Parents’ Knowledge and Practices Regarding Children’s Oral Hygiene: A Cross-Sectional Survey
Renea Popovic, Stipo Cvitanovic, Inge Sarac, Zvonimir Lukac, Zorana Ivankovic Buljan, Ruzica Zovko

TL;DR
This study explores how well parents in Bosnia and Herzegovina understand and practice proper oral hygiene for their children, finding gaps in early dental care and toothpaste use.
Contribution
The study provides new insights into parental oral-hygiene practices and their association with children’s oral health in Bosnia and Herzegovina.
Findings
Most parents and children brush teeth twice daily, but few start brushing before the child's first year.
Parental knowledge and maternal education strongly predict children's oral-hygiene behaviors.
Only 78.2% of children use age-appropriate toothpaste, with inconsistent adherence among parents of younger children.
Abstract
Objective To assess parents’ knowledge of recommended oral-hygiene practices for children and to describe oral-hygiene behaviors within families (parents and children), as well as factors associated with children’s oral-hygiene outcomes. Methods A cross-sectional study was conducted in Mostar (January-June 2025) among 405 parents or guardians of children aged 0-18 years. A structured questionnaire assessed sociodemographic characteristics, oral-hygiene habits, and parental knowledge. The questionnaire was specifically developed for this study and validated through expert review and pilot testing. Descriptive statistics, Spearman’s correlation, Mann-Whitney U, and chi-square tests were used, with statistical significance set at p<0.05. Results Most parents (n=367; 90.6%) and children (n=359; 88.6%) brushed their teeth at least twice daily. Only (n=139; 34.3%) of parents began…
Click any figure to enlarge with its caption.
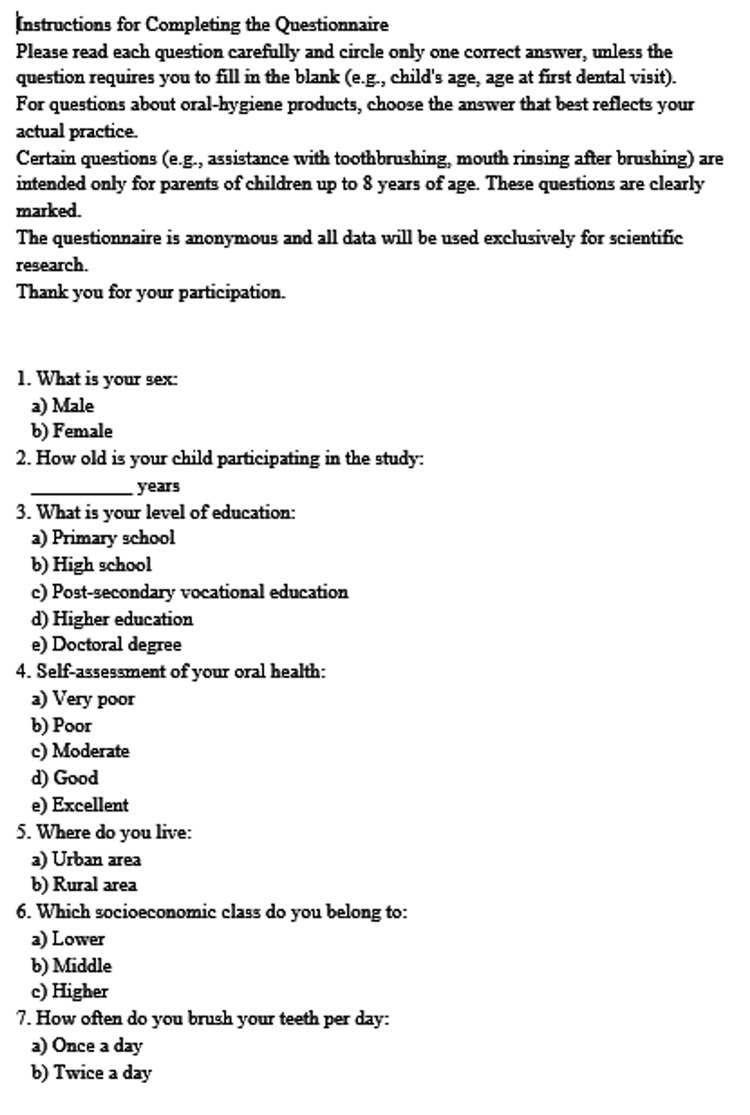 Figure 1
Figure 1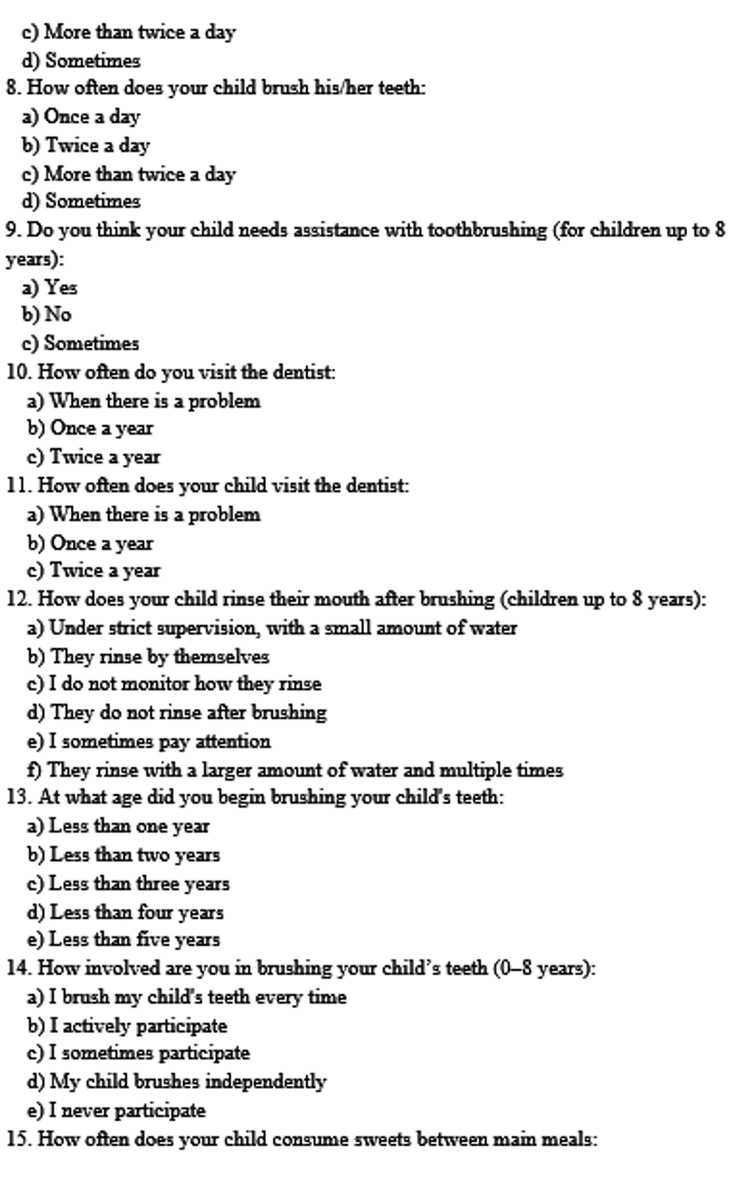 Figure 2
Figure 2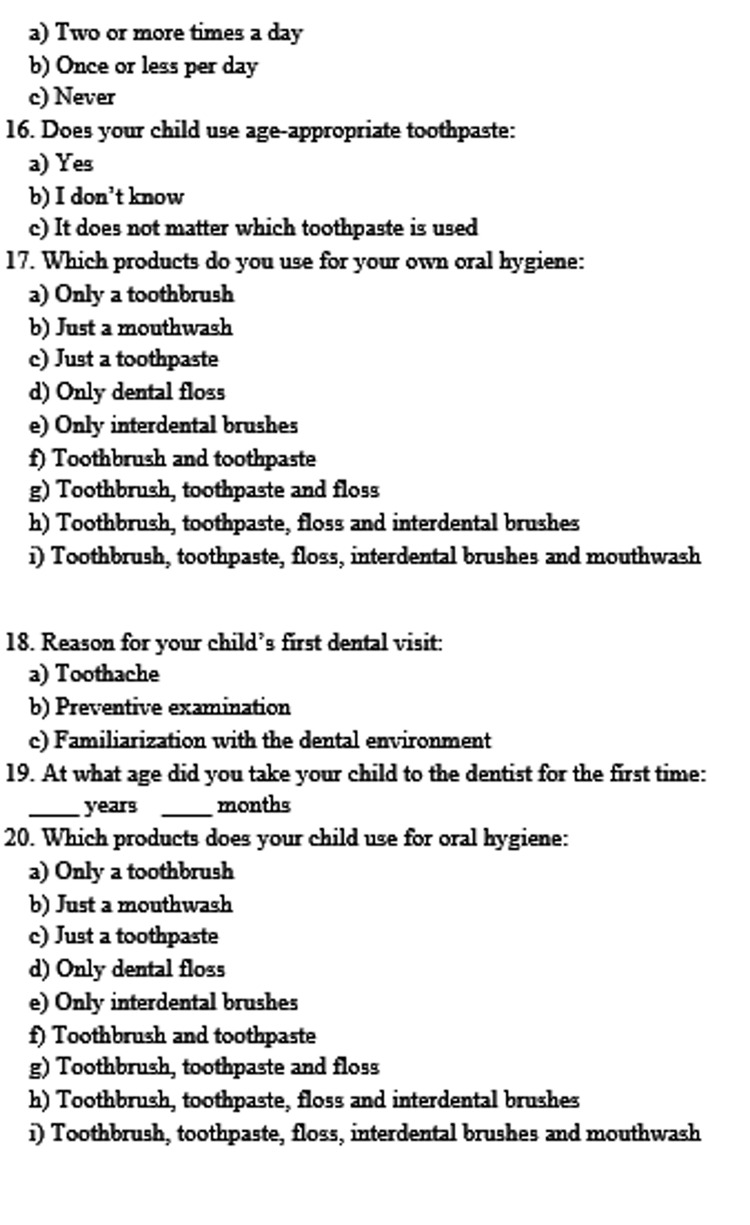 Figure 3
Figure 3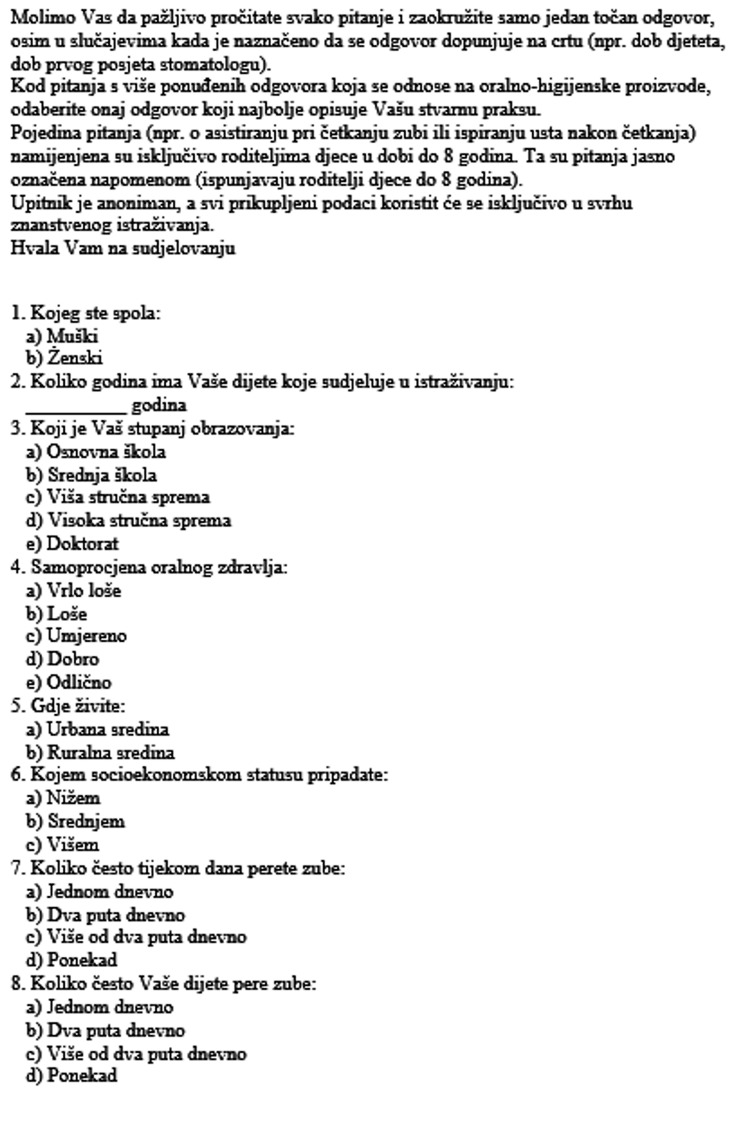 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6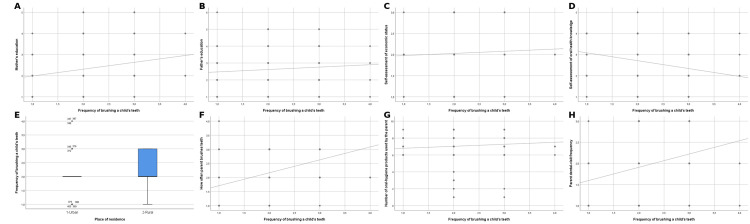 Figure 7
Figure 7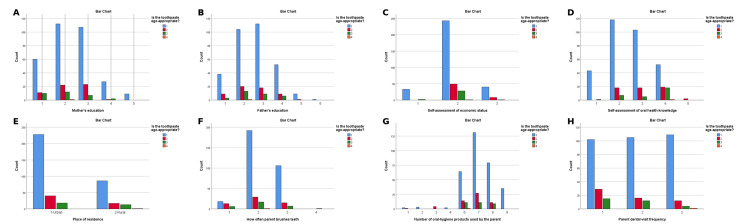 Figure 8
Figure 8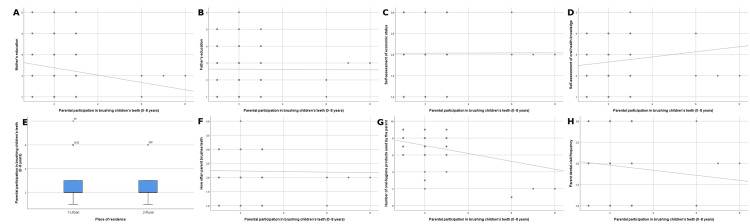 Figure 9
Figure 9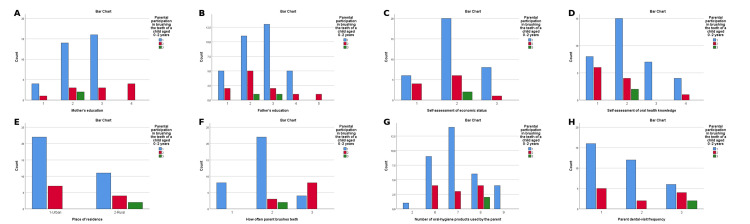 Figure 10
Figure 10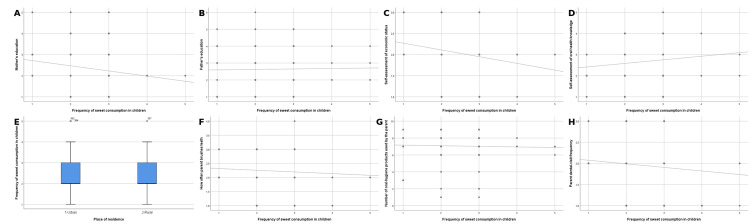 Figure 11
Figure 11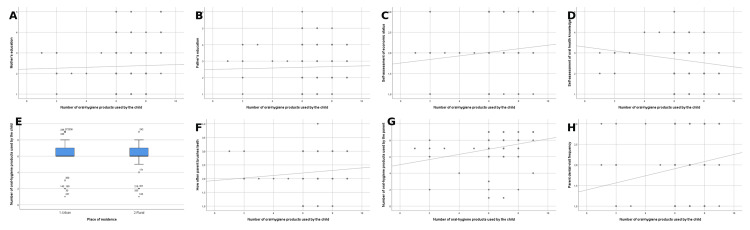 Figure 12
Figure 12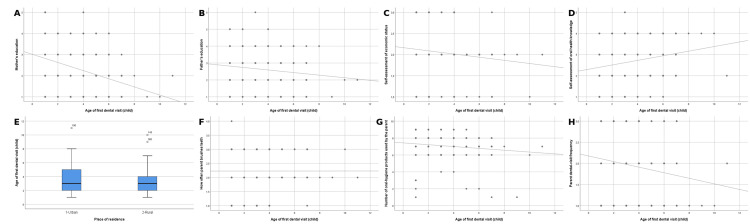 Figure 13
Figure 13| Variable | Category | N=405 | N(%) |
| Sex | Male | 157 | 38.8% |
| Female | 248 | 61.2% | |
| n | 405 | 100% | |
| Child's age | Mean 8.36± SD 4.39 years | ||
| Mother's education level | Primary school | 50 | 20% |
| High school | 90 | 36.4% | |
| Post-secondary vocational education | 84 | 33.9% | |
| Higher education | 18 | 7.4% | |
| Doctorate | 6 | 2.2% | |
| n | 248 | 61.2% | |
| Father's education level | Primary school | 19 | 12.3% |
| High school | 54 | 34.1% | |
| Post-secondary vocational education | 55 | 34.3% | |
| Higher education | 25 | 16.5% | |
| Doctorate | 4 | 2.7% | |
| n | 157 | 38.8% | |
| Oral health self-assessment | Very poor | 18 | 4.4% |
| Poor | 64 | 15.8% | |
| Moderate | 177 | 43.7% | |
| Good | 104 | 25.7% | |
| Excellent | 42 | 10.4% | |
| n | 405 | 100 % | |
| Place of residence | Rural area | 117 | 29.0% |
| Urban area | 286 | 71.0% | |
| n | 403 | 99.51% | |
