Knowledge, attitudes, and practices of Tougan population towards dengue in Burkina Faso in 2024
Ter Tiero E. Dah, Abdoul S. Moné, Désiré L. Dahourou, Kadari Cissé, Hamidou Savadogo, Nongognan I. Lengane, Zanga D. Ouattara, Abdoulaye Sawadogo, Linda A. Koubi, Isidore T. Traore, Samiratou Ouedraogo, Jocelyne Gare, Abdoulaye H. Diallo, Smaïla Ouedraogo, Blahima Konate

TL;DR
This study examines how well people in Tougan, Burkina Faso, understand and respond to dengue, finding that internally displaced populations have lower knowledge.
Contribution
The study identifies factors influencing dengue knowledge in a semi-urban setting, focusing on internally displaced populations.
Findings
Internally displaced populations had significantly lower dengue knowledge compared to residents.
Participants with stagnant water at home had better dengue knowledge.
Good practices towards dengue were associated with higher knowledge scores.
Abstract
Recent dengue outbreaks in Burkina Faso have caused substantial morbidity and mortality among semi-urban and urban populations. To assess the knowledge, attitudes, and practices (KAP) among the population of Tougan, a semi-urban city, towards dengue. Between April 2024 and July 2024, a cross-sectional study was performed among residents and internally displaced populations (IDPs) in Tougan. Participants aged 18 years and older, recruited through an adapted three-stage random sampling were eligible. Sociodemographic data as well as information on knowledge, attitudes, and practices (KAP) were collected using a questionnaire. Factors associated with good knowledge of dengue (i.e. knowledge score ≥ 11) were identified using logistic regression models. A total of 419 participants, including 130 (31.1%) IDPs, were enrolled in the study. The majority were male (53.9%), with a mean age of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
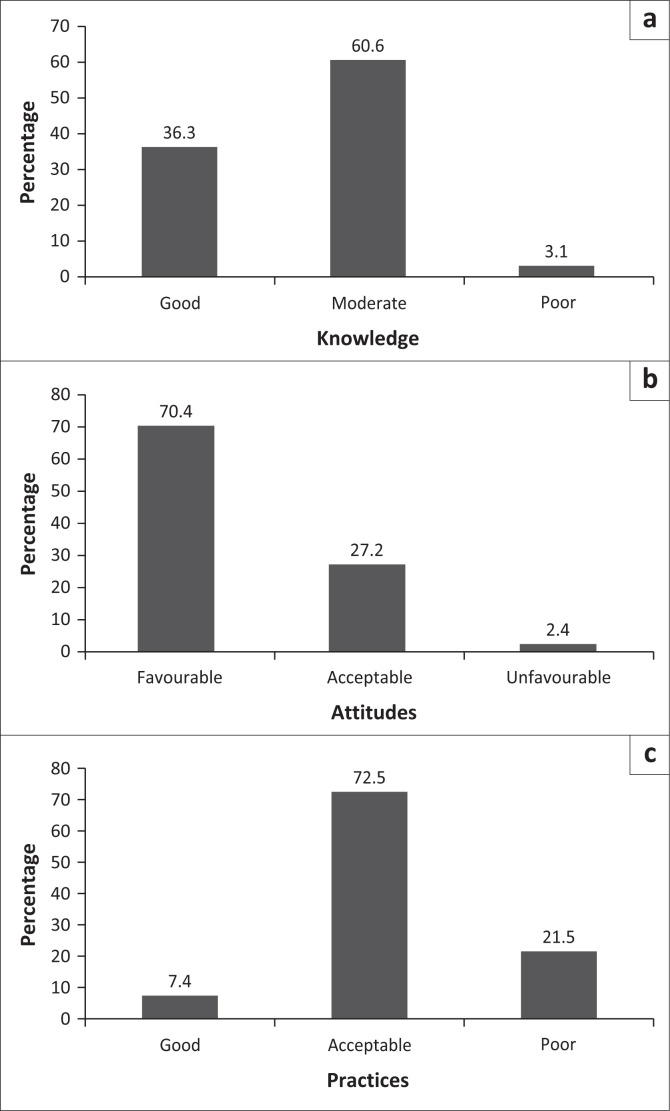 FIGURE 1
FIGURE 1| Variables | All participants ( | Residents ( | IDPs ( | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
| % | mean | s.d. |
| % | mean | s.d. |
| % | mean | s.d. | ||
|
| - | - | 38.5 | 12.9 | - | - | 39.3 | 12.5 | - | - | 36.8 | 12.9 | - |
| 18–24 | 46 | 11 | - | - | 22 | 7.6 | - | - | 24 | 18.5 | - | - | < 0.001 |
| 25–59 | 326 | 77.8 | - | - | 230 | 79.6 | - | - | 96 | 73.8 | - | - | 0.002 |
| ≥ 60 | 47 | 11.2 | - | - | 37 | 12.8 | - | - | 10 | 7.7. | - | - | - |
|
| |||||||||||||
| Male | 226 | 53.9 | - | - | 148 | 51.2 | - | - | 78 | 60 | - | - | 0.095 |
| Female | 193 | 46.1 | - | - | 141 | 48.8 | - | - | 52 | 40 | - | - | - |
|
| |||||||||||||
| Never attended school | 161 | 38.4 | - | - | 95 | 33 | - | - | 66 | 50.8 | - | - | 0.002 |
