outcome, and all variables univariably associated with alcohol intake (p < 0.05) were included in the model, using a multinomial distribution and a generalized logit (glogit) link function. Because multinomial logistic regression odds ratios can be challenging to interpret, we instead presented estimated marginal percents of participants falling within a given alcohol intake category for each level of each characteristic of interest, similar to the calculation of least squares means for continuous outcome variables. First, predicted probabilities of alcohol intake were calculated for each combination of all variables in the model. Then, for a given level of a given characteristic of interest, the mean of the predicted probabilities of alcohol intake for that level were determined by averaging all predicted probabilities for that level across all combinations of the other variables in the model. These marginal predicted probabilities were multiplied by 100 to arrive at predicted percents.
Change in alcohol intake from baseline to Year 4 was assessed using Bowker’s test of symmetry. Following this, we examined univariable associations of changes in alcohol intake from baseline to Year 4 with characteristics of interest, again using Monte Carlo-based Fisher exact tests. For these associations, data were subset to participants with baseline alcohol intake of 1–4 or 5–14 drinks per week, since participants at the lower extreme of alcohol intake (< 1 drink per week) could not decrease alcohol consumption at Year 4 and those at the higher extreme (15 + drinks per week) could not increase alcohol consumption at Year 4. Participants were grouped into three change categories based on change in alcohol intake from baseline: decreased alcohol intake at Year 4, no change in alcohol intake at Year 4, increase in alcohol intake at Year 4. Multivariable analyses again included all variables found to be univariably significant (p < 0.05), and resulting marginal percents calculated, similar to the Year 4 cross-sectional analyses.
All statistical tests were two-sided, and all analyses were carried out using the SAS system (SAS Institute, Inc., Cary, NC).
RESULTS
A total of 2230 patients with stage 0-3 BC returned a baseline questionnaire. Of these, we excluded 1502 who either did not return the Year 4 questionnaire or provided insufficient alcohol intake data at baseline or at Year 4, 2 whose BC recurred prior to the Year 4 questionnaire, and 7 who returned their baseline survey more than one year after their original diagnosis, resulting in a final cohort of 719 patients. Associations of participant characteristics with return of the Cohort 4 questionnaire, amongst all 2230 patients, are provided in Supplemental Table 1. Patients who were white, premenopausal, with Stage 0-2 disease, who did not undergo chemotherapy or radiotherapy, and who had higher PROMIS-10 mental and physical health scores were more likely to return the Year 4 questionnaire than their demographic and clinical counterparts.
Cohort characteristics are provided in Table 1. The mean age at BC diagnosis was 58.6 years (SD = 12.0). Ninety-nine percent of participants were female and 97% were of White race. Most participants were post-menopausal (74%). Approximately two-thirds of participants were never smokers (67%). More than half held a bachelor’s or graduate-level degree. One quarter of participants reported financial difficulty and 27% reported not engaging in at least mild exercise per week. Nearly half of participants had stage 1 BC (49%), and the majority of tumors were ER positive (85%), PR positive (77%) and HER2 negative (88%). Slightly more than half of the participants (51%) underwent lumpectomies, 66% received endocrine therapy, 27% received chemotherapy and 52% received radiotherapy.
Cross-sectional associations of alcohol intake at Year 4 with participant characteristics
Of the 719 participants, 217 (30%) reported little or no alcohol intake, 351 (49%) consumed 1-4 drinks per week, 134 (19%) consumed 5-14 drinks per week and 17 (2%) reported consuming 15 or more drinks per week. Univariable associations of alcohol intake at year 4 with participants characteristics are provided in Table 1. Lower alcohol consumption was associated with older age at diagnosis, such that 38.5% of participants aged 70 and older reported no alcohol intake compared to 6.4% of participants < 40 (p<0.001) (Table 1, Figure 1). Thirteen percent of current smokers reported consuming 15 or more alcoholic drinks per week compared to 3.7% for former smokers and 1.5% for never smokers (p<0.001). Alcohol intake was lower in participants reporting zero minutes of moderate exercise per week (p=0.001) and in participants reporting zero minutes of mild exercise per week (p=0.005) compared to those reporting at least some exercise. Similarly, participants with lower PROMIS global physical health scores were more likely to abstain from alcohol compared to those with higher scores: 71% with scores < 46 abstained compared to 54% with scores of 56 or greater (p<0.001). No significant associations were observed between alcohol intake and tumor-related or treatment characteristics (p>0.05 for each).
Age at diagnosis remained a significant correlate of alcohol consumption in multivariable analyses, in that 6.6% of participants less than age 40 reported no alcohol intake compared to 38.1% of participants 70 and older (p=0.022, Figure 1a, Supplemental Table 2). Smoking also remained significantly associated with alcohol consumption, such that 22% of current smokers abstained and 17.5% consumed 15 or more drinks per week compared to 33.4% and 1.6% for never smokers (p<0.001, Figure 1b, Supplemental Table 2). Exercise and physical health scores were no longer significantly associated with alcohol intake in multivariable analyses.