| Socioeconomic class | Lower | 35 | 8.6% |
| Medium | 321 | 79.3% | |
| Higher | 49 | 12.1% | |
| n | 405 | 100% | |
| Oral hygiene practices in children and parents | Results N=405 | n percentage% | |
| How often do parents brush their teeth daily? | Once a day | 37 | 9.1% |
| Twice a day | 239 | 59.0% | |
| More than twice a day | 128 | 31.6% | |
| Sometimes | 1 | 0.2% | |
| n | 405 | 100% | |
| How often does your child brush his/her teeth? | Once a day | 42 | 10.4% |
| twice a day | 271 | 66.9% | |
| More than twice a day | 88 | 21.7% | |
| Sometimes | 4 | 1.0% | |
| n | 405 | 100% | |
| Do you think a child should be assisted to brush his/her teeth (0-8 years old)? | Yes | 79 | 39.9% |
| No | 58 | 29.3% | |
| Sometimes | 61 | 30.8% | |
| n | 198 | 48.89% | |
| Do you think a child should be assisted to brush his/her teeth (0-2 years)? | Yes | 29 | 63.0% |
| No | 7 | 15.2% | |
| Sometimes | 10 | 21.7% | |
| n | 46 | 11.36% | |
| Do you think a child should be assisted to brush his/her teeth (3-8 years old)? | Yes | 50 | 32.9% |
| No | 51 | 33.6% | |
| Sometimes | 51 | 33.6% | |
| n | 152 | 37.53% | |
| How often do you visit the dentist? | When there is a problem | 146 | 36.0% |
| Once a year | 133 | 32.8% | |
| Twice a year | 126 | 31.1% | |
| n | 405 | 100% | |
| How often does your child visit the dentist? | When there is a problem | 115 | 28.6% |
| Once a year | 107 | 26.6% | |
| Twice a year | 180 | 44.8% | |
| n | 402 | 99.26% | |
| How your child rinses his/her mouth after brushing (0-8 years) | Under strict supervision, with little water | 28 | 19.4% |
| They wash themselves. | 35 | 24.3% | |
| I don't care how they rinse their teeth. | 18 | 12.5% | |
| They don't rinse their teeth afterwards. | 23 | 16.0% | |
| Sometimes I pay attention to how they rinse their teeth. | 30 | 20.8% | |
| They rinse their teeth with a larger amount and more often | 10 | 6.9% | |
| n | 144 | 35.56% | |
| How your child rinses his/her mouth after brushing (0-2 years) | Under strict supervision, with little water | 12 | 27.3% |
| They rinse themselves. | 3 | 6.8% | |
| I don't care how they rinse their teeth. | 5 | 11.4% | |
| They don't rinse their teeth afterwards. | 14 | 31.8% | |
| Sometimes I pay attention to how they rinse their teeth. | 10 | 22.7% | |
| n | 44 | 10.86% | |
| How your child rinses his/her mouth after brushing (2-8 years) | Under strict supervision, with little water | 16 | 17.2% |
| They rinse themselves. | 26 | 28.0% | |
| I don't care how they rinse their teeth. | 13 | 14.0% | |
| They don't rinse their teeth afterwards. | 9 | 9.7% | |
| Sometimes I pay attention to how they rinse their teeth. | 20 | 21.5% | |
| They rinse their teeth with more water and more often | 9 | 9.7% | |
| n | 93 | 22.96% | |
| At what age did you start brushing your child's teeth? | Less than a year | 139 | 34.3% |
| Less than two years | 186 | 45.9% | |
| Less than three years | 54 | 13.3% | |
| Less than four years | 19 | 4.7% | |
| Less than five years | 7 | 1.7% | |
| n | 405 | 100% | |
| Parental participation in brushing children's teeth (0-8 years) | Parents brush their child's teeth every time | 17 | 12.1% |
| I actively participate in brushing teeth. | 67 | 47.5% | |
| I sometimes participate in brushing teeth. | 34 | 24.1% | |
| Child brushes teeth independently | 17 | 12.1% | |
| I never participate in that. | 6 | 4.3% | |
| n | 141 | 34.81% | |
