The Effectiveness of Physical Adjunctive Interventions in the Acceleration of Orthodontic Tooth Movement: An Umbrella Review and Meta‐Analysis
Mohamad Radwan Sirri, Mohammad Osama Namera, Mohamad Yaman Salahi Alasbahi, Salar Karim Khalil

TL;DR
This study reviews physical interventions to speed up orthodontic tooth movement, finding that some methods like laser therapy show promise but need better standardization.
Contribution
The paper provides an umbrella review and meta-analysis of physical adjunctive interventions for accelerating orthodontic tooth movement, evaluating their effectiveness and methodological quality.
Findings
Vibration devices showed minimal or no clinically significant acceleration of orthodontic tooth movement.
Low-level laser therapy (LLLT) shortened alignment time and showed early canine retraction gains.
Bioelectric stimulation (BES) showed some acceleration but with low certainty of evidence.
Abstract
Orthodontic treatment often lasts around 20 months, and prolonged duration increases the risk of adverse events. Physical adjunctive interventions (PAIs) are proposed to accelerate tooth movement, but their efficacy remains uncertain. This umbrella review synthesized systematic reviews and meta‐analyses of randomized clinical trials (RCTs) on PAIs published through March 2025 (PubMed, Web of Science, Scopus, Cochrane Library). Review quality was appraised with the A Measurement Tool to Assess Systematic Reviews‐2 (AMSTAR‐2) and the Risk of Bias in Systematic Reviews (ROBIS) tools. Study overlap was quantified using the corrected Graphical Representation of Overlap for Overviews (GROOVE) method. Risk of bias in the primary studies was reassessed, when required, using the Cochrane Risk of Bias 2 (RoB 2) tool. Certainty of evidence was rated with the Grading of Recommendations Assessment,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
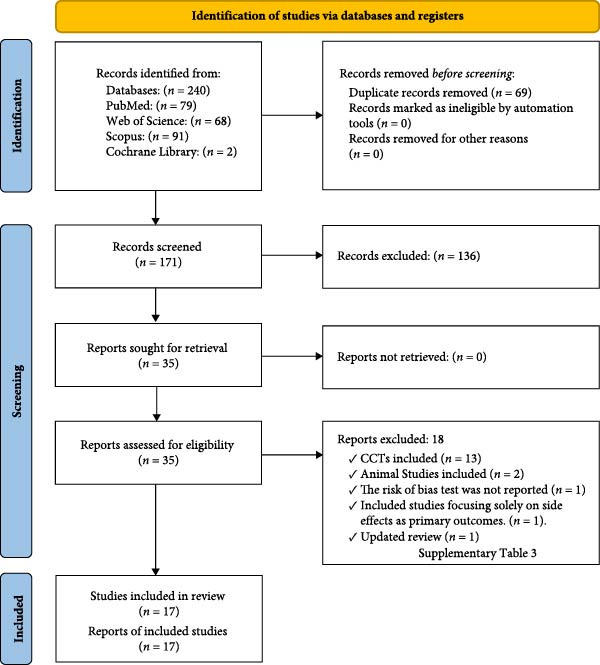 Figure 1
Figure 1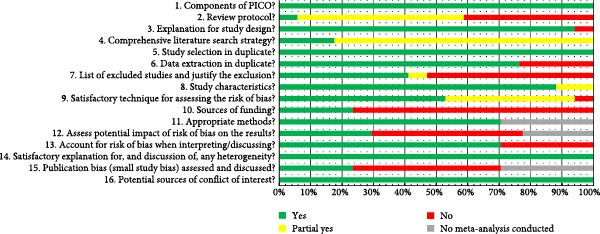 Figure 2
Figure 2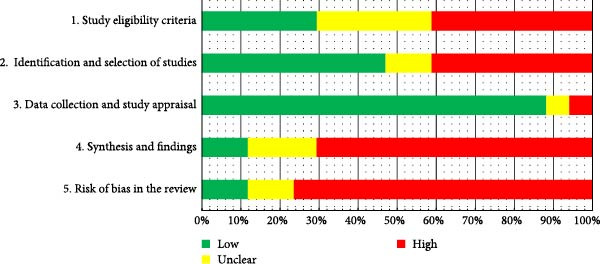 Figure 3
Figure 3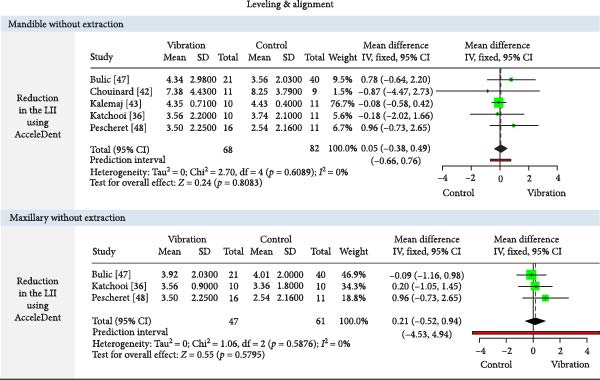 Figure 4
Figure 4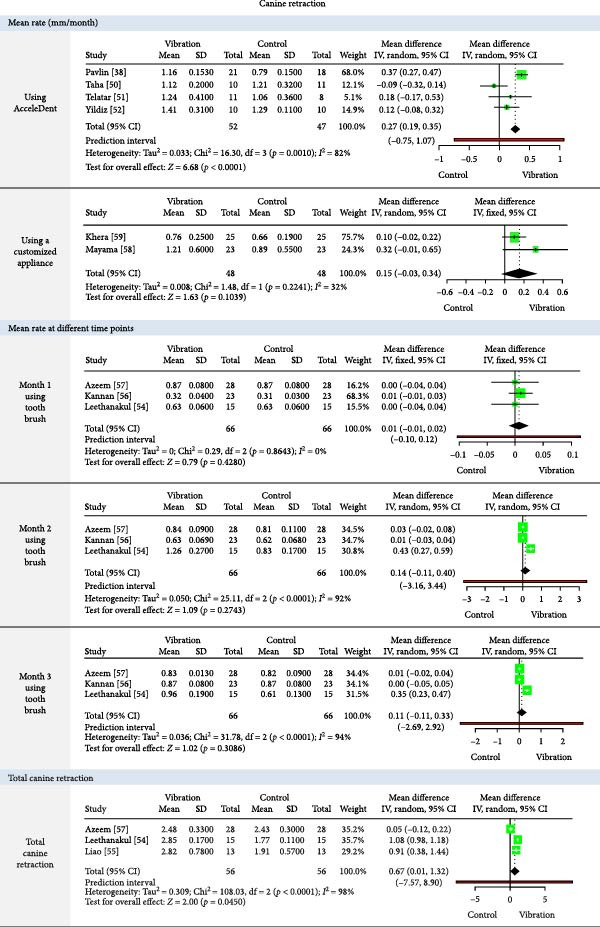 Figure 5
Figure 5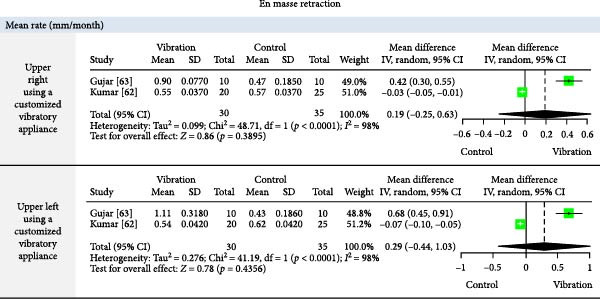 Figure 6
Figure 6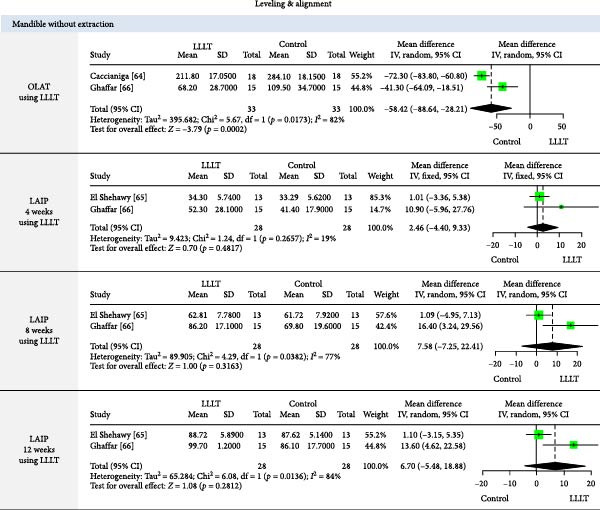 Figure 7
Figure 7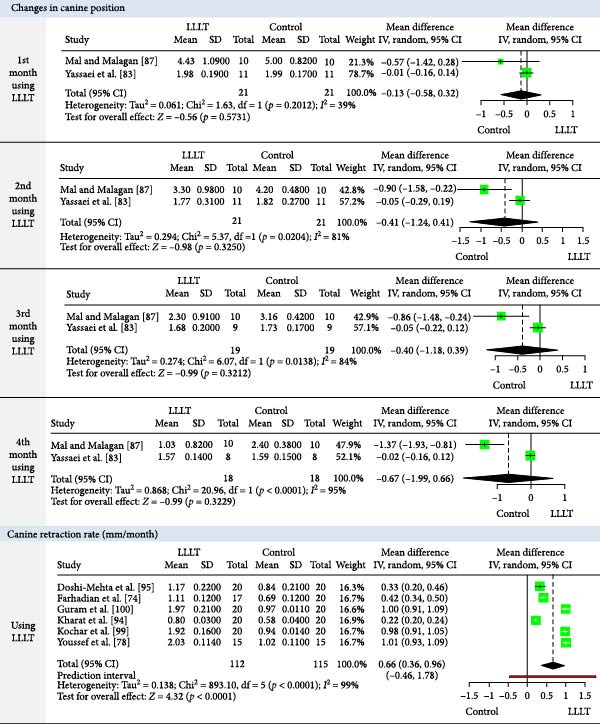 Figure 9
Figure 9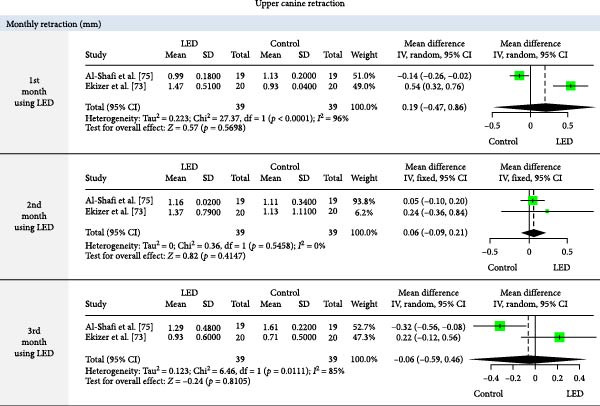 Figure 10
Figure 10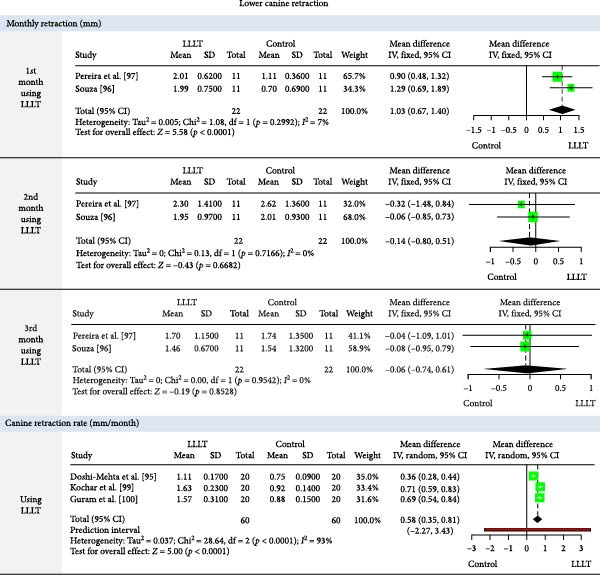 Figure 11
Figure 11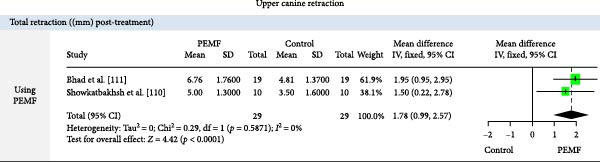 Figure 12
Figure 12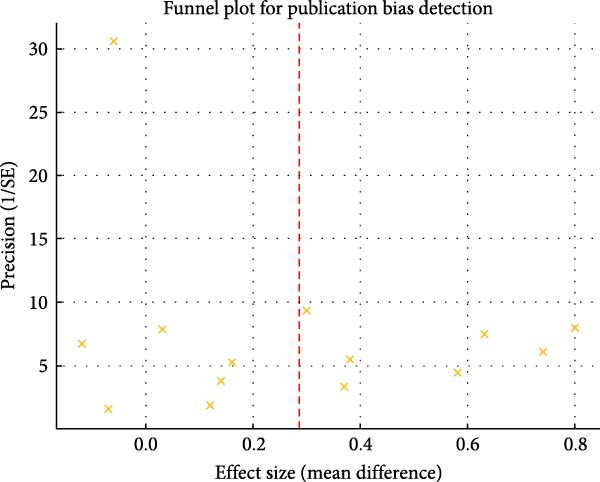 Figure 13
Figure 13| Intervention type | General information | Study identification and search | Methodological quality | Interventions and comparisons | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study ID/author, year, country | Study design | No. of trials and design | Age of participants | No. of participants | Registration status | Search strategy/restrictions | Date of search | ROB assessment tool/quality of evidence | Device |
Specifications VD: Frequency/force/daily use PBMD: WL (nm)/IP/time SE/ED (J/cm²)/ OP (mW) BES: Parameters/duration/Location | Type of orthodontic treatment | Additional details | |
| General physical adjunctive interventions | El‐Angbawi et al. [ | SR/MA |
–23 RCTs (parallel) –13 in MA: 1. LVF analysis: ✓ Overall orthodontic treatment duration ✓ Number of appliance adjustment visits ✓ Tooth movement rate during early alignment (4–6 weeks) ✓ Rate of space closure (En masse) 2. LLLT analysis: ✓ Alignment stage duration ✓ Number of visits during alignment ✓ Tooth movement rate during space closure (maxillary arch) 3. LED analysis: ✓ Alignment stage duration ✓ Tooth movement rate during space closure | 8–50 years |
Total: 1027 – VD: – SD: – LLLT: – PLA: – Con: |
Cochrane CD010887 |
Electronic databases (5) + manual search No restriction for language | Up to September 2022 |
ROB1 UROB: 2 RCTs HROB: 22 RCTs GRADE: LQE VLQE | AcceleDent (9 RCT) | 30 Hz/0.25 N/20 min/day |
LADC without EX: 2 RCTs LADC without EX: 1 RCT DR without EX: 3 RCT UCR: 3 RCTs | Used with FA and CA |
| Tooth Masseuse (1 RCT) | 111 Hz/0.06 N/20 min/day | LADC without EX: 1 RCTs | |||||||||||
| Tooth Bruch (1 RCT) | 30–60–120 Hz/0.001 N/20 min/day | UCR: 1 RCTs | |||||||||||
| Customized vibratory appliance (1 RCT) | 30 Hz/0.2 N/20 min/day | ER: 1 RCT | |||||||||||
| LLLT (10 RCT) |
635–980 nm/1–10 points/3–10 s per point Daily‐every 15–30 days SE/2.25–25.7 j/cm2/8–2500 mW |
LADC without EX: 5 RCTs UADC with EX: 2 RCTs ER: 1 RCT UI: 2 RCTs | |||||||||||
| LED (2 RCTs) |
640–850 nm/intraoral/5–20 min per day Daily SE/10–108 j/cm2/40–90 mW/cm2 |
LADC without EX: 1 RCTs UCR: 1 RCT | |||||||||||
| BES | Dutta et al. [ | SR/MA |
– 4 RCTs (3 SMD/1 parallel) – 2 of them in MA for the RCR in the third and fifth months | 18–24 years |
Total: 78 – BES – SD –Con |
Pro CRD42023495077 |
Electronic databases (4) + manual search Unclear restriction for language | Up to November 2023 |
ROB2 LROB: 1 RCT HROB: 3 RCTs GRADE: MQE | LIDEC (1 RCT/ SMD) |
20 μA (15 V)/5 h/day Upper canines | UCR: 1 RCT | Used with FA |
| PEMF (2 RCTs/ SMD) |
0.5 mT, 1 Hz/8 h/night Upper canines | UCR: 2 RCTs | |||||||||||
| BM (1 RCT/Parallel) |
10 μA/5 min/week Lower incisors | LADR: 1 RCT | |||||||||||
| Vibration devices | Aljabaa et al.[ | SR | – 6 RCTs (parallel) | 11.1–40 years |
Total: 339 – VD – SD – Con | Not registered |
Electronic databases (3) + manual search No restriction for language | Up to March 2018 |
ROB 1: ROB: 4 RCTs HROB: 2 RCTs | AccelDent 5RCTs | 30 Hz/0.2 N/20 min/day |
– UCR: 1 RCT ER: 1 RCT – LADC with EX: 1 RCT – LADC without EX: 1 RCT – DR without EX: 1 RCT | – Used with FA (5 RCTs) and CA (1 RCT) |
| Tooth Masseuse 1RCT | 111 Hz/0.06 N/20 min/day | – LADC without EX: 1 RCT | |||||||||||
| Abd Elmotaleb et al. [ | SR/MA |
– 6 RCTs (parallel) – 3 of them in MA (LII) | 11–40 years |
Total: 232– VD – SD – Con | At the Evidence‐Based Center, in their faculty (Registration number: 14–2018) |
Electronic databases (3) + manual search English only | Up to July 2018 |
ROB 1: LROB: 2 RCTs HROB: 4 RCTs | AcceleDent 5 RCTs | 30 Hz/0.2 N/20 min/day |
– LADC with EX: 1 RCT – LADC without EX: 1 RCT – UCR: 1 RCT ER: 2 RCTs | – Used with FA (6 RCTs) | |
| Tooth Masseuse 1RCT | 111 Hz/0.06 N/20 min/day | – LADC without EX: 1 RCT | |||||||||||
| Bakdach et al. [ | SR | – 17 RCTs (14 parallel/ 3 SMD) | 12–33 years |
Total: 730– VD – SD – Con | Not registered |
Electronic databases (7) + manual search No restriction for language | Up to November 2019 |
ROB 1:LROB 5 RCTs UROB: 11 RCTs HROB: 1 RCT | AcceleDent 12 RCTs | 30 Hz/20 min/day |
– LADC with EX: 1 RCT – LADC without EX: 2 RCTs – DR without EX: 5 RCT – UCR: 2 RCTs – ER: 2 RCTs | – Used with FA (12 RCTs) and CA (5 RCTs) | |
| Electric Toothbrush 3 RCTs |
125 Hz/20 min/day 125 Hz/15 min/day 113 Hz/10 min/day | – UCR: 3 RCTs | |||||||||||
| VPro5 1 RCT | 120 Hz/5 min/day | – LADC without EX: 1 RCT | |||||||||||
| Tooth Masseuse 1 RCT | 111 Hz/20 min/day | – LADC without EX: 1 RCT | |||||||||||
| Keerthana et al. [ | SR/MA |
– 12 RCTs (9 parallel/3 SMD) – 8 of them in MA (RTM) | 12–40 years |
Total: 526– VD – SD – Con |
PROSPERO CRD42020169675 |
Electronic databases (3) + manual search English only | Up to Jan 31, 2020 |
ROB 1: UROB: 2 RCTs HROB: 8 RCTs Grade: MQE: (9 RCTs) HQE: (1 RCT) | AcceleDent 7 RCTs | 30 Hz/0.2 N/20 min/day |
– LADC with EX: 1 RCT – LADC without EX: 1 RCT – DR without EX: 1 RCT – UCR: 2 RCTs – ER: 2 RCTs | – Used with FA (11 RCTs) and CA (1 RCTs) | |
| Electric toothbrush 4 RCTs |
50 Hz/0.2 N/10 min/day 30 Hz–60 Hz–120 Hz/0.001 N/20 min/day 100–105 Hz/5 min/day | – UCR: 4 RCTs | |||||||||||
| Tooth Masseuse 1 RCT | 30 Hz/0.2 N/20 min/day | – LADC without EX: 1 RCT | |||||||||||
| García Vega et al. [ | SR | – 15 RCTs (11 parallel/ 4 SMD) | 11–45 years |
Total: 670– VD – SD – Con |
PROSPERO CRD42021245217 |
Electronic databases (6) + manual search English only | From 2010 to June 2021 |
ROB 1: LROB: 3 RCTs UROB: 5 RCTs HROB: 7 RCT Grade: LQE: 15 RCTs | AcceleDent 7 RCTs | 30 Hz/0.2 N/20 min/day |
– LADC with EX: 1 RCTs – LADC without EX: 1 RCTs – DR without EX: 2 RCT – UCR: 2 RCTs – ER: 1 RCTs | – Used with FA (12 RCTs) and CA (3 RCTs) | |
| Electric Toothbrush 5 RCTs |
50 Hz/0.2 N/10 min/day 30 Hz–60 Hz–120 Hz/0.001 N/20 min/day 100–105 Hz/5 min/day 125 Hz/5 min/day | – UCR: 5 RCTs | |||||||||||
| VPro5 1 RCT | 120 Hz/0.0003 N/5 min/day | – LADC without EX: 1 RCT | |||||||||||
| Tooth Masseuse 1 RCT | 111 Hz/0.06 N/20 min/day | – LADC without EX: 1 RCTs | |||||||||||
| Customized appliance 1 RCTs | 30 Hz/0.2 N/20 min/day | – ER: 1 RCTs | |||||||||||
| Dutta et al. [ | SR/MA |
– 21 RCTs (14 parallel/ 7 SMD) – 14 of them in MA (5 for LII / 6 for CRR | 12–40 years |
Total: 815 – VD – SD – Con |
PROSPERO CRD42024542014 |
Electronic databases (5) + manual search No restriction for language | Up to April 2024 |
ROB 2: LROB: 3 RCTs SROB: 18 RCTs Grade: MQE: 14 RCTs | AcceleDent 9 RCTs | 30 Hz/0.2 N/20 min/day |
– LADC with EX: 1 RCTs – LADC without EX: 2 RCTs – DR without EX: 1 RCT – UCR: 3 RCTs – ER: 2 RCTs | – Used with FA (19 RCTs) and CA (2 RCTs) | |
| Electric Toothbrush 5 RCTs |
50 Hz/0.2 N/10 min/day 30 Hz–60 Hz–120 Hz/0.001 N/20 min/day 100–105 Hz/5 min/day 125 Hz/5 min/day | – UCR: 5 RCTs | |||||||||||
| VPro5 1 RCT | 120 Hz/0.0003 N/5 min/day | – LADC without EX: 1 RCT | |||||||||||
| Tooth Masseuse 1 RCT | 111 Hz/0.06 N/20 min/day | – LADC without EX: 1 RCTs | |||||||||||
| Customized appliance 5 RCTs |
30 Hz/0.2 N/20 min/day 102 Hz/0.05 N/3 min/visit 125–150 Hz/1 min/tooth |
– LADC without EX: 1 RCTs – UCR: 2 RCTs – ER: 2 RCTs | |||||||||||
| Photobiomodulation | Almeida et al. [ | SR/MA |
– 6 RCTs (SMD) – 5 of them in MA for the CRR | 10.5–23 years |
Total: 73 – LLLT – PLA – Con |
PROSPERO CRD42015025009 |
Electronic databases (6) No restriction for language | Up to September 2015 |
Selection criteria and scores, adapted from Cericato et al. MQ: 1 RCT HQ: 5 RCTs |
LLLT 6 RCTs (6 SMD) GaAlAs: 5 RCTs GaAs: 1 RCT |
NA/3–5 points/NA 3–8 SE/4.2–10 (J/cm²)/NA |
UCR: 3 RCTs U&LCR: 3 RCTs | – Used with FA |
| Imani et al. [ | SR/MA |
– 6 RCTs (SMD) – 6 in MA for the CRR | 10.5–31 years |
