Outcomes after reoperated medial unicompartmental knee arthroplasties compared with primary total and primary unicompartmental knee arthroplasties: a cohort study based on local Danish databases
Christian Bredgaard JENSEN, Claus VARNUM, Simon KORNVIG, Kristine Ifigenia BUNYOZ, Kirill GROMOV, Anders TROELSEN

TL;DR
This study compares outcomes of reoperated medial unicompartmental knee surgeries with primary and reoperated total knee surgeries using patient-reported scores.
Contribution
The study provides new comparative data on patient-reported outcomes for reoperated medial unicompartmental knee arthroplasties.
Findings
Reoperated mUKAs had lower PROM scores than primary mUKAs and TKAs but higher than reoperated TKAs.
PPF mUKAs had scores similar to reoperated TKAs, while PJI and BD mUKAs had scores comparable to primary surgeries.
PJI and BD reoperations achieved outcomes similar to primary mUKAs and TKAs.
Abstract
Tibial periprosthetic fractures (PPF), periprosthetic joint infections (PJI), and bearing dislocations (BD) are among the most common short-term complications in medial unicompartmental knee arthroplasty (mUKA). We aim to assess whether patients with these complications have patient-reported outcome measures (PROMs) that differ from patients with primary mUKA, primary total knee arthroplasty (TKA), or after revision TKA . This observational study included 74 mUKA patients reoperated for PPF (n = 22), PJI (n = 15), or BD (n =3 7) between January 2018 and January 2023. Comparator groups included 1,940 primary mUKA, 3,485 primary TKA, and 350 reoperated TKA patients. The primary endpoint was Oxford Knee Score (OKS) at 12 months. Missing data was imputed, and multilevel Tobit regression was used to analyze differences in PROMs. At 12 months, reoperated mUKAs had lower PROM scores than…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
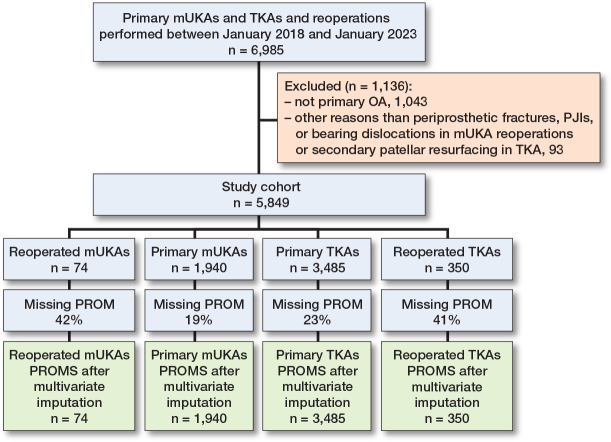 Figure 1
Figure 1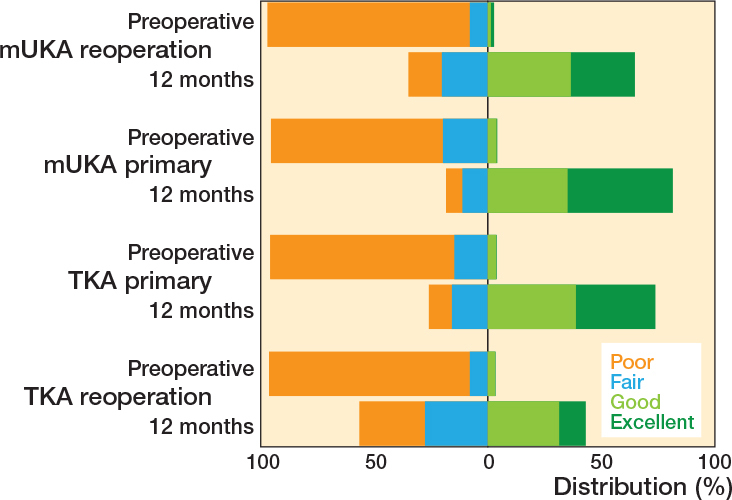 Figure 2
Figure 2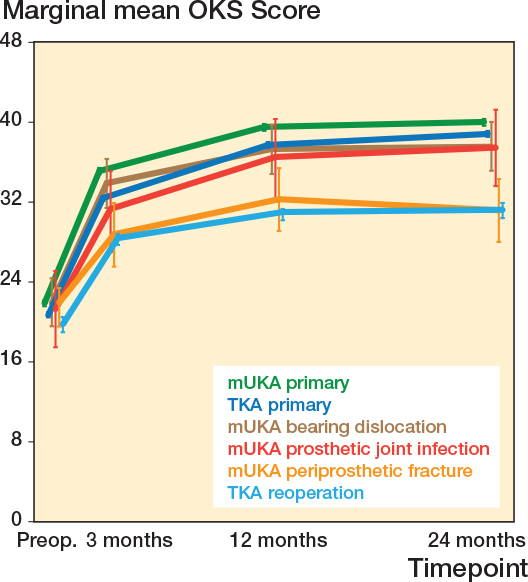 Figure 3
Figure 3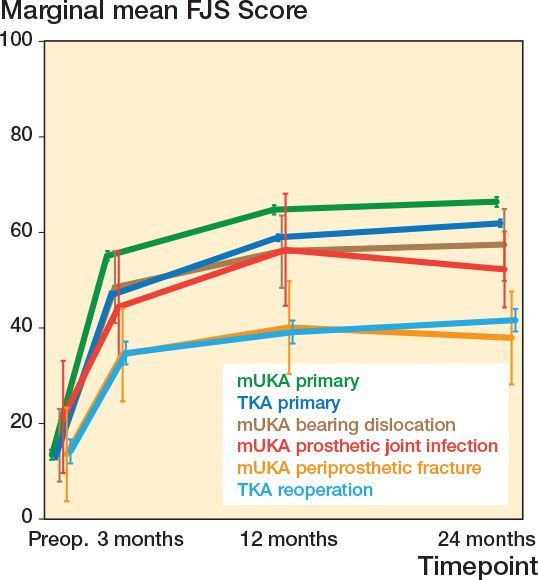 Figure 4
Figure 4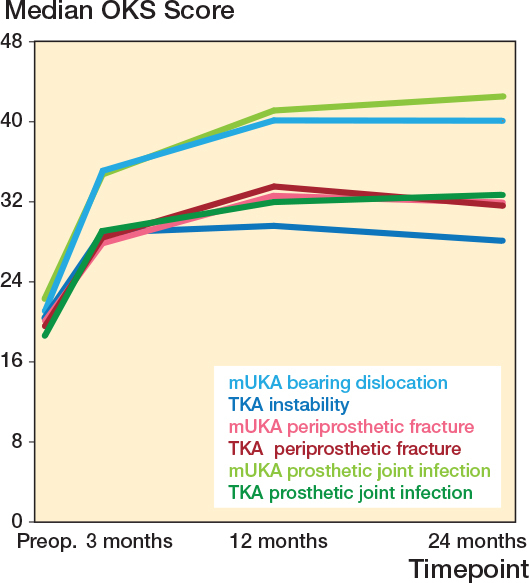 Figure 5
Figure 5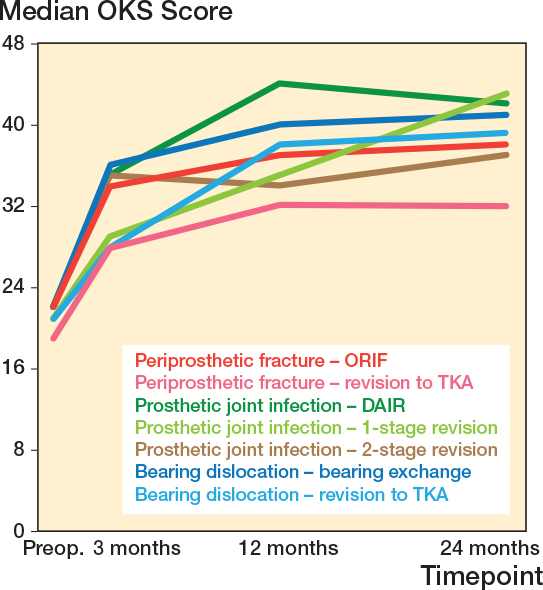 Figure 6
Figure 6| Factor | mUKA | mUKA | TKA | TKA |
|---|---|---|---|---|
| Age | 67.0 (9.2) | 66.9 (9.0) | 69.4 (9.3) | 68.6 (10.4) |
| Female sex | 36 (49) | 1,028 (53) | 2,166 (62) | 192 (55) |
| Body mass index | 30 (5.3) | 30 (5.5) | 30 (6.1) | 30 (4.8) |
| Surgical center | ||||
| Center 1 | 33 (45) | 697 (36) | 1,227 (35) | 166 (47) |
| Center 2 | 41 (55) | 1,243 (64) | 2,258 (65) | 184 (53) |
| Preoperative OKS | 21 (17–24) | 22 (17–26) | 21 (16–25) | 20 (16–24) |
| Preoperative FJS | 14 (7–20) | 13 (5–21) | 12 (5–22) | 14 (7–20) |
| Op. duration, minutes | 63 (41) | 49 (13) | 67 (16) | 116 (49.2) |
| Indication for reoperation | ||||
| Periprosthetic fracture | 22 (30) | – | – | 8 (2.3) |
| Periprosthetic joint infection | 15 (20) | – | – | 82 (23) |
| Bearing dislocation | 37 (50) | – | – | 0 (0) |
| Aseptic loosening | – | – | – | 108 (31) |
| Pain, no loosening | – | – | – | 45 (13) |
| Instability | – | – | – | 68 (19) |
| Polyethylene wear | – | – | – | 21 (6.0) |
| Other | – | – | – | 18 (5.1) |
| Factor | n | Preoperative | OKS | OKS | OKS | Preoperative | FJS | FJS | FJS |
|---|---|---|---|---|---|---|---|---|---|
| Primary mUKA | 1,940 | 22 (17–26) | 36 (31–41) | 41 (36–45) | 42 (36–45) | 13 (5–21) | 55 (38–73) | 67 (49–83) | 70 (50–84) |
