Parkinson’s and Alzheimer’s disease impairs temporal precision
Matthew A. Weber, Christopher M. Hunter, Nandakumar S. Narayanan

TL;DR
This paper finds that Parkinson’s and Alzheimer’s diseases consistently impair the ability to judge time accurately and precisely.
Contribution
The study shows that temporal precision is consistently impaired in Parkinson’s and Alzheimer’s disease across diverse timing tasks.
Findings
Temporal precision is reliably impaired in Parkinson’s disease across multiple studies.
Temporal precision is also impaired in Alzheimer’s disease, despite varied timing paradigms.
Temporal accuracy remains unaffected in both diseases.
Abstract
Several studies have reported temporal processing deficits in neurodegenerative diseases such as Parkinson’s and Alzheimer’s disease. These deficits can be quantified by interval timing paradigms that require participants to estimate or produce an interval of several seconds and require working memory for temporal rules as well as attention to time. Timing performance can be quantified by a variety of measures; however, two relatively universal metrics include: 1) temporal accuracy, defined as the mean temporal estimate and 2) temporal precision, reflected by the variability of temporal estimates. We examined temporal accuracy and precision in a meta-analysis of 14 studies in patients with Parkinson’s disease and 10 studies in patients with Alzheimer’s disease. Strikingly, in both diseases, temporal precision was reliably impaired across studies, while temporal accuracy was not. Our…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
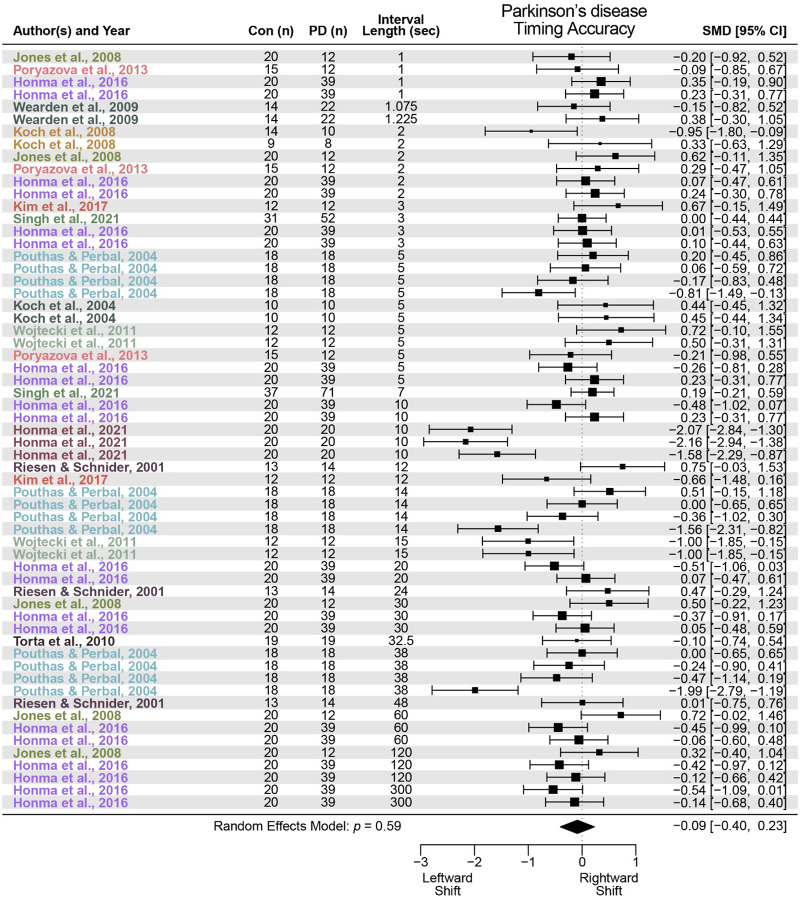 Figure 1
Figure 1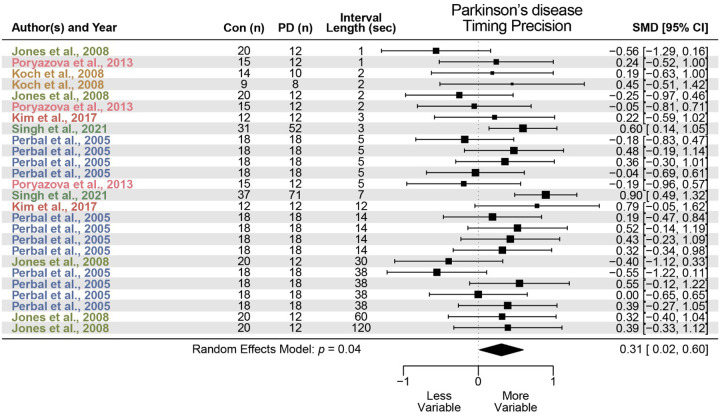 Figure 2
Figure 2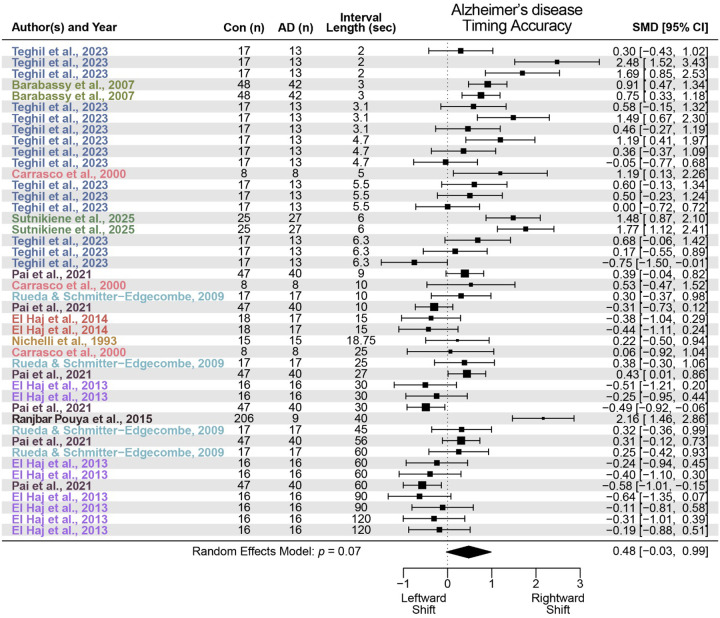 Figure 3
Figure 3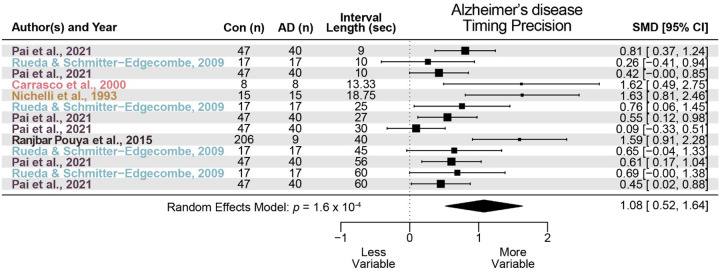 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroscience and Music Perception · Cognitive Functions and Memory · Music Therapy and Health