Total: 96 – LLLT – PLA – Con | Not registered |
Electronic databases (5) No restriction for language | Up to October 2017 |
ROB 1: UROB: 5 RCTs HROB: 1 RCT |
LLLT 6 RCTs (6 SMD) GaAlAs |
780–940 nm/NA/3–10 s per point 3–17 SE/5–8 (J/cm² per point)/20–200 mW |
UCR: 4 RCTs U&LCR: 2 RCTs | – Used with FA | |
| Deana et al. [ | SR/MA |
16 RCTs (2 parallel/ 14 SMD) – 12 of them in MA for the CRR per month/Accumulated OTM rate | 10.5–31 years |
Total: 273 – LLLT – PLA – Con | Not registered |
Electronic databases (4) + manual search Language restrictions (English/Spanish/Portuguese) | Up to March 2018 |
ROB 1: UROB: 9 RCTs HROB: 7 RCTs Grade: VLQE/LQE/MQE |
LLLT 16 RCTs (2 parallel/14 SMD) GaAlAs: 15 RCTs GaAs: 1 RCTs |
780–980 nm/4–10 points/3–30 s per point 1–17 SE/33–214 (J/cm²)/0.25–200 mW |
UCR: 8 RCTs U&LCR: 5 RCTs – UADC with EX: 1 RCTs – LADC without EX: 1 RCTs – ER: 1 RCTs | – Used with FA | |
| Bakdach et al. [ | SR/MA |
25 RCTs (7 parallel/18 SMD) – 17 MA studies: upper CR/month; 5 included lower canines | 12–40 years |
Total: 570 – LLLT – PLA – Con | Not registered |
Electronic databases (9) + manual search No restriction for lg | Up to June 2019 |
ROB 1: LROB: 4 RCTs UROB: 17 RCTs HROB: 4 RCTs Grade: LQE/VLQE |
LLLT 20 RCTs (3 Parallel/17 SMD) GaAlAs: 19 RCTs GaAs: 1 RCTs |
780–980 nm/4–10 points/3–30 s per point 3–17 SE per month/2.25–150 (J/cm²)/0.25–1000 mW |
– LADC without EX: 1 RCTs. – UADC with EX: 1 RCTs – DR without EX: 1 RCT UCR: 10 RCTs U&LCR: 7 RCTs | – Used with FA (24 RCTs) and CA (1 RCTs) | |
| LED 5 RCTs (4 parallel/1SMD) | 618–850 nm/NA (extra ‐intra oral)/3–20 min per session 21–180 SE/ 0.063–108 (J/cm²)/20–90 mW/cm² |
– LADC without EX: 1 RCTs – UADC with EX: 1 RCTs – DR without EX: 1 RCT UCR: 1 RCTs – ER: 1 RCTs | |||||||||||
| Camacho et al. [ | SR |
9 RCTs (1 parallel/8 SMD) | 12–35 years |
Total: 126– LLLT – PLA – Con |
PROSPERO CRD42019117648 |
Electronic databases (4) + manual search English only | From January 2001 to February 2018 |
ROB 1: UROB: 2 RCTs HROB: 7 RCTs |
LLLT 9 RCTs (1 Parallel/8 SMD) |
670–904 nm/NA/NA 2–9 SE/NA/12–200 mW |
UCR: 3 RCTs U&LCR: 3 RCTs – UADC with EX: 1 RCTs – UPR: 1 RCTs – ER: 1 RCTs | – Used with FA | |
| Grajales et al. [ | SR/MA |
19 RCTs (1 parallel/18 SMD) – 18 of them in MA: UCRR/month Linking WL and energy to accelerated OTM | 10–35 years |
Total: 311 – LLLT – PLA – Con | PROSPERO CRD42022332585 |
Electronic databases (4) + manual search No restriction for language | Up to October 2022 |
ROB 2: LROB: 2 RCTs SROB: 17 RCTs | LLLT 19 RCTs (1 parallel/18 SMD) |
658–980 nm/4–10 points/3–23 s per point 3–17 SE/4.2–25 (J/cm²)/NA |
UCR: 10 RCTs U&LCR: 7 RCTs – ER: 2 RCTs | – Used with FA | |
| Jnaneshwar et al. [ | SR/MA |
10 RCTs (3 Parallel/7 SMD) – 6 of them in MA (4 UCRR/2 Anterior Alignment) | 12–24 years |
Total: 223 – LLLT – PLA – Con | PROSPERO CRD42020196472 |
Electronic databases (5) + manual search No restriction for language | Up to June 2020 |
ROB 1: LROB: 3 RCTs UROB: 7 RCTs GRADE: HQE MQE |
LLLT 8 RCTs (2 Parallel/6 SMD) |
808–980 nm/4–10 points/10–184 s per point or tooth 3–15 SE/7.5–150 (J/cm²)/20–1000 mW |
– LADC without EX: 1 RCTs. – UADC with EX: 1 RCTs. U&LCR: 2 RCTs UCR: 4 RCTs | – Used with FA | |
|
LED 2 RCTs (1 parallel/1 SMD) |
618–850 nm/NA (extra–intra oral)/20 min per day Daily SE/150 (J/cm²)/20–90 (mW/cm²) |
– LADC without EX: 1 RCTs. UCR: 1 RCTs | |||||||||||
| Malik et al. [ | SR/MA |
6 RCTs (4 Parallel/2 SMD) – 2 of them in MA: UCRR/month | Not available |
Total: NA – LLLT – PLA – Con | Not registered |
Electronic databases (5) English only | Not available |
ROB 1: LROB: 4 RCTs HROB: 2 RCTs |
LLLT 4 RCTs (2 Parallel/2 SMD) |
810–980 nm/4–6 points/8–30 s per point Variable SE (monthly to daily)/5–150 (J/cm²)/100–1000 mW |
– LADC without EX: 1 RCTs – UADC with EX: 1 RCTs U&LCR: 2 RCTs | – Used with FA | |
|
LED 2 RCTs (2 parallel) |
850 nm/NA (extra–intra oral)/5–20 min per day Daily/0.065–108 (J/cm²)/65 mW–90 (mW/cm²) |
– LADC without EX: 1 RCTs – UADC without EX: 1 RCTs | |||||||||||
| Hmida et al. [ | SR | 14 RCTs (5 parallel/9 SMD) | Mean age 13.4–21.5 years |
Total: 416 – LLLT – PLA – Con | Not registered |
Electronic databases (3) + manual search English only | Up to October 15, 2023 |
ROB 2: LROB: 10 RCTs SROB: 4 RCTs GRADE: HQE: 6 RCTs/ MQE: 8 RCTs |
LLLT 11 RCTs (11 SMD) |
810–980 nm/4–10 points/3 s per point‐80 s per aspect 3–16 SE/25.7–150 (J/cm2)/100 mW |
LADR without EX:1 RCT UADR with EX: 1 RCT DR without EX:1 RCT UCR: 6 RCTs U&LCR: 1 RCT UER: 1 RCT | – Used with FA | |
| LED 3 RCTs (3 SMD) |
450–850 nm/NA (extra‐intra oral)/10–20 min per day Daily‐Biweekly SE/36–144 (J/cm2/session)/60 mW/cm² |
LADR: 2 RCTs UCR: 1 RCT | |||||||||||
| Intervention type | Study ID/author, year, country | Outcomes | Ethics and funding | |||||
|---|---|---|---|---|---|---|---|---|
| Primary outcomes | Outcome measurement tools | Follow‐up period | MA reported outcomes | Descriptive reported outcomes | Source of funding | Declared conflicts of interest | ||
| General physical adjunctive interventions | El‐Angbawi et al. [ |
✓ Overall orthodontic treatment duration ✓ Number of appliance adjustment visits ✓ Rate of tooth movement during treatment phases (alignment, space closure) |
✓ Time documentation (in months) ✓ Clinic records ✓ LII for malalignment measurement ✓ SC: mm per month on study models |
✓ Duration: VD: 4–16 weeks LLLT: 6–12 weeks LED: 3–6 months ✓ Frequency: VA: 4–6 weeks LLLT: every 2 weeks, 4 per month LED: 20 min daily ✓ Focus: Short‐term effects only |
Light Vibrational Forces (LVF) Analysis: 1. Overall orthodontic treatment duration (2 RCTs/77 PT): ◦ No significant difference found (MD: −0.61 months; 95% CI: −2.44 to 1.22) 2. Number of appliance adjustment visits (2 RCTs/77 PT): ◦ No reduction observed (MD: −0.32 visits; 95% CI: −1.69 to 1.05) 3. Tooth movement rate during early alignment (4–6 weeks) (3 RCTs/144 PT): ◦ No acceleration detected (MD: 0.12 mm; 95% CI: −1.77 to 2.01) 4. Rate of space closure (En masse) (2 RCTs/81 PT): ◦ Minimal clinical effect (MD: 0.10 mm/month; 95% CI: −0.08 to 0.29) 5. Rate of canine retraction = (2 RCTs/40 PT): ◦ No acceleration detected (MD: −0.01 mm/month; 95% CI: −0.20 to 0.18) Low‐Level Laser Therapy (LLLT) Analysis: 1. Alignment stage duration (3 RCTs/92 PT): ◦ Statistically significant reduction (MD: −48.87 days; 95% CI: −56.48 to −41.26) 2. Number of visits during alignment (2 RCTs/125 PT): ◦ Reduction observed (MD: −2.25 visits; 95% CI: −2.52 to −1.97) Light‐Emitting Diode (LED) Analysis: 1. Alignment stage duration (1 RCTs/34 PT): ◦ Reduction observed (MD: −24.5 days; 95% CI: −42.45 to −6.55) 2. Tooth movement rate during space closure (1 RCTs/39 PT): ◦ No significant difference (MD: 0.006 mm/day; 95% CI: 0 to 0.02) | — |
SR: NF PS: Katchooi et al. [ Funded by OrthoAccel Technologies (manufacturer of vibrational devices like Acceledent). |
SR: NC PS: Funding from OrthoAccel Technologies creates a potential conflict of interest (COI) in the cited studies (Katchooi et al. [ |
| BES | Dutta et al. [ |
UCR (mm/month) Decrowding DR |
✓ RCR: Digital calipers (millimeter measurements between teeth/anchors) ✓ LII (crowding severity scoring) |
✓ Duration: Ranged from 4 weeks to 5 months One study continued until treatment completion ✓ Frequency: Weekly Monthly Pre‐ and post‐treatment only ✓ Focus: Short‐term effects only |
• Positive correlation between electrical stimulation and accelerated orthodontic tooth movement (30–40% faster movement in some studies) • Meta‐analysis results: – 3rd month (2 RCTs/29 PT): Standardized Mean Difference (SMD) = 0.69 (95% CI: −1.26 to 0.12), – 5th month (2 RCTs/29 PT): SMD = 1.64 (95% CI: −3.44 to 0.16), | — | NF | NC |
| Vibration devices | Aljabaa et al. [ |
RTM DR/CR/SC |
✓ LII On study models by Digital caliper ✓ RCR: mm per month, Direct in the patient’s mouth by Digital caliper ✓ SC: mm per month on study models by Digital caliper |
✓ Initial alignment studies: 8 weeks–7 months. ✓ CRR: until canine retraction ✓ SC: 10 weeks–6 months | — |
• Tooth Movement: 1/6 studies (Pavlin et al. [ 5/6 studies found no significant difference • Pain: No reduction in 3/3 studies (except reduced analgesic use in Miles & Fisher) |
SR: NF PS: ✓ Pavlin et al. [ ✓ Katchooi et al. [ ✓ Woodhouse et al. [ |
SR: NC PS: ✓ Pavlin et al. [ ✓ Katchooi et al. [ ✓ Woodhouse et al. [ |
| Abd Elmotaleb et al. [ |
RTM CR/DR/SC |
✓ LII On study models by Digital caliper ✓ RCR: mm per month, directly in the patient’s mouth by digital caliper. ✓ SC: mm per month on study models by Digital caliper | 10–18 weeks (short‐term) | • LII (3 RCTs/162 PT): no significant difference between vibration and control groups (MD: −0.24 mm, 95% CI: −0.92 to 0.45, | — |
SR: NM PS: Pavlin et al. [ |
SR: NC PS: Pavlin et al. [ | |
| Bakdach et al. [ |
RTM DR/CR/SC |
✓ LII On plaster models by digital caliper or on digital models ✓ PCPD ✓ Tracking Percentage ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster models by Digital caliper ✓ SC: mm per month on study models |
✓ Short‐Term: 3–12 weeks (e.g., canine retraction studies). ✓ Long‐Term: Up to 12 months (e.g., alignment studies). ✓ Variable: Some studies followed patients until specific milestones (e.g., complete crowding resolution) | — |
• 30 Hz (20 min/day): No significant acceleration in most studies (12 RCTs) • 113 Hz (10 min/day): Significant acceleration in CRR (1 RCT) • 120 Hz (5 min/day): Reduced aligner change intervals (1 RCT) • 125 Hz (15 min/day): Faster CRR (1 RCT) • Pain Reduction: Mixed results: Some studies reported reduced pain with vibration | NF | NC | |
| Keerthana et al. [ |
RTM DR/CR/SC |
✓ LII On plaster models by digital caliper or on digital models ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster/ digital models ✓ SC: mm per month on study models by digital caliper |
✓ Short‐Term Monitoring (Days to Weeks): Measured outcomes from 0 days (immediate) up to 3 months (e.g., 24 h, 48 h, weekly, or 4–12‐week intervals). ✓ Medium‐Term Monitoring (Weeks to Months): Tracked changes at 5–10‐week intervals or monthly evaluations until treatment completion ✓ Long‐Term Monitoring (Until Treatment Completion): Follow‐up until final outcomes | • (10 RCTs/310 PT): 30 Hz vibratory devices (e.g., AcceleDent, powered toothbrushes) accelerate orthodontic tooth movement (mean difference: 0.34 mm, 95% CI: 0.25–0.42, | — | NM | NC | |
