Blended Delivery of a Primary Care Parenting Program for Child Development: A Randomized Clinical Trial
Susan M. Chang, Joanne A. Smith, Amika S. Wright, Julia Rowe-Porter, Kemisha Shaw-Kelly, Florencia Lopez-Boo, Susan P. Walker

TL;DR
A blended parenting program delivered through primary health care in Jamaica improved child development and parenting practices.
Contribution
Demonstrates the effectiveness of combining in-person and remote delivery of parenting programs within government health systems.
Findings
Children in the intervention group had higher developmental levels compared to controls.
Parents in the intervention group provided more stimulating home environments.
Blended delivery methods showed promise for scaling early childhood development programs.
Abstract
This randomized clinical trial explores whether blended in-person and remote delivery of an early childhood parenting program benefits child development and parenting practices among caregiver-child dyads in Jamaica. Does a parenting program combining in-person and remote delivery and implemented by a government primary health system benefit early childhood development and parent behavior? In this randomized clinical trial of 627 parent-child pairs in Jamaica, children in the intervention group had significantly higher developmental levels and their parents provided more stimulating home environments compared with controls. The findings suggest combining in-person and remote delivery methods is a promising strategy for scaling early childhood development programs. There is substantial evidence that programs that build parents’ abilities to support early learning benefit children’s…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Participants | |||
|---|---|---|---|---|
| Total sample (N = 627) | End line sample (n = 491) | |||
| Control (n = 316) | Intervention (n = 311) | Control (n = 254) | Intervention (n = 237) | |
|
| ||||
| Sex | ||||
| Female | 144 (45.6) | 161 (51.8) | 117 (46.1) | 120 (50.6) |
| Male | 172 (54.4) | 150 (48.2) | 137 (53.9) | 117 (49.4) |
| Birth weight, kg | 3.09 (0.53) | 3.06 (0.60) | 3.08 (0.53) | 3.07 (0.64) |
| Age at enrollment, mo | 14.2 (5.6) | 14.3 (5.7) | 14.3 (5.6) | 14.3 (5.7) |
| z Score | ||||
| Height for age | −0.29 (1.32) | −0.36 (1.32) | −0.29 (1.30) | −0.38 (1.38) |
| Weight for length | 0.43 (1.19) | 0.37 (1.14) | 0.44 (1.17) | 0.38 (1.14) |
| Mother’s first child | 106 (33.5) | 97 (31.2) | 89 (35.0) | 71 (30.0) |
|
| ||||
| Age, y | 29.6 (9.0) | 28.5 (8.3) | 29.9 (9.3) | 29.0 (8.3) |
| Maternal characteristics | ||||
| Highest educational grade completed | 10.3 (1.3) | 10.2 (1.7) | 10.2 (1.4) | 10.1 (1.8) |
| Completed secondary education | 202 (63.9) | 191 (61.4) | 161 (63.4) | 139 (58.6) |
| Employed | 158 (50.0) | 151 (48.6) | 124 (48.8) | 115 (48.5) |
| Occupation | ||||
| None or unskilled | 55 (17.4) | 49 (15.8) | 49 (19.3) | 38 (16.0) |
| Semiskilled | 135 (42.7) | 139 (44.7) | 106 (41.7) | 104 (43.9) |
| Skilled or highly skilled | 126 (39.9) | 123 (39.5) | 99 (39.0) | 95 (40.1) |
| Depressive symptoms (CES-D-10 score) | 11.1 (6.6) | 11.4 (6.6) | 11.2 (6.7) | 11.5 (6.6) |
| Parenting attitudes, total score | 30.6 (4.0) | 30.7 (3.9) | 30.5 (3.9) | 30.7 (3.8) |
| FCI activities score | 2.9 (1.3) | 2.9 (1.3) | 2.9 (1.3) | 2.9 (1.3) |
| Father lives with child | 143 (45.3) | 141 (45.3) | 118 (46.5) | 111 (46.8) |
|
| ||||
| Possessions, No. | 7.9 (2.7) | 7.7 (2.6) | 8.0 (2.7) | 7.6 (2.6) |
| Crowding, persons/room, No. | 2.1 (1.3) | 2.1 (1.4) | 2.0 (1.2) | 2.1 (1.3) |
| Sanitation (water and toilet ratings) | 8.8 (3.2) | 8.5 (3.3) | 8.6 (3.2) | 8.4 (3.2) |
| SES factor score | 0.04 (0.99) | −0.04 (1.01) | 0.04 (0.98) | −0.07 (1.00) |