INTRODUCTION
Interval timing requires participants to estimate a temporal epoch of several seconds by making a motor response and has been studied for more than 150 years (Gibbon, 1977; Gibbon et al., 1984; Staddon, 2005; Vierordt, 1868). While heavily studied in rodent models, human studies suggested that patients with Parkinson’s disease (PD) and Alzheimer’s disease (AD) have impaired interval timing (Nichelli et al., 1993; Pastor et al., 1992). Critically, characterizing timing deficits in PD and AD is important because it could: 1) illuminate neuronal mechanisms in humans (Coull et al., 2011) and how these mechanisms malfunction in neurodegenerative disease; 2) advance translational animal models (Buhusi & Meck, 2005); and 3) add to our existing neuropsychological toolbox.
However, it is unclear how PD and AD affect interval timing, as there have been many competing theories and explanations (Armstrong et al., 2020; Bangert & Balota, 2012; Jones & Jahanshahi, 2014; Meck, 2005; Merchant & De Lafuente, 2014; Q. Zhang et al., 2021). Both diseases have motor features, including slow movements observed in PD (Berardelli et al., 2001) and inaccurate movements observed in AD (Ghilardi et al., 1999). Furthermore, both diseases have marked cognitive deficits that affect executive functions such as working memory and attention (Kensinger et al., 2003) and in other cognitive features, such as declarative memory in AD (Albert, 1996). In addition, more complex deficits in interval timing have been proposed (Malapani et al., 1998, 2002), and temporal deficits in PD have been highly heterogenous (Merchant et al., 2007). Determining how temporal processing deficits relate to universal and quantified metrics such as precision and accuracy would add consistency to measures of interval timing in patients with neurodegenerative disease.
