Pulmonary Veno-Occlusive Disease: A Clue to Underlying Lymphoma
Chaynez Rachid, Othman Abouobayd, Mohamed Ijim, Hind Rachidi, Hanane Rais, Oussama Fikri, Lamyae Amro

TL;DR
A rare lung disease called PVOD can be a sign of hidden lymphoma, requiring careful diagnosis to avoid dangerous treatments.
Contribution
This case highlights PVOD as a potential indicator of underlying lymphoma, emphasizing the need for thorough evaluation.
Findings
PVOD can present as a secondary phenomenon due to Hodgkin's lymphoma.
Radiological features of PVOD with lymphadenopathy necessitate a thorough workup for malignancy.
Standard pulmonary vasodilators may be fatal in malignancy-associated PVOD.
Abstract
Pulmonary veno-occlusive disease (PVOD) is a rare cause of post-capillary pulmonary hypertension. Unlike the more common pulmonary arterial hypertension (PAH), PVOD specifically involves the small pulmonary veins. While often idiopathic or genetic, PVOD can occasionally be the presenting symptom of an occult malignancy, such as lymphoma, through direct venous infiltration or extrinsic compression. We report the case of a 31-year-old patient who presented with progressive dyspnea, non-productive cough, and signs of right-sided heart failure. Initial thoracic computed tomography (CT) imaging showed characteristic signs of PVOD: diffuse ground-glass opacities, thickened interlobular septa, and mediastinal lymphadenopathy. Although right heart catheterization was indicated to confirm pre-capillary pulmonary hypertension, it could not be carried out because of the patient’s clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3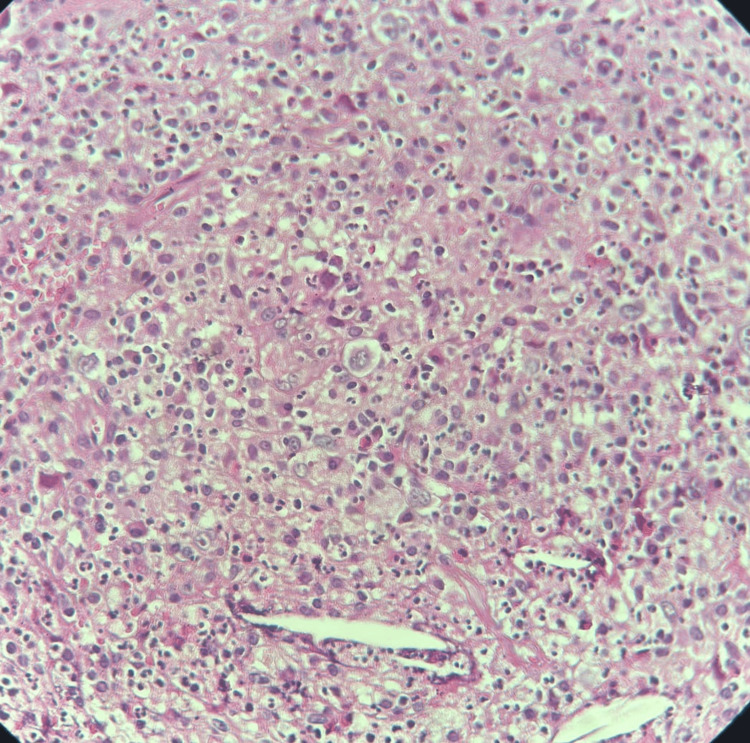 Figure 4
Figure 4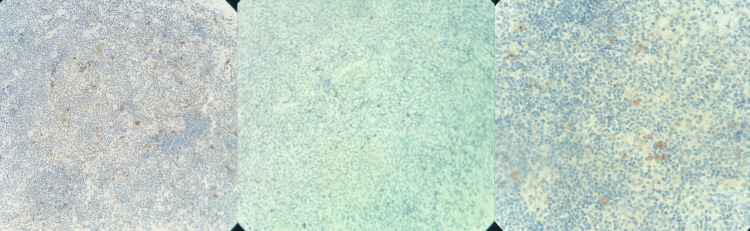 Figure 5
Figure 5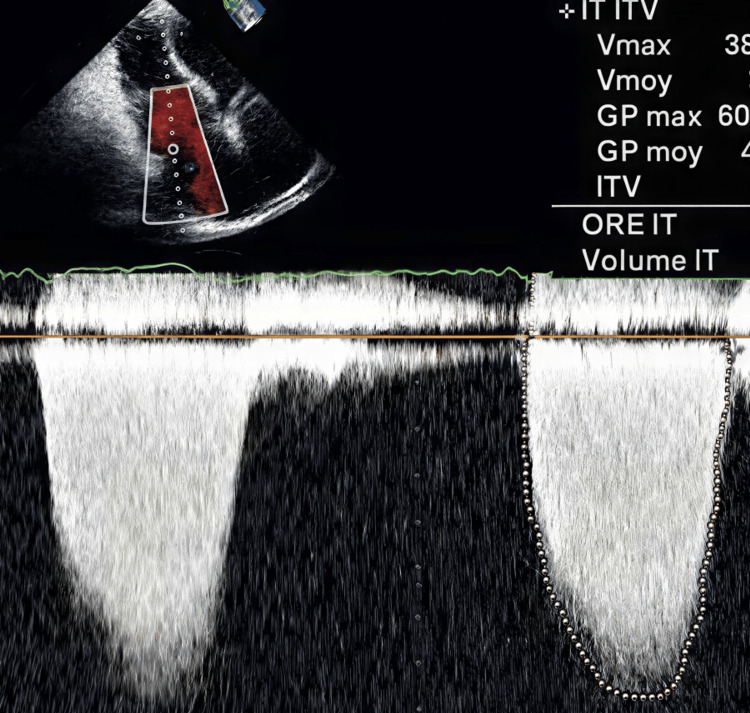 Figure 6
Figure 6| Parameters | Patient values | Reference range |
| Serum calcium | 100.21 mg/L | 85–105 mg/L |
| Urinary calcium | 269 mg/24 h | 100–300 mg/24 h |
| Serum phosphate | 46 mg/L | 25–45 mg/L |
| Urinary phosphate | 2029 mg/24 h | 400–1300 mg/24 h |
| Corrected serum calcium | 2.1 mmol/L | 2.20 à 2.60 mmol/L |
| Parameters | Patient values | Reference range |
| PH | 7.46 | 7.35–7.45 |
| PaO2 | 32.2 mmHg | 80-100 mmHg |
| PcO2 | 33.8 mmHg | 35–45 mmHg |
| HCO3- | 24.9 mmol/L | 22–26 mmol/L |
| S02 | 76% | 95%–100% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPulmonary Hypertension Research and Treatments · Cardiac tumors and thrombi · Vascular Anomalies and Treatments
Introduction
Pulmonary veno-occlusive disease (PVOD) represents a rare and devastating subset of pulmonary arterial hypertension, characterized by the progressive fibrous occlusion of small pulmonary veins and capillaries. While the idiopathic form is frequently linked to EIF2AK4 genetic mutations or toxic exposures, PVOD can also emerge as a secondary phenomenon. Among its most elusive triggers is malignant lymphoma, where the disease serves as the