| mUKA reoperation | 74 | 21 (17–24) | 33 (25–37) | 38 (29–42) | 38 (30–44) | 15 (8–23) | 42 (27–57) | 52 (28–73) | 54 (29–75) |
| Revised to TKA | 25 | 20 (16–22) | 29 (24–33) | 33 (28–37) | 32 (27–38) | 9 (6–17) | 35 (21–47) | 39 (19–56) | 38 (26–55) |
| Retained mUKA | 49 | 22 (18–25) | 35 (29–39) | 40 (35–44) | 40 (34–45) | 15 (8–20) | 43 (27–60) | 63 (36–75) | 61 (44–79) |
| Periprosthetic fracture | 22 | 20 (16–23) | 28 (23–34) | 33 (28–37) | 32 (26–38) | 13 (13–22) | 39 (26–48) | 56 (31–75) | 78 (36–81) |
| ORIF | 6 | 22 (21–28) | 34 (31–37) | 37 (33–41) | 38 (29–40) | 16 (15–20) | 42 (38–50) | 63 (48–90) | 79 (44–81) |
| Revision to TKA | 16 | 19 (16–23) | 28 (23–33) | 32 (26–36) | 32 (24–38) | 17 (12–20) | 40 (29–43) | 52 (35–54) | 72 (49–82) |
| Periprosthetic joint infection | 15 | 22 (18–25) | 35 (27–37) | 41 (33–45) | 42 (34–46) | 16 (13–22) | 41 (32–48) | 56 (31–75) | 78 (36–81) |
| DAIR | 9 | 22 (19–25) | 35 (24–37) | 44 (35–46) | 42 (35–46) | 16 (15–20) | 42 (38–50) | 63 (48–90) | 79 (44–81) |
| 1-stage revision to TKA | 3 | 21 (19–24) | 29 (27–32) | 35 (30–39) | 43 (35–44) | 17 (12–20) | 40 (29–43) | 52 (35–54) | 72 (49–82) |
| 2-stage revision to TKA | 3 | 22 (18–23) | 35 (32–39) | 34 (31–38) | 37 (35–41) | 6 (6–25) | 35 (32–56) | 40 (31–59) | 38 (36–58) |
| Bearing dislocation | 37 | 22 (18–25) | 35 (27–40) | 40 (35–43) | 39 (35–44) | 13 (6–20) | 44 (27–68) | 63 (36–75) | 60 (45–73) |
| Bearing exchange | 31 | 22 (19–25) | 36 (30–41) | 40 (36–44) | 41 (36–45) | 13 (6–20) | 48 (27–70) | 65 (42–77) | 60 (45–75) |
| Revision to TKA | 6 | 21 (18–29) | 28 (25–34) | 38 (34–38) | 39 (31–41) | 15 (8–17) | 34 (23–45) | 40 (31–50) | 52 (36–65) |
| Primary TKA | 3,485 | 21 (16–25) | 33 (27–38) | 39 (33–43) | 40 (35–44) | 12 (5–22) | 48 (29–65) | 61 (41–78) | 65 (45–81) |
| TKA reoperation | 350 | 20 (16–24) | 29 (23–33) | 32 (25–37) | 31 (23–38) | 14 (7–20) | 35 (19–50) | 41 (20–58) | 42 (19–61) |
| Periprosthetic joint infection | 82 | 19 (17–23) | 29 (25–32) | 32 (26–37) | 33 (27–38) | 15 (9–20) | 36 (25–46) | 45 (31–58) | 46 (34–60) |
| Periprosthetic fracture | 8 | 20 (18–21) | 28 (26–34) | 33 (28–38) | 32 (25–34) | 14 (12–17) | 46 (29–58) | 44 (38–49) | 47 (32–60) |
| Instability | 68 | 20 (15–24) | 29 (23–33) | 30 (23–36) | 28 (20–38) | 15 (6–23) | 28 (15–47) | 35 (8–55) | 40 (17–56) |
| Pain, no loosening | 45 | 19 (15–22) | 26 (20–31) | 31 (23–36) | 32 (22–38) | 12 (5–18) | 25 (19–40) | 37 (15–58) | 36 (18–59) |
| Aseptic loosening | 108 | 20 (15–24) | 29 (23–37) | 34 (28–38) | 32 (24–39) | 14 (7–21) | 36 (18–52) | 42 (21–57) | 42 (19–63) |
| Polyethylene wear | 21 | 21 (17–22) | 31 (28–35) | 30 (25–42) | 33 (20–41) | 14 (4–18) | 33 (21–53) | 44 (15–69) | 46 (14–68) |
| Other | 18 | 22 (19–25) | 31 (28–34) | 33 (27-37) | 31 (25–39) | 17 (10–23) | 46 (30–66) | 44 (18–75) | 37 (16–70) |
| Factor | Oxford Knee Score | Forgotten Joint Score | ||||
|---|---|---|---|---|---|---|
| mUKA primary | TKA primary | TKA reoperation | mUKA primary | TKA primary | TKA reoperation | |
|
| ||||||
| mUKA reoperation | ||||||
| Crude | –2.7 (–4.5 to –1.0) | –1.2 (–2.9 to 0.6) | 1.8 (0.1 to 3.7) | –14.3 (–19.8 to –8.7) | –6.1 (–11.6 to –0.7) | 6.9 (0.9 to 12.8) |
| Adjusted | –2.7 (–4.5 to –1.0) | –1.2 (–2.9 to 0.6) | 1.8 (0.1 to 3.7) | –14.3 (–19.8 to –8.8) | –6.2 (–11.7 to –0.7) | 6.8 (0.9 to 12.8) |
| Periprosthetic fracture | ||||||