| García Vega et al. [ |
RTM DR/CR/SC |
✓ LII On plaster models by digital caliper or on digital models ✓ Tracking Percentage ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster/digital models ✓ SC: mm per month on study models by digital caliper |
Varied Durations: ✓ Ranged from 5 days to full treatment completion (e.g., space closure or alignment) ✓ Common intervals: 10 weeks, 3 months, 60 days, and 1‐month post‐vibration | — |
• Limited Evidence: Most studies had high or moderate risk of bias, with only 4 out of 15 suggesting vibrations might accelerate tooth movement • No Clear Benefit: Current evidence does not conclusively show that vibrations increase tooth movement speed, reduce alignment time, or improve canine retraction • Method Issues: Variations in devices, vibration types, and short follow‐up periods weaken the reliability of results • Future Needs: High‐quality, standardized trials (especially for high‐frequency vibrations) with longer follow‐up are critical to confirm effectiveness |
M Institutional resources of the Meritorious Autonomous University of Puebla funded this research | NC | |
| Dutta et al. [ |
RTM DR/CR/SC |
✓ LII On plaster models by digital caliper or on digital models ✓ Tracking Percentage ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster/digital models ✓ SC: mm per month on plaster or digital models by digital caliper |
✓ Most studies: 3–6 months (tooth movement and pain tracking) ✓ Initial alignment studies: 8–12 weeks ✓ CRR/ SC studies: 3–12 months (case‐dependent) ✓ Aligner studies: 3–9 months (with aligner changes every 7–14 days) |
• LII (5 RCTs/209 PT): No significant difference between vibration and control groups (SMD = 0.16, CI: −0.11 to 0.43, • RCR (6 RCTs/244 PT): Significant improvement in the vibration group (SMD = 2.48, CI: 0.90–4.07, • Pain (VAS) (3 RCTs/144 PT): No significant reduction in pain (SMD = −0.31, CI: −0.68 to 0.06, | — | NF | NC | |
| Photobiomodulation | Almeida et al. [ |
RCR (U/L) (mm/month) | ✓ RCR: mm per month, directly in the patient’s mouth by digital caliper |
✓ Duration: 1–4.5 months (varied across studies) ✓ Frequency: Monthly measurements (tracked movement over 3–4.5 months) ✓ Focus: Short‐term effects only; long‐term outcomes not assessed |
RCR (5 RCTs/63 PT): • Maxilla: Significant acceleration (0.33 mm difference, • Mandible: Significant acceleration (1.03 mm difference, • No overall acceleration: No consistent evidence across time points • No clear benefit of LLLT for accelerating orthodontic tooth movement | — | NF | NC |
| Imani et al. [ |
RCR (U/L) (mm/month) | ✓ Undefined |
✓ Duration: Measurements taken at 6 intervals: 21 days, 1 month, 1.5 months, 2 months, 3 months, and 4.5 months ✓ Frequency: varied per study ✓ Focus: Short‐term effects only; long‐term outcomes not assessed |
• Tooth Movement Distance (mm): Significant increase in LLLT group vs. control at all intervals: ✓ 21 days (2 RCTs/33 PT): MD = 0.74 (95% CI: 0.17–1.31; ✓ 1 month (4 RCTs/59 PT): MD = 0.40 (95% CI: 0.10–0.69; ✓ 1.5 months (1 RCTs/11 PT): MD = 0.72 (95% CI: 0.51–0.93; ✓ 2 months (2 RCTs/44 PT): MD = 0.84 (95% CI: 0.23–1.44; ✓ 3 months (3 RCTs/48 PT): MD = 0.92 (95% CI: 0.06–1.78; ✓ 4.5 months (1 RCTs/20 PT): MD = 1.53 (95% CI: 0.92–2.14; • LLLT significantly speeds up canine movement and reduces treatment time | — | NM | NC | |
| Deana et al. [ | OTM acceleration, monthly/accumulated rates, and ED efficacy |
✓ LII On plaster models by digital caliper or on digital models ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster models by Digital caliper Reference wires and palatal plugs 3D models/visual assessments ✓ SC: mm per month on study models |
✓ Duration: CR: 8 weeks–10 months Alignment: not explicitly specified ✓ Frequency: Weekly, biweekly, or monthly ✓ Focus: Short‐term OTM acceleration |
RCR: • First month OTM (3 RCTs/38 PT): ED 50–75 J/cm²: MD 0.58 mm (95% CI: 0.36–0.80; • Second month OTM (2 RCTs/23 PT): ED 50–75 J/cm²: MD 0.41 mm (95% CI: 0.14–0.68; • Accumulated OTM (4 RCTs/59 PT): ED 50–75 J/cm²: MD 1.40 mm (95% CI: 0.94–1.85; • No significant acceleration with ED 33–42 J/cm² or 200–214 J/cm² • PBMT with 50–75 J/cm² per tooth significantly accelerates OTM in the short term | — | NF | NC | |
| Bakdach et al. [ |
RTM CR Alignment time SC velocity |
✓ LII On plaster models by digital caliper or on digital models ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster models by Digital caliper Reference wires and palatal plugs 3D models/visual assessments ✓ SC: mm per month on study models |
✓ Duration: Ranged from 8 weeks to 6 months ✓ Frequency: Weekly, biweekly, or monthly ✓ Focus: Short‐term acceleration |
Upper CR: • Month 1 (9 RCTs/113 PT): No significant difference (WMD = 0.21 mm, 95% CI [−0.09, 0.51], • Month 2 (12 RCTs/168 PT): Significant acceleration (WMD = 0.50 mm, 95% CI [0.29, 0.72], • Month 3 (6 RCTs/89 PT): Significant acceleration (WMD = 0.49 mm, 95% CI [0.02, 0.96], Lower CR: • Month 1 (3 RCTs/34 PT): No significant difference (WMD = 0.56 mm, 95% CI [−0.37, 1.50], • Month 2 (5 RCTs/74 PT): Significant acceleration (WMD = 0.28 mm, 95% CI [0.17, 0.40], • Month 3 (3 RCTs/42 PT): Significant acceleration (WMD = 0.52 mm, 95% CI [0.40, 0.63], – LLLT accelerates tooth movement, but clinical significance is questionable (low‐quality evidence) – No consensus on optimal laser dosage (Recommendation: report total joules/month instead of J/cm²) | — | NF | NC | |
| Camacho et al. [ |
RTM CR PR Alignment time |
✓ LII On plaster models by digital caliper or on digital models ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster/digital models/Stereomicroscope |
✓ Duration: Ranged from 45 days to 3–4 months. ✓ Frequency: varied between 2 and 9 sessions, typically administered weekly or biweekly ✓ Focus: Short‐term acceleration | — |
• 780–830 nm: Most studies showed significant tooth movement acceleration within this range • 24% increase in tooth movement speed compared to control groups (calculated across 9 studies) • 780–809 nm: Highest acceleration rates (up to 34–54% in specific studies) • 830–860 nm: Moderate acceleration (e.g., 26% reduction in treatment time) • > 900 nm: No significant effect (e.g., 904 nm) | NF | NC | |
| Grajales et al. [ |
RTM CR ER |
✓ RCR: mm per month, Direct in the patient’s mouth or on plaster/ digital models ✓ SC: mm per month on study models by digital caliper |
✓ Duration: 3–4 months ✓ Frequency: Varied: Weekly, biweekly, or monthly ✓ Focus: Short‐term acceleration |
Upper CR: ✓ Significant acceleration in LLLT groups during months 1–3: – Month 1 (12 RCTs/143 PT): OR = 0.28 (95% CI: 0.07–0.48) – Month 2 (13 RCTs/181 PT): OR = 0.52 (95% CI: 0.31–0.73) – Month 3 (10 RCTs/143 PT): OR = 0.41 (95% CI: 0.03–0.79) – Month 4 (3 RCTs/51 PT): No significant difference (OR = 0.41, 95% CI: −0.11 to 0.94) • Wavelength ≤810 nm and energy density ≤5.3 J/cm² showed statistically significant acceleration (subgroup analysis) | — | NF | NC | |
| Jnaneshwar et al. [ |
RTM CR Alignment time |
✓ LII On plaster models by digital caliper or on digital models ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster models by Digital caliper |
✓ Duration: Not explicitly mentioned in most studies ✓ Frequency: Varied: Weekly, biweekly, or monthly ✓ Limitations: No long‐term follow‐up ✓ Focus: Short‐term acceleration |
• RCR: – (4 RCTs/ 48 PT): LLLT applied ≥4 times in the first month significantly increased OTM (SMD = 0.46 mm, • Reduced Alignment Duration: – (2 RCTs/60 PT): LLLT reduced anterior alignment time by 25.58 days ( | — | NF | NC | |
| Malik et al. [ |
RTM CR Alignment time |
✓ LII On plaster models by digital caliper or on digital models ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster models by Digital caliper |
✓ Duration: Varied: 67 days–6 months ✓ Frequency: Varied: Weekly, biweekly, or monthly ✓ Limitations: ✓ Focus: Limitations: No long‐term follow‐up ✓ Focus: Short‐term acceleration |
(OTM) Rate (6 RCTs): • Significant acceleration observed in OTM starting from the 2nd month (WMD = 0.50 mm, • No significant difference in the 1st month (WMD = 0.20 mm, 95% CI: −0.09 to 0.51, | — | NF | NC | |
| Hmida et al. [ |
RTM CR Alignment time |
✓ LII On plaster models by digital caliper or on digital models ✓ RCR: mm per month, Direct in the patient’s mouth or on plaster models by Digital caliper |
✓ Duration: Short‐Term (1–3 months) Medium‐Term (3–7 months) Variable/Unspecified ✓ Frequency: Weekly, biweekly, monthly, or mixed intervals | — |
• Efficacy: 12 out of 14 studies demonstrated that PBM accelerates orthodontic tooth movement by 12.5%–40% and reduces treatment duration by 22%–26% • Heterogeneity: Varied treatment parameters (e.g., 810–980 nm wavelength, sessions 3–16) | NM | NM | |
| Domains | General PAI | BES | VDs | PBM | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| El‐Angbawi et al. [ | Dutta et al. [ | Aljabaa et al. [ | Abd Elmotaleb et al. [ | Bakdach et al. [ | Keerthana et al. [ | García Vega et al. [ | Dutta et al. [ | Almeida et al. [ | Imani et al. [ | Deana et al. [ | Bakdach et al. [ | Camacho et al. [ | Grajales et al. [ | Jnaneshwar et al. [ | Malik et al. [ | Hmida et al. [ | |
| 1. Did the research questions and inclusion criteria for the review include the components of PICO? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 2. Did the report of the review contain an explicit statement that the review methods were established prior to the conduct of the review and did the report justify any significant deviations from the protocol? | Yes | Partial Yes | No | Partial Yes | No | Partial Yes | Partial Yes | Yes | Partial Yes | No | No | No | Partial Yes | Partial Yes | Yes | No | No |
| 3. Did the review authors explain their selection of the study designs for inclusion in the review? | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 4. Did the review authors use a comprehensive literature search strategy? | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | ||
