Assessing Nanopore Targeted Sequencing for the Diagnosis of Pulmonary Infections: A Comparative Multidisease Approach
Ying Zhao, Guannan Ma, Tianxiao Ma, Yongshuai Miao, Heya Na, Yuhui Liu, Xiaohua Li

TL;DR
Nanopore sequencing outperforms traditional tests in diagnosing lung infections, especially for fungi and mixed infections in patients with conditions like hypertension.
Contribution
Demonstrates nanopore sequencing's superior sensitivity in detecting diverse pathogens in pulmonary infections compared to conventional methods.
Findings
NTS detected 91.85% of pathogens, significantly higher than conventional tests at 74.81%.
NTS showed 81.7% sensitivity for fungal infections and 99.65% for mixed infections.
Hypertensive patients had higher rates of fungal and mixed infections, detected effectively by NTS.
Abstract
Pulmonary infections remain a significant global health burden, particularly in immunocompromised individuals and patients with chronic respiratory or systemic diseases. Conventional microbiological tests (CMTs), though widely used, often have limited sensitivity and delayed results, especially in polymicrobial or atypical infections. This study evaluated the diagnostic performance of nanopore targeted sequencing (NTS) in 284 patients with suspected lower respiratory tract infections at Chifeng Municipal Hospital, using CMTs and clinical diagnosis as references. NTS demonstrated markedly higher sensitivity (91.85%) compared to CMTs (74.81%), with substantial improvements in detecting fungal (81.7%) and mixed infections (99.65%). A total of 259 pathogens were detected. Among them, bacteria were the most frequently identified pathogens (69.5%), followed by fungi (15.44%) and viruses…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
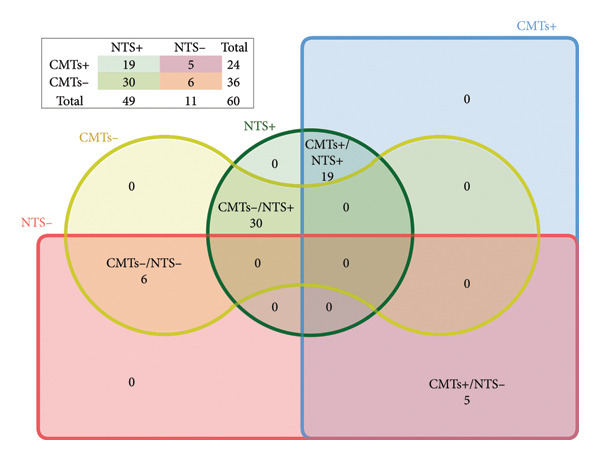 Figure 4
Figure 4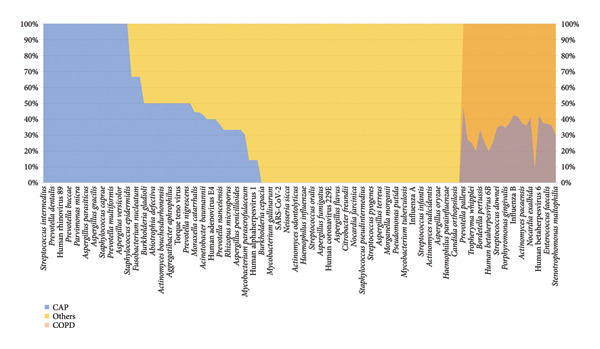 Figure 5
Figure 5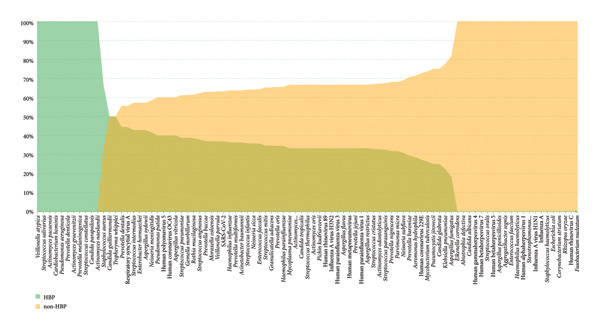 Figure 6
Figure 6| Characteristics | Patients, |
|---|---|
| Gender | |
| Male | 118 (41.55%) |
| Female | 166 (58.45%) |
| Age (years%) | |
| Range | 15–90 |
| Average | 58.80 ± 13.97 |
| Infection types | |
| CAP | 211 (74.29%) |
| Infection | 43 (15.14%) |
| COPD | 37 (13.03%) |
| Bronchitis | 24 (8.45%) |
| Tuberculosis | 23 (8.10%) |
| CB | 20 (7.04%) |
| Bronchiectasis | 18 (6.33%) |
| Cancer | 18 (6.33%) |
| AECB | 13 (4.58%) |
| Asthma | 10 (3.52%) |
| ILD | 15 (5.28%) |
| Major complications | |
| Hypertension | 104 (36.62%) |
| History of surgery and trauma | 47 (16.55%) |
| Diabetes | 24 (8.45%) |
| Liver and renal diseases | 21 (7.39%) |
| Malignancy or immunocompromised | 18 (6.34%) |