Trend in alcohol intake from Baseline to Year 4
The proportion of participants falling into each alcohol intake category at Year 4 was not significantly different from that at baseline (Bowker test for homogeneity p=0.13): 27.7% reported no alcoholic drinks per week at baseline compared to 30.2% at Year 4, 48.3% reported 1-4 weekly drinks at baseline compared to 48.8% at Year 4, 21.0% reported 5-14 drinks per week at baseline compared to 18.6% at Year 4, and 3.1% reported 15+ drinks per week at baseline compared to 2.4% at Year 4 (Table 2). Of the 719 participants, 73 (10.2%) increased alcohol intake from baseline to Year 4, 112 (15.6%) decreased intake and 534 (74.3%) did not change their intake.
Associations of change in alcohol intake from baseline to Year 4 with participant characteristics
Univariable associations of change in alcohol use from baseline to Year 4 with demographic and clinical characteristics, among the 498 participants not at the lowest or highest levels of baseline alcohol use, are presented in Table 3. Increases in alcohol consumption were more common in participants reporting 60-119 (13.0%) and 120+ minutes of strenuous exercise per week (15.9%) compared to those reporting 0 (7.5%) or 1-59 minutes per week (6.9%, p=0.011). Conversely, decreases in alcohol consumption were more common in participants reporting 0 (21.0%) or 1-59 minutes of strenuous exercise per week (34.5%) compared to those reporting 120+ minutes per week (7.2%, p=0.011). Similarly, participants reporting 240 or more weekly minutes of mild exercise per week were more likely to increase their alcohol consumption (18.4%) compared to those with 0 (9.7%), 1-119 (7.0%) or 120-239 minutes per week (4.6%, p=0.012). A lower proportion of participants who received endocrine therapy decreased their alcohol consumption from baseline to Year 4 (16.8%) than those who did not receive therapy (25.6%, p=0.047). No other demographic or clinical characteristics were significantly associated with changes in alcohol consumption (p>0.05 for each). In multivariable analyses, the only attribute associated with change in alcohol consumption was weekly minutes of mild exercise per week (p=0.026, Figure 2, Supplemental Table 3). Results were similar to those seen in univariable analyses, in that participants reporting lower levels of exercise were more likely to decrease their alcohol consumption compared to those reporting higher levels, and those reporting 240 or minutes of mild exercise per week were more likely to increase consumption compared to those reporting lower exercise levels.
DISCUSSION
In this prospective cohort study of BC survivors, we examined clinical, demographic, lifestyle, and socioeconomic factors associated with alcohol consumption four years after diagnosis, as well as changes in alcohol use from the time of diagnosis to late survivorship. Our group has previously found that in early survivorship (Year 1), participants were noted to overall reduce alcohol consumption compared to baseline, with the proportion of participants consuming <1 drink/week increasing from 28.9% at baseline to 60.2% at Year 1 and those drinking ≥1 drink/week declined from 71.2% at baseline to 39.8% at Year 1.^19^ Our new findings extend our prior research by evaluating behavior at a later point in the survivorship trajectory. This later timepoint captures a distinct and underexamined phase in survivorship, during which behavior patterns may stabilize or shift in response to long-term psychosocial adjustment, evolving health status, and changes in care intensity.
Consistent with prior studies in cancer populations, younger age at diagnosis was strongly associated with higher levels of alcohol intake in both univariable and multivariable cross-sectional analyses of alcohol use at Year 4. Studies have shown that cancer survivors <65 years of age are more likely to engage in current alcohol consumption, exceed moderate drinking and engage in binge drinking compared to those aged 65 years and older.^21-22^ These findings highlight the need for targeted interventions to address alcohol consumption and support sustainable behavioral change among younger cancer survivors, given the potential adverse effects on treatment outcomes and overall health.
Current smoking status remains a strong and consistent association with higher alcohol intake at Year 4 and across all timepoints including in our prior studies at baseline and Year 1. This is consistent with well-documented clustering of health risk behaviors. Continued smoking through several timepoints in survivorship may be influenced by comorbid psychological distress, anxiety and depression as well as insufficient cessation support.^23-24^ This dual-risk profile of combined alcohol and tobacco use has particular relevance for survivorship care, as combined use is associated with worse cancer outcomes such as recurrence and development of subsequent primary cancers as well as overall mortality.^25-26^ Identifying individuals with multiple behavioral risk factors highlights the need for increased psychologic support over time for affected patients and can help integrate behavioral counseling approaches more effectively.
In a multivariable model, survivors reporting higher levels of mild or strenuous exercise were found to be more likely to increase alcohol intake, while those with lower activity levels were more likely to reduce consumption. This finding mirrors the literature suggesting that some individuals may compensate for alcohol consumption through healthy behaviors such as exercise or may socialize more frequently in physically active settings that promote alcohol use.^27-29^
Treatment-related variables were not significantly associated with alcohol intake in cross-sectional models. This is a change from analyses at Year 1 revealing an association of chemotherapy with reduction in alcohol intake (which may have been due to chemotherapy-related taste-disturbances and nausea). This may reflect a decoupling of medical and behavioral trajectories as patients transition from active treatment into survivorship.