| Outcome | Participants, mean (SD) | Unadjusted B (SE) [95% CI] | Adjusted B (SE) [95% CI] | |||
|---|---|---|---|---|---|---|
| Control (n = 254) | Intervention (n = 237) | |||||
|
| ||||||
| Developmental quotient | 89.2 (12.3) | 91.3 (14.1) | 2.08 (1.20) [−0.27 to 4.45] | .08 | 2.31 (1.08) [0.19 to .42] | .03 |
| Language | 90.6 (18.6) | 92.1 (18.0) | 1.53 (1.66) [−1.72 to 4.79] | .35 | 1.69 (1.53) [−1.33 to 4.71] | .27 |
| Fine motor ability | 89.2 (13.5) | 91.9 (15.5) | 2.77 (1.31) [0.20 to 5.34] | .04 | 2.82 (1.22) [0.42 to 5.23] | .02 |
| Cognition and problem solving | 87.9 (14.3) | 89.8 (16.8) | 1.94 (1.41) [−0.83 to 4.70] | .17 | 2.40 (1.29) [−0.13 to 4.93] | .06 |
|
| ||||||
| Mother’s depressive symptoms (CES-D-10 score) | 11.0 (6.7) | 10.8 (6.8) | −0.20 (0.61) [−1.40 to 1.01] | .75 | NA | NA |
| Parenting attitudes score | 31.2 (4.0) | 31.8 (3.6) | 0.57 (0.34) [−0.11 to 1.24] | .10 | 0.63 (0.33) [−0.03 to 1.28] | .06 |
| HOME total score | 20.4 (3.8) | 21.2 (3.5) | 0.78 (0.33) [0.13 to 1.43] | .02 | 0.90 (0.32) [0.28 to 1.52] | .004 |
| FCI activities score | 2.5 (1.4) | 2.6 (1.3) | 0.05 (0.12) [−0.19 to 0.28] | .68 | NA | NA |
| Language rating | 7.9 (1.4) | 8.0 (1.3) | 0.08 (0.13) [−0.17 to 0.33] | .51 | NA | NA |
| Outcome | Participants No. (%) | Unadjusted OR (SE) [95% CI] | Adjusted OR (SE) [95% CI] | |||
|---|---|---|---|---|---|---|
| Control (n = 252) | Intervention (n = 237) | |||||
| Praise if child behaved well most of the time | 185 (73.4) | 197 (83.1) | 1.78 (0.40) [1.15-2.77] | .01 | 1.84 (0.42) [1.17-2.89] | .008 |
| Praise if child did something that made the parent happy, No./total No. (%) | 132/237 (55.7) | 131/219 (59.9) | 1.12 (0.20) [0.79-1.60] | .52 | NA | NA |
| Parent made toy(s) for child | ||||||
| No | 175 (69.4) | 133 (56.1) | 1.78 (0.34) [1.23-2.58] | .002 | 1.71 (0.33) [1.17-2.48] | .005 |
| Yes | 77 (30.6) | 104 (43.9) | ||||
| Other toys in home, No. | ||||||
| 0-8 | 78 (31.0) | 78 (32.9) | 0.94 (0.16) [0.68-1.31] | .73 | NA | NA |
| 9-14 | 82 (32.5) | 74 (31.2) | ||||
| ≥15 | 92 (36.5) | 85 (35.9) | ||||
| Children’s books in home, No. | ||||||
| 0-1 | 96 (38.1) | 78 (32.9) | 1.22 (0.20) [0.88 to 1.69] | .24 | NA | NA |
| 2-3 | 77 (30.6) | 76 (32.1) | ||||
| ≥4 | 79 (31.3) | 83 (35.0) | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfant Development and Preterm Care · Maternal Mental Health During Pregnancy and Postpartum · Early Childhood Education and Development
Introduction
Responsive caregiving and opportunities to learn are critical components of care, as indicated in the World Health Organization’s Nurturing Care Framework.^1^ Guidelines for improving early childhood development (ECD) call on governments to provide support services for families who are the main providers of care for young children.^2^ There is consistent evidence that building parent skills to promote development benefits parenting behaviors and children’s development.^3,4,5,6^ There is also evidence that offering ECD programs with other services for families, such as health and social protection, may be suitable strategies for scaling.^7,8,9,10,11,12^
The Reach Up early childhood parenting program was developed to increase capacity for implementation of ECD parenting programs in low- and middle-income countries and provides curricula, comprehensive training materials, and manuals on toy making, adaptation, and planning.^13^ The program has been implemented in several countries, and a meta-analysis of evaluations across 8 countries showed significant benefits for children’s cognitive, language, and fine motor abilities and the quality of the home environment.^14^