| Coronary heart disease | 14 (4.93%) |
| Cerebral infarction | 10 (3.52%) |
| Cerebral hemorrhage | 3 (1.06%) |
| Detection method | Positive (%) | Negative (%) | Total (%) |
|---|---|---|---|
| NTS | 260 (91.55) | 24 (8.45) | 284 (100) |
| CMTs | 208 (73.24) | 76 (26.76) | 284 (100) |
| Method | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) |
|---|---|---|---|---|
| NTS | 81.7 | 53.6 | 32.0 | 91.6 |
| CMTs | 40.0 | 92.0 | 57.1 | 85.1 |
| NTS + CMTs | 90.0 | 51.3 | 33.1 | 95.0 |
| Pathogen | NTS | Traditional culture |
|
|
|---|---|---|---|---|
| 2 or more species | 283 (99.65%) | 16 (5.63%) | 499.68 |
|
| 2 or more types | 278 (97.89%) | 12 (4.23%) | 494.76 |
|
- —Natural Science Foundation of Chifeng
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Pneumocystis jirovecii pneumonia detection and treatment · Cystic Fibrosis Research Advances
Summary
- •NTS significantly outperformed CMTs in sensitivity and spectrum of pathogen detection, including organisms often missed by conventional methods. Its integration into diagnostic workflows may improve etiological precision and support personalized antimicrobial strategies, particularly in patients with comorbidities.
1. Introduction
Pulmonary infections are a major cause of morbidity and mortality worldwide, particularly among immunocompromised individuals and hospitalized patients [1]. These infections encompass a wide spectrum of diseases caused by bacteria, viruses, fungi, and mycobacteria, with pathogen distribution varying significantly depending on clinical settings and patient populations. For instance, community‐acquired pneumonia (CAP) is predominantly caused by Streptococcus pneumoniae, Haemophilus influenzae, Mycoplasma pneumoniae, and respiratory viruses such as influenza virus and SARS‐CoV‐2 [2]. In contrast, hospital‐acquired pneumonia (HAP) is caused by Gram‐negative bacteria (GNB) among bacterial pneumonia [3], including Pseudomonas aeruginosa, Acinetobacter baumannii, and methicillin‐resistant Staphylococcus aureus (MRSA), which pose significant challenges for empirical treatment due to high antibiotic resistance rates.
In immunocompromised patients, such as those with hematologic malignancies, solid organ transplantation, or HIV infection, opportunistic pulmonary infections are common [4, 5]. Additionally, patients with chronic lung diseases (such as cystic fibrosis [CF], chronic obstructive pulmonary disease [COPD], and bronchiectasis) frequently experience polymicrobial infections. Haemophilus influenzae (H. influenzae) and Moraxella catarrhalis (M. catarrhalis) are associated with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) [6, 7].