| Crude | –4.7 (–7.9 to –1.5) | –3.2 (–6.3 to 0.0) | –0.2 (–3.5 to 3.1) | –20.8 (–30.8 to –10.6) | –12.6 (–22.7 to –2.6) | 0.4 (–10.0 to 10.6) |
| Adjusted | –4.7 (–7.9 to –1.6) | –3.2 (–6.3 to 0.0) | –0.2 (–3.5 to 3.1) | –20.8 (–30.9 to –10.7) | –12.7 (–22.7 to –2.6) | 0.3 (–9.9 to 10.6) |
| Periprosthetic joint infection | ||||||
| Crude | –3.2 (–7.1 to 0.6) | –1.7 (–5.5 to 2.2) | 1.3 (–2.6 to 5.2) | –18.7 (–30.7 to –6.8) | –10.6 (–22.5 to 1.3) | 2.4 (–9.8 to 14.5) |
| Adjusted | –3.2 (–7.1 to 0.6) | –1.7 (–5.6 to 2.2) | 1.3 (–2.6 to 5.2) | –18.7 (–30.7 to –6.8) | –10.6 (–22.6 to 1.3) | 2.4 (–9.8 to 14.5) |
| Bearing dislocation | ||||||
| Crude | –1.3 (–3.8 to 1.2) | 0.3 (–2.2 to 2.7) | 3.2 (0.7 to 5.8) | –8.6 (–16.3 to –0.8) | –0.5 (–8.2 to 7.3) | 12.6 (4.5 to 20.6) |
| Adjusted | –1.3 (–3.8 to 1.2) | 0.3 (–2.2 to 2.7) | 3.2 (0.7 to 5.8) | –8.6 (–16.4 to –0.8) | –0.5 (–8.2 to 7.3) | 12.5 (4.4 to 20.6) |
|
| ||||||
| mUKA reoperation | ||||||
| Crude | –3.3 (–5.0 to –1.5) | –2.7 (–4.4 to –0.9) | 3.0 (1.1 to 4.9) | –16.1 (–21.6 to –10.6) | –10.4 (–15.9 to –4.9) | 10.3 (4.3 to 16.3) |
| Adjusted | –3.3 (–5.0 to –1.5) | –2.7 (–4.4 to –0.9) | 3.0 (1.1 to 5.0) | –16.1 (–21.7 to –10.6) | –10.4 (–15.9 to –4.9) | 10.3 (4.3 to 16.3) |
| Periprosthetic fracture | ||||||
| Crude | –5.6 (–8.8 to –2.4) | –5.0 (–8.1 to –1.8) | 0.7 (–2.5 to 4.0) | –24.8 (–34.9 to –14.7) | –19.1 (–29.1 to –9.0) | 1.6 (–8.7 to 11.9) |
| Adjusted | –5.6 (–8.8 to –2.4) | –5.0 (–8.1 to –1.8) | 0.7 (–2.5 to 3.9) | –24.8 (–34.9 to –14.7) | –19.1 (–29.1 to –9.0) | 1.6 (–8.7 to 11.9) |
| Periprosthetic joint infection | ||||||
| Crude | –2.4 (–6.2 to 1.4) | –1.7 (–5.6 to 2.1) | 3.9 (0.0 to 7.9) | –16.3 (–28.3 to –4.3) | –10.6 (–22.6 to 1.3) | 10.1 (–2.1 to 22.2) |
| Adjusted | –2.4 (–6.2 to 1.5) | –1.7 (–5.6 to 2.1) | 4.0 (0.0 to 7.9) | –16.3 (–28.3 to –4.3) | –10.6 (–22.6 to 1.4) | 10.1 (–2.1 to 22.2) |
| Bearing dislocation | ||||||
| Crude | –2.2 (–4.7 to 0.2) | –1.6 (–4.1 to 0.8) | 4.1 (1.5 to 6.7) | –10.8 (–18.6 to –3.0) | –5.1 (–12.8 to 2.7) | 15.6 (7.5 to 23.7) |
| Adjusted | –2.2 (–4.7 to 0.2) | –1.6 (–4.1 to 0.8) | 4.1 (1.5 to 6.7) | –10.8 (–18.6 to –3.0) | –5.1 (–12.9 to 2.7) | 15.6 (7.5 to 23.6) |
|
| ||||||
| mUKA reoperation | ||||||
| Crude | –3.8 (–5.5 to –2.0) | –3.7 (–5.5 to –2.0) | 2.9 (1.0 to 4.8) | –16.9 (–22.4 to –11.4) | –12.5 (–18.0 to –7.1) | 8.7 (2.7 to 14.6) |
| Adjusted | –3.8 (–5.5 to –2.0) | –3.7 (–5.5 to –2.0) | 2.9 (1.0 to 4.8) | –16.9 (–22.5 to –11.4) | –12.5 (–18.1 to –7.1) | 8.7 (2.6 to 14.6) |
| Periprosthetic fracture | ||||||
| Crude | –7.2 (–10.3 to –4.0) | –7.1 (–10.3 to –3.9) | –0.5 (–3.7 to 2.8) | –28.6 (–38.7 to –18.5) | –24.3 (–34.3 to –14.2) | –3.1 (–13.4 to 7.2) |
| Adjusted | –7.2 (–10.3 to –4.0) | –7.1 (–10.3 to –4.0) | –0.5 (–3.7 to 2.8) | –28.6 (–38.7 to –18.5) | –24.3 (–34.3 to –14.3) | –3.1 (–13.4 to 7.2) |
| Periprosthetic joint infection | ||||||
| Crude | –1.9 (–5.8 to 1.9) | –1.9 (–5.7 to 1.9) | 4.7 (0.8 to 8.7) | –14.0 (–26.0 to –2.0) | –9.7 (–21.6 to 2.3) | 11.5 (–0.7 to 23.7) |
| Adjusted | –1.9 (–5.8 to 1.9) | –1.9 (–5.7 to 1.9) | 4.7 (0.8 to 8.7) | –14.0 (–26.0 to –2.0) | –9.7 (–21.6 to 2.3) | 11.5 (–0.7 to 23.7) |
| Bearing dislocation | ||||||
| Crude | –2.5 (–4.9 to 0.0) | –2.5 (–4.9 to 0.0) | 4.2 (1.6 to 6.8) | –11.0 (–18.8 to –3.2) | –6.7 (–14.5 to 1.1) | 14.5 (6.4 to 22.6) |
| Adjusted | –2.5 (–5.0 to 0.0) | –2.5 (–5.0 to 0.0) | 4.2 (1.6 to 6.7) | –11.0 (–18.9 to –3.2) | –6.7 (–14.5 to 1.0) | 14.5 (6.3 to 22.5) |