The COVID-19 pandemic accelerated development of remote delivery methods for ECD programs. Experiences in Latin America and the Caribbean indicated that remote delivery facilitated continued delivery of services^15^ and was accepted by the ECD workforce and families.^16^ However, more evidence is needed on the effectiveness of remote delivery methods and whether these methods may facilitate scaling. Evidence before the pandemic showed promise,^17,18^ with mixed findings during the pandemic. Remote delivery benefited parenting practices in Jamaica,^19^ but there were no significant associations with ECD or parenting practice when text and audio messaging were sent to families in Uruguay.^20^ A telephone-based intervention for Syrian and Jordanian families reduced maternal depressive symptoms but had no significant effects on other parenting outcomes (including parent-child learning activities) or child development.^21^ Interviews with health staff and families in Jamaica suggested remote methods were feasible and acceptable, although staff felt that some in-person contact was necessary.^19^
Combining remote and in-person delivery could facilitate scaling. The objective of this study was to determine whether the Reach Up program, delivered by government primary health care services using a blended approach, benefited children’s development (primary outcome) and parenting behaviors. A second objective was to determine whether impact varied by child’s age and sex, mother’s educational level, or maternal depressive symptoms.
Methods
The Reach Up program is implemented in Jamaica by the Ministry of Health & Wellness (MOHW). In 2019, each parish health team (13 parishes) nominated a health district to participate. Districts generally comprise 3 to 7 primary care centers. Six parishes began fortnightly home visits delivered by community health workers (CHWs) before visits were suspended in March 2020 due to the COVID-19 pandemic. Remote delivery was implemented in these 6 parishes in September 2020 and evaluated from July to October 2021.^19,22^ For this single-blind randomized clinical trial, we recruited a new evaluation sample from the health districts originally nominated. The study was approved by the University of the West Indies research ethics committee (protocol in Supplement 1). Written informed consent was obtained from each child’s primary caregiver before data collection. Participants were advised that participation was voluntary, and they could withdraw from the study at any time. Data were kept in a locked file cabinet or password-protected computer, and access was limited to research staff. The results reported herein adhere to the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline.
Sample
Families were eligible if they had a child aged 3 to 28 months and were beneficiaries of the Jamaica conditional cash transfer program or known by the health staff to live in low-income circumstances. Exclusion criteria were maternal age less than 18 years, due to requirement for adult consent; a child who attended daycare; no consistent caregiver at home; or a child who had a disability likely to affect development.
Families were identified by CHWs and nurses. The research team conducted eligibility checks and collected informed consent from the primary caregiver. All children received usual care at the health centers (eg, well-child checks, immunization).
Sample Size
To enable the CHWs to conduct the intervention together with their usual duties, the number of families enrolled per CHW was limited to 8, with 4 families randomly assigned to intervention and 4 to the waiting list control group. With approximately 8 CHWs per health district, we estimated 32 children in each group per district, giving 416 per group across all 13 districts.