inaugural clinical manifestation of an occult hematological malignancy. The pathophysiology of lymphoma-associated PVOD is complex, often involving direct intravascular infiltration by neoplastic cells or extrinsic compression of the pulmonary venous system by mediastinal lymphadenopathy. This clinical overlap creates a significant diagnostic "trap": the symptoms of progressive dyspnea and right heart failure can easily be attributed to more common etiologies, delaying the detection of the underlying lymphoma. Furthermore, recognizing this association is of paramount clinical importance. The standard treatment for pulmonary hypertension - vasodilator therapy - is supported by limited evidence and is associated with notorious side effects in PVOD patients, as it can precipitate life-threatening pulmonary edema. When PVOD is the revealing sign of a lymphoma, the diagnostic window is narrow, and the prognosis often hinges on the rapid initiation of systemic chemotherapy rather than traditional pulmonary vascular targeting. This article presents a clinical case that underscores the necessity of including lymphoma in the differential diagnosis of PVOD, particularly when atypical radiological features or systemic symptoms are present [1].
Case presentation
We present the case of a 31-year-old female with no significant history and no professional or environmental exposure. Two years before her admission, she presented with a dry cough, dyspnea on exertion, and polyarthralgia of inflammatory appearance in the context of general deterioration. Clinical examination revealed a conscious patient, tachypneic with a respiratory rate of 24 breaths per minute, with an oxygen saturation of 70% on room air, improving to 94% under 3 L/min of supplemental oxygen. The respiratory examination was unremarkable. Digital clubbing was noted, along with a mobile, painless left axillary lymphadenopathy. The chest x-ray showed an interstitial syndrome with diffuse reticulomicronodular opacities and diffuse bilateral ground-glass opacities (Figure 1).
Posteroanterior chest radiograph showing the presence of an interstitial syndromeThe image shows diffuse bilateral infiltrates with ground-glass attenuation.
Sputum microscopy and Xpert MTB/RIF (Mycobacterium tuberculosis/rifampicin resistance) assay were negative. The angiotensin-converting enzyme (ACE) level was 61 IU/L (normal range: <70 IU/L), reflecting macrophage activation and the presence of granulomatous reactions associated with lymphoma (sarcoid-like reaction). The serum and urinary calcium-phosphate profile showed a serum calcium level of 100.21 mg/L, urinary calcium level of 269 mg/24 h, serum phosphate level of 46 mg/L, and urinary phosphate level of 2029 mg/24 h (elevated). The corrected serum calcium level was slightly decreased (2.1 mmol/L), consistent with an inflammatory context associated with lymphoma, probably related to hypoalbuminemia (Table 1).