| Parental participation in brushing children's teeth (0-2 years) | Parents brush their child's teeth every time | 15 | 34.1% |
| I actively participate in brushing teeth | 24 | 54.5% | |
| I sometimes participate in brushing teeth | 5 | 11.4% | |
| Child brushes teeth independently | 0 | 0% | |
| I never participate in that. | 0 | 0% | |
| n | 44 | 10.86% | |
| Parental participation in brushing children's teeth (3-8 years) | Parents brush their child's teeth every time | 2 | 2.0% |
| I actively participate in brushing teeth. | 42 | 42.8% | |
| I sometimes participate in brushing teeth. | 28 | 28.6% | |
| Child brushes teeth independently | 17 | 17.3% | |
| I never participate in that. | 9 | 9.1% | |
| n | 98 | 24.20% | |
| How often do your children consume sweets (total) | Never | 17 | 4.3% |
| Once or less per day | 191 | 48.0% | |
| Two or more times a day | 190 | 47.7% | |
| n | 398 | 98.27% | |
| For children up to 2 years old | Never | 6 | 13.3% |
| Once or less per day | 24 | 53.3% | |
| Two or more times a day | 15 | 33.3% | |
| n | 45 | 11.11% | |
| For children 3-8 years | Never | 10 | 6.8% |
| Once or less per day | 80 | 54.1% | |
| Two or more times a day | 58 | 39.2% | |
| n | 148 | 36.54% | |
| Do you put toothpaste on your child's teeth? (0-8 years) | Yes | 53 | 37.3% |
| No | 29 | 20.4% | |
| Sometimes | 60 | 43.3% | |
| Does your child use age-appropriate toothpaste? | Yes | 316 | 78.2% |
| I don't know. | 57 | 14.1% | |
| It doesn't matter what paste he/she uses. | 31 | 7.7% | |
| n | 404 | 99.75% | |
| Products used by parents in oral hygiene | Just a toothbrush | 6 | 1.4% |
| Just dental floss | 4 | 1.0% | |
| Just a mouthwash | 0 | 0% | |
| Just a toothpaste | 0 | 0 | |
| Interdental brushes only | 2 | 0.5% | |
| Toothbrush and toothpaste | 90 | 22.2% | |
| Toothbrush, toothpaste and floss | 169 | 41.7% | |
| Brush, toothpaste, floss and interdental brushes | 99 | 24.4% | |
| Toothbrush, toothpaste, floss, interdental brushes and mouthwash | 35 | 8.6% | |
| n | 405 | 100% | |
| Reason for a child's first visit to the dentist | Toothache | 81 | 20.4% |
| Preventive examination | 214 | 53.9% | |
| Familiarity with the surroundings | 102 | 25.7% | |
| n | 397 | 98.02% | |
| At what age did you take your child to his/her first dental check-up? | Mean 3.42 SD 1.85 | 405 | 100% |
| What products does the child use for oral hygiene? | Just a toothbrush | 2 | 0.49% |
| Just dental floss | 0 | 0% | |
| Just a mouthwash | 0 | 0% | |
| Just a toothpaste | 0 | 0% | |
| Interdental brushes | 0 | 0% | |
| Toothbrush and toothpaste | 226 | 55.8% | |
| Toothbrush, toothpaste and dental floss | 125 | 30.84% | |
| Toothbrush, toothpaste, dental floss and interdental brushes | 40 | 9.8% | |
| Toothbrush, toothpaste, dental floss, interdental brushes and mouthwash | 12 | 2.9% | |
| n | 405 | 100% | |
| Outcome (Dependent variable) | Independent variable | Test used | Statistic | p-value |
| Frequency of brushing a child’s teeth | Mother’s education | Spearman ρ | 0.185 | <0.001 |
| Father’s education | Spearman ρ | 0.092 | 0.065 | |
| Economic status | Spearman ρ | 0.068 | 0.171 | |
| Parental oral-health knowledge | Spearman ρ | –0.240 | <0.001 | |
| Place of residence | Mann–Whitney U | 15802.5 | 0.292 | |
| Parent brushing frequency | Spearman ρ | 0.451 | <0.001 | |
| Parent oral-hygiene products | Spearman ρ | 0.177 | <0.001 | |