Recruitment was not possible in 1 health district, reducing the estimated total to 384 per group. Effect size (ES) was calculated by dividing the regression coefficient by the pooled-sample SD. From prior work,^23^ we estimated an ES for child developmental quotient (DQ) of 0.3 SD (ie, 3.6 points [SD, 12 points]); the total DQ range for ages 0 to 2 years is 60 to 140 points, with lower scores suggesting delayed development.^24^ A sample size per group of 178 was required for 80% power at a significance level of P < .05. The estimated sample of 384 allowed for lower recruitment levels in some districts and loss to follow-up.
Description of Intervention
The Reach Up program works through strengthening parents’ skills and enjoyment in helping their child learn through play and responsive interactions. The intervention curriculum provides age-appropriate activities. Children begin at their age level and usually move on to the next activities with each contact. The curriculum suggests ways to adjust activities depending on the child’s ability. CHWs made fortnightly contacts by home visits or telephone calls, conducted alternately. Details of the intervention are provided in the Box.
Box. Description of InterventionType of Community
- Three urban and 9 rural health districts Implementing Agency
- Ministry of Health & Wellness, Jamaica Supervisors
- Public health nurses and midwives Delivery Agents
- CHWs Intervention Content Received by Caregivers
- Parent handbook with brief descriptions and pictures of language and play activities
- Home visit or telephone call alternately every 2 wk
- Play materials, provided once per month at home visit
- Weekly text messages Outline of Contacts
- Contacts began with a brief interaction about how the caregiver and child had progressed with previous activities.
- Home visits: The CHW introduced new activities by first observing what the child did, then demonstrating and describing the activity to the caregiver and child; encouraging the child to try it and offering help if needed; and then encouraging the caregiver and child to do the activity together. CHWs demonstrated ways to talk about and show the child objects and activities in their environment and encourage caregivers to respond to the child’s vocalizations and actions. CHWs created a happy atmosphere and modeled giving praise and showing love throughout the visit.
- Telephone calls: Followed a similar sequence, guided by a script. For each activity, the CHW asked the caregiver to turn to the relevant page in the parent handbook and described the new activity. The CHW then asked the caregiver to try it with the child and to explain what they did. The CHW praised the efforts and offered further description and explanation where necessary.
- Both contacts ended with a recap of activities and encouragement to continue activities daily. Training for CHWs and Nurses
- CHWs and nurses received training in 3-d workshops in the blended delivery method, covering conduct of home visits and telephone calls and review of intervention methods. In all, 76% of CHWs had previously received full 10-d training for home visits. CHWs were provided with the curriculum (comprising activities from the home visit curriculum and parent handbook) and visit record books. Supervision
- Nurses were asked to review visits monthly with CHWs individually, provide supportive feedback, and sign the CHW record books. They were also asked to discuss the program at routinely held group meetings and conduct observations of visits using a provided 15-item checklist. Supervision was reviewed with the nurses at the 3-d workshops.
Abbreviation: CHW, community health worker.
Staff Training
Prior to initial implementation in 2019, the MOHW organized training of trainers workshops for nurses and health education officers. Workshops were conducted by the research team and covered training in the program and how to deliver the training and supervision. CHWs were trained in delivery of home visits in 10-day workshops conducted by the MOHW trainers. A member of the research team (S.M.C.) attended 1 day of the workshops and provided feedback to the MOHW trainers.
Due to staff turnover after initial training, nurses identified additional CHWs to deliver the intervention along with CHWs who participated previously. In all, 71 of 93 CHWs (76.3%) had received the 10-day training. Given the time since initial training (3 years) and staff turnover, 3-day workshops were conducted by the research team for nurses and CHWs from May to June 2022 (Box).