| Primary | 128 | 30.5 | - | - | 97 | 33.5 | - | - | 31 | 23.8 | - | - | - |
| Secondary | 130 | 31.1 | - | - | 97 | 33.5 | - | - | 33 | 25.4 | - | - | - |
|
| |||||||||||||
| Married or free union | 264 | 63.1 | - | - | 178 | 61.6 | - | - | 86 | 66.2 | - | - | 0.371 |
| Single | 155 | 36.9 | - | - | 111 | 38.4 | - | - | 44 | 33.8 | - | - | - |
|
| |||||||||||||
| Government employee | 25 | 6 | - | - | 25 | 8.7 | - | - | - | - | - | - | 0.001 |
| Liberal | 78 | 18.6 | - | - | 57 | 19.7 | - | - | 21 | 16.2 | - | - | - |
| Unemployed | 316 | 75.4 | - | - | 207 | 71.6 | - | - | 109 | 83.8 | - | - | - |
|
| |||||||||||||
| 1–5 | 152 | 36.3 | - | - | 111 | 38.4 | - | - | 41 | 31.5 | - | - | 0.389 |
| 6–10 | 223 | 53.2 | - | - | 148 | 51.2 | - | - | 75 | 57.7 | - | - | - |
| ≥ 10 | 44 | 10.5 | - | - | 30 | 10.4 | - | - | 14 | 10.8 | - | - | - |
|
| |||||||||||||
| Yes | 269 | 64.2 | - | - | 196 | 67.8 | - | - | 73 | 56.2 | - | - | 0.021 |
| No | 150 | 35.8 | - | - | 93 | 32.2 | - | - | 57 | 43.8 | - | - | - |
|
| |||||||||||||
| Yes | 278 | 66.4 | - | - | 158 | 54.7 | - | - | 120 | 92.3 | - | - | < 0.001 |
| No | 141 | 33.6 | - | - | 131 | 45.3 | - | - | 10 | 7.7 | - | - | - |
| Questions | All participants ( | Residents ( | IDPs ( | ||||
|---|---|---|---|---|---|---|---|
|
| % |
| % |
| % | ||
|
| |||||||
| Yes | 209 | 49.9 | 112 | 38.8 | 97 | 74.6 | < 0.001 |
| No | 210 | 50.1 | 177 | 61.2 | 33 | 25.4 | - |
|
| |||||||
| Yes | 327 | 78.1 | 208 | 71.9 | 119 | 91.5 | < 0.001 |
| No | 92 | 21.9 | 81 | 28.1 | 11 | 8.5 | - |
|
| |||||||
| Yes | 407 | 97.2 | 277 | 95.8 | 130 | 100 | 0.07 |
| No | 12 | 2.8 | 12 | 4.2 | 0 | - | - |
|
| |||||||
| Yes | 392 | 93.6 | 262 | 90.6 | 130 | 100 | < 0.001 |
| No | 27 | 6.4 | 27 | 9.4 | 0 | - | - |
|
| |||||||
| Yes | 415 | 99 | 289 | 100 | 126 | 96.9 | 0.135 |
| No | 4 | 10 | 0 | - | 4 | 3.1 | - |
|
| |||||||
| Yes | 419 | 100 | 289 | 100 | 130 | 100 | - |
| No | 0 | - | 0 | - | 0 | - | - |
|
| |||||||
| Yes | 310 | 74 | 195 | 67.6 | 115 | 88.4 | < 0.001 |
| No | 109 | 26 | 94 | 32.4 | 15 | 11.6 | - |
|
| |||||||
| Yes | 387 | 92.4 | 270 | 93.4 | 117 | 90 | < 0.001 |
| No | 32 | 7.6 | 19 | 6.6 | 13 | 10 | - |
|
| |||||||
| Yes | 349 | 83.3 | 237 | 82.1 | 112 | 86.2 | < 0.001 |
| No | 70 | 16.7 | 52 | 17.9 | 18 | 13.8 | - |
|
| |||||||
| Yes | 343 | 81.9 | 232 | 80.2 | 111 | 85.4 | 0.027 |
| No | 76 | 18.1 | 57 | 19.8 | 18 | 13.8 | - |
|
| |||||||
| Yes | 108 | 25.8 | 99 | 34.3 | 9 | 6.9 | < 0.001 |
| No | 311 | 74.2 | 190 | 65.7 | 121 | 93.1 | - |
|
| |||||||
| Oui | 414 | 98.8 | 288 | 99.6 | 126 | 96.9 | 0.075 |
| Non- | 4 | 1.2 | 1 | 0.4 | 4 | 3.1 | - |
|
| |||||||
| Oui | 419 | 100 | 289 | 100 | 130 | 100 | 0.574 |