Despite the clinical significance of pulmonary infections, traditional microbial culture (conventional microbiological tests [CMTs]), including culture‐based methods, serology, and PCR, has notable limitations. These approaches often have low sensitivity for slow‐growing or nonculturable pathogens, are time‐consuming, and may fail to detect polymicrobial infections, particularly in patients receiving prior antibiotic therapy [8]. Furthermore, traditional methods are inadequate for the rapid identification of emerging or rare pathogens, limiting their utility in guiding timely clinical decision making [9].
Nanopore targeting sequencing (NTS) has recently emerged as a promising diagnostic technology, offering real‐time sequencing, broad‐spectrum pathogen detection, and higher sensitivity compared to conventional methods [10]. NTS enables the simultaneous identification of bacteria, fungi, mycobacteria, and viruses, providing a more comprehensive approach to diagnosing pulmonary infections [11]. Several studies have demonstrated that metagenomic sequencing improves pathogen detection, particularly in polymicrobial infections and cases where standard diagnostics yield negative results [12–14]. However, the clinical performance of NTS in pulmonary infections, particularly its sensitivity, specificity, and agreement with CMTs and clinical diagnosis, remains inadequately explored.
This study evaluates the diagnostic value of NTS for pulmonary infections by comparing its pathogen detection with CMTs and clinical diagnosis. Analyzing 284 patients, we found bacteria were the most common pathogens, followed by fungi and viruses, with CAP (74.29%) being the predominant disease. NTS showed significantly higher sensitivity (81.7%) than CMTs (40%), especially in detecting complex infections. Pathogen distribution varied by infection type (e.g., CAP and COPD) and comorbidities (e.g., hypertension [HBP]), underscoring the need for precise diagnosis and personalized treatment. Our findings may contribute to optimizing pathogen detection strategies and guiding more effective antimicrobial therapy in clinical practice.
2. Materials and Methods
2.1. Patient Cohort
This observational study enrolled 284 patients with suspected lower respiratory tract infection (LRTI) who presented to Chifeng Municipal Hospital between June 2023 and September 2024. Demographic data, clinical characteristics, medical history, diagnostic and therapeutic interventions, radiologic and laboratory results, microbiological testing, pathology, and clinical outcomes were collected. All patients underwent bronchoscopy, and bronchoalveolar lavage fluid (BALF) was collected from the lesion site based on CT imaging. Then the BALF was aseptically aliquoted and subjected to CMTs and NTS, respectively.
2.2. CMTs
BALF samples were subjected to standard microbiological analyses, including Gram staining, culture for bacteria, mycobacteria, and fungi, and acid‐fast staining. Additional tests were conducted as clinically indicated, such as fungal immunofluorescence staining, galactomannan antigen testing for Aspergillus, and cryptococcal antigen detection.
3. NTS
Respiratory tract samples (placed in sterile sputum containers) are collected and immediately transported to a commercial laboratory (Hangzhou DIAN Medical Laboratory, Hangzhou, China) using dry ice for testing. For a detailed procedure of NTS testing, please refer to the attached document (Supplementary 1).
3.1. Bioinformatic Analysis
Real‐time basecalling and demultiplexing were performed using MinKNOW software. Reads with low quality were filtered out, and human host sequences were removed using Minimap2 against the human reference genome (hg38). Pathogen identification was performed using Centrifuge v1.0.3 with the NCBI nonredundant nucleotide (NT) database. When the data size of a sample reaches 50 Mb and the number of detected sequences for the internal control (Lactococcus lactis) exceeds 100, the sample is deemed to have passed the quality control, and further analysis is conducted to determine positive species.
4. Final Clinical Diagnosis
Each patient’s final diagnosis was established at discharge based on a comprehensive evaluation that included clinical presentation, radiologic findings, laboratory tests, pathology, and results from CMTs and NTS. Diagnoses were made jointly by two respiratory physicians. In case of disagreement, a panel of three experts reviewed the case to reach consensus. These diagnoses served as the reference standard for assessing the diagnostic performance of NTS and CMTs.