Randomization and Implementation Procedure
Training and participant recruitment were done in parishes sequentially, with implementation beginning when recruitment in a parish was complete. For each CHW, a random order for participant group assignment was generated by an independent statistician and kept by a single member of the research team (S.M.C.). Following baseline interviews, participants were given the next available group assignment. CHWs were informed of the assignments and began the intervention with families assigned to the intervention group. Text messages for intervention families began 1 week later. Enrollment began in July 2022, and intervention delivery started on a phased basis from September 2022 to August 2023. End line assessments were conducted after families had received the intervention for 8 months (May 2023 to April 2024).
Measurements
Baseline information was obtained using an interviewer-administered questionnaire.^19,23^ Family data included mother’s age, educational level, and employment status; father’s age and whether he resided in the home; and home environment variables—crowding (persons per room), type of toilet, water supply, and household possessions.^23^ The mother’s attitude concerning child development and parents’ role was assessed by maternal report.^23^ The Family Care Indicators (FCI) questionnaire was used to assess activities the primary caregiver did with the child.^25^ Maternal depressive symptoms were assessed by the brief 10-item Center for Epidemiological Studies–Depression (CES-D-10) scale (score range, 0-30, with scores ≥10 indicating depression).^26^ The CES-D has been used previously in Jamaica.^23^ Child characteristics, including date of birth, sex, birth weight, and current weight and length, were obtained from children’s clinic records.
At end line, measurements of parenting attitudes, parent practices (FCI questionnaire), and maternal depressive symptoms were repeated. Child development was assessed with the Griffiths Mental Development Scales,^24,27^ which have been used in several studies in Jamaica.^23,28,29^ Three of the 5 subscales were used—hearing and speech (language), hand and eye (fine motor), and performance (cognition)—and the DQ was calculated. Four of 6 subscales from the Home Observation for Measurement of the Environment (HOME) were used to measure parenting behaviors—involvement, responsivity, acceptance, and learning materials.^23,30^ Five university graduates, blinded to study objectives and participant group assignment, conducted interviews or testing. Training was approximately 4 weeks.
Interobserver reliability was assessed using intraclass correlations between interviewers and the trainer (A.S.W.) (n = 19 interviews; r > 0.97 for all questionnaires) and between testers and the trainer (S.M.C.) (n = 19 tests; r > 0.97 for all subscales). Ongoing measurement quality remained high for interviews (n = 15) and tests (n = 20). Measurements were conducted in private rooms in health centers.
Information on Program Costs
Cost information was collected in 2022 using invoices from suppliers and salary scales provided by the MOHW for personnel costs. Details are provided in eTable 1 in Supplement 2. We conducted a benefit-cost analysis, following prior reports,^31,32,33^ with sensitivity analysis for discount rates, wages, and treatment intervals. To estimate the present value of benefits, we used the Jamaican efficacy trial of weekly home visiting on which Reach Up is based.^28^
Statistical Analysis
Comparisons of enrollment characteristics for the end line sample were done using t tests or χ^2^ analyses. Principal-component analysis of crowding, water and toilet ratings, and household possessions was used to generate a socioeconomic status (SES) factor score. Multivariate regression analyses were used to examine the treatment effect. A 2-sided P value less than .05 was considered to be statistically significant.
Analysis was by intention to treat. For child development outcomes, group assignment (control = 0, intervention = 1), child sex and age at assessment, and dummy variables for tester were entered. Mother’s educational level (completed secondary level or not), maternal depressive symptoms, and the SES factor score were included as covariates, as these have been related to development in prior studies.^23,34^
We used 3 variables—maternal age, maternal educational level, and household sanitation scores (sum of water and toilet ratings), which differed between participants lost to follow-up and those assessed at end line—to estimate probability of loss and calculated inverse probability weights (IPWs). IPWs were used to adjust for any bias in loss to follow-up.
The same model (omitting tester dummy variables) was used for parent outcomes. We then examined whether impact varied by maternal characteristics (educational level, depressive symptoms) or child’s age and sex using interaction terms. Analyses were conducted with Stata/SE, version 16.0 (StataCorp LLC).