| Non | 0 | - | 0 | - | 0 | - | - |
| Variables | Good knowledge | Bad knowledge | Crude | Adjusted | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| % |
| % | OR | 95% CI | OR | 95% CI | |||
|
| ||||||||||
| IDPs | 37 | 28.5 | 93 | 71.5 | 0.6 | 0.38–0.94 | 0.026 | 0.49 | 0.29–0.81 | 0.006 |
| Resident | 115 | 39.8 | 174 | 60.2 | 1 | - | - | - | - | - |
|
| ||||||||||
| 18–24 | 13 | 28.3 | 33 | 71.7 | 1 | - | - | - | - | - |
| 25–59 | 119 | 36.5 | 207 | 63.5 | 1.45 | 0.73–2.88 | 0.276 | - | - | - |
| ≥ 60 | 20 | 42.5 | 27 | 57.5 | 1.88 | 0.79–4.46 | 0.152 | - | - | - |
|
| ||||||||||
| Male | 87 | 38.5 | 139 | 61.5 | 1.23 | 0.82–1.84 | 0.307 | - | - | - |
| Female | 65 | 33.7 | 128 | 66.3 | 1 | - | - | - | - | - |
|
| ||||||||||
| Never attended school | 61 | 37.9 | 100 | 62.1 | 1 | - | - | - | - | - |
| Primary | 49 | 38.3 | 79 | 61.7 | 1.01 | 0.63–1.63 | 0.946 | - | - | - |
| Secondary | 42 | 32.3 | 88 | 67.7 | 0.78 | 0.48–1.27 | 0.323 | - | - | - |
|
| ||||||||||
| Célibataire | 59 | 38.1 | 96 | 61.9 | 1 | - | - | - | - | - |
| Married or in a couple | 93 | 35.2 | 171 | 64.8 | 0.88 | 0.58–1.33 | 0.56 | - | - | - |
|
| ||||||||||
| Government employed | 1 | 40 | 15 | 60 | 1 | - | - | - | - | - |
| Liberal | 28 | 35.9 | 50 | 64.1 | 0.84 | 0.33–2.11 | 0.712 | - | - | - |
| Unemployed | 114 | 36.1 | 202 | 63.9 | 0.84 | 0.36–1.94 | 0.695 | - | - | - |
|
| ||||||||||
| Yes | 101 | 37.5 | 168 | 62.5 | 1.16 | 0.76–1.77 | 0.469 | - | - | - |
| No | 51 | 34 | 99 | 66 | 1 | - | - | - | - | - |
|
| ||||||||||
| 1–5 | 58 | 38.2 | 94 | 61.8 | 1 | - | - | - | - | - |
| 6–10 | 77 | 34.5 | 146 | 65.5 | 0.85 | 0.55–1.31 | 0.472 | - | - | - |
| ≥ 10 | 17 | 38.6 | 27 | 61.4 | 1.02 | 0.51–2.03 | 0.954 | - | - | - |
|
| ||||||||||
| Yes | 116 | 41.7 | 162 | 58.3 | 2.08 | 1.33–3.26 | 0.001 | 3.03 | 1.84–4.96 | < 0.001 |
| No | 41 | 29.1 | 100 | 70.9 | 1 | - | - | - | - | - |
|
| ||||||||||
| Good | 18 | 58.1 | 13 | 41.9 | 3.67 | 1.55–8.67 | 0.003 | 3.39 | 1.37–8.38 | 0.008 |
| Acceptable | 111 | 36.5 | 193 | 63.5 | 1.52 | 0.89–2.60 | 0.121 | - | - | - |
| Poor | 23 | 27.4 | 61 | 72.6 | 1 | - | - | - | - | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMosquito-borne diseases and control · Viral Infections and Outbreaks Research · Dengue and Mosquito Control Research
Introduction