5. Results
5.1. Clinical Information
This study included 284 patients recruited from one hospital between June 2023 and September 2024, comprising 118 males (41.55%) and 166 females (58.45%). The clinical features are shown in Table 1. Ages ranged from 15 to 90 years, with a mean of 58.80 years. The most common symptoms were cough, sputum, and fever. Of the participants, 195 patients had one or more background diseases, with HBP being the most prevalent (n = 104, 36.62%). Posttreatment, 182 patients (64.08%) showed clinical improvement or complete cure, while four patients died. Among the 284 patients, 270 were classified as infection‐related, with pathogens being the primary cause of their lung infections. As shown in Table 1, CAP was the most common disease type (n = 211, 74.29%), followed by COPD (n = 37, 13.03%) and bronchitis (n = 24, 8.45%). Comorbidities such as HBP (36.62%), history of surgery and trauma (16.55%), and diabetes (8.45%) were also frequently observed.
5.2. Specimen Types and Pathogen Distribution in NTS
We analyzed the distribution of sample sources and pathogen types in this study, revealing key insights into the characteristics of pulmonary infections. The majority of the samples were obtained from BALF, accounting for 85.2% (242/284) of the total samples, followed by sputum with 11.62% (33/284) and hydrothorax contributing 3% (8/284) (Figure 1(a)). Only 1 sample was collected using a throat swab, representing less than 1% of the samples. The 259 pathogens identified were mainly bacteria, which accounted for 56.76% (147 cases) of the total infections, underscoring their dominant role in pulmonary infections. Mycobacterium species contributed to 12.74% (33 cases, including Mycobacterium tuberculosis, Nontuberculous mycobacterium, Mycobacterium abscess, and Mycobacterium ornithine), reflecting their importance in chronic and opportunistic infections. Fungal infections were identified in 15.44% (40 cases). Viral infections were also observed, with RNA viruses and DNA viruses comprising 7.72% (20 cases) and 6.56% (17 cases), respectively. Mycoplasma, Chlamydia, and spirochetes were less common, accounting for only 0.77% (2 cases) (Figure 1(b)).
Figure 1. Distribution of sample sources (a) and pathogen types (b) of NTS.(a)(b)
6. Comparison of Pathogen Detection Methods
A comparative analysis was performed to evaluate the effectiveness of CMTs and NTS in pathogen detection. Among the analyzed samples, 260 cases (91.6%) tested positive by NTS, and 208 cases (73.2%) tested positive by CMTs (Table 2). Notably, 8 cases (2.8%) were negative in both methods, and 192 cases (67.6%) were concordantly positive in both methods. However, 24 cases (8.5%) were exclusively detected as negative by NTS, whereas 76 cases (26.8%) were exclusively detected as negative by CMTs. The agreement analysis revealed 39 cases (13.7%) with full concordance, 143 cases (50.4%) with partial concordance, and 10 cases (3.5%) with discrepancies, highlighting significant differences between the two detection methods (Figure 2(a)).
Figure 2. Comparison of NTS and CMTs diagnostic performance. (a) The distribution of test results across NTS and CMTs, including positive (NTS+ and CMTs+), negative (NTS− and CMTs−), and overlapping categories (Double+ and Double−). The inset highlights the classification of matched, partly matched, and mismatched cases. (b) Diagnostic performance of NTS vs. CMTs (clinical diagnosis as reference; N = 284). Bars show point estimates with 95% CIs. Blue = NTS; red = CMTs.(a)(b)
The diagnostic performance is summarized in Figure 2(b). For NTS, sensitivity was 91.85%, specificity was 14.29%, accuracy was 88.03%, PPV was 95.38%, and NPV was 8.33%. For CMTs, sensitivity was 74.81%, specificity was 57.14%, accuracy was 73.94%, PPV was 97.12%, and NPV was 10.53%. Thus, NTS yielded higher sensitivity and overall accuracy, whereas CMTs demonstrated higher specificity; PPV was high and NPV low for both tests, consistent with the high disease prevalence. Paired McNemar comparison result showed a significant difference in overall accuracy favoring NTS (p = 2.09 × 10^5^) and a significant sensitivity advantage for NTS (p = 1.68 × 10^7^), while specificity did not differ significantly between methods (p = 0.114) (Table S1).