Results
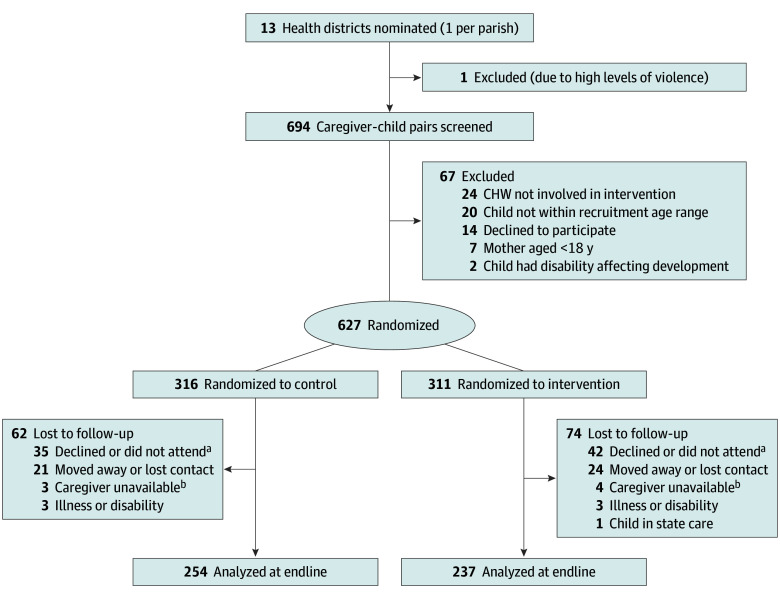
The total sample enrolled was 627 children (311 randomized to intervention and 316 to control; 305 [48.6%] female and 322 [51.4%] male). A total of 491 children were assessed at end line (237 [76.2%] of those in the intervention group and 254 [80.4%] of controls), a follow-up rate of 78.3% (Figure). A total of 393 mothers (62.7%) had completed secondary school. Children lost to follow-up had younger mothers, mothers with higher school grade completed, and higher sanitation scores (sum of water and toilet ratings) than those assessed at end line. There were no other significant differences. Participant characteristics on enrollment are shown in Table 1 for the total sample and end line sample. There were no statistically significant differences in characteristics or in loss to follow-up by group. Children’s mean (SD) ages at end line were 27.0 (5.8) months in the control group and 27.0 (6.1) months in the intervention group; the end line sample consisted of 237 females (48.3%) and 254 males (51.7%). A maximum of 16 contacts occurred per participant (2 per month), with a median of 7 (IQR, 2-10).
CONSORT DiagramCHW indicates community health worker.aCaregiver did not attend assessment after 2 appointments.bCaregiver was unavailable to attend due to work.
Child, parent, and home environment outcomes are shown in Table 2 and Table 3. Unadjusted analyses showed fine motor and HOME scores were significantly greater in the intervention than in the control group (Table 2), and more caregivers in the intervention group made toys and praised their child when they behaved well (Table 3). No other outcomes were significantly different between the groups.
Multivariate regression analyses were conducted for the primary outcomes of child development and for 4 of 10 parent outcomes where unadjusted analyses showed difference at P ≤ .10 (Table 2). Children’s DQ ES (0.17 SD; 95% CI, 0.01-0.33 SD), fine motor subscale score ES (0.19 SD; 95% CI, 0.03-0.36 SD), and HOME score ES (0.25 SD; 95% CI, 0.08-0.41 SD) were higher in the intervention group. There were no between-group differences in language or cognition subscale scores or in parenting attitudes. Logistic regression analyses (Table 3) showed caregivers in the intervention group were more likely to use praise when their child behaved well and to have made toys for their child.
There was no significant heterogeneity of impact by child age (above or below the median age of 26.4 months [IQR, 12.2-46.9 months]), child sex, mother’s educational level (completed secondary-level or not), or maternal depressive symptoms (CES-D-10 score of 0-9 vs 10-30). The estimated annual cost per child per year for the intervention was US $245.79 (eTable 1 in Supplement 2).