Dengue is a viral infection transmitted to humans through the bite of mosquitoes (Aedes aegypti or Aedes albopictus).^1,2,3^ When it is symptomatic, the main manifestations are fever, headaches, joint pain, nausea, and vomiting. Dengue is a major public health concern, particularly in tropical and subtropical regions where it re-emerges and occurs throughout endemic and epidemic episodes.^4^ During the past two decades, the spread of dengue has been driven by climate change, human migration, and uncontrolled urbanisation.^5^ In 2024, the World Health Organization (WHO) estimated more than 7.5 million cases of dengue worldwide, resulting in more than 10 000 deaths.^6^ These figures are increasing, from 505 430 cases in 2000 to 5.2 million in 2019, as well as an excess mortality rate of 65% between 2000 and 2017.^4,5^
The West Africa region is among the most affected by dengue. The number of confirmed cases evolved from 14 000 in 2014 to 70 000 in 2023, and Burkina Faso accounted for 85% of all reported cases and 90% of all deaths.^7^ The first cases of dengue in this country were documented in 1925.^8,9^ Since then, the country has officially declared outbreaks in 2006, 2016, and 2023.^10,11^ By the end of the 33rd week of 2023, Burkina Faso had recorded 79 867 suspected cases, 34 687 probable cases, and 349 deaths.^12^ The outbreak mainly affected the two largest cities (Ouagadougou and Bobo-Dioulasso) and other secondary ones. It resulted in high number of hospitalisations, overcrowding in emergency and inpatient services, and disruptions in healthcare provision. In addition, cases of self-medication with herbal remedies among hospitalised patients and nephrological complications such as tubular necrosis were documented.^13,14^
Similar to other vector-borne diseases, the control of dengue is influenced by structural factors, including the organisation of curative and preventive care, environmental factors (such as sanitation), and individual factors (such as the use of repellents and bed nets).^15,16^ In Burkina Faso, the healthcare context has been exacerbated since 2015 by a security crisis, which has led to the displacement of populations from rural to urban and semi-urban areas. Internally displaced populations (IDPs) are particularly vulnerable to health issues, including dengue.^17^ However, only a few studies conducted in Burkina Faso have examined individual factors contributing to the dengue burden, particularly among these vulnerable populations. Specific information on populations’ knowledge, attitudes, and practices (KAP) regarding dengue is essential to better organise the national response, particularly for guiding awareness and prevention messages. We hypothesise that IDPs compared to resident populations have poorer knowledge, less favourable attitudes, and worse practices regarding dengue.
This study aims to assess the knowledge, attitudes, and practices regarding dengue in resident populations and in IDPs settled in Tougan, and to identify factors associated with good knowledge of dengue in 2024.