| Parent dental-visit frequency | Spearman ρ | 0.235 | <0.001 | |
| Is the toothpaste age-appropriate? | Mother’s education | χ² | 11.866 | 0.457 |
| Father’s education | χ² | 5.40 | 0.988 | |
| Economic status | χ² | 9.85 | 0.131 | |
| Parental oral-health knowledge | χ² | 56.05 | <0.001 | |
| Place of residence | χ² | 5.97 | 0.427 | |
| Parent brushing frequency | χ² | 34.63 | <0.001 | |
| Parent oral-hygiene products | χ² | 44.95 | 0.002 | |
| Parent dental visits | χ² | 15.30 | 0.018 | |
| Parental participation in brushing child's teeth (0–8 yrs) | Mother’s education | Spearman ρ | –0.148 | 0.003 |
| Father’s education | Spearman ρ | 0.020 | 0.686 | |
| Economic status | Spearman ρ | –0.014 | 0.779 | |
| Parental oral-health knowledge | Spearman ρ | 0.129 | 0.009 | |
| Place of residence | Mann–Whitney U | 17145.0 | 0.677 | |
| Parent brushing frequency | Spearman ρ | 0.018 | 0.722 | |
| Parent oral-hygiene products | Spearman ρ | –0.122 | 0.014 | |
| Parent dental visits | Spearman ρ | –0.067 | 0.181 | |
| Parental participation (0–2 yrs) | Mother’s education | χ² | 20.927 | <0.001 |
| Father’s education | χ² | 6.92 | 0.226 | |
| Economic status | χ² | 5.95 | 0.051 | |
| Parental oral-health knowledge | χ² | 37.45 | <0.001 | |
| Place of residence | χ² | 1.16 | 0.560 | |
| Parent brushing frequency | χ² | 3.81 | 0.283 | |
| Parent oral-hygiene products | χ² | 10.36 | 0.169 | |
| Parent dental visits | χ² | 20.53 | <0.001 | |
| Child sweet consumption (total) | Mother’s education | Spearman ρ | –0.160 | 0.001 |
| Father’s education | Spearman ρ | 0.001 | 0.979 | |
| Economic status | Spearman ρ | –0.201 | <0.001 | |
| Parental oral-health knowledge | Spearman ρ | 0.109 | 0.029 | |
| Place of residence | Mann–Whitney U | 17504.5 | 0.413 | |
| Parent brushing frequency | Spearman ρ | –0.067 | 0.175 | |
| Parent oral-hygiene products | Spearman ρ | –0.111 | 0.025 | |
| Parent dental visits | Spearman ρ | –0.051 | 0.307 | |
| Number of oral-hygiene products child uses | Mother’s education | Spearman ρ | –0.036 | 0.473 |
| Father’s education | Spearman ρ | 0.058 | 0.245 | |
| Economic status | Spearman ρ | 0.109 | 0.028 | |
| Parental oral-health knowledge | Spearman ρ | –0.119 | 0.016 | |
| Place of residence | Mann–Whitney U | 18606.0 | 0.051 | |
| Parent brushing frequency | Spearman ρ | 0.128 | 0.010 | |
| Parent oral-hygiene products | Spearman ρ | 0.357 | <0.001 | |
| Parent dental visits | Spearman ρ | 0.147 | 0.003 | |
| Age of first dental visit (child) | Mother’s education | Spearman ρ | –0.371 | <0.001 |
| Father’s education | Spearman ρ | –0.117 | 0.019 | |
| Economic status | Spearman ρ | –0.147 | 0.003 | |
| Parental oral-health knowledge | Spearman ρ | 0.200 | <0.001 | |
| Place of residence | Mann–Whitney U | 17416.0 | 0.513 | |
| Parent brushing frequency | Spearman ρ | –0.023 | 0.644 | |
| Parent oral-hygiene products | Spearman ρ | –0.180 | <0.001 | |
| Parent dental visits | Spearman ρ | –0.139 | 0.005 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Oral microbiology and periodontitis research · Pediatric health and respiratory diseases
Introduction