For the 8-month intervention period, the cost was US 163.86 per child. To estimate the present value of benefits, we used the Jamaican efficacy trial, which had an impact on DQ of 0.80 SD.^[28](#zoi251494r28)^ The ES of 0.17 SD in the current trial was 21% of the former. Follow-up of the Jamaican efficacy trial participants at age 21 years found 25% higher wages for the treatment group.^[35](#zoi251494r35)^ We multiplied the 25% impact by 0.21 to estimate the impact of the intervention, resulting in an estimated wage increase of 5.3%. We multiplied 0.053 by the average wage to estimate the yearly wage return and used a discount rate of 5% to estimate the net present value of these income gains. Assuming participants enter the labor market at age 17 years and retire at age 65 years and assuming an average annual wage in 2022 of US 4394 (estimated from the weekly minimum wage), the summed yearly gains resulted in a total discounted benefit of $2016 with a benefit-cost ratio of 12.3. Sensitivity analyses and lower and upper bounds are shown in eTable 2 in Supplement 2.
Discussion
Blended delivery of the Reach Up program showed modest benefits to children’s development and parenting behaviors. Implementation and most costs were undertaken by the MOHW, with limited support from the research team related to costs of text messaging and telephone calls. Effect sizes for child development were within the range of other effectiveness trials of Reach Up^36,37,38^ and of other parenting programs using home visits,^10,39,40,41^ although they were lower than the average effect sizes in a meta-analysis of randomized clinical trials evaluating Reach Up^14^ that included small-scale efficacy trials,^28,29,42^ where impact is usually greater. Furthermore, in several effectiveness trials in the meta-analysis, delivery staff and supervisors were hired for the trial and trained by the research teams.^36,43,44^ In 2 trials in Bangladesh, the intervention was delivered by government health workers with large benefits for child development.^11,45^ However, health workers were trained and supervised by the research team. In the current trial, MOHW trainers conducted the main training of CHWs, and supervision was done by nurses.
No significant effect moderation was found when considering child age and sex, maternal educational level, and maternal depressive symptoms. Two meta-analyses^4,14^ suggested impact may be greater for children aged older than 12 months at the start of intervention compared with younger children. In the current study, the median age was above that cutoff. Moderation by child sex is likely to vary by context, with evidence of greater impact in girls in Kenya,^46^ whereas no moderation was observed in Colombia.^37^ Lack of moderation by maternal educational level is consistent with several studies.^14,37,46^ Although the importance of maternal mental health for children’s development is recognized,^2,47^ few studies have examined moderation of intervention impact by maternal depressive symptoms. Further studies examining this are needed.
Implementation of the program was disrupted in 2020 by the COVID-19 pandemic, leading to a gap of 3 years between the 10-day training of CHWs in 2019 and the current implementation. Staff turnover during this period resulted in 1 in 4 of the CHWs who delivered the current program having not participated in that training. The research team therefore conducted 3-day training for all CHWs and nurses prior to the delivery of the blended program, which may not have been sufficient for those without prior training.
CHWs missed contacts because of caregiver unavailability, violence in the community, or conflicting duties such as immunization drives in schools, and in some cases, contacts were missed because the CHWs lacked motivation to conduct the visits. In several centers, monthly supervision by nurses was either not done or done inconsistently, largely because of other work commitments. Similar challenges with staff attrition, staff overwork, and provision of supervision have been reported in other evaluations of home visiting programs integrated in government systems.^48,49,50,51,52^ This study reinforces the importance of attention to staff workload and motivation in future scaling of ECD interventions.
The annual cost per child of the intervention was approximately one-third of that in the original Jamaica efficacy trial^53^ and lower than the costs for weekly home visits in Colombia, Peru, and China.^37,48,53^ The benefit-cost ratio of 12.3 in this study is higher than that of 5.4 reported in Peru^48^ and similar to estimates reported by Karoly^31^ and the higher end of the range (5-11.7) in Nicaragua.^41^ Unlike most other estimates of long-term benefits of ECD interventions,^54^ ours were based on findings for the intervention in the same country (Jamaica).