Research methods and design
Study design and setting
We conducted a cross-sectional study between April 2024 and July 2024 in Tougan, a semi-urban city in northwestern Burkina Faso, bordering Mali. Tougan is part of the Boucle du Mouhoun region and had a population of 26 347 in 2022.^18^ In March 2023, the ‘Secrétariat Permanent du Conseil National des Secours d’Urgence et de Réhabilitation’ reported a total of 134 000 IDPs as a result of insecurity in the Boucle du Mouhoun.^19^ During the study period, Tougan comprised seven sectors (or neighbourhoods) and four IDP camps.
Study population and sampling
The study population was composed of resident and displaced individuals aged 18 years or older, present at the time of the study, and consented to participate. Participants were selected using an adapted three-stage random sampling method. Firstly, three sectors and two IDP camps were randomly chosen. Secondly, households were randomly selected. Thirdly, within each household, an eligible individual, usually the head of the household, was chosen to respond to the questionnaire.^20^ Choosing the head of household is mainly related to norms around decision-making in this context.
A minimum sample size was calculated using Schwartz’s formula.^21^ We assumed a previously documented knowledge proportion of 50% and a first-type error risk (α) of 5%. Accounting for a potential 10% refusal rate, the required sample size was 419 individuals.
Data collection and study variables
Data were collected using a face-to-face questionnaire administered by trained interviewers. The questionnaire was based on the literature review and included sociodemographic information, as well as knowledge, attitudes, and practices regarding dengue. Knowledge was assessed through 13 questions allowing mutually exclusive answers: ‘yes’, ‘no’, or ‘don’t know’. Correct answers were assigned a score of 1, while incorrect answers were scored 0. The total knowledge score ranged from 0 to 13. Knowledge was classified as poor (score ≤ 7), moderate (score 8–10) or good (score ≥ 11). Attitudes were assessed using eight questions with response options ‘yes’, ‘indifferent’, or ‘no’, scored as 2, 1, and 0, respectively. The total attitude score ranged from 0 to 16 and was classified as unfavourable (≤ 8), acceptable (9–13), or favourable (≥ 14). Practices were assessed using seven questions with response options ‘always’, ‘sometimes’, and ‘never’, scored as 2, 1, and 0, respectively. The total practice score ranged from 0 to 14 and was classified as poor (≤ 7), acceptable (8–10), or good (≥ 11).
Statistical analysis
Firstly, we described the characteristics of the study participants. Quantitative variables were summarised using means and standard deviations (s.d.), while categorical variables were presented as absolute (counts) and relative (percentages) frequencies. Secondly, we described knowledge, attitudes, and practices regarding dengue and compared them between resident and IDPs using Pearson’s Chi-square test or Fisher’s exact test when appropriate. Thirdly, we identified factors associated with good knowledge of dengue (score ≥ 11) using a logistic regression. Variables associated with good knowledge of dengue with a p-value ≤ 0.20 were specified in the complete multivariate model. A manual backward elimination based on the log-likelihood method was used to determine the final multivariate model.
For all calculations, statistical significance was defined with a p-value ≤ 0.05. The goodness of fit of the retained model was assessed using the Hosmer and Lemeshow test. All analyses were performed using STATA software (version 16; Stata Corp LP, College Station, Texas, United States).
Ethical considerations
Ethical clearance to conduct this study was obtained from the Ministry of Health and Public Hygiene, Ministry of Higher Education, Research and Innovation Health Research Committee (Comité d’Ethique pour la Recherche en Santé [CERS] No. 2024-04-119). All participants provided written informed consent. Illiterate participants benefited from the information note translation in their mother tongue by a person that they choose. Anonymity as well as confidentiality were respected during all the study steps (data collection, analysis, and diffusion).
Results
Characteristics of the study participants
A total of 419 participants, including 226 (53.9%) men, were included in the study. Their mean age was 38.5 years (s.d.: 12.9 years). A total of 289 (68.9%) participants were residents, while 130 (31.1%) were IDPs. Slightly more than two-thirds of the population (n = 289, 68.9%) had an education level below secondary school. Two-thirds of the participants (n = 269, 64.2%) engaged in domestic animal husbandry. The characteristics of the participants are presented in Table 1.