| Factor | Oxford Knee Score | Forgotten Joint Score | ||||
|---|---|---|---|---|---|---|
| mUKA primary | TKA primary | TKA reoperation | mUKA primary | TKA primary | TKA reoperation | |
|
| ||||||
| mUKA reoperation (imputed cohort, tobit) | ||||||
| Crude | –2.7 (–4.5 to –1.0) | –1.2 (–2.9 to 0.6) | 1.8 (0.1 to 3.7) | –14.3 (–19.8 to –8.7) | –6.1 (–11.6 to –0.7) | 6.9 (0.9 to 12.8) |
| Adjusted | –2.7 (–4.5 to –1.0) | –1.2 (–2.9 to 0.6) | 1.8 (0.1 to 3.7) | –14.3 (–19.8 to –8.8) | –6.2 (–11.7 to –0.7) | 6.8 (0.9 to 12.8) |
| mUKA reoperation (complete case, tobit) | ||||||
| Crude | –3.9 (–6.7 to –1.0) | –2.0 (–4.9 to 0.8) | 1.4 (–1.7 to 4.5) | –13.9 (–23.4 to –4.4) | –4.5 (–14.0 to 4.9) | 8.6 (–1.6 to 18.8) |
| Adjusted | –3.5 (–6.5 to –0.6) | –1.7 (–4.7 to 1.3) | 1.8 (–1.4 to 5.1) | –13.1 (–23.0 to –3.1) | –3.8 (–13.7 to 6.1) | 8.6 (–2.0 to 19.3) |
| mUKA reoperation (imputed cohort, conventional multilevel) | ||||||
| Crude | –2.7 (–4.4 to –1.0) | –1.2 (–2.9 to 0.5) | 1.8 (0.1 to 3.7) | –13.5 (–18.7 to –8.2) | –5.7 (–10.8 to –0.5) | 6.4 (0.7 to 12.0) |
| Adjusted | –2.7 (–4.4 to –1.0) | –1.2 (–2.9 to 0.5) | 1.8 (0.1 to 3.7) | –13.5 (–18.7 to –8.2) | –5.7 (–10.8 to –0.5) | 6.4 (0.7 to 12.0) |
| mUKA reoperation (complete case, conventional multilevel) | ||||||
| Crude | –3.8 (–6.6 to –1.0) | –2.0 (–4.8 to 0.8) | 1.5 (–1.6 to 3.5) | –14.6 (–23.6 to –5.5) | –5.6 (–14.6 to 3.4) | 6.9 (–2.8 to 16.6) |
| Adjusted | –3.6 (–6.5 to –0.6) | –1.8 (–4.7 to 1.2) | 1.8 (–1.3 to 3.7) | –14.7 (–23.7 to –5.7) | –5.8 (–14.8 to 3.2) | 6.7 (–3.0 to 16.3) |
|
| ||||||
| mUKA reoperation (imputed cohort, tobit) | ||||||
| Crude | –3.3 (–5.0 to –1.5) | –2.7 (–4.4 to –0.9) | 3.0 (1.1 to 4.9) | –16.1 (–21.6 to –10.6) | –10.4 (–15.9 to –4.9) | 10.3 (4.3 to 16.3) |
| Adjusted | –3.3 (–5.0 to –1.5) | –2.7 (–4.4 to –0.9) | 3.0 (1.1 to 5.0) | –16.1 (–21.7 to –10.6) | –10.4 (–15.9 to –4.9) | 10.3 (4.3 to 16.3) |
| mUKA reoperation (complete case, tobit) | ||||||
| Crude | –3.5 (–6.3 to –0.6) | –2.7 (–4.4 to –1.0) | 3.7 (0.6 to 6.7) | –13.1 (–22.5 to –3.8) | –7.2 (–16.5 to 2.2) | 15.0 (4.9 to 25.1) |
| Adjusted | –3.5 (–6.5 to –0.6) | –2.9 (–5.9 to 0.0) | 3.8 (0.6 to 7.0) | –13.1 (–22.9 to –3.3) | –7.4 (–17.2 to 2.3) | 15.8 (5.2 to 26.4) |
| mUKA reoperation (imputed cohort, conventional multilevel) | ||||||
| Crude | –3.2 (–5.0 to –1.5) | –2.9 (–4.6 to –1.2) | 2.9 (1.0 to 4.7) | –13.8 (–21.1 to –6.4) | –8.4 (–15.7 to –1.1) | 11.1 (2.7 to 19.5) |
| Adjusted | –3.2 (–5.0 to –1.5) | –2.7 (–4.4 to –1.0) | 2.9 (1.0 to 4.7) | –13.8 (–21.1 to –6.4) | –8.4 (–15.7 to –1.1) | 11.1 (2.7 to 19.5) |
| mUKA reoperation (complete case, conventional multilevel) | ||||||
| Crude | –3.4 (–6.2 to –0.7) | –2.8 (–5.6 to –0.1) | 3.5 (0.5 to 5.5) | –14.5 (–23.3 to –5.6) | –9.0 (–17.8 to –0.2) | 13.4 (3.8 to 23.0) |
| Adjusted | –3.4 (–6.3 to –0.5) | –2.9 (–5.8 to 0.0) | 3.7 (0.6 to 5.7) | –14.4 (–23.3 to –5.6) | –9.1 (–17.9 to –0.3) | 13.3 (3.8 to 22.9) |
|
| ||||||
| mUKA reoperation (imputed cohort, tobit) | ||||||
| Crude | –3.8 (–5.5 to –2.0) | –3.7 (–5.5 to –2.0) | 2.9 (1.0 to 4.8) | –16.9 (–22.4 to –11.4) | –12.5 (–18.0 to –7.1) | 8.7 (2.7 to 14.6) |
| Adjusted | –3.8 (–5.5 to –2.0) | –3.7 (–5.5 to –2.0) | 2.9 (1.0 to 4.8) | –16.9 (–22.5 to –11.4) | –12.5 (–18.1 to –7.1) | 8.7 (2.6 to 14.6) |
| mUKA reoperation (complete case, tobit) | ||||||