Accordingly, we conducted a meta-analysis of interval timing in PD and AD. From 207 studies with PD and 116 studies with AD, we could extract data from 14 PD and 10 AD studies comparing suprasecond interval timing between a PD/AD population and matched control participants. To our surprise, we found that both PD patients and AD patients had markedly impaired temporal precision but no reliable difference in temporal accuracy, providing insight into timing deficits in PD and AD.
METHODS
Search strategy and inclusion/exclusion criteria
An electronic search of PubMed was performed to identify peer-reviewed articles that studied interval timing behavior in patients with Parkinson’s disease (PD) or Alzheimer’s disease (AD). We were interested in two key measures of interval timing behavior: 1) timing accuracy – measure of early or late timing and 2) timing precision – measure of timing variability. Three separate searches were conducted for PD using the search terms “Parkinson’s” and “interval timing” or “time perception” or “time estimation”. We utilized PubMed’s Boolean operator “NOT” to exclude published review articles and Species filter to include only “Human” studies. An identical search was conducted for AD. After removing duplicates, a total of 150 peer-reviewed abstracts for PD and 72 peer-reviewed abstracts for AD remained. Identical searches for both PD and AD were also conducted using PsycINFO. A total of 57 abstracts for PD and 44 abstracts for AD were unique to PsycINFO. All abstracts were then independently screened by two authors (MAW and CH). We synthesized data from studies that measured interval timing behavior using estimation, production, or reproduction tasks above 1 second. Inclusion criteria were: 1) peer-reviewed original research that compared healthy control participants against patients; 2) timed intervals greater than or equal to 1 second; and 3) results reported as timed response or difference in seconds (or milliseconds). Importantly, we required the results to indicate directionality – i.e., a left or right shift in timed response and a decrease or increase in variability. Exclusion criteria were: 1) non-original research, case study, or computational modeling; 2) sub-second durations; 3) duration discrimination tasks (i.e., temporal bisection); 4) temporal order judgement tasks; and 5) motor synchronization tasks. This process resulted in 14 peer-reviewed publications for PD (Honma et al., 2016, 2021; Jones et al., 2008; Y.-C. Kim et al., 2017; Koch et al., 2004, 2008; Perbal et al., 2005; Poryazova et al., 2013; Pouthas & Perbal, 2004; Riesen & Schnider, 2001; Singh et al., 2021; Torta et al., 2010; Wearden et al., 2009; Wojtecki et al., 2011) and 10 peer-reviewed publications for AD (Barabassy et al., 2007; Carrasco et al., 2000; El Haj et al., 2013, 2014; Nichelli et al., 1993; Pai et al., 2021; Ranjbar Pouya et al., 2015; Rueda & Schmitter-Edgecombe, 2009; Sutnikiene et al., 2025; Teghil et al., 2023). From each of these studies, we collected article title, authors, publication year, type of interval timing behavior, number of participants, average accuracy and precision value, and standard deviation (or standard error of the mean; SEM). Most studies directly reported means and standard deviations (or SEMs) in the results section or in table form. However, if these values were not directly reported, we used a plot digitizer tool (Rohatgi, 2019; WebPlotDigitizer: Version 4.2, 2020, https://automeris.io) to extract relevant data.
The goal of this meta-analysis was to include as many data points as possible because of the limited number of manuscripts that met inclusion criteria. As such, there are relevant details to note. Pouthas & Perbal (2004) and Perbal et al. (2005) reported the same accuracy data, which was only extracted from Pouthas & Perbal (2004). Variability data was extracted from Perbal et al. (2005). Kim and colleagues (2017) did not report variability data in the manuscript, so data was obtained from N.S.N and is available with this manuscript. Pai and colleagues (2021) report data from prodromal AD participants. Sutnikiene and colleagues (2025) report data from two AD cohorts: 1) participants that met criteria for mild cognitive impairment due to AD and 2) participants that met criteria for mild dementia and probable AD.