Limitations
This study has limitations. Evaluation was conducted after 8 months with 2 contacts per month, giving a maximum of 16 contacts with a median of 7 (IQR, 2-10) delivered. This is relatively short compared with prior studies that have generally lasted 1 to 2 years.^14^ The intervention impact on the HOME score and on use of praise and making toys indicated gains in parenting behaviors; with longer duration, these gains may have contributed to larger impact on child development.
The MOHW trained all CHWs in the health districts so that the program could be sustained after evaluation and centers would have capacity to provide the intervention to the waiting list group. Individual randomization was therefore used rather than randomization by center. This introduced the possibility of spillover if CHWs provided elements of the intervention to control families. This is unlikely, as the CHWs did not routinely visit these families. Nonetheless, it is possible that some spillover may have occurred.
Based on a study by Barnett and Masse,^32^ we assumed constant returns in our benefit-cost analysis. Furthermore, the earlier trial^28^ was highly controlled, and long-term impact would likely be lower in most at-scale settings.
Conclusions
This randomized clinical trial of blended delivery of a parenting program by a government primary health care system found benefits to children’s DQ and fine motor ability and the quality of their home environment. This suggests that combining remote and in-person visits could be used to expand coverage of ECD programs. Through our ongoing collaboration with Jamaica’s MOHW, a 5-year plan for ECD has been developed that includes phased scaling of this parenting program. This reinforces the value of sustained partnerships between researchers and policymakers for scaling ECD programs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization, United Nations Children’s Fund, World Bank Group. Nurturing Care for Early Childhood Development: A Framework for Helping Children Survive and Thrive to Transform Health and Human Potential. World Health Organization; 2018. Accessed December 22, 2025. https://www.who.int/publications/i/item/9789241514064
- 2World Health Organization. Improving Early Childhood Development: WHO Guideline. World Health Organization; 2020. Accessed December 22, 2025. https://www.who.int/publications/i/item/97892400020986 32200595 · pubmed ↗
- 3Britto PR, Lye SJ, Proulx K, ; Early Childhood Development Interventions Review Group, for the Lancet Early Childhood Development Series Steering Committee. Nurturing care: promoting early childhood development. Lancet. 2017;389(10064):91-102. doi:10.1016/S 0140-6736(16)31390-3 27717615 · doi ↗ · pubmed ↗
- 4Jeong J, Franchett EE, Ramos de Oliveira CV, Rehmani K, Yousafzai AK. Parenting interventions to promote early child development in the first three years of life: a global systematic review and meta-analysis. P Lo S Med. 2021;18(5):e 1003602. doi:10.1371/journal.pmed.1003602 33970913 PMC 8109838 · doi ↗ · pubmed ↗
- 5Ahun MN, Ali NB, Hentschel E, Jeong J, Franchett E, Yousafzai AK. A meta-analytic review of the implementation characteristics in parenting interventions to promote early child development. Ann N Y Acad Sci. 2024;1533(1):99-144. doi:10.1111/nyas.15110 38354095 · doi ↗ · pubmed ↗
- 6Nores M, Vazquez C, Gustafsson-Wright E, . The cost of not investing in the next 1000 days: implications for policy and practice. Lancet. 2024;404(10467):2117-2130. doi:10.1016/S 0140-6736(24)01390-4 39571590 · doi ↗ · pubmed ↗
- 7Powell C, Baker-Henningham H, Walker S, Gernay J, Grantham-Mc Gregor S. Feasibility of integrating early stimulation into primary care for undernourished Jamaican children: cluster randomised controlled trial. BMJ. 2004;329(7457):89. doi:10.1136/bmj.38132.503472.7C 15217841 PMC 449816 · doi ↗ · pubmed ↗
- 8Yousafzai AK, Rasheed MA, Rizvi A, Armstrong R, Bhutta ZA. Effect of integrated responsive stimulation and nutrition interventions in the Lady Health Worker programme in Pakistan on child development, growth, and health outcomes: a cluster-randomised factorial effectiveness trial. Lancet. 2014;384(9950):1282-1293. doi:10.1016/S 0140-6736(14)60455-4 24947106 · doi ↗ · pubmed ↗