Knowledge of dengue
The mean dengue knowledge score was 10.1 (s.d.: 1.2) out of 13. Approximately one-third of the participants (n = 152/419, 36.3%) had good knowledge, more than half (n = 254/419, 60.6%) had moderate knowledge, and 13 out of 419 (3.1%) had poor knowledge (Figure 1). Half of the participants (49.9%) believed that there was no difference between malaria and dengue. Specifically, IDPs confused the two diseases more than resident populations (74.6% vs. 38.6%, p < 0.001). Overall knowledge of dengue symptoms and prevention methods was 98.8% and 100%, respectively. These figures did not differ significantly according to population type (99.6% vs. 96.9%, p = 0.075, and 100% vs. 100%, p = 0.574, respectively). Details of responses to the knowledge-related questions are presented in Table 2.
Overall knowledge (a), attitudes (b), and practices (c) of Tougan population towards dengue in 2024 (N = 419).
Attitudes towards dengue
The mean attitude score towards dengue was 13.5 (s.d.: 1.9) out of 16. A total of 295 participants (70.4%) had favourable attitudes, 114 (27.2%) had acceptable attitudes, and 10 (2.4%) had unfavourable attitudes (Figure 1). Attitudes towards dengue were significantly more favourable in IDPs than in resident populations (85.4% vs. 63.7%, p < 0.001). Details of responses to the attitudes related questions are presented in Appendix 1 – Table 1-A1.
Practices regarding dengue
The mean dengue practice score was 9.4 (s.d.: 2.2) out of 14. Very few participants (n = 31, 7.4%) had good dengue-related practices, 304 (72.6%) had moderate practices, and 84 (20.1%) had poor practices (Figure 1). Good practices with regard to dengue were significantly higher in resident populations than in IDPs (9.3% vs. 3.1%, p < 0.001). Details of responses to the practices related questions are presented in Appendix 1 – Table 2-A1.
Factors associated with good knowledge of dengue
The level of knowledge in IDPs was significantly lower than that in residents (adjusted odds ratio [aOR]: 0.49, 95% confidence interval [CI]: 0.29–0.81, p = 0.006) (Table 3). Participants who reported stagnant water in their homes had a higher level of knowledge (aOR: 3.03, 95% CI: 1.84–4.96, p < 0.001) than those who did not. Participants who reported good practices towards dengue also had better knowledge (aOR: 3.39, 95% CI: 1.37–8.38, p = 0.008) compared to those who did not.
Discussion
Our study highlighted a low level of knowledge of dengue in the population of Tougan, acceptable attitudes, and poor practices. The IDPs had lower knowledge and poorer practices than resident populations. However, they had better attitudes.
Knowledge, attitudes and practices towards dengue
Although IDPs had lower levels of knowledge than residents, it is noteworthy that overall knowledge remained low. Our findings are consistent with a study conducted in Ouagadougou in 2015, which also found a low level of knowledge of dengue.^22^ This may be partly explained by the fact that dengue is a relatively new public health issue in Burkina Faso and is therefore not widely known, especially in secondary cities such as Tougan. These results highlight the need for educational efforts to enhance dengue-related knowledge among the population of Burkina Faso, particularly in rural and semi-urban areas.
A thorough analysis of the responses to knowledge-related questions revealed three key points requiring focused communication to dispel misconceptions and establish accurate information. The first point is the confusion between malaria and dengue. Half of the respondents believed that there was no difference between these two diseases. This confusion may arise from the similarities in their clinical manifestations (headache, fever, joint and muscle pain) and the fact that both are mosquito-borne illnesses. Moreover, it is important to observe that dengue infection is commonly called as ‘paludengue’ by the Burkina Faso population.
The second point requiring clarification is the availability of dengue treatment. Only 16% of respondents knew that dengue has no specific treatment. This is crucial, as a significant proportion of participants reported using traditional medicine when experiencing dengue-like symptoms. Previous studies in Burkina Faso documented an acute kidney failure rate of 20% among patients hospitalised for severe dengue during the 2016 outbreak.^11^ This complication was partially attributed to self-medication and the use of traditional treatments, often decoctions of roots and other plant parts.
The third point for communication and intervention is the existence of a dengue vaccine and its potential future implementation.^23,24^ In May 2024, the WHO recommended the use of recombinant live-attenuated vaccines (CYD-TVD and TAK-003) for dengue prevention. The implementation of these vaccines in Burkina Faso, particularly among vulnerable populations, could help prevent future outbreaks.