Statistics
We used R statistical software (v 4.3.2; R Core Team) and the metafor meta-analysis package for R (Viechtbauer, 2009, 2010) to calculate standardized mean difference (i.e., Cohen’s d effect size) for measures of timing accuracy and timing precision for all studies, meta-regression analyses to determine summary effect sizes, and fixed-effects meta-regression models to determine if either disease has a larger effect on timing precision or accuracy. Importantly, the number of studies reporting the effects of PD or AD on interval timing behavior is limited; thus, we extracted multiple effect sizes when possible, meaning a manuscript may contribute multiple data points from the same participants. Several studies reported multiple interval lengths (10/14 PD; 5/10 AD), different interval timing tasks (6/14 PD; 5/10 AD), or separate cohorts of participants (2/14 PD; 1/10 AD). Finally, effect sizes were adjusted so that a leftward shift in timing or decreased timing variability were reflected by negative values and a rightward shift in timing or increased timing variability were reflected by positive values. Importantly, our meta-analytical approach accounts for multiple effects sizes from the same manuscript or participants by using multivariate/multilevel linear mixed-effects models (rma.mv in R). Our statistical approach was checked by Iowa’s Biostatistics and Epidemiology Research and Design Core, and our code and data are available at https://narayanan.lab.uiowa.edu/article/datasets and https://zenodo.org/records/18272471 (M. Weber et al., 2026)
RESULTS
We identified 14 studies that met criteria for PD. We found that PD did not significantly alter interval timing accuracy, with a standardized mean difference of −0.09 (95% confidence interval (CI) −0.40–0.23, p = 0.59; Fig. 1). However, PD was associated with greater interval timing variability and impaired precision with a standardized mean difference of 0.31 (95% CI 0.02–0.60, p = 0.04; Fig. 2). These data indicate no reliable effect of PD on timing accuracy and a small but reliable effect on timing precision.
We identified 10 studies that met criteria for AD. Similar to PD, we found that AD did not reliably alter interval timing accuracy with a standardized mean difference of 0.48 (95% CI −0.03–0.99, p = 0.07; Fig. 3) but did reliably increase interval timing variability with a standardized mean difference of 1.08 (95% CI 0.52–1.64, p = 1.6 × 10^−4^; Fig. 4). These data indicate a moderate but not statistically significant effect of AD on timing accuracy and a large and reliable effect on timing precision.
Finally, a separate meta-regression model indicated that PD had a larger effect on timing variability compared to timing accuracy that did not reach statistical significance (estimate = 0.21, 95% CI −0.01–0.42, z = 1.88, p = 0.06). However, a meta-regression model indicated that AD had a significantly larger effect on timing variability compared to timing accuracy (estimate = 0.75, 95% CI 0.37–1.13, z = 3.90, p = 9.4 × 10^−5^). Taken together, these data suggest that PD and AD reliably impair temporal precision without affecting temporal accuracy.
DISCUSSION
We conducted a meta-analysis of interval timing deficits in PD and AD. We focused on studies that used intervals greater than or equal to 1 second from which we could extract statistics on temporal accuracy and precision. We found that both PD and AD reliably affected temporal precision, or the variability of temporal estimates, without affecting temporal accuracy, suggesting that PD and AD increase the variability of interval timing.
Our data suggest that PD and AD decrease temporal precision, regardless of the task specifics. Interestingly, this did not depend on the length of the interval, meaning that perturbations in precision were evident even at intervals as short as a second. Prior work by our group showed that PD patients had impaired temporal precision during a 7-second fixed-interval timing task (Singh et al., 2021; M. A. Weber, Sivakumar, Bova, et al., 2025) and that rodents administered amphetamine had impaired temporal variability (M. A. Weber, Sivakumar, Kirkpatrick, et al., 2025). Of note, impaired temporal variability predicted cognitive dysfunction as measured by the Montreal Cognitive Assessment (Dalrymple-Alford et al., 2010; Nasreddine et al., 2005; Singh et al., 2021). However, cognitive function and other patient-specific factors were not uniformly measured across included studies, so we are unable to determine which aspects of PD or AD best predict temporal variability. Future studies will determine how specific neuropsychological metrics and measures of brain activity best account for impaired temporal precision in PD or AD.