| Crude | –3.9 (–7.0 to –0.8) | –4.2 (–7.2 to –1.1) | 3.2 (–0.1 to 6.5) | –14.1 (–24.3 to –3.8) | –10.1 (–20.3 to 0.1) | 12.0 (1.1 to 23.0) |
| Adjusted | –3.9 (–7.1 to –0.8) | –4.4 (–7.5 to –1.2) | 3.7 (–0.3 to 7.1) | –14.2 (–24.7 to –3.6) | –10.7 (–21.1 to –0.2) | 13.7 (2.4 to 25.0) |
| mUKA reoperation (imputed cohort, conventional multilevel) | ||||||
| Crude | –3.6 (–5.3 to –1.8) | –3.6 (–5.3 to –1.9) | 2.9 (1.1 to 4.7) | –13.7 (–21.1 to –6.4) | –9.6 (–16.9 to –2.3) | 9.9 (1.5 to 18.4) |
| Adjusted | –3.6 (–5.3 to –1.8) | –3.6 (–5.3 to –1.9) | 2.9 (1.1 to 4.7) | –13.7 (–21.1 to –6.4) | –9.6 (–16.9 to –2.3) | 9.9 (1.5 to 18.4) |
| mUKA reoperation (complete case, conventional multilevel) | ||||||
| Crude | –3.6 (–6.6 to –0.6) | –3.9 (–6.9 to –0.9) | 3.4 (–0.1 to 5.4) | –15.0 (–24.6 to –5.4) | –11.7 (–21.2 to –2.1) | 11.7 (1.3 to 22.0) |
| Adjusted | –3.5 (–6.6 to –0.4) | –4.0 (–7.1 to –0.9) | 3.9 (–0.6 to 5.9) | –14.9 (–24.5 to –5.3) | –11.6 (–21.2 to –2.0) | 11.7 (1.3 to 22.0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Orthopaedic implants and arthroplasty · Orthopedic Infections and Treatments
Medial unicompartmental knee arthroplasty (mUKA) is a recommended surgical treatment for isolated anteromedial knee osteoarthritis, offering advantages over total knee arthroplasty (TKA) [1], including faster recovery, higher patient satisfaction, and better PROMs [2,3]. However, reoperations occur in 2.3% of mUKAs within 1 year, often due to tibial periprosthetic fractures (PPF), prosthetic joint infection (PJI), or bearing dislocations (BD) [4]. Understanding outcomes for these complications is essential for managing patient expectations and improving preoperative counselling.
While TKA revisions are associated with worse patient-reported outcomes compared with primary TKAs [5], these findings may not apply directly to mUKA. Complications like bearing dislocations are specific to mobile-bearing mUKA designs [6], and primary TKA components can be used in revisions from mUKA to TKA, whereas TKA revisions often require constrained implants [7]. PROMs after mUKAs revised to TKA have been shown to be either similar to or worse than primary TKAs [8,9]. In TKAs, it has been shown that PROMs after revised TKAs are impacted by the reason for revision [10], but similar knowledge in reoperated mUKAs is lacking.
The aim of our study was to investigate whether mUKA patients who experience a tibial periprosthetic fracture, PJI or bearing dislocation have PROM scores that differ from patients with a primary mUKA, primary TKA, or after reoperated TKA.
Methods
Study design
The study was designed as an observational study on routinely, prospectively collected data. The reporting of this study is in accordance with the Reporting of studies Conducted using Observational Routinely-Collected health Data (RECORD) Statement [11].
Study populations
All included patients were operated or reoperated on between January 2018 and January 2023 at 2 high-volume, fast-track arthroplasty centers with a high UKA-usage (≥ 20%) in relation to TKA. Patients undergoing reoperation within this period were included, irrespective of when or where their primary procedure had been performed. The primary study group consisted of mUKA patients reoperated on for tibial periprosthetic fractures, PJIs, or bearing dislocations. The contextual comparator groups were primary mUKAs without reoperation, primary TKAs without reoperation, and reoperated TKAs.
