Artemisinin resistance threat in Central and West Africa needs holistic action
Loick Pradel Kojom Foko, Amit Sharma

TL;DR
Artemisinin resistance is spreading in Central and West Africa, requiring urgent and comprehensive action to prevent public health and economic impacts.
Contribution
The paper highlights the growing threat of artemisinin resistance in Central and West Africa and proposes strategies for surveillance and mitigation.
Findings
Artemisinin resistance is emerging in Central and West Africa, linked to mutations in the Plasmodium falciparum kelch13 gene.
Funding cuts and armed conflicts threaten malaria control efforts in the region.
Near real-time surveillance systems are proposed to enhance data use and guide tailored control strategies.
Abstract
Artemisinin partial resistance (ART-R) has now emerged in the Horn, Eastern and Southern Africa. Mutations in the Plasmodium falciparum kelch13 gene, strongly associated with ART-R, are increasingly reported in several Central and West Africa countries. Here, we opine that the emergence and spread of ART-R in Central and West Africa should not be overlooked given public health, clinical and economic consequences. Again, in addition to the recent funding cuts from the United States (US) government, some regions in these countries are affected by armed conflicts that undoubtedly will disrupt malaria control measures. Thus, measures should be proactively taken to prevent the emergence of ART-R or mitigate its spread in these two regions. We also propose strategies that could be valuable in implementing a near real-time surveillance and information system, will produce high-quality…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
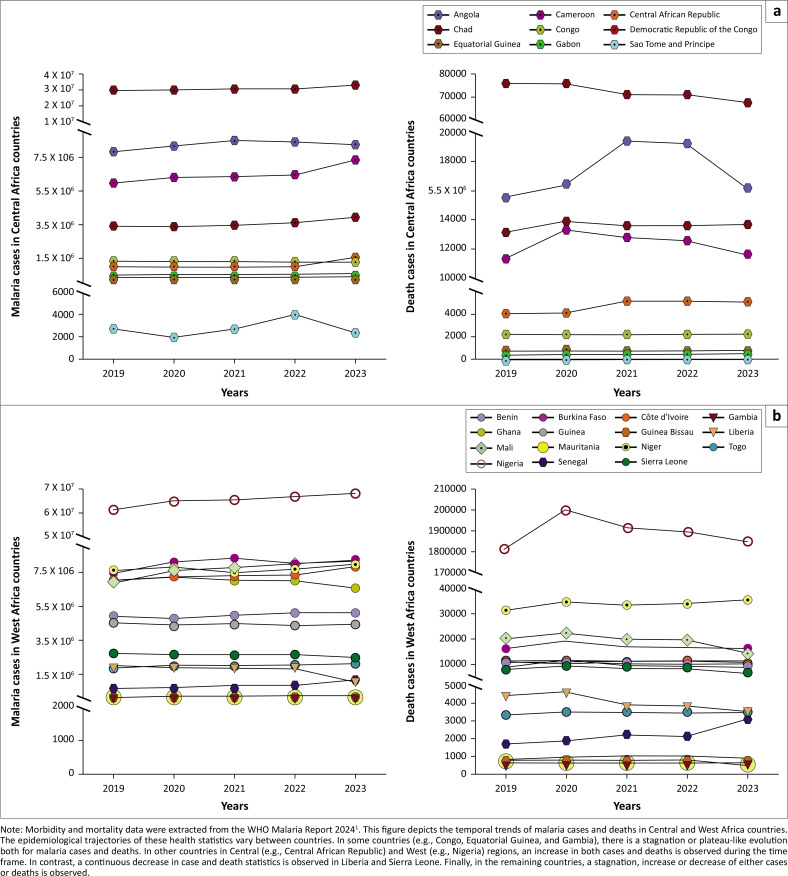 Figure 1
Figure 1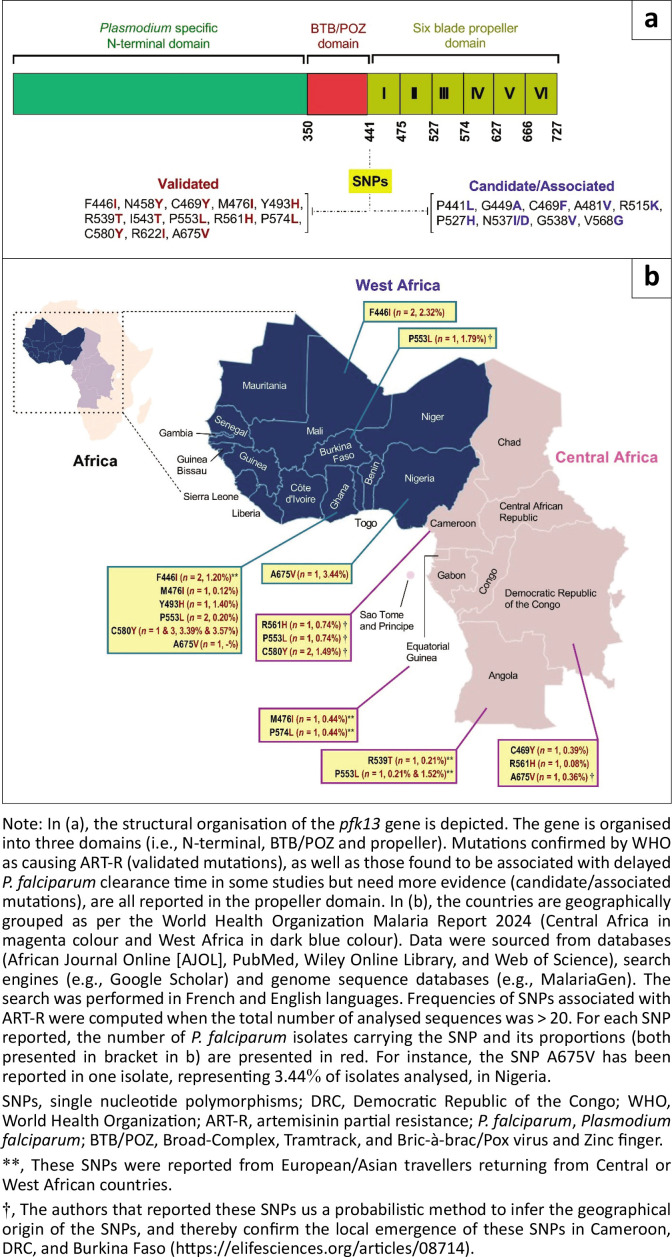 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMalaria Research and Control · Pharmaceutical Quality and Counterfeiting · vaccines and immunoinformatics approaches