Despite the existence of several knowledge gaps, responses regarding symptoms and prevention methods were largely accurate. This encouraging result may be because of the population’s association of dengue with malaria. Strengthening this knowledge by clearly distinguishing the similarities and differences between these two diseases is essential.
Overall, participants had favourable attitudes towards dengue, with IDPs demonstrating more positive attitudes than resident populations. This is encouraging, as it suggests that the population is willing to take appropriate preventive and management actions. National dengue response efforts should capitalise on this positive dynamic when designing interventions.
However, dengue-related practices remained poor, particularly among IDPs. This result may be explained by the suboptimal knowledge levels. Intuitively, an individual’s practices in a given domain are often determined by their level of knowledge in the same area.^25^ This is the fundamental principle behind behaviour change education. In addition, IDPs often live in challenging social conditions, sometimes lacking proper housing, which may make issues like environmental sanitation a lower priority.
Study’s limitations
Our findings should be interpreted with caution. Firstly, the study was conducted in a single site, the semi-urban town of Tougan, making it difficult to generalise results to other semi-urban areas in Burkina Faso. Secondly, the fact of choosing sometimes the heads of households at the third stage of population selection could result in a potential bias. Thirdly, the data had been collected using an invalid tool (questionnaire). Fourthly, given the face-to-face data collection method, social desirability bias may have influenced some responses, potentially leading to an overestimation of good practices. Fifthly, certain key potential confounders for good knowledge on dengue (e.g. access to health information, duration of displacement) were not collected. Nevertheless, our study is one of the first in these vulnerable populations in Burkina Faso. The findings will help filling an important data gap regarding dengue-related KAPs, designing effective prevention messages, and improving dengue preparedness.
Conclusion
The population of Tougan has insufficient specific knowledge about dengue. Moreover, differences in knowledge, attitudes, and practices were observed between residents and IDPs. There is an urgent need to develop and disseminate context-specific prevention messages and targeted interventions to these populations in semi-urban areas in Burkina Faso.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Paz-Bailey G, Adams LE, Deen J, Anderson KB, Katzelnick LC. Dengue. Lancet. 2024;403(10427):667–682. 10.1016/S 0140-6736(23)02576-X 38280388 PMC 12372472 · doi ↗ · pubmed ↗
- 2Wilder-Smith A, Ooi EE, Horstick O, Wills B. Dengue. Lancet. 2019;393(10169):350–363. 10.1016/S 0140-6736(18)32560-130696575 · doi ↗ · pubmed ↗
- 3World Health Organization. Dengue: Guidelines for diagnosis, treatment, prevention and control. Geneva: World Health Organization; 2009, p. 159.23762963 · pubmed ↗
- 4Zeng Z, Zhan J, Chen L, Chen H, Cheng S. Global, regional, and national dengue burden from 1990 to 2017: A systematic analysis based on the global burden of disease study 2017. e Clinical Medicine. 2021;32:100712. 10.1016/j.eclinm.2020.10071233681736 PMC 7910667 · doi ↗ · pubmed ↗
- 5Power GM, Vaughan AM, Qiao L, et al. Socioeconomic risk markers of arthropod-borne virus (arbovirus) infections: A systematic literature review and meta-analysis. BMJ Glob Health. 2022;7(4):e 007735. 10.1136/bmjgh-2021-007735 PMC 901403535428678 · doi ↗ · pubmed ↗
- 6Global dengue surveillance [homepage on the Internet]. 2024 [cited 2025 Feb 12]. Available from: https://worldhealthorg.shinyapps.io/dengue_global/
- 7Dengue in the WHO African Region: Situation report 01: 19 December 2023 [homepage on the Internet]. WHO | Regional Office for Africa. 2023 [cited 2025 Feb 12]. Available from: https://www.afro.who.int/countries/burkina-faso/publication/dengue-who-african-region-situation-report-01-19-december-2023
- 8Lim JK, Seydou Y, Carabali M, et al. Clinical and epidemiologic characteristics associated with dengue during and outside the 2016 outbreak identified in health facility-based surveillance in Ouagadougou, Burkina Faso. PLOS Negl Trop Dis. 2019;13(12):e 0007882. 10.1371/journal.pntd.000788231809504 PMC 6897397 · doi ↗ · pubmed ↗