The respiratory PCR panel was negative. The search for Pneumocystis jirovecii in sputum was negative. Axillary ultrasound showed left axillary lymphadenopathy measuring 3.8 cm (Figure 2).
Axillary ultrasound image showing left axillary lymphadenopathyThis image shows the left axillary lymphadenopathy measuring 3.8 cm in its long axis, with an oval shape.
The thoracic computed tomography (CT) scan showed bilateral alveolo-interstitial involvement associated with centrilobular ground-glass nodules and scattered micronodules in both lung fields, thickening of the interlobular septa, as well as mediastinal and left axillary lymphadenopathy. There is also an associated pleural and pericardial effusion. Overall, the suggestion of a crazy-paving pattern is highly suggestive of PVOD (Figure 3).
Thoracic CT scan images showing interlobular septal thickening and ground-glass opacitiesDiffuse bilateral thickening of the interlobular septa, with bilateral areas of ground-glass opacities, more marked in the upper lobes and both basal regions, was observed. Branching centrilobular micronodules and parenchymal nodules were present. Mediastinal lymphadenopathy involving the subcarinal region, para-aortic area, Barety’s space, and bilateral hilar regions was present. Bilateral pleural effusion and right fissural pleural effusion, associated with a mild to moderate pericardial effusion, were observed.
Neither bronchoscopy nor lung biopsy could be performed due to the patient’s respiratory condition. A biopsy of the axillary lymph node was performed, which showed that the tumor proliferation was composed of large cells compatible with Reed-Sternberg cells and Hodgkin cells (Figure 4).
Reed–Sternberg cells and Hodgkin cellsThe tumor proliferation is composed of large cells, mononucleated or binucleated, with one or two central nucleoli. The cytoplasm is moderately abundant and eosinophilic. This tumor proliferation is found within a granulomatous inflammatory stroma containing a few eosinophilic polymorphonuclear cells (H&E stain, ×40 magnification).
Immunohistochemical analysis demonstrates findings in favor of Hodgkin lymphoma (Figure 5).
Immunohistochemical analysis demonstrates findings in favor of Hodgkin lymphomaA moderate and diffuse membranous expression of anti-CD15 and anti-CD30 antibodies was observed in the large tumor cells. The large tumor cells lacked expression of anti-CD20, with a positive internal control (H&E stain, ×20 magnification).
Arterial blood gas analysis showed a pH of 7.46, PaO_2_ of 32.2 mmHg, PaCO_2_ of 33.8 mmHg, and HCO_3_^-^ of 23.9 mmol/L, with an oxygen saturation of 76%, consistent with respiratory alkalosis associated with severe hypoxemia (Table 2).
Transthoracic echocardiography showed a dilated and hypertrophied right ventricle, no pericardial effusion, and pulmonary hypertension estimated at 70 mmHg (Figure 6). Right heart catheterization could not be performed due to very severe pulmonary hypertension with a high risk of hemodynamic decompensation.
Transthoracic echocardiogram image with pulmonary hypertensionThis image shows a dilated and hypertrophied right ventricle, moderate mitral regurgitation, and pulmonary hypertension estimated at 70 mmHg.
The patient received standard first-line chemotherapy for Hodgkin lymphoma with appropriate supportive care. The total duration of the treatment was 12 months, with regular follow-up conducted once per month. A favorable clinical and radiological response was observed, leading to complete remission at the end of treatment. Therapy was well tolerated, with only mild and transient adverse effects. The patient remains disease-free under regular follow-up.
Discussion
PVOD is a rare and often underdiagnosed cause of pulmonary hypertension, characterized by progressive fibrotic occlusion of small pulmonary veins and venules. Clinically, PVOD closely mimics pulmonary arterial hypertension (PAH), yet its prognosis, management, and underlying mechanisms differ substantially. The present case highlights PVOD as an unusual but critical manifestation revealing an underlying lymphoma, emphasizing the need to consider secondary and potentially reversible causes in patients presenting with rapidly progressive pulmonary hypertension [2].
PVOD may occur in idiopathic, heritable, drug-induced, or secondary forms. Secondary PVOD has been described in association with connective tissue diseases, infections, exposure to chemotherapeutic agents, and malignancies, particularly hematologic cancers. Lymphoma-associated PVOD remains exceptionally rare, and its pathophysiology is not fully elucidated. Proposed mechanisms include direct venous infiltration by malignant cells, paraneoplastic immune-mediated endothelial injury, cytokine-driven fibroproliferative remodeling, or microthrombotic processes affecting the post-capillary pulmonary vasculature [3].