The latest report from the World Health Organization (WHO) highlights a rise in the global malaria burden from 219 million cases in 2022 to 263 million in 2023.^1^ The precise cause of this increase remains unclear, but it is probably due to a complex action of several factors such as the emergence or re-emergence of originally zoonotic pathogens (e.g., coronavirus disease 2019 [COVID-19]), climate change, armed conflicts and decline in malaria control efforts. In addition, mosquito insecticide resistance, Anopheles stephensi invasion, low coverage of preventive strategies, the emergence of Plasmodium falciparum parasites escaping histidine-rich protein 2 gene (pfhrp2)-targeting rapid diagnostic tests, and the development of artemisinin partial resistance (ART-R) in Africa have likely all contributed.^1^
Artemisinin-based combination therapies (ACTs) are the backbone of the current therapeutic strategies to treat uncomplicated P. falciparum malaria in Africa, while intravenous artesunate is recommended for severe malaria.^2^ In Central and West African countries, ACTs such as artesunate + amodiaquine, artemether + lumefantrine and now dihydroartemisinin + piperaquine are commonly used against uncomplicated P. falciparum malaria. ART-R is defined as ‘a delay in the clearance of malaria parasites from the bloodstream following treatment with an ACT’ (https://www.who.int/news-room/questions-and-answers/item/artemisinin-resistance). Well-established in the Greater Mekong subregion (GMS), Southeast Asia, ART-R is now being reported in the Horn of Africa.^3^ Signals of ART-R have also been reported in other countries (e.g., Uganda, Rwanda).^1^
Since 2018, WHO proposed a targeted malaria response strategy referred to as ‘High Burden to High Impact (HBHI)’ in endemic countries. Now, the HBHI list is constituted totally by African countries, where there is a need for more aggressive malaria control efforts. Several Central and West African countries belong to HBHI countries (i.e., Nigeria, the Democratic Republic of the Congo [DRC], Niger, Angola, Burkina Faso, Benin, Guinea, Mali, Chad, Cameroon, Ghana and Côte d’Ivoire).^1^ These countries show contrasting epidemiological trajectories for malaria incidence and death cases during the last five years (2019–2023). In some countries in Central (e.g., Central African Republic) and West (e.g., Nigeria, Senegal) regions, an increase in both cases and deaths was observed during the time frame (Figure 1).