6.1. NTS Unveils Diverse Pathogens in Pulmonary Infections
In this study, we analyzed the pathogens in 284 patients with pulmonary infections, identifying a wide range of bacteria, fungi, viruses, and other microorganisms using NTS (Figure 3). The most frequently detected bacterial pathogens included Enterococcus faecalis (219 cases), Rothia mucilaginosa (218 cases), and Streptococcus mitis (184 cases) (Figure 3(a)). Among fungal pathogens, Candida albicans (154 cases) and Pneumocystis jirovecii (45 cases) were predominant (Figure 3(b)). Viral pathogens such as human betaherpesvirus 7 (63 cases) and human gammaherpesvirus 4 (58 cases) and SARS‐CoV‐2 (32 cases) were also identified (Figures 3(c) and 3(d)). The diversity of pathogens highlights the complexity of pulmonary infections and the importance of comprehensive diagnostic approaches.
Figure 3. Distribution of detected microorganisms across different pathogen categories. (a) Most prevalent bacterial species identified in this cohort (Top50). (b) Most prevalent fungal species identified in this cohort (Top10). (c) DNA viruses identified in this cohort (Top10). (d) RNA viruses identified in this cohort (Top10).(a)(b)(c)(d)
The NTS analysis revealed a broad spectrum of bacterial pathogens. Gram‐positive bacteria were the most common, with Enterococcus faecalis, Rothia mucilaginosa, and Streptococcus mitis being the top three most frequently identified. Other notable Gram‐positive bacteria included Granulicatella adiacens and Veillonella parvula. GNB were also identified, with Acinetobacter odontolyticus and Haemophilus influenzae among the more common ones. The presence of both Gram‐positive bacteria and GNB underscores the need for broad‐spectrum initial empiric therapy in pulmonary infections (Figure 3(a)). Fungal pathogens were also prevalent in the patient cohort. Candida albicans was the most frequently detected fungal pathogen, followed by Pneumocystis jirovecii and Aspergillus penicillioides. Other fungi such as Candida glabrata and Candida tropicalis were also identified. The detection of these fungi highlights the importance of considering fungal infections in patients with pulmonary symptoms, particularly in immunocompromised individuals (Figure 3(b)). Viral pathogens were identified in a significant number of patients. Human betaherpesvirus 7 and human gammaherpesvirus 4 were the most common, followed by human betaherpesvirus 5 and human alphaherpesvirus 1. Other viruses such as SARS‐CoV‐2 and human polyomavirus 5 were also detected (Figures 3(c) and 3(d)). The identification of these viruses suggests that viral infections play a substantial role in pulmonary infections and should be considered in the differential diagnosis. In addition to bacteria, fungi, and viruses, other microorganisms such as Mycoplasma pneumoniae (45 cases) were identified. These findings emphasize the diverse etiology of pulmonary infections and the value of NTS in detecting a wide range of pathogens. The identification of a wide variety of bacterial, fungal, viral, and other microbial pathogens underscores the complexity of these infections and the importance of accurate and rapid diagnostic methods to guide appropriate treatment.
6.2. Comparison of Fungal Detection Among NTS, CMTs, and Clinical Diagnosis
A total of 284 patients were included, among whom 60 were clinically diagnosed with fungal infections. NTS alone detected 153 positives, of which 49 were true positives. The sensitivity was 81.7% (49/60), specificity was 53.6% (120/224), PPV was 32.0% (49/153), and NPV was 91.6% (120/131). CMTs alone detected 42 positives, of which 24 were true positives. The sensitivity was 40.0% (24/60), specificity was 92.0% (206/224), PPV was 57.1% (24/42), and NPV was 85.1% (206/242) (Figure 4 and Table 3). Combined NTS + CMTs (defined as positive if either method was positive) detected 163 positives, of which 54 were true positives. The sensitivity was 90.0% (54/60), specificity was 51.3% (115/224), PPV was 33.1% (54/163), and NPV was 95.0% (115/121). NTS achieved higher sensitivity than CMTs but at the cost of reduced specificity and PPV. CMTs alone were highly specific but lacked sensitivity. Combined testing markedly improved sensitivity (90.0%) and NPV (95.0%), reducing the chance of missed diagnoses, but this came at the expense of lower specificity (51.3%) and PPV (33.1%), due to the accumulation of false positives when either test was considered sufficient for positivity. Therefore, the diagnosis of fungal infection cannot rely on a single test result; it must be made cautiously on the basis of comprehensive evaluation, avoiding “test‐driven” misdiagnosis and overtreatment.