The diagnostic challenge of PVOD lies in its clinical and hemodynamic resemblance to PAH. However, several features should raise suspicion for PVOD, including profound hypoxemia, severely reduced diffusing capacity for carbon monoxide (DLCO), radiological findings such as centrilobular ground-glass opacities, interlobular septal thickening, and mediastinal lymphadenopathy. In the context of lymphoma, these imaging features may be mistakenly attributed to infection, pulmonary edema, or lymphangitic carcinomatosis, potentially delaying the correct diagnosis [4].
Importantly, the recognition of PVOD has major therapeutic implications. Unlike PAH, the use of pulmonary vasodilators in PVOD may precipitate life-threatening pulmonary edema due to increased capillary hydrostatic pressure in the setting of venous obstruction. In secondary PVOD related to malignancy, management should primarily focus on treating the underlying disease. Several reports suggest that effective lymphoma therapy may stabilize or partially reverse pulmonary vascular involvement, reinforcing the concept that PVOD in this context may represent a paraneoplastic or reactive process rather than irreversible vascular remodeling [5].
This case underscores the importance of a multidisciplinary approach combining clinical, radiological, hemodynamic, and oncological evaluation. Early identification of lymphoma in patients with suspected PVOD is crucial, as timely initiation of disease-specific therapy may significantly impact prognosis. Some lymphoma treatments may worsen PVOD due to the use of specific chemotherapeutic agents employed in its management. Moreover, this association highlights the need to systematically search for occult malignancy when PVOD is diagnosed, particularly in the presence of lymphadenopathy, systemic symptoms, or atypical imaging findings [6].
In conclusion, PVOD can be the initial manifestation of an underlying lymphoma and should prompt an extensive etiological workup. Recognizing this rare association is essential to avoid inappropriate treatment with pulmonary vasodilators and to enable targeted therapy of the causative malignancy. Increased awareness among clinicians may lead to earlier diagnosis, improved management strategies, and potentially better outcomes in this otherwise devastating condition [7].
Conclusions
PVOD represents a rare and frequently overlooked cause of pulmonary hypertension, with clinical and radiological features that closely resemble PAH. This case highlights PVOD as an unusual presenting manifestation of an underlying lymphoma, underscoring the importance of considering secondary and potentially reversible etiologies. Early recognition of this association is crucial, as misdiagnosis may lead to inappropriate use of pulmonary vasodilators and severe clinical deterioration. A thorough etiological assessment, particularly in the presence of suggestive imaging findings or systemic features, is essential. Identifying and treating the underlying malignancy may significantly influence disease progression and patient outcomes. Increased awareness of lymphoma-associated PVOD may improve diagnostic accuracy and guide optimal multidisciplinary management of this challenging condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1From the archives of the AFIP: pulmonary vasculature: hypertension and infarction Radiographics Frazier AA Galvin JR Franks TJ Rosado-De-Christenson ML 4915242020001071534710.1148/radiographics.20.2.g 00mc 17491 · doi ↗ · pubmed ↗
- 2Pulmonary veno-occlusive disease and Hodgkin's lymphoma Eur Respir J Swift GL Gibbs A Campbell IA Wagenvoort CA Tuthill D 59659861993 https://pubmed.ncbi.nlm.nih.gov/8491311/8491311 · pubmed ↗
- 3Pulmonary veno-occlusive disease: a comprehensive review of diagnostic challenges, therapeutic limitations, and evolving management Adv Respir Med Foster B Khan S Suarez Gonzalez A Gillenwater S 48932025 https://doi.org/10.3390/arm 930600484128356810.3390/arm 93060048 PMC 12641799 · doi ↗ · pubmed ↗
- 4Pulmonary veno-occlusive disease: pathogenesis, risk factors, clinical features and diagnostic algorithm - state of the art Adv Respir Med Szturmowicz M Kacprzak A Szołkowska M Burakowska B Szczepulska E KuśJ 131141862018 https://doi.org/10.5603/ARM.2018.002110.5603/ARM.2018.002129960280 · doi ↗ · pubmed ↗
- 5Pulmonary veno-occlusive disease Eur Respir J Montani D Lau EM Dorfmüller P 15181534472016 https://pubmed.ncbi.nlm.nih.gov/27009171/2700917110.1183/13993003.00026-2016 · doi ↗ · pubmed ↗
- 6Pulmonary hypertension: CT of the chest in pulmonary venoocclusive disease AJR Am J Roentgenol Resten A Maitre S Humbert M 657018320041520811210.2214/ajr.183.1.1830065 · doi ↗ · pubmed ↗
- 7Pulmonary veno-occlusive disease: the role of CT Radiol Med Mineo G AttinàD Mughetti M 66767311920142429759710.1007/s 11547-013-0363-y · doi ↗ · pubmed ↗