Poor oral health, particularly tooth decay, in early childhood is a significant public health problem [1]. Oral diseases affect the oral health-related quality of life of more than half of children and adolescents worldwide [2]. Low political priority, combined with the failure to integrate oral health into broader health systems, has contributed to its neglect in previous decades [3]. Data from the latest Global Burden of Disease Study indicate that between 1990 and 2019, the number of new cases of untreated primary tooth decay increased by 1.15 billion. Of these, about 62.9 million can be attributed to sociodemographic inequalities [4].
Early childhood caries (ECC) is a disease of deciduous teeth in children under six years of age. ECC is often untreated, causing painful conditions and impairing the overall health, growth, and development of children [5]. The key factors that cause carious lesions in adults and children are similar. Freshly eroded tooth surfaces may have hypoplastic defects that facilitate the accumulation of bacterial biofilms and an increased risk of caries [6]. A literature review conducted in Canada highlighted the main risk factors for caries: enamel hypoplasia, dietary habits, difficulty with brushing, guardian influence, low income, and low level of education. In addition, those who do not have their first dental check-up within 24 months of age appear to be at higher risk of developing carious lesions. Countries in Central and Eastern Europe have shown a high prevalence of tooth decay among children [6].
The risk of developing dental caries in Bosnia and Herzegovina is twice the regional average among 12-year-olds. Similarly, the overall oral health status in Bosnia and Herzegovina is among the worst in Europe [7]. The role of family and community is well established as a key factor in children's oral health. Children usually learn oral health habits from their parents, as parents and guardians are responsible for the care and perception of children's oral health, especially among preschool children [1]. Mechanical removal of dental plaque, if properly implemented, can be the most effective method of maintaining good oral hygiene, reducing caries, and promoting better gingival health [8].
It is recommended that children start brushing their teeth when their first tooth erupts, and their first visit to the dentist should occur no later than one year of age. The Centers for Disease Control and Prevention (CDC) recommends that children start using fluoride toothpaste at age two. Too much fluoride while teeth are developing can result in noticeable changes in the structure of the enamel, such as discoloration and pitting (dental fluorosis). Children under three years of age should use a rice-sized amount of toothpaste, and children over three years of age should use a pea-sized amount (0.25 g) until the age of six, when the swallowing reflex is sufficiently developed to prevent accidental swallowing [9].
The need for this study arose from the fact that, compared to neighboring countries and the European Union, Bosnia and Herzegovina has the worst oral health among children. This cross-sectional study aimed to assess parents’ knowledge of recommended oral-hygiene practices for children and to describe oral-hygiene behaviors within families (parents and children) in Bosnia and Herzegovina, as well as factors associated with children’s oral-hygiene outcomes. The search included databases, Google Scholar, PubMed, Scopus, and Hrčak until June 2025, using the keywords in Croatian and English "Oral hygiene in children", parental knowledge, tooth brushing habits, Bosnia and Herzegovina, independently and in combination with Boolean operators.