Venn diagram of fungal detection results across NTS, CMTs, and clinical diagnosis.
6.3. Diagnostic Efficacy of NTS in Mixed Infections
We present the comparison of detection rates for mixed infections identified by NTS and traditional microbial culture methods. The analysis focused on two categories: infections involving two or more species and those involving two or more types (Table 4). NTS detected mixed infections with two or more species in 283 cases (99.65%), significantly higher than traditional culture methods, which identified such infections in only 16 cases (5.63%). The χ ^2^ test yielded a value of 499.68, with a p value less than 0.001, indicating a statistically significant difference between the two methods. For mixed infections involving two or more types, NTS identified these in 278 cases (97.89%), compared to traditional culture methods that detected them in 12 cases (4.23%). These results demonstrate that NTS has a markedly higher detection rate for mixed infections compared to traditional microbial culture methods. The significant differences observed (p < 0.001) underscore the enhanced sensitivity and comprehensiveness of NTS in identifying complex infection profiles, which is crucial for accurate diagnosis and appropriate therapeutic interventions.
6.4. Microorganism Distribution in CAP and COPD
In this study, we confirmed that the pathogen spectrum varied among different clinical types of pulmonary infection (Figure 5). In CAP, the main pathogens were bacteria and viruses. The frequently detected bacterial species were Streptococcus pneumoniae, Haemophilus influenzae, Prevotella melaninogenica, and Veillonella parvula. Viral pathogens included influenza A virus, human rhinovirus 89, and human metapneumovirus.
The comparative analysis of pathogen distribution across three categories of pulmonary infections: CAP (blue region); COPD (orange region).
The relatively high proportion of viruses indicates that bacterial‐viral coinfection is a major feature of CAP. In contrast, infections in COPD were mainly bacterial and fungal. The dominant bacterial species were Pseudomonas aeruginosa, Klebsiella pneumoniae, and Staphylococcus aureus, while Aspergillus fumigatus, Aspergillus flavus, and Candida albicans were the most common fungal pathogens.
A few slow‐growing and opportunistic organisms such as Mycobacterium tuberculosis and Nocardia farcinica were also found, consistent with the chronic and recurrent nature of infection in COPD. Several species, such as Haemophilus influenzae, Streptococcus mitis, and Veillonella atypica, appeared in both groups, suggesting a shared core airway microbiota. Overall, CAP was characterized mainly by bacterial‐viral coinfections, whereas COPD was dominated by bacterial‐fungal coinfections.
6.5. Microorganism Distribution in Patients With and Without HBP
To characterize the distinct microbial profiles of pulmonary infections between patients with and without HBP, we compared pathogen distributions in the HBP and non‐HBP groups. The results revealed differences in pathogen prevalence between the two groups (Figure 6).
The comparative analysis of pathogen distribution across HBP patients (light green region) and non‐HBP patients (yellow region). The middle merge region contains pathogens detected in both HBP and non‐HBP.
In the HBP group, commensal anaerobic bacteria were markedly enriched, including Veillonella atypica, Streptococcus parasanguinis, and Granulicatella adiacens. In contrast, non‐HBP patients showed higher detection rates of opportunistic and viral pathogens, such as Pseudomonas aeruginosa, Acinetobacter baumannii, Klebsiella pneumoniae, Aspergillus fumigatus, influenza A virus, and human coronavirus 229E. Some species, including Haemophilus influenzae and Streptococcus pneumoniae, were common to both groups.