| 5. Did the review authors perform study selection in duplicate? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 6. Did the review authors perform data extraction in duplicate? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | No | No |
| 7. Did the review authors provide a list of excluded studies and justify the exclusions? | Yes | No | Yes | No | Yes | Partial Yes | Yes | No | No | No | No | Yes | Yes | Yes | No | No | No |
| 8. Did the review authors describe the included studies in adequate detail? | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 9. Did the review authors use a satisfactory technique for assessing the risk of bias (RoB) in individual studies that were included in the review? | Yes | Partial Yes | Yes | Partial Yes | Partial Yes | Partial Yes | Partial Yes | Yes | Partial Yes | Yes | Partial Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| 10. Did the review authors report on the sources of funding for the studies included in the review? | Yes | No | Yes | Yes | No | No | No | No | No | No | No | Yes | No | No | No | No | No |
| 11. If meta‐analysis was performed did the review authors use appropriate methods for statistical combination of results? | Yes | Yes | No meta‐analysis conducted | Yes | No meta‐analysis conducted | Yes | No meta‐analysis conducted | Yes | Yes | Yes | Yes | Yes | No meta‐analysis conducted | Yes | Yes | Yes | No meta‐analysis conducted |
| 12. If meta‐analysis was performed, did the review authors assess the potential impact of RoB in individual studies on the results of the meta‐analysis or other evidence synthesis? | No | No | No meta‐analysis conducted | No | No meta‐analysis conducted | No | No meta‐analysis conducted | No | No | No | No | Yes | No meta‐analysis conducted | No | No | No | No meta‐analysis conducted |
| 13. Did the review authors account for RoB in individual studies when interpreting/ discussing the results of the review? | Yes | Yes | Yes | No | Yes | No | Yes | Yes | No | No | Yes | Yes | Yes | No | Yes | Yes | Yes |
| 14. Did the review authors provide a satisfactory explanation for, and discussion of, any heterogeneity observed in the results of the review? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes |
| 15. If they performed quantitative synthesis did the review authors carry out an adequate investigation of publication bias (small study bias) and discuss its likely impact on the results of the review? | No | Yes | No meta‐analysis conducted | No | No meta‐analysis conducted | Yes | No meta‐analysis conducted | Yes | No | No | No | Yes | No meta‐analysis conducted | No | No | No | No meta‐analysis conducted |
| 16. Did the review authors report any potential sources of conflict of interest, including any funding they received for conducting the review? | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Overall quality | LQ | LQ | LQ | CLQ | LQ | LQ | MQ | LQ | CLQ | CLQ | CLQ | LQ | MQ | CLQ | CLQ | CLQ | CLQ |
| Review | Phase 2 | Phase 3 | |||
|---|---|---|---|---|---|
| 1. Study eligibility criteria | 2. Identification and selection of studies | 3. Data collection and study appraisal | 4. Synthesis and findings | Risk of bias in the review | |
| El‐Angbawi et al. [ | ☺ | ☺ | ☺ | ☺ | ☺ |
| Dutta et al. [ | ☺ | ☺ | ☺ | ☹ | ☹ |
| Aljabaa et al. [ | ? | ☺ | ☺ | ☹ | ☹ |
| Abd Elmotaleb et al. [ | ☹ | ☹ | ☺ | ☹ | ☹ |
| Bakdach et al. [ | ? | ☺ | ☺ | ☹ | ☹ |
| Keerthana et al. [ | ☹ | ☹ | ☺ | ? | ☹ |
| García Vega et al. [ | ☹ | ☹ | ☺ | ☹ | ☹ |
| Dutta et al. [ | ☺ | ☺ | ☺ | ? | ? |
| Almeida et al. [ | ☹ | ? | ☹ | ☹ | ☹ |
| Imani et al. [ | ? | ? | ☺ | ☹ | ☹ |
| Deana et al. [ | ? | ☹ | ? | ☹ | ☹ |
| Bakdach et al. [ | ? | ☺ | ☺ | ? | ? |
| Camacho et al.[ | ☹ | ☹ | ☺ | ☹ | ☹ |
| Grajales et al. [ | ☺ | ☺ | ☺ | ☹ | ☹ |
| Jnaneshwar et al. [ | ☺ | ☺ | ☺ | ☺ | ☺ |
| Malik et al. [ | ☹ | ☹ | ☺ | ☹ | ☹ |
| Hmida et al. [ | ☹ | ☹ | ☺ | ☹ | ☹ |
| Intervention | VDs | Treatment effect | 95% CI | No. of primary trials | No. of events |
| ||
|---|---|---|---|---|---|---|---|---|
| Leveling & alignment | Mandible without extraction | Reduction in the LII (mm) | AcceleDent | 0.05 | −0.38, −0.49 | 5 RCTs [ | 150 | 0.808a |
| Tooth Masseuse | 0.60 | — | 1 RCT [ | 64 | >0.05 | |||
| Customized appliance | 0.83 | — | 1 RCT [ | 12 | =0.05 | |||
| Mandible with extraction | AcceleDent | 0.01 | −0.02, 0.03 | 1 RCT [ | 53 | 0.66 | ||
| Maxillary without extraction | AcceleDent | 0.21 | −0.52, 0.94 | 3 RCTs [ | 109 | 0.579a | ||
| Canine retraction | Mean CRR (mm/month) | AcceleDent | 0.27 | 0.19, 0.35 | 4 RCTs (49‐52) | 99 | <0.0001a | |
| Customized appliance | 0.15 | ‐0.03, 0.34 | 2 RCTs (58, 59) | 96 | 0.103a | |||
| Mean CR at different time points (mm) | 1st month | Tooth Bruch | 0.01 | −0.01, 0.02 | 3 RCTs [ | 132 | 0.428a | |
| 2nd month | 0.14 | −0.11, 0.40 | 3 RCTs [ | 132 | 0.274a | |||
| 3rd month | 0.11 | −0.11, 0.33 | 3 RCTs [ | 132 | 0.308a | |||
| Total CR (mm) | 0.67 | 0.01, 1.32 | 3 RCTs (54, 56, 57) | 112 | 0.045a | |||
| En masse retraction | Mean ERR (mm/month) | Total upper | AcceleDent | 0.05 | −0.23, 0.33 | 1 RCT [ | 40 | 0.73 |
| Upper right | Customized appliance | 0.19 | −0.25, 0.63 | 2 RCTs [ | 65 | 0.389a | ||
| Upper left | 0.29 | −0.44, 1.03 | 2 RCTs [ | 65 | 0.435a | |||
| Lower right | −0.020 | −0.103, 0.063 | 1 RCT [ | 45 | 1 | |||
| Lower left | ‐0.020 | −0.108, 0.069 | 1 RCT [ | 45 | 1 | |||
| Intervention | PBM | Treatment effect | 95% CI | No. of primary trials | No. of events |
| |||
|---|---|---|---|---|---|---|---|---|---|
| Leveling and Alignment | Mandible without extraction | OLAT (day) | LLLT | −58.42 | −88.64, −28.21 | 2 RCTs [ | 66 | 0.0002a | |
| LAIP (%) | Early alignment 4 weeks | 2.46 | −5.96, 27.76 | 2 RCTs [ | 56 | 0.481a | |||
| Early alignment 8 weeks | 7.58 | −7.25, 22.41 | 2 RCTs [ | 56 | 0.316a | ||||
| Early alignment 12 weeks | 6.70 | −5.48, 18.88 | 2 RCTs [ | 56 | 0.281a | ||||
| OLAT (day) | LED | −19.5 | −37.45, −1.55 | 1 RCT [ | 34 | 0.043 | |||
| MD = −57 | — | 1 RCT (68) | 89 | <0.001 | |||||
| Maxilla with extraction | OLAT (day) | LLLT | −28.00 | −39.34, −16.66 | 1 RCT [ | 26 | <0.001 | ||
| Maxilla without extraction | OLAT (day) | LED | −22.3 | — | 1 RCT [ | 26 | 0.028 | ||
| Both jaws without extraction | Alignment rate (mm/week) | LED | 0.63 | — | 1 RCT [ | 90 | <0.00001 | ||
| Effect of LLLT on daily wear time (hours) | LLLT | LLLT enhanced success Reducing aligner wear time from 22 to 12 hours/day. | — | 1 RCT [ | 21 | <0.001 | |||
| Upper Canine Retraction | Mean CRR (mm/day) | LED | 0.005 | −0.001, 0.012 | 1 RCT [ | 39 | 0.15 | ||
| Monthly CR (mm) | 1st month | 0.19 | −0.47, 0.86 | 2 RCTs [ | 78 | 0.569a | |||
| 2nd month | 0.06 | −0.09, 0.21 | 2 RCTs [ | 78 | 0.414a | ||||
| 3rd month | −0.06 | −0.59, 0.46 | 2 RCTs [ | 78 | 0.810a | ||||
| Monthly CR (mm) | 2nd month | LLLT | 0.27 | 0.08, 0.46 | 6 RCTs [ | 150 | 0.005a | ||
| 3rd month | 0.12 | −0.13, 0.37 | 4 RCTs [ | 90 | 0.351a | ||||
| 4th month | 0.52 | 0.14, 0.90 | 1 RCT [ | 20 | 0.03 | ||||
| Cumulative CR (mm from Baseline) | 21 days | 0.74 | 0.17, 1.31 | 2 RCTs [ | 66 | 0.011a | |||
| 1st month | 0.31 | 0.13, 0.49 | 14 RCTs [ | 354 | 0.0009a | ||||
| 2nd month | 0.72 | 0.18, 1.26 | 9 RCTs [ | 240 | 0.0089a | ||||
| 3rd month | 0.46 | 0.06, 0.86 | 6 RCTs [ | 202 | 0.02a | ||||
| Total CR ((mm) post‐treatment) | 1.08 | 0.33, 1.82 | 4 RCTs [ | 130 | 0.0046a | ||||
| Changes in canine position (mm) | 1st month | −0.13 | −0.58, 0.32 | 2 RCTs [ | 42 | 0.576a | |||
| 2nd month | −0.41 | −1.24, 0.41 | 2 RCTs [ | 42 | 0.325a | ||||
| 3rd month | −0.40 | −1.18, 0.39 | 2 RCTs [ | 38 | 0.321a | ||||
| 4th month | −0.67 | −1.99, 0.66 | 2 RCTs [ | 36 | 0.322a | ||||
| CRR (mm/month) | 0.66 | 0.36, 0.96 | 6 RCTs [ | 227 | <0.0001a | ||||
| Days to achieve space closure | 13.14 | — | 1 RCT [ | 82 | <0.001 | ||||
| Total CR without extraction (mm) | 0.63 | — | 1 RCT [ | 54 | 0.009 | ||||
| Lower Canine Retraction | Monthly CR (mm) | 1st month | LLLT | 1.03 | 0.67, 1.40 | 2 RCTs [ | 44 | <0.0001a | |
| 2nd month | −0.14 | −0.80, 0.51 | 2 RCTs [ | 44 | 0.668a | ||||
| 3rd month | −0.06 | −0.74, 0.61 | 2 RCTs [ | 44 | 0.852a | ||||
| CRR (mm/month) | 0.58 | 0.35, 0.81 | 3 RCTs [ | 120 | <0.0001a | ||||
| En Masse Retraction | Daily ER (mm/day) | LLLT | 0.04 | — | 1 RCT [ | 40 | <0.0001 | ||
| Monthly ERR (mm/month) | Total upper | 0.194 | — | 1 RCT [ | 24 | 0.017 | |||
| Upper right | 0.18 | 0.05, 0.3 | 1 RCT [ | 45 | 0.003 | ||||
| Upper left | 0.19 | 0.06, 0.32 | 1 RCT [ | 45 | 0.002 | ||||
| Lower right | 0.16 | 0.12, 0.19 | 1 RCT [ | 45 | <0.0001 | ||||
| Lower left | 0.185 | 0.13, 0.23 | 1 RCT [ | 45 | <0.0001 | ||||
| Monthly ERR (mm/month) | LED | 0.22 | 0.09, 0.49 | 1 RCT [ | 45 | 0.007 | |||
| Upper molars intrusion | Average at 6 months in adults | LLLT | −0.64 | — | 1 RCT [ | 20 | > 0.05 | ||
| Average at 7 months in children | 0.39 | — | 1 RCT [ | 28 | 0.018 | ||||
| Intervention | BES device | Treatment effect | 95% CI | No. of primary trials | No. of events |
| ||
|---|---|---|---|---|---|---|---|---|
| Leveling and alignment | Mandible without extraction | 3 months of crowding reduction (mm) | BM | 1.9 | — | 1 RCTs [ | 28 | <0.05 |
| Upper canine retraction | Cumulative CR (mm from baseline) | 1st month | LIDEC | 0.53 | — | 1 RCT [ | 14 | 0.001 |
| Total CR ((mm) post‐treatment) | PEMF | 1.78 | 0.99, 2.57 | 2 RCTs [ | 58 | <0.0001a | ||
| Interventions | Quality assessment criteria | Summary of findings | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. of studies | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | No. of patients | Effect | Overall quality of evidence | ||
| Accelerating leveling and alignment | ||||||||||
| Lower Jaw without extraction | Serious | Not serious | Not serious | Serious | None | 150 | Adding AcceleDent did not produce a clinically important speed‐up in lower‐arch alignment |
⨁⨁◯◯a Low | ||
| Using AcceleDent | 5 RCTs | |||||||||
| Using Tooth Masseuse | 1 RCT | Serious | Not serious | Not serious | Serious | None | 64 | Adding the Tooth Masseuse vibrating appliance did not produce a clinically important increase in the rate of lower‐front‐teeth alignment |
⨁⨁◯◯b Low | |