The only research that includes a parental perspective is Oral health behavior of nine-year-old children and their parents in Sarajevo (2019), while other papers focus on dental caries, local indicators of oral health, and adolescent attitudes, without a direct analysis of parental knowledge, which plays a key role in maintaining and promoting oral health in children. We hypothesized that parental knowledge, education level, and parents’ own oral-hygiene behaviors would be significantly associated with their children’s oral-hygiene practices.
Materials and methods
Ethical approval and standard of reporting
This cross-sectional study was approved by the Ethics Committee of the Mostar Health Center (Approval number: 933-37-228/25). Parents were informed about the research process and the conditions of voluntary participation. Written informed consent was obtained from all participants. This cross-sectional survey was conducted from January to June 2025 among parents of preschool and school-age children in Mostar.
The study used a convenience sample of parents who were willing and available to participate at the time of data collection. A total of 700 questionnaires were printed and distributed among parents of preschool and school children, but 405 sufficiently completed questionnaires were collected, which corresponds to a response rate of 57.86%. The remaining questionnaires were not returned or were insufficiently completed for adequate analysis.
The minimum required sample size was calculated using the standard formula for prevalence studies, assuming a 95% confidence level, a 5% margin of error, and a default expected prevalence of 50% - a recommended approach when no prior prevalence data are available (Naing et al.). This calculation yielded a minimum required sample size of 385 participants [10].
Inclusion criteria were that respondents were parents or guardians of children aged 0-18 who voluntarily agreed to participate in the study by completing an anonymous questionnaire. Exclusion criteria were: questionnaires that were largely incomplete and could not be analysed, adults who were not parents or guardians of a child under 18, and ambiguous or contradictory answers that prevented reliable analysis.
Sociodemographic measures
Socioeconomic class was self-assessed by participants and categorized into three groups: lower (financial difficulty or below-average household income), medium (stable average household income), and higher (above-average income or comfortable financial status). Self-assessed oral health was measured using a five-point Likert scale: 1 = very poor, 2 = poor, 3 = moderate, 4 = good, 5 = excellent. Subjective Likert scales for oral-health assessment are routinely used in international epidemiological surveys (WHO Oral Health Surveys, Eurobarometer). These scales intentionally measure perceived rather than clinically defined oral-health status. To limit interindividual variability, all respondents received identical instructions, the variable was treated strictly as ordinal, and non-parametric tests (Spearman’s correlation, Mann-Whitney U, χ²) were applied.
Development and validation of the questionnaire
For the purposes of this study, a questionnaire was developed de novo by the authors, based on relevant literature [6] and international guidelines [European Academy of Paediatric Dentistry (EAPD), CDC] [11-13]. No previously published or proprietary instruments were used. The questionnaire consisted of two sections: the first covered sociodemographic characteristics of parents and children, while the second examined oral-hygiene habits and parental knowledge of recommended practices. The survey was distributed in kindergartens, primary schools, and family medicine or community health centers in Mostar. Parents received the paper-based questionnaire either when bringing or collecting their children from educational institutions or during routine visits to primary healthcare facilities.
The instrument contained 20 items, most of which were closed-ended questions. These items addressed sociodemographic characteristics, oral-hygiene habits of parents and children, and parental knowledge of recommended oral-health guidelines. Since the questionnaire was originally developed in Croatian specifically for this study, no permissions were required for its use. For publication purposes, the questionnaire was translated into English to ensure linguistic clarity. Content validity was confirmed by a three-member expert panel (paediatric dentistry, preventive dentistry, and epidemiology). Pilot testing was conducted among 30 parents who did not participate in the main study, resulting in minor adjustments. The complete questionnaire is provided in Appendices 1-3 (English version) and Appendices 4-6 (Croatian version).
Statistical analysis
Data preparation and coding were performed in Microsoft Excel, while all statistical analyses were conducted using SPSS version 29 (IBM Corp., Armonk, NY). Descriptive statistics (frequencies, percentages, means, and standard deviations) were used to summarise the characteristics of the study sample. Normality of continuous and ordinal variables was assessed using the Shapiro-Wilk test and visual inspection of distribution histograms. Given the ordinal and categorical nature of the variables and their non-parametric distribution of the data, the following statistical methods were applied: Spearman’s rank correlation coefficient to assess associations between ordinal variables; the Mann-Whitney U test to compare differences in ordinal dependent variables between two independent groups; and the chi-square test of independence (χ² test) to examine relationships between categorical variables and differences in response distributions. Response categories were coded numerically in ascending order according to increasing levels of frequency, intensity, or educational attainment, as appropriate for ordinal analyses. All statistical tests were two-tailed, with the significance level set at p<0.05. Results are presented as correlation coefficients (ρ), Mann-Whitney U statistics, and chi-square values (χ²), together with corresponding p-values.
Explanation for the use of Spearman correlation with ordinal categorical variables
Spearman’s rank correlation was used because many questionnaire items were categorical but inherently ordinal in nature. Variables such as brushing frequency, dental visit frequency, and several self-assessment items consisted of ordered response categories (e.g., “never”, “sometimes”, “often”, “always”), which can be meaningfully ranked. Spearman’s correlation does not require normally distributed data and is appropriate for ranked variables. Therefore, all variables with ordered response options were treated as ordinal and analyzed using Spearman’s rank correlation to ensure correct and transparent handling of non-parametric, non-normally distributed data.
Results
Characteristics of research participants
The questionnaire was completed by 405 parents or guardians of children aged 0-18 years. All surveys were completed in paper format, and the sociodemographic characteristics of the parents or guardians are listed in Table 1. The majority of responses, 248 (61.2%), were completed by mothers. The average age of the child surveyed in the study was 8.36 years with a standard deviation of 4.39 years. Most mothers who participated in the study had a high school diploma, 90 (36.4%), while the largest proportion of fathers reported having a post-secondary vocational education, 55 (34.3%). On a self-assessment scale of oral health knowledge, most parents stated that their knowledge of oral health was moderate, 177 (43.7%). The majority of parents who completed the survey, 286 (71%), resided in urban areas. Furthermore, most parents 321 (79.3%) declared that their socioeconomic status was average (Table 1).
Oral hygiene habits of children and parents
Adherence to oral hygiene habits in children and their parents was investigated based on the 2018 guidelines of the EAPD for children, CDC recommendations, and the 2023 Tooth Brushing Recommendations Through Professional Consensus for the general population.