These results indicate both shared and distinct microbial characteristics between hypertensive and nonhypertensive individuals. Hypertensive patients tended to harbor increased proportions of oral‐derived commensals, while nonhypertensive patients were more susceptible to opportunistic bacterial and viral infections. This difference suggests that HBP may influence airway microbial composition and highlights the importance of considering underlying conditions such as HBP in the clinical management of pulmonary infections.
7. Discussion
This study systematically analyzed the distribution of pathogens and the diagnostic performance of NTS compared with CMTs in 284 patients with pulmonary infections. Bacteria were the predominant pathogens, followed by fungi and viruses, with CAP being the most common type. Compared with CMTs, NTS demonstrated markedly higher sensitivity and detected a wider range of pathogens, especially in mixed infections. These findings are consistent with previous studies confirming the superior diagnostic yield of NTS in respiratory and systemic infections [15, 16].
NTS effectively identified diverse bacteria, fungi, and viruses, including Enterococcus, Candida, and Herpesviridae, that were frequently missed by traditional culture‐based methods. Its broad‐spectrum detection capability enables earlier diagnosis and more accurate antimicrobial therapy. Although CMTs retain high specificity, their dependence on culture limits detection of slow‐growing or low‐abundance pathogens. The combined use of both methods can enhance diagnostic accuracy, reduce false negatives, and improve etiological precision.
In this study, NTS also proved valuable for distinguishing pathogen profiles across pulmonary infection types. In CAP, the detection rate of viral pathogens such as influenza A and parainfluenza virus was significantly higher with NTS, suggesting that bacterial‐viral coinfections are common [17]. Early identification of viral infections is crucial for optimizing treatment, reducing unnecessary antibiotic use, and promoting targeted antiviral therapy. In contrast, infections associated with COPD were predominantly bacterial‐fungal. The main bacterial pathogens included Pseudomonas aeruginosa, Klebsiella pneumoniae, and Staphylococcus aureus, accompanied by opportunistic fungi such as Aspergillus fumigatus and Candida orthopsilosis[18]. These findings align with prior evidence that COPD patients are prone to polymicrobial colonization and secondary infections due to chronic airway inflammation, mucus retention, and impaired clearance [6, 7].
NTS further revealed distinct microbial patterns among patients with and without HBP (HBP vs. non‐HBP). In hypertensive individuals, commensal anaerobes such as Veillonella atypica, Streptococcus parasanguinis, and Granulicatella adiacens were more abundant, suggesting an altered airway microbial ecosystem. In contrast, nonhypertensive patients exhibited higher frequencies of opportunistic and viral pathogens, including Pseudomonas aeruginosa, Acinetobacter baumannii, Klebsiella pneumoniae, influenza A virus, and human coronavirus 229E. Shared respiratory pathogens such as Haemophilus influenzae and Streptococcus pneumoniae were detected in both groups, whereas Veillonella atypica was dominant among hypertensive patients. These results indicate that HBP may influence airway microbial composition, possibly through immune dysregulation or systemic inflammation, as also suggested by other studies [19, 20].
Importantly, NTS not only identified classical pathogens but also provided ecological insights into the airway microbiota. The coexistence of pathogens and commensal organisms implies that pulmonary infections represent ecological disturbances rather than isolated infectious events. The microbial imbalance observed in CAP, COPD, and hypertensive patients likely reflects both pathogenic processes and host‐microbiota interactions. This concept supports the growing view that infection susceptibility is closely linked to microbial dysbiosis, rather than the presence of a single dominant pathogen [21, 22].
Despite its advantages, NTS has limitations. Its high sensitivity can lead to false positives due to the detection of nonpathogenic or contaminant organisms. Therefore, interpretation requires correlation with clinical and radiological findings. In contrast, while CMTs exhibit higher specificity, they are often limited by false negatives, particularly for anaerobes, mycobacteria, or fungi with specific growth requirements. Furthermore, CMTs are less effective for viral detection, which is essential for CAP and other pulmonary infections [23]. Consequently, combining NTS and CMTs offers complementary strengths: NTS provides broad‐spectrum screening, while CMTs confirm clinical relevance and resistance profiles.