All patients had primary knee arthroplasty for osteoarthritis, and the primary procedure comparator groups excluded those reoperated on within the study period. We defined reoperations as any surgical procedure performed due to arthroplasty complications, including soft-tissue debridement, and this definition is therefore broader than revisions. In reoperated TKA cases, all causes except secondary patellar resurfacing were included, to generate a representative TKA reoperation cohort, serving as contextual comparison. In reoperation groups only the first reoperation was included.
All included mUKAs were operated on using the mobile bearing Oxford Partial Knee (Zimmer Biomet, Warsaw, IN, USA) with a minimally invasive surgical technique with microplasty instruments. Both centers adhere to the contemporary indications for mUKA [12]: primary reduced joint space width or bone-on-bone anteromedial knee osteoarthritis, correctable deformity, functionally intact anterior cruciate ligament, and no inflammatory arthritis. The primary TKAs included in the comparator groups were operated on using either the Persona or the NexGen TKA systems (Zimmer Biomet, Warsaw, IN, USA) at 1 center and the Triathlon TKA system (Stryker, Mahwah, NJ, USA) at the other center.
Data sources
Both centers have a local database on hip and knee arthroplasty using the Procordo software (www.procordo.com). The databases include patient characteristics, surgical data, and PROMs. Patients answered questionnaires, including PROMs preoperatively and at 3, 12, and 24 months postoperatively. Minimum questionnaire follow-up was 1 year, and maximum was 2 years. Preoperative questionnaires were filled out either at home before the preoperative physical examination or nurse-assisted at the preoperative examination. Surgeons reported surgical data postoperatively. Postoperative questionnaires were sent via email when reaching the follow-up times. If patients did not answer the questionnaire, they received a reminder via email or a phone call 2 weeks later. Patients with no reply after the reminder, or patients without an email, were sent the questionnaire in a paper version by post. We considered the data missing if no reply by email or paper version was received.
Reoperated mUKAs and TKAs were identified by reviewing the surgical schedule and the local databases on reoperated patients. We reviewed the charts of all reoperated patients to identify reasons for the reoperation, the type of reoperation, new prosthesis components, and surgical duration.
Outcomes
The PROMs included in the local database were Oxford Knee Score (OKS) and Forgotten Joint Score (FJS). Both are developed and validated for use in knee arthroplasty [13,14]. The OKS has also been validated in revision knee arthroplasty [15]. The OKS ranges from 0 to 48 points, with 48 being the lowest pain and best function in the operated knee [14]. The OKS can be divided into poor (< 27), fair (27 to < 34), good (34 to < 42), and excellent (42–48) scores [16]. The FJS ranges from 0 to 100, with 100 being the lowest joint awareness during everyday activities following arthroplasty. The FJS is not originally meant for use preoperatively but has been used in this regard in previous arthroplasty literature to establish a baseline [17].
The primary outcome of the study was the OKS at the 12-month follow-up [18]. The secondary outcomes of the study were the OKS at 3 and 24 months’ and the FJS at 3, 12, and 24 months’ follow-up. Exploratively, we also present the proportion of OKS within the categories poor, fair, good, and excellent.
Missing data
Complete data in PROM scores for all follow-ups were present in 50% of patients, and 81% had complete data in PROM scores at 12 months. Body mass index (BMI) was missing in 8% of patients. We imputed missing PROM scores and BMI in patients with Multivariate Imputation by Chained Equation (MICE) using Predictive Mean Matching (PMM) under the assumption of data being missing at random [19]. Missing BMI as well as, OKS, and FJS preoperatively, and at 3 months, 12 months, and 24 months, were imputed based on age, sex, BMI, type of surgery (primary mUKA/reoperated mUKA/primary TKA/reoperated TKA), and non-missing OKS and FJS. The imputation was conducted 5 times, each with 10 iterations. We present pooled mean PROM scores and BMI across all 5 imputations. PROM scores and BMI before (complete case cohort) and after imputation are presented in Table A.1 and A.2 (see Supplementary data).
Statistics
We evaluated whether continuous variables were normally distributed using histograms and quantile–quantile plots. We presented normally distributed data using mean and SD, while non-normally distributed data was presented as median and interquartile range (IQR).
We used multilevel Tobit regression to compare PROM scores between the reoperated mUKA patients and our 3 comparator groups, taking potential ceiling effects into account [20]. A crude model with individuals as a random effect and the same model adjusted for age, sex, and BMI (see directed acyclic graph in Supplementary data) [21]) was conducted. We reported marginal means and marginal mean differences based on multilevel Tobit regression models including 95% confidence intervals (CI). Marginal means represent the model-adjusted average outcome for each group, and marginal mean differences represent the adjusted difference between groups. A significance level of 0.05 was used in all analyses.
The following contextual comparisons in primary and secondary outcomes were made using multilevel Tobit regression:
Reoperated mUKA patients compared with the comparator groups.mUKA patients reoperated for tibial periprosthetic fractures compared with the comparator groups.mUKA patients reoperated for PJI compared with the comparator groups.mUKA patients reoperated for bearing dislocations compared with the comparator groups.
3 sensitivity analyses were conducted to evaluate the impact of missing data, imputation, and the use of the multilevel tobit regression model (see Table 4). The first sensitivity analysis was the multilevel Tobit regression analysis conducted on the complete case cohort (before imputation). The second and third sensitivity analyses were conventional multilevel regression models, with individuals as a random effect, conducted on the imputed cohort and the complete case cohort.
Statistical analyses were conducted using R version 4.3.0 (R Core Team, 2023; R Foundation for. Statistical Computing, Vienna, Austria) and STATA 18.0 BE (StataCorp LLP, College Station, TX, USA).
Ethics, funding, and disclosures
Access to chart data was approved by the Regional Council of the Capital Region of Denmark (R-24011865). Data storage and retrieval of data from the local databases was approved by the Knowledge Centre on Data Protection Compliance in the Capital Region of Denmark (P-2024-17761). The local databases gathered data with consent and were approved by the Knowledge Centre on Data Protection Compliance in the Capital Region of Denmark (P-2022-290) and the Record of Data Processing Activities in the Region of Southern Denmark (17/1942). No funding was received for this study.
Complete disclosure of interest forms according to ICMJE are available on the article page, doi: 10.2340/17453674.2025.45182
Results
We included 74 reoperated mUKAs. In the contextual comparator groups, we included 1,940 primary mUKAs, 3,485 primary TKAs, and 350 reoperated TKAs (Figure 1). Average follow-up was 2.0 years (standard deviation [SD] 0.2), with 214 patients only having 1-year follow-up. A higher proportion of women was observed in the primary TKA groups and TKA reoperations had longer surgical duration (Table 1).