| Using a Customized appliance | 1 RCT | Serious | Not serious | Not serious | Serious | None | 12 | Adding the customized vibration appliance significantly increased the rate of lower‐front‐teeth alignment and reduced pain during initial leveling and alignment |
⨁⨁◯◯c Low | |
| Lower Jaw with extraction | Not serious | Not serious | Not serious | Serious | None | 53 | Adding AcceleDent did not produce a clinically important speed‐up in lower‐arch alignment | ⊕⊕⊕◯d Moderate | ||
| Using AcceleDent | 1 RCT | |||||||||
| Upper jaw without extraction | Serious | Not serious | Not serious | Serious | None | 56 | Adding AcceleDent did not produce a clinically important speed‐up in upper‐arch alignment |
⨁⨁◯◯e Low | ||
| Using AcceleDent | 3 RCTs | |||||||||
| Accelerating canine retraction | ||||||||||
| Using AcceleDent | Mean rate (mm/month) | 4 RCTs | Serious | Serious | Not serious | Very serious | None | 107 |
≈ 0.3 mm/month faster (MD = +0.27 mm/month; 95 % CI +0.19 to +0.35) | ⨁◯◯◯f Very low |
| Using a customized appliance | 2 RCTs | Serious | Serious | Not serious | Serious | None | 48 | Essentially, no clinically or statistically significant acceleration |
⨁◯◯◯g Very low | |
| Using tooth brush | Mean rate at different time points | 3 RCTs | Serious | Serious | Not serious | Serious | None | 66 | Essentially, no clinically or statistically significant acceleration | ⨁◯◯◯h Very low |
| Total canine retraction | 3 RCTs | Serious | Very serious | Not serious | Serious | None | 56 | +0.67 mm (0.01 to 1.32 mm) more retraction—favors vibration |
⨁◯◯◯i Very low | |
| Accelerating en‐masse retraction | ||||||||||
| Using AcceleDent | Mean rate (mm/month) | 1 RCT | Serious | Not serious | Not serious | Serious | None | 40 | Essentially, no clinically or statistically significant acceleration |
⨁⨁◯◯j Low |
| Using a customized appliance | 2 RCT | Serious | Very serious | Not serious | Serious | None | 65 | MD = 0.19 mm/month (95% CI −0.25 to 0.63)—an average gain of about two‐tenths of a millimeter per month, but the CI includes both slower and faster movement, so the difference is not statistically or clinically meaningful |
⨁◯◯◯k Very low | |
| Interventions | Quality assessment criteria | Summary of findings | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of studies | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | No. of patients | Effect | Overall quality of evidence | |||
| Accelerating leveling and alignment | |||||||||||
| Lower jaw without extraction | |||||||||||
| Using LLLT | OLAT | 2 RCTs | Serious | Serious | Not serious | Not serious | Large absolute benefit (≈ 2 months faster); no clear publication‐bias signals | 66 | LLLT shortened alignment time by 58 days (Mean Difference −58.4 days, 95 % CI −88.6 to −28.2) – statistically significant | ⨁⨁◯◯a Low | |
| LAIP | 2 RCTs | Serious | Not serious | Not serious | Serious | None | 56 | LLLT may slightly improve leveling and alignment improvement percentage (LAIP) compared to control, but without a statistically significant effect in the pooled analysis ( | ⨁⨁◯◯b Low | ||
| Using LED | OLAT | 1 RCT | Very serious | Not serious | Not serious | Serious | None | 34 | Mean difference −19.5 days (≈ 22 % faster alignment; | ⨁◯◯◯c Very low | |
| Upper jaw with extraction | |||||||||||
| Using LLLT | OLAT | 1 RCT | Serious | Not serious | Not serious | Serious | None | 26 | LLLT shortened OLAT by ≈ 28 days (MD = –28 days, 95% CI –39 to –17; | ⨁⨁◯◯d Low | |
| Upper jaw without extraction | |||||||||||
| Using LED | OLAT | 1 RCT | Serious | Not serious | Not serious | Serious | None | 26 | ≈ 22 days faster alignment with LLLT (41 d vs. 63 d; significant, | ⨁⨁◯◯e Low | |
| Both jaws without extraction | |||||||||||
| Using LLLT | Effect of LLLT on daily wear time (hours) | 1 RCT | Serious | Not serious | Not serious | Serious | Large effect size | 21 | LLLT enhanced success, reducing aligner wear time from 22 to 12 h/day | ⨁◯◯◯f Very low | |
| Using LED | Alignment rate (mm/week) | 1 RCT | Serious | Not serious | Not serious | Serious | Manufacturer funding may introduce publication bias | 90 | Mean difference ≈ +0.63 mm/week (1.12 vs. 0.49 mm/week). About 2.3× faster alignment; statistically significant ( | ⨁◯◯◯g Very low | |
| Accelerating upper canine retraction | |||||||||||
| Using LED | Mean rate (mm/day) | 1 RCT | Serious | Not serious | Very serious | Very serious | None | 39 | +0.006 mm day⁻¹ (≈ +0.18 mm month⁻¹) 95 % CI ‐0.001 → +0.012 mm day⁻¹, NS ( | ⨁◯◯◯h Very low | |
| Monthly retraction (mm) | 2 RCT | Serious | Serious | Not serious | Serious | None | 39 | LED may have little to no effect on monthly retraction rate; point estimates fluctuate (e.g. +0.19 mm [−0.47, 0.86] at 1st month; +0.06 mm [−0.09, 0.21] at 2nd month; −0.06 mm [−0.59, 0.46] at 3rd month), no statistically significant differences ( | ⨁⨁◯◯i Low | ||
| Using LLLT | Monthly retraction (mm) | 2nd month | 6 RCTs | Serious | Not serious | Not serious | Not serious | None | 75 | At 2nd month: LLLT increased monthly canine retraction by 0.27 mm (95% CI: 0.08 to 0.46), | ⨁⨁⨁◯j Moderate |
| 3rd month | 4 RCTs | Serious | Serious | Not serious | Serious | None | 45 | At 3rd month: increase of 0.12 mm (95% CI: −0.13 to 0.37), | ⨁⨁◯◯k Low | ||
| Cumulative retraction (mm from baseline) | 21 days | 2 RCTs | Serious | Serious | Not serious | Serious | None | 33 | Use of LLLT may accelerate cumulative upper canine retraction by approximately 0.74 mm more than control over 21 days | ⨁⨁◯◯l Low | |
| 1st month | 14 RCTs | Serious | Serious | Not serious | Serious | None | 177 | LLLT likely increased monthly canine retraction by ~0.3 mm (95% CI: 0.13 to 0.49), statistically significant but with substantial variability across studies. | ⨁⨁◯◯m Low | ||
| 2nd month | 9 RCTs | Serious | Serious | Not serious | Not serious | None | 120 | LLLT likely increased monthly canine retraction by 0.72 mm (95% CI: 0.18 to 1.26) | ⨁⨁◯◯n Low | ||
| 3rd month | 6 RCTs | Serious | Serious | Not serious | Serious | None | 101 | LLLT increased canine retraction by ~0.46 mm (95% CI 0.06 to 0.86) at 3 months vs. control (statistically significant, but wide variation) | ⨁⨁◯◯o Low | ||
| Total retraction ((mm) post‐treatment) | 4 RCTs | Serious | Serious | Not serious | Very Serious | None | 65 | LLLT increased total retraction by 1.08 mm (95% CI: 0.33 to 1.82); statistically significant | ⨁◯◯◯p Very low | ||
| Changes in canine | position | 2 RCTs | Serious | Very serious | Not serious | Serious | None | 21 | Mean differences from −0.13 mm (1st month) to −0.67 mm (4th month) favoring slightly less movement with LLLT, but all 95% CIs cross zero; no statistically significant effect | ⨁◯◯◯q Very low | |
| Canine retraction rate (mm/month) | 6 RCTs | Serious | Not serious | Not serious | Serious | None | 115 | LLLT increased canine retraction rate by 0.66 mm/month compared to control; statistically significant ( | ⨁⨁◯◯r Low | ||
| Accelerating lower canine retraction | |||||||||||
| Using LLLT | Monthly retraction (mm) | 2 RCTs | Serious | Serious | Not serious | Serious | None | 22 |
1st month: MD ≈ +1.03 mm favoring LLLT (95% CI: 0.67 to 1.40) statistically significant 2nd month: MD ≈ −0.14 mm (95% CI: −0.80 to 0.51) not significant 3rd month: MD ≈ −0.06 mm (95% CI: −0.74 to 0.61) not significant | ⨁⨁◯◯s Low | |
| Canine retraction rate (mm/month) | 3 RCTs | Serious | Not serious | Not serious | Serious | None | 60 | LLLT increased the canine retraction rate by 0.58 mm/month compared to the control. Statistically significant ( | ⨁⨁◯◯t Low | ||
| Accelerating En‐masse retraction | |||||||||||
| Using LLLT | Daily retraction (mm/day) | 1 RCT | Serious | Not serious | Not serious | Serious | None | 20 | +30% faster tooth movement on laser side vs control over ~3 months (≈0.09 mm/day vs. 0.07 mm/day), statistically significant ( | ⨁⨁◯◯u Low | |
| Monthly retraction (mm/month) | 1 RCT | Serious | Not serious | Not serious | Very serious | None | 12 | 0.694 mm/month (LLLT) vs. 0.500 mm/month (control). LLLT increased rate by 12.6%. The difference was statistically significant ( | ⨁◯◯◯v Very low | ||
| Using LED | Monthly retraction (mm/month) | 1 RCT | Serious | Not serious | Not serious | Serious | None | 60 |
Mean difference: +0.22 mm/month (LED group: 1.08 ± 0.54 vs. control: 0.86 ± 0.42) ➡ ~26% faster closure Statistically significant ( | ⨁⨁◯◯w Low | |
| Accelerating upper molars intrusion | |||||||||||
| Using LLLT | Average at six months in adults. | 1 RCT | Serious | Not serious | Not serious | Serious | None | 20 | Mean intrusion at 6 months: PBM group: 2.31 ± 0.65 mm vs. Control: 2.95 ± 0.17 mm (slightly slower, no statistically significant difference, | ⨁⨁◯◯x Low | |
| Average at seven months in childs | 1 RCT | Not serious | Not serious | Not serious | Serious | None | 42 | The mean intrusion was 1.21 mm in the FPBB + LLLT group vs. 0.82 mm in FPBB alone, a difference ≈ 0.39 mm more intrusion with LLLT, statistically significant ( | ⨁⨁◯◯y Low | ||
| Interventions | Quality assessment criteria | Summary of findings | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. of studies | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | No. of patients | Effect | Overall quality of evidence | ||
| Accelerating leveling and alignment | ||||||||||
| Lower jaw without extraction | Serious | Not serious | Not serious | Serious | None | 28 | ≈ 1.9 mm extra crowding reduction over 3 months (no statistically significant difference reported) | ⨁⨁◯◯a Low | ||
| Using BM | 1 RCT | |||||||||
| Accelerating upper canine retraction | ||||||||||
| Using LIDEC | Cumulative CR 1st month (mm from baseline) | 1 RCT | Serious | Not serious | Not serious | Serious | None | 7 | Mean difference + 0.53 mm over 4 weeks (≈ 31 % faster); statistically significant ( | ⨁⨁◯◯b Low |
| Using PEMF | Total CR ((mm) post‐treatment) | 2 RCTs | Serious | Not serious | Not serious | Serious | None | 29 |
≈ +1.8 mm more retraction (≈ 35 % increase)
| ⨁⨁◯◯c Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Temporomandibular Joint Disorders · Laser Applications in Dentistry and Medicine
Summary
- •Photobiomodulation (PBM) accelerates tooth movement by 12.5%–54% and reduces treatment time by 19–58 days.