From this data analysis (Table 2), it follows that 239 (59%) of parents adhere to the recommendation to brush their teeth twice a day, while 128 (31.6%) report brushing their teeth more than twice daily. Parents reported that their children brush their teeth twice daily in 271 (66.9%) of cases. Additionally, 88 (21%) of respondents report brushing their teeth more than twice a day. Parents of children in the 0 to eight-year age group reported in 79 (39.9%) of cases that children should be assisted when brushing their teeth, while in the 0 to two-year group, 29 (63%) of parents stated that their children require assistance with toothbrushing. In the three to eight-year age group, 50 (32.9%) of parents think that children should be helped to brush their teeth.
Most parents 146 (36.0%) visit the dentist only when a problem arises. Parents stated in 180 (44.8%) of cases that they take their children for dental visits. Most parents 35 (24.3%) in the 0 to eight-year age group reported that their children rinse their mouths with water after brushing. In the 0 to two-year group, 14 (31.8%) of parents stated that their children do not rinse after brushing, while in the two to eight-year group, 26 (28%) of parents reported that their children rinse with water after brushing. In the 0 to two-year age group, parents stated that in 24 (54.5%) of cases, they actively participate in brushing their children’s teeth, while in the two to eight-year group, parents actively participate in 42 (42.8%) of cases. Children consume sweets once or less per day in 191 (48%) of cases. For individual groups, for children up to two years old, in 24 (53.3%) of cases, they consume sweets once or less per day. In the age group of three to eight years, 80 (54.1%) of children eat sweets once or less per day. In the age group 0 to eight years, 60 (43.3%) of parents stated that they sometimes apply toothpaste to their child's toothbrush. In the 0 to two-year group, this practice is dominant. In the analysis of the answers to the question of when they started brushing their children's teeth, 186 (45.9%) of cases indicated that they began brushing before the age of two, while 139 (34.3%) reported that they began before the age of one. The majority of parents 169 (41.7%) use a toothbrush, toothpaste, and dental floss to maintain oral hygiene. A toothbrush and toothpaste alone are used by 226 (55.8%) of children. The average age of a child's first visit to the dentist was 3.42 years, with a standard deviation of 1.85. The reason for the first visit in 214 (53.9%) of cases was a preventive examination (Table 2).
Bivariate analysis of selected socioeconomic factors in relation to oral hygiene habits in children and parents
Significant associations were observed between several parental factors and children’s oral-health behaviors (Table 3). The frequency of brushing a child’s teeth was significantly associated with mothers’ level of education (p<0.001), parents’ self-assessed oral-health knowledge (p<0.001), parents’ brushing frequency (p<0.001), the number of oral-hygiene products parents use (p<0.001), and parental dental-visit frequency (p<0.001). No significant difference was found for place of residence (p=0.292). Choosing age-appropriate toothpaste for children was significantly associated with parental oral-health knowledge (p<0.001) and parents’ tooth-brushing frequency (p<0.001). It was also associated with parental use of oral-hygiene products (p=0.002) and the frequency of dental visits (p=0.018).
Table 3: Bivariate analysis of selected socioeconomic factors in relation to oral hygiene habits in children and parentsp<0.05 was considered statistically significant
Parental participation in brushing their child’s teeth was significantly associated with maternal education level (p=0.003), parental oral-health knowledge (p=0.009), and the number of oral-hygiene products used by the child (p=0.014). No significant associations were observed with socioeconomic status or place of residence.
For children aged 0 to two years, significant differences were found according to maternal education (p<0.001), parents’ oral-health knowledge (p<0.001), and parental dental-visit frequency (p<0.001).
Children of mothers with higher education (p=0.001) and from families with higher socioeconomic status (p<0.001), as well as those whose parents used a greater number of oral-hygiene products (p=0.025), consumed sweets less frequently between meals. The number of oral-hygiene products the child uses was significantly associated with socioeconomic status (p=0.028), parental oral-health knowledge (p=0.016), parental brushing frequency (p=0.010), the number of products parents use (p<0.001), and parental dental-visit frequency (p=0.003).
The timing of the child’s first dental check-up was significantly associated with maternal education, parents’ self-assessed oral-health knowledge, socioeconomic status, both the use of oral-hygiene products and the frequency of dental visits by parents (all p<0.05). Graphical representations of all bivariate associations presented in Table 3 are provided in Appendices 7-13 to facilitate visual interpretation of the results.
Discussion
Epidemiological data on the incidence of cavities in children in Bosnia and Herzegovina are very scarce. Given the lack of an adequate national database or a national program for the treatment of cavities in children, we cite data from the World Health Organization (WHO), which reports that the prevalence of untreated caries in children aged one to nine years in Bosnia and Herzegovina is 52.7% [14].
According to various studies, the prevalence of childhood caries in Bosnia and Herzegovina ranges between 87.61% and 89.1% [15,16]. Given that there are almost no significant regional or national actions aimed at promoting oral health in Bosnia and Herzegovina, our research focused on the knowledge and habits of parents in maintaining oral hygiene. It has been known for a long time that parents and guardians play a key role in maintaining oral hygiene in children and promoting proper nutrition [17-19].
Compliance with recommendations
Given that there are no national guidelines for maintaining oral hygiene in children and adults, we investigated adherence to certain recommendations by the American Dental Association and to the 2024 consensus-based guidelines (Glenny et al. Development of Tooth Brushing Recommendations Through Professional Consensus) [20].
In practice, our findings show that the vast majority of parents and children do not adhere to the recommendations for maintaining oral hygiene. Parents overwhelmingly adhere to recommendations on the frequency of tooth brushing, with 367 (90.6%) of parents brushing their teeth two or more times a day, while 359 (88.6%) of children brush their teeth two or more times a day. What is concerning is that in the category of children up to eight years of age, 61 (30.8%) of parents think that their child should not be assisted in brushing his/her teeth, while 58 (29.3%) of parents think that they should not be assisted at all. Even more concerning is that 7 (15.25%) of parents of children up to two years of age do not think that their child should be assisted in brushing his/her teeth, and 10 (21.7%) of them think that they should sometimes assist their child in brushing his/her teeth. Parents or guardians should continue to help or supervise tooth brushing until the child can brush his/her teeth effectively on their own [20]. According to various studies and guidelines, the period during which partial or complete supervision of brushing a child's teeth is required is six to eight years.
It should also be noted that most parents visit the dentist when there is a problem and do not go for recommended preventive check-ups. The vast majority of parents stated that their child visits the dentist once or twice a year. Also, only 23 (16%) of parents of children under the age of eight follow the recommendation not to rinse their mouth after brushing their teeth, while 14 (31.8%) of children under the age of two do not rinse their mouth after brushing.