Flowchart of patients from the local databases. In the reoperated mUKA group we included only mUKA patients reoperated due to periprosthetic fracture, periprosthetic joint infection, and bearing dislocations. In the reoperated TKA group, all causes for reoperation were included, except for 13 cases of secondary patellar resurfacing. Missing PROM questionnaires is presented as the proportion (%) of missingness across all planned PROM questionnaire follow-ups within each group. OA = knee osteoarthritis, mUKA = medial unicompartmental knee arthroplasty, TKA = total knee arthroplasty, PROM = patient reported outcome measure.
Median OKS and FJS for all groups and subgroups are presented in Table 2.
Overall outcomes for reoperated mUKAs
At 12 months, reoperated mUKAs had lower PROM scores than primary mUKAs (OKS_diff_ –3.3, CI –5.0 to –1.5) and primary TKAs (OKSdiff –2.7, CI –4.4 to –0.9) but higher scores than reoperated TKAs (OKS_diff_ 3.0, CI 1.1–5.0) (Table 3). This trend persisted at 3 and 24 months. Excellent OKS at 12 months were achieved in 28% of reoperated mUKAs, compared with 47% of primary mUKAs, 35% of primary TKAs, and 12% of reoperated TKAs (Figure 2). The sensitivity analyses did not provide results leading to different conclusions; however, in the complete case cohort larger differences between groups were observed (Table 4).
Proportion of patients achieving poor (< 27), fair (27 to < 34), good (34 to < 42), and excellent (42–48) Oxford Knee Scores within primary and reoperated mUKAs and primary and reoperated TKAs preoperatively and 12 months postoperatively. TKA = total knee arthroplasty, mUKA = medial unicompartmental knee arthroplasty.
Outcomes based on mUKA reoperation indication
At 12 months, mUKAs reoperated on for tibial periprosthetic fractures had PROM scores comparable to reoperated TKAs (OKS_diff_ 0.7, CI –2.5 to 3.9; FJS_diff_ 1.6, CI –8.7 to 11.9). However, both primary mUKAs and primary TKAs had statistically significantly higher scores (Table 3, Figures 3 and 4).
Oxford Knee Scores with 95% confidence interval (error bars) from the adjusted multilevel tobit regression models for each of the specific mUKA reoperation indications and the 3 comparator groups. TKA = total knee arthroplasty, mUKA = medial unicompartmental knee arthroplasty, OKS = Oxford Knee Score.
Forgotten Joint Scores with 95% confidence interval (error bars) from the adjusted multilevel tobit regression models for each of the specific mUKA reoperation indications and the 3 comparator groups. TKA = total knee arthroplasty, mUKA = medial unicompartmental knee arthroplasty, FJS = Forgotten Joint Score.
At 12 months, mUKAs reoperated on due to PJI had PROM scores comparable to primary mUKAs (OKS_diff_ –2.4, CI –6.2 to 1.5) and primary TKAs (OKS_diff_ –1.7, CI –5.6 to 2.1), but statistically significantly higher than those of reoperated TKAs (OKS_diff_ 4.0, CI 0.0–0.9) (see Table 3, Figure 3).
At 12 months, mUKAs reoperated on for bearing dislocations had PROM scores comparable to primary mUKAs (OKS_diff_ –2.2, CI –4.7 to 0.2) and primary TKAs (OKS_diff_ –1.6, CI –4.1 to 0.8), but statistically significantly higher than those of reoperated TKAs (OKS_diff_ 4.1, CI 1.5–6.7) (see Table 3, Figure 3).
For FJS at 12 months, mUKAs reoperated on due to PJI or bearing dislocation had scores resembling primary TKAs, but statistically significantly lower than primary mUKAs (see Table 3 and Figure 4).
PJI after mUKA had higher median PROM scores at 12 months compared with PJI after TKA, while mUKAs and TKAs had similar PROM scores after periprosthetic fractures (Figure 5, Table 2).
Oxford Knee Scores for reoperated mUKAs and TKAs sorted for similar indications. TKA = total knee arthroplasty, mUKA = medial unicompartmental knee arthroplasty, OKS = Oxford Knee Score.
Overall, reoperated mUKAs that retained their mUKA (including bearing exchange) had higher PROM scores at 12 months, compared with mUKAs revised to TKA (see Table 2 and Table 3). The least invasive treatment options for each complication resulted in the highest PROM scores (Figure 6).
Oxford Knee Scores for reoperated mUKAs sorted for indication and treatment option. TKA = total knee arthroplasty, mUKA = medial unicompartmental knee arthroplasty, ORIF = open reduction and internal fixation, OKS = Oxford Knee Score.
Discussion
The aim of our study was to investigate whether mUKA patients who experienced complications had PROM scores that differ from primary mUKA patients, primary TKA patients, and reoperated TKA patients. We found that mobile-bearing mUKAs reoperated on due to the most frequent short-term complications (periprosthetic fractures, PJI, and bearing dislocations) have postoperative OKS and FJS that are better than those of reoperated TKAs but worse than those of primary TKAs and primary mUKAs at 3, 12, and 24 months. Reoperation in mUKAs specifically for PJI or bearing dislocation resulted in OKS that were comparable to those of primary mUKAs and primary TKAs at 12 months and significantly higher than those of reoperated TKAs. FJS remained better in primary mUKAs compared with reoperated mUKAs for PJI or bearing dislocation.
Comparing reoperated arthroplasty patients with primary patients helps evaluate whether the outcomes can still be comparable to primary procedures despite complications. Our findings show that reoperated mUKAs achieve lower PROM scores than primary mUKAs and TKAs, but higher than reoperated TKAs. The minimal important difference (MID) for OKS is typically 5 points [22]. However, to consider smaller differences (e.g., 3 points) irrelevant is controversial. In our study, mean OKS differences for reoperated mUKAs compared with primary procedures or reoperated TKAs did not reach the MID threshold, though confidence intervals at 12 months left the possibility open. Similarly, a prior study on revised mobile-bearing mUKAs found lower PROM improvements compared with primary mUKAs and TKAs at 20 months [23]. A study on New Zealand Joint Registry data showed mUKAs revised to TKAs (mean OKS = 30.0) had similar scores to revised TKAs (mean OKS = 29.4) but lower scores than primary mUKAs (mean OKS = 39.2) and TKAs (mean OKS = 37.2) [16]. However, pain was the leading reason for revision in the mUKAs (49%), which likely contributed to poor outcomes, as unexplained pain is not a recommended revision indication [24,25].