Our study also found that most BC survivors in our cohort (74.3%) reported a similar amount of alcohol consumption at baseline and at 4 years following diagnosis. Only 15.6% reported a decrease and 10.2% reported an increase in intake. This is a significant difference from the declines seen in alcohol use in this cohort one year after diagnosis. This suggests that the greatest behavior shifts may occur early post-diagnosis, with subsequent trajectories either stabilizing or partially reverting over time, and that initial post-diagnosis changes in behavior may not be sustained over time. This finding aligns with existing literature on “teachable moments” in cancer care, highlighting that early survivorship may be a limited window in which survivors are most receptive to lifestyle change.^30-31^ The adoption of healthier behaviors during and soon after cancer treatment may not be sustained in the long term as initial motivations wane, routine medical oversight lessens, and long-term coping patterns may change.^32^ This underscores the importance of addressing alcohol use as a dynamic, long-term behavior, and the need for repeated counseling throughout survivorship with regular reassessment and coordinated care between oncology and primary care providers to ensure sustained lifestyle improvements and better long-term health outcomes.
Strengths of this study include its longitudinal design, a large sample size, comprehensive collection of clinical, demographic, and lifestyle data, and its focus on a relatively unexplored phase of survivorship. To our knowledge, this is among the first studies to explore predictors of alcohol intake in BC survivors several years after diagnosis, providing insight into long-term behavioral patterns and their determinants. While our findings have important implications, they must be interpreted considering potential limitations. Supplemental analyses indicate that patients who were White, premenopausal, had lower-stage disease, did not receive chemotherapy or radiation, and reported higher physical and mental health scores were more likely to complete the Year 4 survey. These differences suggest that our sample may underrepresent survivors with more intensive treatment histories or poorer health status. The study is limited by lack of detailed information on the type of alcohol consumed (such as wine, beer, or spirits) and the context of consumption (e.g., with meals or binge drinking). Additionally, alcohol intake was self-reported and subject to recall and social desirability bias, which may have led to underreporting. Our sample was also demographically homogeneous with the vast majority being White and well-educated, limiting generalizability to more diverse populations.
In conclusion, many BC survivors drink alcohol four years after a BC diagnosis (a greater proportion than we found previously at one year after a BC diagnosis).^19^ These findings highlight the importance of continued, nuanced health behavior counseling in both early and late survivorship care, particularly targeting younger survivors, smokers, and those with more active lifestyles (perhaps because they may not perceive their alcohol intake as a health risk). Further research is warranted to explore the motivations underlying changes in alcohol use during cancer survivorship and to develop tailored interventions to support long-term health in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giaquinto AN, Sung H, Newman LA, Freedman RA, Smith RA, Star J, Jemal A, Siegel RL. Breast cancer statistics 2024. CA Cancer J Clin. 2024 Nov-Dec;74(6):477–495. doi: 10.3322/caac.21863.39352042 · doi ↗ · pubmed ↗
- 2Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021 May;71(3):209–249. doi: 10.3322/caac.21660.33538338 · doi ↗ · pubmed ↗
- 3International Agency for Research on Cancer. (2012). Review of human carcinogens (Vol. 100). World health organization.
- 4Schwedhelm C, Boeing H, Hoffmann G, Aleksandrova K, Schwingshackl L. Effect of diet on mortality and cancer recurrence among cancer survivors: a systematic review and meta-analysis of cohort studies. Nutr Rev. 2016 Dec;74(12):737–748. doi: 10.1093/nutrit/nuw 045.27864535 PMC 5181206 · doi ↗ · pubmed ↗
- 5Sohi I, Rehm J, Saab M, Virmani L, Franklin A, Sánchez G, Jhumi M, Irshad A, Shah H, Correia D, Ferrari P, Ferreira-Borges C, Lauby-Secretan B, Galea G, Gapstur S, Neufeld M, Rumgay H, Soerjomataram I, Shield K. Alcoholic beverage consumption and female breast cancer risk: A systematic review and meta-analysis of prospective cohort studies. Alcohol Clin Exp Res (Hoboken). 2024 Dec;48(12):2222–2241. doi: 10.1111/acer.15493. Epub 2024 Nov 24.39581746 PMC 11629438 · doi ↗ · pubmed ↗
- 6Islami F, Goding Sauer A, Miller KD, Siegel RL, Fedewa SA, Jacobs EJ, Mc Cullough ML, Patel AV, Ma J, Soerjomataram I, Flanders WD, Brawley OW, Gapstur SM, Jemal A. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018 Jan;68(1):31–54. doi: 10.3322/caac.21440.29160902 · doi ↗ · pubmed ↗
- 7World Health Organization. (2024, June 28). Alcohol. World Health Organization. https://www.who.int/news-room/fact-sheets/detail/alcohol
- 8Huang H, Zhao Y, Yi J, Chen W, Li J, Song X, Ni Y, Zhu S, Zhang Z, Xia L, Zhang J, Yang S, Ni J, Lu H, Wang Z, Nie S, Liu L. Post-diagnostic lifestyle and mortality of cancer survivors: Results from a prospective cohort study. Prev Med. 2024 Aug;185:108021. doi: 10.1016/j.ypmed.2024.108021.38821420 · doi ↗ · pubmed ↗