This study found that only 34% of parents took their child to the dentist for the first time before the age of one. The vast majority of parents, 316 (78.2%), reported that they make sure that their child has age-appropriate toothpaste. Another troubling fact is that only 139 (34.3%) of parents started brushing their children's teeth when they were less than a year old. According to WHO recommendations, it is advisable to start brushing a child's teeth when the first tooth erupts, at an average age of six months [14]. This research has unequivocally shown that parents' habits, such as their own tooth brushing, significantly influence children's habits and behavior.
The results presented in this paper show substantial differences in parents' knowledge of oral health and oral hygiene habits, which, in our opinion, is a consequence of the lack of any significant health policy at the national level to educate parents and children. It would be important to focus attention on parents and to encourage parental education because we know that parents play a key role in maintaining oral hygiene in children. Astrom and Jakobsen reported that parents' behavior towards oral health is a model that their children copy [21]. In this bivariate analysis, several parental factors demonstrated significant associations with children’s oral-hygiene behaviours, most notably maternal education and parents’ self-assessed socioeconomic status. Additionally, the frequency of tooth brushing by parents and the amount of products that parents use in oral hygiene were highlighted. It has also been shown that the more often parents visit the dentist, the more often their children visit the dentist.
This study, as well as the study by Kuter et al., shows that there is a relationship between the level of education of mothers and the habits of brushing their children's teeth [22]. Goldenfum et al. also reported that the frequency of brushing children's teeth increased to three times a day with a higher level of maternal education. Another study reported that a higher level of maternal knowledge about oral health was associated with brushing their children's teeth twice a day [23].
Kuter et al. also found a positive correlation between mothers' level of education and the frequency of brushing their children's teeth. As mothers' level of education increased, so did their children's frequency of brushing their teeth. [22] This study found that the most important factors for adequate oral hygiene in children were the mother's knowledge of oral health, socioeconomic status, and the mother's level of education. In the study, place of residence did not play a significant role in the oral habits of children and parents. It was also shown that the father's education, except for the frequency of candy consumption, did not play a significant role in children's oral hygiene.
Also, self-assessment of oral health did not correlate with oral hygiene habits in children. This study, as well as similar studies in Bosnia and Herzegovina [7] and the European Union [24-26], showed that parents do not have enough knowledge about oral hygiene. In Bosnia and Herzegovina, in particular, compared to other studies, it is emphasized that children visit the dentist when there is a problem, and not for a preventive examination, that children come to the dentist for the first examination later, and that oral hygiene maintenance in children is started later. Significant socioeconomic differences in Bosnia and Herzegovina affect the availability of products for maintaining oral hygiene.
We also emphasize again that almost all European Union countries have a national policy on children's oral health, while in Bosnia and Herzegovina, there is no unified national program for oral hygiene for either children or adults [27]. In our opinion, special attention should be paid to educating parents about oral health. We believe that it is urgent to create guidelines for maintaining oral hygiene in children and adults in Bosnia and Herzegovina and to intensify health policy in this direction based on already known, proven public policies in the European Union.
Limitations
This study has several limitations. First, its cross-sectional design prevents the establishment of causality between parental factors and children’s oral-hygiene outcomes. Second, all variables were self-reported, which introduces recall and social-desirability bias. A small proportion of individual items contained missing data (e.g., place of residence and dietary habits). However, the overall level of missing responses was low and handled using pairwise deletion, which is appropriate for cross-sectional survey data. Third, the sample was collected from a single geographic region, which may limit generalizability. Finally, although the questionnaire underwent expert review and pilot testing, full psychometric validation (e.g., test-retest reliability or internal consistency metrics) was not performed.
Conclusions
This study demonstrated that parents in Bosnia and Herzegovina lack sufficient knowledge of recommended oral-hygiene practices and that common mistakes in everyday oral care are frequent. A substantial proportion of children begin tooth brushing later than recommended, toothpaste is often inadequately dosed, and the first dental examination typically occurs after the age of three, frequently prompted by a toothache rather than by preventive care.
Maternal education and parents’ self-assessed oral-health knowledge emerged as the most consistent predictors of children’s oral-hygiene behaviors, while socioeconomic status and parents’ own hygiene habits were associated with several, but not all, oral-health outcomes. Given the high prevalence of dental caries among children in Bosnia and Herzegovina, these findings underscore the urgent need for national oral-health guidelines, earlier first dental visits, and systematic parental education programs aimed at improving children’s oral-health outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perceptions of mothers of preschool children towards oral health services - a qualitative study BMC Oral Health Alkhtib AO Gasim HM Ali K Abidia R Anweigi L 3242520254002546510.1186/s 12903-025-05682-3PMC 11871696 · doi ↗ · pubmed ↗
- 2Global perspective on child and adolescent oral health: a systematic review and meta-analysis of oral impacts on daily performance Evid Based Dent Purohit A Singh A Purohit BM Shakti P 1122520243841369610.1038/s 41432-024-00988-7 · doi ↗ · pubmed ↗
- 3Comparing oral health systems for children in six European countries to identify lessons learned for universal oral health coverage: a study protocol HRB Open Res Mc AuliffeÚ Woods N Barrett S 5520223776720110.12688/hrbopenres.13458.1PMC 10520513 · doi ↗ · pubmed ↗
- 4Trends and age-period-cohort effect on dental caries prevalence from 2008 to 2019 among Brazilian preschoolers Braz Oral Res Ramadan YH Knorst JK Brondani B Agostini BA Ardenghi TM 038202410.1590/1807-3107 bor-2024.vol 38.0004 PMC 1137660238198304 · doi ↗ · pubmed ↗
- 5The burden of early childhood caries in children under 5 years old in the European Union and associated risk factors: an ecological study Nutrients Bencze Z Mahrouseh N Andrade CA Kovács N Varga O 13202110.3390/nu 13020455 PMC 791136933573027 · doi ↗ · pubmed ↗
- 6Evaluation of children caries risk factors: a narrative review of nutritional aspects, oral hygiene habits, and bacterial alterations Children (Basel) Butera A Maiorani C Morandini A Simonini M Morittu S Trombini J Scribante A 9202210.3390/children 9020262 PMC 887066835204983 · doi ↗ · pubmed ↗
- 7Oral health behaviour of nine-year-old children and their parents in Sarajevo Int J Environ Res Public Health Karamehmedovic E Bajric E Virtanen JI 18202110.3390/ijerph 18063235 PMC 800383733800979 · doi ↗ · pubmed ↗
- 8Effectiveness of supervised toothbrushing and oral health education in improving oral hygiene status and practices of urban and rural school children: a comparative study J Int Soc Prev Community Dent Damle SG Patil A Jain S Damle D Chopal N 175181420142537483610.4103/2231-0762.142021 PMC 4209617 · doi ↗ · pubmed ↗