- •Vibrational devices (e.g., AcceleDent) show minimal clinical benefit (<0.3 mm/month).
- •Pulsed electromagnetic field therapy (PEMF) boosts canine retraction by 1.78 mm in 3 months (p < 0.0001).
- •PBM effectiveness is higher in the mandible (1.03 mm) than maxilla (0.33 mm).
- •Evidence quality is low (AMSTAR‐2/ROBIS); standardized protocols and rigorous trials are needed.
1. Introduction
Orthodontic treatment typically lasts 14–33 months (mean: 19.9 months) and requires roughly 18 clinical visits [1]. Treatment duration varies with clinician decisions, case complexity, patient adherence, and the use of acceleration strategies, which are commonly classified as surgical, pharmacological, or physical [2, 3].
Shortening treatment is desirable because it improves comfort and adherence and reduces complications such as root resorption, demineralization, and periodontal disease [4]. However, surgical acceleration may introduce adverse effects, including interdental bone loss [5], loss of tooth vitality [6], surgical scarring [7], gingival recession [8], mechanical root injury [9], subcutaneous hematomas [10], and bacteremia [11].
Therefore, developing nonsurgical adjunctive interventions is essential to deliver accelerated orthodontic treatment that mitigates current complications and avoids introducing new adverse effects.
In orthodontics, physical adjunctive interventions (PAIs) are classified by the type of energy used to stimulate tissues and cells. Mechanical energy includes low‐intensity pulsed ultrasound (LIPUS), which generates gentle acoustic waves that induce mechanical stress and promote bone remodeling [12], and mechanical vibrations (MVs) at low or high frequencies, which activate cells by stressing the periodontal ligament [13]. Light‐based approaches, such as low‐level laser therapy (LLLT) and light‐emitting devices (LEDs), act via photobiomodulation (PBM) to increase mitochondrial ATP production, enhance osteoblastic activity, and trigger controlled sterile inflammation [14]. Bioelectric stimulation (BES) includes methods that use electrical or electromagnetic energy to modulate cellular activity. These include low‐intensity electrical stimulation (LIES), which applies mild currents to enhance signaling (e.g., upregulating RANKL to stimulate bone remodeling) [15], and pulsed electromagnetic fields (PEMF), which alter electrochemical signaling and regulate ion fluxes (e.g., calcium) to activate bone cells [16]. Despite the different energy sources, these modalities converge on intra‐ and extracellular pathways that increase blood flow and RANKL expression, thereby accelerating tooth movement via the regional acceleratory phenomenon [4, 13, 17].
Although marketing frequently claims meaningful time savings and fewer side effects, the clinical evidence from human‐based randomized controlled trials (RCTs), systematic reviews, and meta‐analyses remains inconclusive [18–20]. Marked heterogeneity in intervention types (vibration, PBM, electrical stimulation), treatment mechanics (canine retraction, leveling and alignment, En‐masse retraction; fixed appliances vs clear aligners), outcome measurements (e.g., Little’s Irregularity Index, monthly millimetric progress; direct vs model‐based assessments), and primary study quality has produced inconsistent findings across reviews of adjunct physical interventions for accelerating orthodontic tooth movement (OTM) [4, 16, 21, 22]. Some studies report increased tooth‐movement rates [23–25], whereas others show no significant difference [26–28]. These discrepancies are compounded by methodological issues, such as pooling diverse interventions within a single analysis and repeatedly including the same trials across multiple reviews [23, 27]. These practices reduce specificity, create redundancy, and make it difficult for clinicians to interpret the evidence and select effective techniques.
This umbrella review critically appraises the evidence on PAIs for accelerating OTM by systematically integrating data from existing systematic reviews and meta‐analyses. The umbrella‐review approach is uniquely suited to map overlap among prior syntheses, compare their methodological quality, and reconcile conflicting conclusions across interventions and outcomes. By synthesizing available data, it clarifies methodological sources of heterogeneity, estimates the true efficacy of each modality, and offers evidence‐based clinical guidance. It also counters unsupported marketing claims, identifies research gaps that warrant rigorous future trials, and aims to strengthen confidence in clinical decision‐making.
To the best of current knowledge, this work represents the first comprehensive umbrella review synthesizing evidence on PAIs designed to accelerate orthodontic tooth movement.
2. Materials and Methods
2.1. Scoping Search
This umbrella review followed a pre‐registered protocol (PROSPERO ID: CRD420251043659). A preliminary PubMed search confirmed no prior umbrella reviews addressing the research objective. The protocol was developed by Preferred Reporting Items for SRs and Meta‐Analyses (PRISMA) and the Cochrane guidelines for systematic reviews.
2.2. Eligibility Criteria
Review question: What is the impact of PAIs on OTM acceleration among patients enrolled in randomized clinical trials (RCTs)?
Inclusion criteria were defined using the PICOS framework:
- •Participants: Healthy individuals of any age, gender, or ethnicity undergoing orthodontic treatment.
- •Interventions: PAIs for accelerating OTM, for example, MV, PBM, BES.
- •Comparisons: Control groups receiving standard orthodontic treatment without adjunctive interventions.
- •Outcomes: Rate of tooth displacement (e.g., mm/week/month) or equivalent efficacy metrics.
- •Study Design: Systematic reviews/meta‐analyses of RCTs (parallel or split‐mouth designs).
Exclusion Criteria:
- •Systematic reviews and meta‐analyses, including those of clinical trials, cohort studies, narrative reviews, case series/reports, or animal research.
- •Studies of PAIs that assess pain, root resorption, or other adverse events as primary outcomes.
- •Comparative studies of PAIs versus alternative acceleration techniques (surgical or nonsurgical interventions, medical approaches, or other methods).
- •Systematic reviews, meta‐analyses, or primary studies lacking comprehensive or retrievable data.
2.3. Search Strategy
A systematic search was conducted across PubMed, Web of Science, Scopus, and the Cochrane Library up to March 2025. Controlled vocabulary (MeSH and related free‐text words) and tailored keywords were combined and optimized for each database. To address publication bias, gray literature (e.g., theses) was sourced through ProQuest Dissertations and archived records from OpenGrey Europe (via DANS EASY). Manual searches included reference lists of relevant studies and four key orthodontic journals (American Journal of Orthodontics and Dentofacial Orthopedics, European Journal of Orthodontics, Journal of Orthodontics, and Journal of Orthodontics and Craniofacial Research). No restrictions were applied to language, publication date, or status. Full search syntax is provided in Supporting Information 1: Table S1.
2.4. Study Selection, Data Extraction Process, and Overlap Assessment
Two reviewers (MRS and MON) independently screened titles and abstracts to identify potentially eligible reports, with full texts assessed against predefined inclusion criteria; any discrepancies were resolved through consultation with a third reviewer (MYSA).
For the SRs, data were extracted via a standardized form capturing publication details (year, authors, study design, sample size, and age range), search characteristics (registration status, strategy, restrictions, and execution date), methodological quality (risk‐of‐bias tool and GRADE metrics), intervention and comparator parameters (device type, frequency, force, duration, treatment, and appliance specifics), outcomes (primary endpoints, measurement tools, follow‐up intervals, and results), and ethics/funding information (sources and conflicts of interest).
For the primary studies, citation matrices were generated to quantify overlap [29] and corrected covered areas (CCAs) calculated using the Graphical Representation of Overlap for Overviews tool (GROOVE) [30] (as detailed in Supporting Information 2: Table S2). Subsequently, data were extracted from these de‐duplicated studies on bibliographic details, sample size, study design, orthodontic intervention type, PAIs and parameters, inclusion frequency in systematic reviews, bias‐assessment method, and resulting bias scores.
2.5. Methodological Quality and Risk‐of‐Bias Assessment in Selected Systematic Reviews and Their Primary Studies
The methodological quality of included systematic reviews was assessed with A Measurement Tool to Assess Systematic Reviews‐2 (AMSTAR‐2, 16 domains: 7 critical, 9 noncritical), and their risk of bias was evaluated using the Risk of Bias in Systematic reviews tool (ROBIS, three phases: Assessing relevance, identifying concerns with the review process, and judging risk of bias). Details of the questions, response options, and rating criteria for both tools are presented in Supporting Information 2: Table S2.
For primary studies, initial bias assessment was based on the results of the highest‐confidence reviews (high confidence according to AMSTAR‐2 and low risk according to ROBIS), followed by a reassessment with the Cochrane Risk of Bias 2 (RoB 2) tool under the following exceptional circumstances:
- 1.A review was rated “moderate,” “low,” or “critically low” in AMSTAR‐2 or identified as “unclear” or “high” risk by ROBIS.
- 2.Conflicting bias judgments existed for the same study between two or more reviews.
- 3.Reviews published before 2019 or after 2019 continued to use RoB 1 rather than upgrading to RoB 2.
All assessments (AMSTAR‐2, ROBIS, and RoB 2) were conducted independently by two reviewers (MRS and MON), with any discrepancies resolved by a third reviewer (MYSA) to ensure a unified final classification.
2.6. Evaluating the Strength of Evidence
The evidence quality was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework. Subgroup analyses were performed for each PAI to evaluate their effects separately.
Evidence quality was classified into four levels (high, moderate, low, or very low). Two independent reviewers (MRS and MON) performed the assessments, and disagreements were resolved through consultation with a third reviewer (MYSA).
2.7. Primary Studies Pooling and Meta‐Analysis
Similar outcomes were combined quantitatively in Review Manager (version 5.4.1; The Nordic Cochrane Centre, Copenhagen, Denmark). Continuous results were expressed as mean differences (MDs; 95% CIs), and heterogeneity was assessed using Tau^2^ and I ^2^ statistics. A random‐effects model was applied when I ^2^ exceeded 50%, with a fixed‐effects model used otherwise. Clinically heterogeneous outcomes were narratively synthesized.
Publication bias was planned to be assessed through visual inspection of contour‐enhanced funnel plots if a sufficient number of trials examining the same intervention and outcome were available.
All data collection, analysis, and presentation of results were conducted by one reviewer (MYSA) and independently checked by a second (MRS).
3. Result
3.1. Search Results
A total of 240 articles were identified through database searches. After 69 duplicates were removed, 171 records underwent title and abstract screening, which excluded 136 articles as irrelevant. The remaining 35 full‐text articles were assessed for eligibility, with 18 excluded for not meeting the predefined inclusion criteria. Ultimately, 17 systematic reviews were included in the final analysis. The literature search process is summarized in the flow diagram (Figure 1). Excluded studies after full‐text review, with reasons, are listed in Supporting Information 3: Table S3.
Preferred reporting items for systematic reviews and meta‐analyses (PRISMA) flow chart for included systematic reviews.
3.2. Characteristics and Findings of the Included Systematic Reviews
This synthesis analyzed 17 SRs published between 2016 and 2025, including 12 quantitative (meta‐analytic) and five qualitative (narrative) reviews. The quantitative reviews examined four distinct interventions: General Physical Acceleration (one review [4]), BES (one review [16]), Vibration Devices (six reviews [13, 22, 23, 26–28]), and PBM (LLLT and LED) (nine reviews [14, 21, 24, 25, 31–35]). All reviews included only RCTs, with five employing the Cochrane ROB2 tool for bias assessment [13, 16, 21, 34, 35] and nine using GRADE for evidence quality evaluation [4, 13, 16, 23, 28, 32–35].
Thematic analysis revealed that most SRs addressed multiple orthodontic approaches. Leveling and alignment were covered in 13 reviews [4, 13, 14, 16, 22, 23, 26–28, 32–35], canine retraction in all 17, En‐masse retraction in 10 [4, 13, 21–23, 25, 27, 28, 32, 33], molar intrusion in one [4], and premolar retraction in one [25]. Table 1 summarizes the characteristics of the Included Systematic Reviews.
Findings on vibrational devices were inconsistent: while Abd Elmotaleb et al. [27] found no significant improvement in Little’s Index (p = 0.49), Keerthana et al. [23] reported a statistically significant overall acceleration in tooth movement (p < 0.00001). Dutta et al. [13] documented substantial acceleration in canine retraction (standardized mean difference [SMD] = 2.48, p < 0.05), despite considerable heterogeneity. Descriptive data further suggested that high‐frequency vibrations (113–125 Hz) were more effective, while low‐frequency vibrations produced negligible results (Table 2).
For LLLT, studies using wavelengths between 780 and 830 nm demonstrated up to a 54% increase in the rate of tooth movement [25], with significantly greater effects in the mandible (MD = 1.03 mm, p < 0.0001) compared to the maxilla (MD = 0.33 mm, p = 0.012) [31]. LLLT also shortened treatment duration by ~25 days (p < 0.00001) [29], with the greatest acceleration observed during the first 3 months (weighted mean difference [WMD] = 0.49–0.50 mm, p < 0.04) [14, 33], followed by a statistically reduced effect in the fourth month [21]. Twelve out of 14 studies confirmed a 12.5%–40% increase in movement speed [35], supporting LLLT as a promising technique, provided that photonic and temporal parameters are precisely controlled (Table 2).
LED therapy improved alignment by an average of 24.5 days (p = 0.008), though it did not significantly affect space closure or the average daily rate of tooth movement (p = 0.07) [27] (Table 2).
BES demonstrated significant acceleration in alleviating crowding by the third month (SMD = 0.69, p < 0.05), but no statistically significant effect was observed by the fifth month (SMD = 1.64, p > 0.05) [16]. Descriptive data from selected studies indicated a 30%–40% increase in movement speed [16].
Table 1 summarizes the findings of the included systematic reviews.