Single nucleotide polymorphisms (SNPs) in the propeller domain of the Kelch 13 gene (pfk13) have been identified as major genetic drivers of ART resistance.^3,4^ Single nucleotide polymorphisms (SNPs) in the propeller domain of the Kelch13 gene (pfk13) have been identified as major genetic drivers of ART resistance.^3^ To date, ~20 of these SNPs are either candidate or validated markers of ART resistance based on their strong in vivo and/orin vitro associations with delayed P. falciparum clearance (Figure 2).^5^ Some of these validated mutations, such as R539T and R561H are prevalent in Africa.^3^ Also, some studies outlined the role of P. falciparum genetic background and non-pfk13 genes (e.g., coronin, or ferredoxin) in the acquisition of ART-R phenotype.^6^ Given the logistic, technical, financial and methodological challenges of clinical trials, typing of drug resistance pfk13 SNPs is more frequently performed for ART-R resistance surveillance and research purposes. The scalability of next-generation sequencing (NGS) tools, such as Oxford Nanopore sequencing, allows for continuous, rapid and timely evaluation of drug resistance profiles.^7^
Artemisinin partial resistance could pose a significant threat to malaria control efforts in Africa, particularly in Central and West regions of the continent. These two regions have so far remained unaffected by ART-R confirmation but are highly vulnerable because of high transmission rates and a substantial malaria burden (Figure 1). Recent cuts to infectious disease funding by the United States (US) government, particularly reductions in support from the President’s Malaria Initiative,^8^ are compounding these risks. These funding shortfalls could delay the procurement and distribution of ACTs, lead to interruptions in control interventions (e.g., long-lasting insecticide-treated nets, indoor residual spraying). This result in the scaling back of molecular surveillance programmes critical to the early detection of ART-R. Without adequate financial and technical support, health systems in these regions may struggle to detect and contain ART-R effectively, increasing the likelihood of its spread. Furthermore, funding cuts will hamper fight against malaria and could lead to dire outcomes in terms of public health and economic aspects.
Molecular signals arose from the eastern DRC (Central Africa) where ART-R pfk13 mutant strains (R561H, P441L) were reported.^9^ Artemisinin partial resistance-related mutations have been reported at marginal rates in other countries (e.g., A675V [n = 1 isolate, 3.44%] in Nigeria, A675V [n = 1 isolate, 2.32%] in Mali, A675V [n = 1 isolate, 1.79%] in Burkina Faso, R561H [n = 1 isolate, 0.74%], P553L [n = 1 isolate, 0.74%] and C580Y [n = 2 isolates, 1.49%] in Cameroon) (Figure 2). Even though not adequately designed, a study reported reduced artemether + lumefantrine efficacy (i.e., treatment failure rates > 20%) in Gourcy and Nanoro, two cities in Burkina Faso where malaria transmission is stable and seasonal.^10^ However, these ACT efficacy data need further work in Central and West Africa countries. It should be noticed that Kelch13 mutations and ACT therapeutic efficacy data in these countries are mostly outdated, with P. falciparum isolated collected in 2019 for the most recent studies in these two regions (e.g., Benin, Gabon). Parasite surveillance is either limited or absent in other countries (e.g., Niger). This hence requires implementation of therapeutic efficacy and molecular studies for understanding the current status of ART-R in Central and West Africa countries.