Few studies have examined PROM outcomes after revision based on the indication [26], and to our knowledge none have reported PROMs for multiple reoperation indications in mUKA. In our study, the differences in OKS did reach the MID threshold. Similarly, a prior study on TKA revisions reported variation in OKS by revision indication, with lower scores for malalignment (24.0), stiffness (24.2), and unexplained pain (25.0), and higher scores for progressive arthritis (31.2), aseptic loosening (30.3), and fractures (29.5) [10]. While our findings for PJI in mUKAs support better outcomes after less invasive treatments, a TKA study found no significant difference in OKS between 1- and 2-stage revisions for PJI (24.9 vs 22.8) [27]. Comparing our 12-month median OKS for PJI reoperations, mUKAs outperformed TKAs (41 vs 32), emphasizing the need for dedicated studies on mUKA outcomes, as TKA data may not directly apply.
Strengths
A strength of this study is that the mUKAs and their reoperations were performed in 2 high-volume, high-usage arthroplasty centers. Another strength is that all causes for reoperations were identified through chart review rather than diagnosis codes, ensuring greater accuracy. Common limitations of using questionnaire and PROM data include the impact of missing data and ceiling effects [28]. To address these challenges, this study utilized imputation to handle missing data and multilevel Tobit regression to account for ceiling effects in PROM scores [20]. To assess the robustness of our findings, we conducted sensitivity analyses on a non-imputed cohort, using both multilevel Tobit and a conventional multilevel regression model that did not account for ceiling effects.
Limitations
A key limitation of this study is the small number of reoperated mUKAs for each specific complication. As a result, we did not perform statistical analyses on smaller subpopulations, such as those based on treatment options, and the data presented for these groups should be interpreted with caution. Confounding by indication is also an issue in this study when evaluating PROMs sorted for treatment options, as the complexity or severity of the complications is not accounted for but likely affects both the chosen treatment and the PROMs. The comparison of reoperated mUKAs with reoperated TKAs was purely contextual, as the primary indications, reasons for reoperation, and available treatment options differ between these groups. Providing this context helps clinicians and patients interpret the outcomes of mUKA reoperations in relation to the broader landscape of knee arthroplasty care. Additionally, we considered only the first reoperation in this study, and the potential impact of any re-reoperations was not evaluated. Missing data was particularly pronounced in the reoperation groups; however, using multiple imputation can decrease bias even in high proportions of missing data [29]. To ensure transparency, we present results based on both imputed and non-imputed data. The consistency between these analyses supports our conclusions and suggests that the observed effects are not solely an artifact of the imputation.
Conclusion
We found that postoperative PROM scores for reoperated mUKAs vary by complication type. Reoperations for PJI and bearing dislocations achieved outcomes comparable to primary mUKAs and TKAs, while periprosthetic fractures resulted in the lowest scores, resembling those of reoperated TKAs. These findings indicate that reoperated mUKAs can achieve outcomes resembling primary knee arthroplasties, particularly with less invasive treatments.
This knowledge can be useful when discussing reoperation in mUKA patients. When comparing reoperation rates between mUKAs and TKAs, other outcomes should be considered to provide a complete understanding of their relative performance.
Supplementary data
Tables A.1–A.2 and a DAG Figure are available as supplementary data on the article page, doi: 10.2340/17453674.2025.45182
Supplementary Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Price A, Thienpont E, Catani F, Abram S, Troelsen A. Consensus statement on unicompartmental knee replacement: a collaboration between BASK and EKS. Knee 2023; 41 391-6. doi: 10.1016/J.KNEE.2023.03.015.37088518 · doi ↗ · pubmed ↗
- 2Wilson H A, Middleton R, Abram S G F, Smith S, Alvand A, Jackson W F, et al. Patient relevant outcomes of unicompartmental versus total knee replacement: systematic review and meta-analysis. BMJ 2019; 364. doi: 10.1136/BMJ.L 352.PMC 638337130792179 · doi ↗ · pubmed ↗
- 3Beard D J, Davies L J, Cook J A, Mac Lennan G, Price A, Kent S, et al. The clinical and cost-effectiveness of total versus partial knee replacement in patients with medial compartment osteoarthritis (TOPKAT): 5-year outcomes of a randomised controlled trial. Lancet 2019; 394(10200): 746-56. doi: 10.1016/s 0140-6736(19)31281-4.31326135 PMC 6727069 · doi ↗ · pubmed ↗
- 4Bredgaard Jensen C, Lindberg-Larsen M, Kappel A, Henkel C, Mark-Christensen T, Gromov K, et al. Analysis of national real-world data on reoperations after medial unicompartmental knee arthroplasty: insights from a high-usage country. Bone Joint J 2025; 107-B(3): 314-21. doi: 10.1302/0301-620X.107B 3.BJJ-2024-0290.R 1.40020705 · doi ↗ · pubmed ↗
- 5Salimy M S, Paschalidis A, Dunahoe J A, Chen A F, Alpaugh K, Bedair H S, et al. Patients consistently report worse outcomes following revision total knee arthroplasty compared to primary total knee arthroplasty. J Arthroplasty 2024; 39(2): 459-65.e 1. doi: 10.1016/J.ARTH.2023.08.014.37572718 · doi ↗ · pubmed ↗
- 6Crawford D A, Berend K R, Lombardi A V. Management of the failed medial unicompartmental knee arthroplasty. J Am Acad Orthop Surg 2018; 26(20): E 426-E 433. doi: 10.5435/JAAOS-D-17-00107.30113345 · doi ↗ · pubmed ↗
- 7Lunebourg A, Parratte S, Ollivier M, Abdel M P, Argenson J N A. are revisions of unicompartmental knee arthroplasties more like a primary or revision TKA? J Arthroplasty 2015; 30(11): 1985-9. doi: 10.1016/J.ARTH.2015.05.042.26100472 · doi ↗ · pubmed ↗
- 8Lim J B T, Pang H N, Tay K J D, Chia S lu, Lo N N, Yeo S J. Clinical outcomes and patient satisfaction following revision of failed unicompartmental knee arthroplasty to total knee arthroplasty are as good as a primary total knee arthroplasty. Knee 2019; 26(4): 847-52. doi: 10.1016/J.KNEE.2019.04.016.31113700 · doi ↗ · pubmed ↗