3.3. Characteristics of Primary Studies Included in SRs
Seventeen SRs incorporated 76 primary studies published between 2004 and 2024, with detailed characteristics in Supporting Informations 4–6: Tables S4–S6. The overall CCA was 0.11 (11% overlap), indicating study repetition inflated conclusions (Supporting Information 7: Table S7). For vibration devices, 7 SRs analyzed 28 RCTs [36–63], focusing on leveling/alignment (13 RCTs), canine retraction (11 RCTs), and En‐mass retraction (4 RCTs) (Supporting Information 4: Table S4), showing considerable overlap (CCA = 0.36, 36%; Supporting Information 8: Table S8). For PBM, 10 SRs assessed 44 RCTs [64–107], covering leveling/alignment (9 RCTs), canine retraction (28 RCTs), and En‐mass retraction (4 RCTs) (Supporting Information 5: Table S5), with notable overlap (CCA = 0.19, 19%; Supporting Information 9: Table S9). 1 SR on BES included 4 RCTs [108–111], addressing leveling/alignment (1 RCT) and canine retraction (3 RCTs) (Supporting Information 6: Table S6).
3.4. Methodological Quality Assessment (AMSTAR‐2)
All systematic reviews exhibited methodological shortcomings, with quality ranging from critically low [14, 21, 24, 27, 31, 32, 34, 35] to moderate [25, 28]. Results from the AMSTAR‐2 tool assessments are summarized in Table 3 and Figure 2, with detailed rationale in Supporting Information 10: Table S10.
Methodological quality of the selected systematic reviews according to the 16 items proposed by the AMSTAR 2 tool.
All reviews met requirements for domains 1, 5, 14, and 16. Among the seven critical domains, compliance was highest in domains 9, 11, and 13 but lowest in domains 2, 4, and 15. Key deficiencies included: 41.1% lacking prior protocol registration; 52.94% of registered protocols failing to explain adherence or deviations; 92% omitting comprehensive searches (e.g., manual/gray literature/unpublished data); and only 23.52% (four reviews [13, 16, 23, 33]) analyzing publication bias.
3.5. ROBIS
A ROBIS assessment of 17 SRs found 2 with low risk [4, 34], 2 unclear [13, 33], and 13 high risk [14, 16, 21–25, 27, 28, 31, 32, 35], summarized in Table 4 and Figure 3 with detailed rationale in Supporting Information 11: Table S11. Domain 1 faced issues from unregistered protocols and eligibility restrictions. Domain 2 was limited by insufficient database coverage and a lack of supplementary methods. Domain 3 demonstrated high compliance via reliable data collection, approved bias tools, and accurate reporting, while Domain 4 performed poorly by failing to assess heterogeneity and conducting meta‐analyses combining high‐bias/varied‐design studies without sensitivity analyses, undermining reliability and highlighting the need for improved rigor in heterogeneity handling and meta‐analyses.
Methodological risk of bias assessment of the selected systematic reviews based on the four stages proposed by the ROBIS tool.
3.6. Reassessment of ROB in Primary Studies Using ROB2
The risk of bias for all primary studies was re‐evaluated using the ROB2 tool due to concerns including low evidence quality (AMSTAR‐2) and high bias risk (ROBIS) in most systematic reviews, significant overlap (CCA) of primary studies across reviews, and the use of ROB1 in 12 systematic reviews (four pre‐ [24, 26, 27, 32] and eight post‐2019 [4, 14, 22, 23, 25, 28, 33, 34]). Variability in bias risk persisted for repeated studies across reviews, even with identical assessment tools, and some primary studies underwent evaluation with multiple tools. Reassessment of ROB in Primary Studies in systematic reviews is justified by Supporting Information 12: Table S12.
Original and updated bias risks are documented in Supporting Informations 4–6: Tables S4–S6 and Supporting Informations 14 and 15: Figures S1 and S2, with detailed assessment rationales in Supporting Information 13: Table S13.
3.7. Findings From the Pooled Primary Studies After Removal of Overlap
The meta‐analysis results (MA‐pool) are presented in Figures 4–12, and both MA‐pool and individual findings (IF‐pool) are summarized in Tables 5–7.
Forest plot comparing AcceleDent vibration therapy versus control for reduction in Little’s irregularity index (LII) during orthodontic leveling and alignment in mandibular and maxillary arches without extractions.
Forest plot comparing vibration and control for mean canine retraction rate (overall), monthly canine retraction (at months 1–3), and total canine retraction.
Forest plot comparing vibration vs. control for mean En‐masse retraction rate (mm/month) in upper quadrants.
Forest plot of low‐level laser therapy (LLLT) versus control effect on orthodontic leveling and alignment time (OLAT) and leveling and alignment improvement percentage (LAIP) in mandible without extraction.
Figure 8. Forest plot comparing low‐level laser therapy (LLLT) and control for monthly upper canine retraction (mm) (at months 2–3), cumulative upper canine retraction (mm from baseline) (at 21 days and months 1–3), and total upper canine retraction (mm) (post‐treatment).
Forest plot comparing low‐level laser therapy (LLLT) versus control for monthly changes in upper canine position (at months 1–4) and upper canine retraction rate (mm/month).
Forest plot comparing light‐emitting diode (LED) therapy versus control for monthly upper canine retraction rate (mm) (at months 1–3).
Forest plot of low‐level laser therapy (LLLT) versus control for monthly lower canine retraction rate (mm) (at months 1–3) and overall lower canine retraction rate (mm).
Forest plot of pulsed electromagnetic fields (PEMF) versus control for total upper canine retraction (mm).
3.7.1. Vibration Devices (Table 5, Figures 4–6)
Leveling and alignment: AcceleDent showed minimal or no clinical benefit in both mandibular and maxillary leveling (effect sizes: −0.12 to 0.21, p > 0.05) across multiple RCTs [36, 39, 41–43, 47, 48]. Tooth Masseuse showed moderate improvement in one small trial [44], while a customized device showed better results (0.83, 1 RCT, p = 0.05) but in a very small sample (n = 12) [45].
Canine retraction: AcceleDent significantly accelerated retraction (0.27 mm/month, four RCTs, p < 0.0001) [38, 50–52], while customized appliances [58, 59] and toothbrush [54, 56, 57] use showed inconsistent or nonsignificant effects. Total retraction was modest (0.67 mm, three RCTs, p = 0.045) [54, 55, 57].
En masse retraction: AcceleDent [60] and customized vibratory devices [62, 63] had no significant impact. Effects were inconsistent and generally negligible, especially in lower arches [62].
3.7.2. PBM (Table 6, Figures 7–11)
Leveling and alignment (Figure 7): LLLT significantly reduced mandibular alignment time without extraction (−58.42 days, 2 RCTs, p = 0.0002) [64, 66], though it did not improve alignment percentage [65, 66]. LED therapy also shortened alignment time (−19.5 to −57 days; p < 0.05) [67, 68] and increased alignment rate (0.63 mm/week; p < 0.00001) [71]. LLLT reduced daily aligner wear from 22 to 12 h (p < 0.001) [72], enhancing treatment efficiency.
Upper canine retraction (Figures 8–10): LLLT showed significant retraction in the 2nd (0.27 mm, six RCTs, p = 0.005) [79, 81, 82, 87, 96, 97] and 4th month (0.52 mm, 1 RCT, p = 0.03) [87]. Cumulative gains were significant up to 3 months (total: 1.08 mm, four RCTs, p = 0.0046) [79, 94, 95, 98]. Retraction rate reached 0.66 mm/month (6 RCTs, p < 0.0001) [74, 78, 94, 95, 99, 100], with space closure accelerated by 13.14 days [88]. LED devices showed no significant effects (p > 0.05).
Lower canine retraction (Figure 11): Significant retraction in the 1st month (1.03 mm, two RCTs, p < 0.0001) [96, 97], with an overall rate of 0.58 mm/month, three RCTs [95, 99, 100]. Later months showed no notable improvement.
En masse retraction: LLLT showed daily retraction of 0.04 mm (one RCT, p < 0.0001) [101]; LED showed monthly effects (0.22 mm, one RCT, p = 0.007) [104]. Total upper arch retraction was 0.194 mm/month (one RCT, p = 0.017) [102], with significant site‐specific effects in both upper and lower quadrants (p < 0.01) [103].
Upper molar intrusion: In adults, LLLT showed a nonsignificant effect (−0.64, one RCT, p > 0.05) [106]. In children, it was effective (0.39, one RCT, p = 0.018) [107].
3.7.3. BES (Table 7, Figure 12)
BES devices significantly improved orthodontic outcomes. The bimaxillary mouthpiece device (BM) reduced mandibular crowding by 1.9 mm more than controls in 3 months (one RCT, p < 0.05). Low‐intensity direct current (LIDEC) achieved 0.53 mm greater upper canine retraction in 1 month (one RCT, p = 0.001). PEMF showed the strongest effect, with 1.78 mm total retraction compared to control (two RCTs, p < 0.0001) (Figure 12).
3.8. Overall Quality of the Evidence Across Studies
The assessment of evidence certainty based on the GRADE methodology is detailed in Tables 8–10, organized according to the acceleration modality (vibration, PBM, or BES). In general, the majority of the included studies were judged to provide low to very low certainty evidence, primarily due to concerns related to high risk of bias or some concerns in key ROB2 domains, coupled with imprecision arising from small sample sizes and wide confidence intervals (CIs).
3.9. Additional Analysis
Publication bias was visually assessed using funnel plots for outcomes reported in ≥10 studies. This included cumulative upper canine retraction (mm) from baseline using LLLT at 1 month. Figure 13 displays the funnel plot of effect estimate versus standard error (SE) for this outcome. The plot exhibited asymmetry, indicating publication bias.
Funnel plot for publication bias detection. Cumulative upper canine retraction (mm) (at the first month) accelerated by low‐level laser therapy (LLLT).
Publication bias analysis was not possible for other interventions/variables due to insufficient trials.
4. Discussion
Despite the widespread use of PAIs to accelerate orthodontic treatment, evidence on their efficacy remains inconsistent due to variability in study designs and protocols. This umbrella review provided a critical synthesis and quantitative analysis of primary studies from existing systematic reviews to optimize PAIs’ use in clinical practice. It assessed the effects of PAIs on orthodontic treatment modalities (leveling and alignment, canine and En‐masse retraction, and molar intrusion). Overall, the certainty of evidence (GRADE) across modalities ranged from moderate to very low.
4.1. Leveling and Alignment
Current evidence shows that vibrational devices offer no clear therapeutic benefit in most orthodontic treatments [13, 26, 27]. In non‐extraction cases [36, 39, 41–43, 47, 48], AcceleDent’s effect is negligible, while devices like Tooth Masseuse [44] and Customized Appliance [45] produce only modest, non‐significant improvements, or benefits seen only in very small samples, limiting how broadly these results can be applied. Vibrations add no measurable advantage in extraction cases either [40]. This variation likely reflects insufficient force levels to trigger the needed biological response, inconsistent patient compliance, differences in treatment stages, and individual variability [28]. GRADE: ranged from moderate to low, for vibration devices.
PBM accelerates tooth movement by boosting cellular energy production and growth‐factor release, which speeds bone remodeling around the roots and shortens alignment time [34]. Clinically, lower‐arch leveling without extractions can be reduced by about 2 months with LLLT, and LED systems show similar, though wavelength‐dependent, effects. However, the early weeks of treatment do not show an immediate rise in the Leveling and Alignment Improvement Percentage index (LAIP) [65, 66], since final precision still depends on appliance design and applied mechanical forces.
LED treatment has been found to cut processing time by roughly 3 weeks in non‐extraction lower arches [67] and by nearly 2 months in upper‐extraction cases [69]. Its broader beam angle and adequate soft‐tissue penetration in the upper arch likely contribute to these gains. LED can increase tooth‐movement rates by over 0.5 mm per week, helping achieve treatment goals more quickly.
LLLT also reduces the required daily wear time for clear aligners from 22 to 12 h by stimulating bone‐forming cells and reducing local inflammation [72]. This makes aligner compliance easier for patients, improving success rates, lowering compliance‐related risks, and shortening overall treatment duration. GRADE: ranged from low to very low, for PBM (LLLT/LED).
BES: In one small RCT [108], BES reduced lower‐arch crowding by 1.9 mm over 3 months, but the tiny sample size limits result credibility. BES likely works by activating osteoblasts through ion‐channel stimulation, improving local blood flow and calcium concentration, thus enhancing bone remodeling and lowering tissue resistance. However, it remains unclear whether the effect accelerates incisor movement or alters tooth axis, raising questions about its precision. These early findings are promising and justify further study, but they do not yet support strong clinical recommendations. GRADE: low for BES.
From a clinical standpoint, these findings indicate that vibration alone is unlikely to justify additional chairside time or device cost for routine leveling and alignment, whereas PBM—particularly LLLT—may be selectively considered in cases where a 3–8‐week reduction in alignment time or a halving of aligner wear (from 22 to 12 h/day) could meaningfully improve adherence, although the overall certainty of evidence remains low.
4.2. Canine Retraction
Canine retraction adjunctive methods exhibit variable efficacy depending on their biological mechanisms of action and implementation quality:
Vibrational Stimulation: Significant superiority using AcceleDent (0.27 mm/month) arises from osteocyte activation via enhanced blood perfusion and increased cytokines [13]. In contrast, manual brushing showed irregular cumulative effects (likely due to inconsistent stimulation or patient compliance variability) [54, 56, 57]. However, the wide CI (0.01–1.32) highlights the need for standardized protocols (e.g., vibration intensity/duration). GRADE: very low for vibration devices.
Photobiostimulation (LLLT and LED): Delayed results (up to the fourth month) correlate with cumulative cellular modifications (e.g., increased ATP production and growth factors like Vascular Endothelial Growth Factor [VEGF]) [87]. The weaker outcomes with LED devices may reflect differences in wavelength penetration [73, 75]. The decline in mandibular stimulation efficacy could stem from high bone density resisting rapid changes or gradual depletion of cellular metabolic reserves, necessitating intermittent protocols to avoid adaptive resistance [96]. GRADE: ranged from moderate to very low for LLLT and from low to very low for LED.
BES: Marked superiority (1.78 mm) reflects activation of calcium channels and Wnt/β‐catenin signaling pathways that accelerate bone remodeling [110, 111]. However, the scarcity of studies and variability in their designs (e.g., stimulation intensity) limit the generalizability of findings. GRADE: low for BES.
Clinically, a gain of roughly 0.27–0.66 mm/month in canine retraction corresponds to ~2–4 mm of additional movement over a 6‐month retraction phase, which may shorten space closure by one or two visits but is unlikely to dramatically reduce total treatment time, whereas the larger point estimate reported for BES (≈1.8 mm at 3 months) remains too uncertain to support routine use until replicated in larger, high‐quality trials.