Regions in Africa with armed conflicts will undoubtedly experience disruptions in malaria control measures. Also, areas where above mutants have been reported are geographically close to Rwanda and Uganda, two countries where ART-R is now evidenced.^1^ This suggests a possible transboundary human movement-driven expansion of these resistant strains. The world has become a veritable ‘planetary village’, and the corollary is an increased risk of globalisation of public health concerns such as ART-R. Other drivers of drug resistance, such as self-medication with antimalarial drugs, widespread use of artemisinin monotherapies, poor prescription practices, substandard and counterfeit drugs and partial ACT adherence, are prevalent in Africa. A recent study in Cameroon showed gaps between knowledge and prescription of ACTs among health caregivers. For instance, only 6.2% of patients receiving artemether + lumefantrine at the correct posology.^11^ In Ivory Coast, N’guessan et al. found that 26% and 7% of artemether + lumefantrine-containing drugs were underdosed and overdosed, respectively.^12^ In Nigeria, a study reported that artemisinin monotherapies were still available in the private market at rates of ~9.2% – 13.3% for artesunate and 9.5% for dihydroartemisinin.^13^ Thus, the risk of the de novo emergence, spread or importation of ART-R to Central and West Africa is high.^4^
Nonetheless, there are reasons for guarded optimism:
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO. World Malaria report 2024 [homepage on the Internet]. 2024 [cited 2025 April 30]. Available from: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2024
- 2WHO. Guidelines for the treatment of Malaria. 3rd ed. 2015 [cited 2025 April 30]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 294440/pdf/Bookshelf_NBK 294440.pdf
- 3White N, Chotivanich K. Artemisinin-resistant malaria. Clin Microbiol Rev. 2024;37(4):e 0010924. 10.1128/cmr.00109-2439404268 PMC 11629630 · doi ↗ · pubmed ↗
- 4Nsanzabana C. Resistance to artemisinin combination therapies (AC Ts): Do not forget the partner drug!. Trop Med Infect Dis. 2019;4(1):26. 10.3390/tropicalmed 401002630717149 PMC 6473515 · doi ↗ · pubmed ↗
- 5WWARN Genotype-Phenotype Study Group. Association of mutations in the Plasmodium falciparum Kelch 13 gene (Pf 3D 7_1343700) with parasite clearance rates after artemisinin-based treatments-a WWARN individual patient data meta-analysis. BMC Med. 2019;17:1. 10.1186/s 12916-018-1207-330651111 PMC 6335805 · doi ↗ · pubmed ↗
- 6Rosenthal MR, Ng CL. Plasmodium falciparum artemisinin resistance: The effect of heme, protein damage, and parasite cell stress response. ACS Infect Dis. 2020;6(7):1599–1614. 10.1021/acsinfecdis.9b 0052732324369 PMC 8528195 · doi ↗ · pubmed ↗
- 7Holzschuh A, Lerch A, Fakih BS, et al. Using a mobile nanopore sequencing lab for end-to-end genomic surveillance of Plasmodium falciparum: A feasibility study. PLOS Glob Public Health. 2024;4(2):e 0002743. 10.1371/journal.pgph.000274338300956 PMC 10833559 · doi ↗ · pubmed ↗
- 8Bockarie MJ, De Souza DK, Ansumana R, et al. The changing funding landscape for infectious disease research and control: Implications for resource-limited countries. Int J Infect Dis. 2025;154:107868. 10.1016/j.ijid.2025.10786840032134 · doi ↗ · pubmed ↗