PD has been traditionally considered a movement disorder (Berardelli et al., 2001). On reaction-time and other motor-specific tasks, PD patients are often slow, consistent with the more generalized bradykinesia in PD (Evarts et al., 1981; Singh et al., 2023). Further, AD certainly has motor features, such as slowed and inaccurate movements (Ghilardi et al., 1999). However, these features cannot easily explain increased temporal variability, as slow movements would result in decreased temporal accuracy without changes in temporal precision. Rather, there may be deficits in executive processing, such as impaired working memory to maintain temporal rules or inattention to the passage of time, that is degrading temporal precision by increasing temporal variability. Future studies will explicitly measure executive function and link these measures to interval timing accuracy and precision.
PD has been better studied in interval timing, leading to theoretical advances on the nature of timing deficits. These deficits have been heterogenous (Merchant et al., 2007); however both PD and AD are complex diseases with many differences in patient-specific factors within each disease category. Some studies have implicated impulsivity (J. Zhang et al., 2016) or motor or perceptual factors (Jones & Jahanshahi, 2014). Other investigators have implicated basal ganglia mechanisms (Malapani et al., 1998), although both PD and AD involve broad brain networks including cortical and subcortical networks (S. Kim et al., 2022; Parker et al., 2013). Our work is important because despite this complexity, both PD and AD patients have decreased temporal precision in interval timing with no reliable effect on temporal accuracy. This finding is helpful in distilling temporal deficits in PD and AD to a single measurable parameter.
Meta-analyses such as ours are inherently limited. First, we could not include every study because they did not meet our inclusion criteria, lacked a control group, or met exclusion criteria. Second, there were myriad nuances between studies that could not be fully captured in a meta-analysis. Third, PD and AD are diseases with distinct pathological processes. While we hypothesize that impairments in frontal brain structures underlie impairments in temporal precision, future work is needed to rigorously test this idea.
In summary, we find that PD and AD patients have decreased temporal precision without reliable effects on temporal accuracy. Our findings capture disruptions in temporal processing in neurodegenerative disease, which will advance new assays and inspire new investigations into their neural substrates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Albert M. S. (1996). Cognitive and neurobiologic markers of early Alzheimer disease. Proceedings of the National Academy of Sciences of the United States of America, 93(24), 13547–13551. 10.1073/pnas.93.24.135478942970 PMC 33644 · doi ↗ · pubmed ↗
- 2Armstrong P., Pardon M.-C., & Bonardi C. (2020). Timing impairments in early Alzheimer’s disease: Evidence from a mouse model. Behavioral Neuroscience, 134(2), 82–100. 10.1037/bne 000035932175759 · doi ↗ · pubmed ↗
- 3Bangert A. S., & Balota D. A. (2012). Keep Up the Pace: Declines in Simple Repetitive Timing Differentiate Healthy Aging from the Earliest Stages of Alzheimer’s Disease. Journal of the International Neuropsychological Society, 18(6), 1052–1063. 10.1017/S 135561771200086022929329 PMC 3505757 · doi ↗ · pubmed ↗
- 4Barabassy A., Beinhoff U., & Riepe M. W. (2007). Cognitive estimation in mild Alzheimer’s disease. Journal of Neural Transmission (Vienna, Austria: 1996), 114(11), 1479–1484. 10.1007/s 00702-007-0752-217520318 · doi ↗ · pubmed ↗
- 5Berardelli A., Rothwell J. C., Thompson P. D., & Hallett M. (2001). Pathophysiology of bradykinesia in Parkinson’s disease. Brain: A Journal of Neurology, 124(Pt 11), 2131–2146. 10.1093/brain/124.11.213111673316 · doi ↗ · pubmed ↗
- 6Buhusi C. V., & Meck W. H. (2005). What makes us tick? Functional and neural mechanisms of interval timing. Nature Reviews Neuroscience, 6(10), 755–765. 10.1038/nrn 176416163383 · doi ↗ · pubmed ↗
- 7Carrasco M. C., Guillem M. J., & Redolat R. (2000). Estimation of short temporal intervals in Alzheimer’s disease. Experimental Aging Research, 26(2), 139–151. 10.1080/03610730024360510755220 · doi ↗ · pubmed ↗
- 8Coull J. T., Cheng R.-K., & Meck W. H. (2011). Neuroanatomical and Neurochemical Substrates of Timing. Neuropsychopharmacology, 36(1), 3–25. 10.1038/npp.2010.11320668434 PMC 3055517 · doi ↗ · pubmed ↗