4.3. En‐Masse Retraction
Vibration devices showed no meaningful benefit, likely due to insufficient amplitude or non‐optimal frequencies failing to stimulate the cellular mechanisms of bone remodeling, compounded by uneven force distribution across arches [4, 63]. GRADE: ranged from low to very low, for vibration devices.
In contrast, both LLLT and LED treatments produced statistically significant increases in daily and monthly tooth movement [101, 104], reflecting enhanced cytokine and growth‐factor signaling that accelerates bone resorption and formation. However, these results stem from single, small RCTs, limiting their generalizability. Future work should optimize vibratory device design and standardize PBM protocols—especially dosing and delivery—to reliably harness their respective effects in a safe, efficient orthodontic regimen. GRADE: ranged from low to very low for LLLT, and low for LED.
In routine practice, the small absolute gains reported with PBM during en‐masse retraction (on the order of fractions of a millimeter to just over 1 mm per month) are unlikely to transform overall treatment duration, but could marginally shorten the retraction phase in complex extraction cases; in contrast, vibration devices currently offer no clinically meaningful advantage in this context and should not be relied upon as primary accelerators.
4.4. Upper Molars Intrusion
In adults, LLLT did not achieve a statistically significant effect over 6 months, possibly due to slow bone remodeling and high bone density [106]. In children, it showed a positive, statistically significant effect after 7 months, reflecting more active bone growth and faster renewal [107]. The absence of CIs, a limited number of studies, and a small sample size limit the ability to generalize the results. GRADE: low for LLLT.
Thus, for molar intrusion, PBM should presently be regarded as an experimental adjunct with limited clinical impact in adults and only a modest, age‐dependent benefit in growing patients, where an additional ≈0.4 mm of intrusion over 7 months is unlikely to alter treatment planning but might slightly reduce the duration of active mechanics.
4.5. Evidence Comparison: Systematic Reviews vs. Pooled Primary Data
Discrepancies between the results reported in the included systematic reviews and those of the current umbrella review (after consolidating primary studies) arise due to:
- 1.Limited primary studies per review: The largest review included only 25 trials.
- 2.Narrative reporting: Outcomes were often described qualitatively, lacking quantitative effect size analysis relative to study quality/quantity.
- 3.Heterogeneous meta‐analyses: Some reviews combined diverse assessment methods, acceleration techniques, parameters, or protocols without subgroup analyses or appropriate statistical models (fixed‐/random‐effects), risking biased effect estimates.
When these effect sizes are considered together, they suggest that—even under favorable conditions—physical adjunctive interventions are unlikely to reduce the overall duration of comprehensive orthodontic treatment by more than a few months or to eliminate multiple visits; rather, their benefits are concentrated in specific phases (such as early alignment or initial space closure) and remain highly dependent on protocol design and patient adherence. Consequently, PAIs should be presented to patients as optional adjuncts that may offer modest, phase‐specific time savings or improved comfort in selected cases, rather than as guaranteed solutions for dramatically shortening orthodontic therapy.
4.6. Strengths and Limitations
This umbrella review’s main benefit is to summarize evidence on physical interventions for accelerating orthodontic treatment and assess its certainty. Strengths include: an extensive electronic search including gray literature, dissertations, and non‐English references. Reviews quality and bias were checked with AMSTAR‐2 and ROBIS. Primary studies were extracted and re‐assessed for bias using ROB2. Evidence quality was graded using GRADE. Systematic review findings were compared with the pooled primary studies’ results.
Key limitations include significant clinical heterogeneity across reviews and primary trials due to variations in PAIs, parameters, appliances, treatments, wire sequences, and protocols. This was mitigated by grouping data with similar treatment goals, PAIs, and parameters. Furthermore, many primary studies exhibited low quality with high/unclear risk of bias, addressed through ROB2 re‐evaluation and GRADE evidence assessment. Substantial overlap among systematic reviews introduced redundancy, as many reiterated the same trials without novel insights. To prevent this, orthodontic journals should adopt Cochrane’s model of updating existing reviews rather than publishing redundant ones. Additionally, the present umbrella review was intentionally focused on efficacy outcomes (rate of tooth movement and treatment duration), without a parallel, comprehensive synthesis of key safety endpoints such as pain and root resorption; these outcomes are being addressed in a separate, complementary review, and future syntheses should incorporate standardized safety measures to support a more balanced risk–benefit appraisal of physical adjunctive interventions. Finally, future trials should prioritize robust RCTs with larger samples, long‐term follow‐up, standardized protocols, and thorough evaluation of interventions’ cost–benefit‐risk profiles.
4.7. Future Research Recommendations and Gaps
Future trials should use preregistered protocols and report according to CONSORT. Randomization, allocation concealment, and blinding must be explicit, with credible sham devices and adherence reporting. Multicenter RCTs with adequate sample sizes are encouraged. A core outcome set should include OTM rate and total treatment time, with standardized measurement methods and 95% CIs. Adverse events and patient‐reported outcomes should be captured, and basic economic endpoints added when feasible. Dosing and parameters must be standardized for each modality: for light‐based therapy, report wavelength, energy density, power, application points, and session timing; for vibration, report frequency, force, session length, and use patterns; for electrical or electromagnetic stimulation, report current or field strength, waveform, duty cycle, and exposure time. Co‐interventions should be minimized or described clearly, and dissimilar modalities should not be pooled in single analyses. De‐identified data and analysis code should be shared, and follow‐up extended to assess durability and late harms. Adhering to these principles will reduce heterogeneity, increase certainty, and enable reliable, modality‐specific conclusions.
5. Conclusions
This umbrella review reveals inconsistent quality in included systematic reviews, with all exhibiting issues in at least one domain (ROB, AMSTAR‐2, or ROBIS). Consequently, their evidence credibility remains questionable and requires cautious interpretation.
After standardizing primary study criteria and removing overlaps, pooled data show orthodontic acceleration effectiveness varies by each technique’s mechanism.
5.1. Vibrational Devices
Current data do not support vibration as a primary acceleration method. It may, however, complement other modalities (e.g., PBM) if patients are well‐informed about its modest effect and maintain strict adherence. Despite widespread marketing, vibration currently holds the weakest scientific support among acceleration strategies. GRADE: ranged from moderate to very low.
5.2. PBM
PBM shows potential in accelerating treatment, particularly during leveling/alignment and retraction phases. Its efficacy appears influenced by treatment stage, arch location, extraction status, and light source (LLLT vs. LED). LLLT generally shows stronger outcomes than LED, with effects often more pronounced in the upper arch. Consistent protocols are essential to optimize results. GRADE: overall ranged from moderate to very low; LLLT: ranged from moderate to very low; LED: ranged from low to very low.
5.3. BES
Preliminary evidence for techniques like PEMF is promising, especially for canine retraction, though further validation is needed. Combining PBM and BES in future multicenter trials using standardized protocols and CBCT‐based assessments is encouraged. GRADE: low.
Finally, studies assessing cost‐effectiveness and patient compliance are crucial to guide practical adoption and ensure long‐term sustainability of these technologies.
NomenclatureAMSTAR‐2:A Measurement Tool to Assess Systematic Reviews‐2ATP:Adenosine TriphosphateBES:Bioelectric StimulationBM:Bimaxillary mouthpieceCCA:Corrected Covered AreaCBCT:Cone Beam Computed TomographyCI:Confidence IntervalCIs:Confidence IntervalsGRADE:Grading of Recommendations Assessment, Development, and EvaluationGROOVE:Graphical Representation of Overlap for OverviewsLAIP:Leveling and Alignment Improvement PercentageLED:Light‐Emitting DiodeLIDEC:Low‐intensity direct currentLIES:Low‐Intensity Electrical StimulationLII:Little’s Irregularity IndexLIPUS:Low‐Intensity Pulsed UltrasoundLLLT:Low‐Level Laser TherapyMA‐Pool:Meta‐Analysis of Pooled DataMD:Mean DifferenceMeSH:Medical Subject HeadingsMV:Mechanical VibrationOLAT:Orthodontic Leveling and Alignment TimeOTM:Orthodontic Tooth MovementPAIs:Physical Adjunctive InterventionsPBM:PhotobiomodulationPEMF:Pulsed Electromagnetic FieldsPICOS:Participants, Interventions, Comparisons, Outcomes, Study DesignPRISMA:Preferred Reporting Items for Systematic Reviews and Meta‐AnalysesPROSPERO:International Prospective Register of Systematic ReviewsRANKL:Receptor Activator of Nuclear Factor Kappa‐B LigandRCTs:Randomized Controlled TrialsROBIS:Risk Of Bias in Systematic ReviewsRoB 2:Cochrane Risk of Bias 2 ToolSMD:Standardized Mean DifferenceSRs:Systematic ReviewsVEGF:Vascular Endothelial Growth FactorVDs:Vibrational DevicesWMD:Weighted Mean Difference.
Ethics Statement
This umbrella review and meta‐analysis is based solely on previously published studies and involves no new data collection from human participants or animals; therefore, ethics approval and informed consent were not required (not applicable).
Disclosure
All authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Conceptualization: Mohamad Radwan Sirri, Mohammad Osama Namera. Methodology: Mohamad Radwan Sirri, Mohammad Osama Namera, Mohamad Yaman Salahi Alasbahi. Software: Mohamad Yaman Salahi Alasbahi. Validation: Mohamad Radwan Sirri, Mohammad Osama Namera, Mohamad Yaman Salahi Alasbahi. Formal analysis: Mohamad Radwan Sirri, Salar Karim Khalil. Investigation: Mohamad Yaman Salahi Alasbahi. Data curation: Mohamad Yaman Salahi Alasbahi, Salar Karim Khalil. Writing – original draft: Mohamad Radwan Sirri, Mohamad Yaman Salahi Alasbahi, Salar Karim Khalil. Writing – review & editing: Mohammad Osama Namera, Salar Karim Khalil, Mohamad Radwan Sirri. Visualization: Mohamad Radwan Sirri, Mohammad Osama Namera. Supervision: Mohamad Radwan Sirri, Mohammad Osama Namera. Project administration: Mohamad Radwan Sirri.
Funding
No funding was received for this research.
Supporting Information
Additional supporting information can be found online in the Supporting Information section.
Supporting information
Supporting Information 1 Table S1: Electronic search strategy.
Supporting Information 2 Table S2: The CCA formula and AMSTAR‐2 tool domains and judgments.
Supporting Information 3 Table S3: Studies excluded and reasons for exclusion.
Supporting Information 4 Table S4: Characteristics of the pooled primary studies on accelerating orthodontic treatment using VDs.
Supporting Information 5 Table S5: Characteristics of the pooled primary studies on accelerating orthodontic treatment using PBM.
Supporting Information 6 Table S6: Characteristics of the pooled primary studies on accelerating orthodontic treatment using BES.
Supporting Information 7 Table S7: The degree of overlap of primary studies included in all systematic reviews.
Supporting Information 8 Table S8: The degree of overlap of primary studies included in systematic reviews of VDs.
Supporting Information 9 Table S9: The degree of overlap of primary studies included in systematic reviews of PBM.
Supporting Information 10 Table S10: Detailed supporting reasons for the AMSTAR‐2 (A Measurement Tool to Assess Systematic Reviews‐2) assessment of each included systematic review.
Supporting Information 11 Table S11: Detailed supporting reasons for the ROBIS Tool assessment of each included systematic review.
Supporting Information 12 Table S12: The need for reassessment of risk of bias in primary studies using ROB2 tool.
Supporting Information 13 Table S13: Risk‐of‐bias reassessment of included RCTs with supporting justifications.
Supporting Information 14 Figure S1: Risk of bias summary of RCT: reviewers’ reassessment of risk of bias for each domain in the included studies using the RoB 2 Tool.
Supporting Information 15 Figure S2: Overall reassessment of risk of bias profile for RCTs: Reviewers’ RoB 2 judgments presented as percentages across all included studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tsichlaki A. , Chin S. Y. , Pandis N. , and Fleming P. S. , How Long Does Treatment With Fixed Orthodontic Appliances Last? A Systematic Review, American Journal of Orthodontics and Dentofacial Orthopedics. (2016) 149, no. 3, 308–318, 10.1016/j.ajodo.2015.09.020, 2-s 2.0-84959352812.26926017 · doi ↗ · pubmed ↗
- 2Fisher M. A. , Wenger R. M. , and Hans M. G. , Pretreatment Characteristics Associated With Orthodontic Treatment Duration, American Journal of Orthodontics and Dentofacial Orthopedics. (2010) 137, no. 2, 178–186, 10.1016/j.ajodo.2008.09.028, 2-s 2.0-75649131460.20152672 · doi ↗ · pubmed ↗
- 3Faruqui S. , Fida M. , and Shaikh A. , Factors Affecting Treatment Duration – A Dilemma in Orthodontics, Journal of Ayub Medical College, Abbottabad: JAMC. (2018) 30, no. 1, 16–21.29504322 · pubmed ↗
- 4El-Angbawi A. , Mc Intyre G. , Fleming P. S. , and Bearn D. , Non-Surgical Adjunctive Interventions for Accelerating Tooth Movement in Patients Undergoing Orthodontic Treatment, Cochrane Database of Systematic Reviews. (2023) 6, no. 6, 10.1002/14651858.CD 010887.pub 3, CD 010887.37339352 PMC 10281004 · doi ↗ · pubmed ↗
- 5Lee W. , Corticotomy for Orthodontic Tooth Movement, Journal of the Korean Association of Oral and Maxillofacial Surgeons. (2018) 44, no. 6, 251–258, 10.5125/jkaoms.2018.44.6.251, 2-s 2.0-85064211655.30637238 PMC 6327016 · doi ↗ · pubmed ↗
- 6Park Y. G. , Frontiers of Oral Biology, Frontiers of Oral Biology. (2016) 18, 109–117, 10.1159/000351904, 2-s 2.0-84949193185.26599124 · doi ↗ · pubmed ↗
- 7Charavet C. , Lecloux G. , and Bruwier A. , et al.Localized Piezoelectric Alveolar Decortication for Orthodontic Treatment in Adults: A Randomized Controlled Trial, Journal of Dental Research. (2016) 95, no. 9, 1003–1009, 10.1177/0022034516645066, 2-s 2.0-84979282941.27129491 · doi ↗ · pubmed ↗
- 8Yavuz M. C. , Sunar O. , Buyuk S. K. , and Kantarcı A. , Comparison of Piezocision and Discision Methods in Orthodontic Treatment, Progress in Orthodontics. (2018) 19, no. 1, 10.1186/s 40510-018-0244-y, 2-s 2.0-85055612665, 44.30370430 PMC 6204431 · doi ↗ · pubmed ↗