This study has several limitations. Being a single‐center study with a moderate sample size, generalizability may be limited. Future multicenter investigations with larger cohorts are necessary to validate these findings. Moreover, patient heterogeneity, including immune status, may influence microbial distribution and should be considered in subsequent research.
8. Conclusion
NTS provides higher sensitivity, broader pathogen coverage, and superior detection of complex infections compared with CMTs. It is particularly useful for the diagnosis of CAP, COPD, and other polymicrobial pulmonary infections. Furthermore, by identifying microbial differences between hypertensive and nonhypertensive patients, NTS expands understanding of host‐microbiota interactions and comorbidity‐related susceptibility. Although cost and technical demands currently limit its use, advances in sequencing efficiency and affordability are improving accessibility [19, 22]. With a turnaround time of approximately 48 h, substantially faster than traditional cultures, NTS facilitates rapid diagnosis and targeted therapy. Its integration into clinical workflows is expected to enhance pathogen detection, guide precise antimicrobial strategies, and contribute to the advancement of precision medicine.
Ethics Statement
Ethical approval was granted by the Ethics Committee of Chifeng Clinical College of Inner Mongolia Medical University (CK20250501).
Disclosure
All authors reviewed and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Ying Zhao designed the study, performed data collection, and wrote the manuscript. Guannan Ma performed data collection, conducted laboratory experiments, and wrote the manuscript. Tianxiao Ma collected clinical data. Yongshuai Miao and Heya Na participated in sample processing. Yuhui Liu conducted data analysis. Xiaohua Li designed the study, supervised the research, and edited the manuscript. Ying Zhao and Guannan Ma are co‐first authors of this article and contributed equally to this article.
Funding
This study was supported by the Natural Science Foundation of Chifeng (SZR24075).
Supporting Information
Detailed procedure of NTS testing. NTS testing: Respiratory tract samples were collected in sterile sputum containers and immediately transported on dry ice to a commercial laboratory (Hangzhou DIAN Medical Laboratory, Hangzhou, China) for testing.
Table S1: Detailed indicators of diagnostic performance.
Supporting information
Supporting Information Additional supporting information can be found online in the Supporting Information section.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giraudo C. , Evangelista L. , Fraia A. S. et al., Molecular Imaging of Pulmonary Inflammation and Infection, International Journal of Molecular Sciences. (January 2020) 21, no. 3, 10.3390/ijms 21030894.PMC 703783432019142 · doi ↗ · pubmed ↗
- 2Zhou Y. , Guo S. , He Y. et al., COVID-19 Is Distinct From SARS-Co V-2-Negative Community-Acquired Pneumonia, Frontiers in Cellular and Infection Microbiology. (2020) 16, no. 10, 10.3389/fcimb.2020.00322.PMC 730944932612961 · doi ↗ · pubmed ↗
- 3Peng Y. , Chen W. , Huang F. et al., SLC 38A 6 Expression in Macrophages Exacerbates Pulmonary Inflammation, Respiratory Research. (January 2023) 24, no. 1, 10.1186/s 12931-023-02330-8.PMC 988125436707853 · doi ↗ · pubmed ↗
- 4Choules M. P. , Wolf N. M. , Lee H. et al., Rufomycin Targets Clp C 1 Proteolysis in Mycobacterium tuberculosis and M. abscessus, Antimicrobial Agents and Chemotherapy. (February 2019) 63, no. 3, e 02204–e 02218, 10.1128/AAC.02204-18, 2-s 2.0-85062343855.30602512 PMC 6395927 · doi ↗ · pubmed ↗
- 5Snarr B. D. , St-Pierre G. , Ralph B. et al., Galectin-3 Enhances Neutrophil Motility and Extravasation into the Airways During Aspergillus fumigatus Infection, P Lo S Pathogens. (August 2020) 16, no. 8, 10.1371/journal.ppat.1008741.PMC 742828932750085 · doi ↗ · pubmed ↗
- 6Taddei L. , Malvisi L. , Hui D. S. et al., Airway Pathogens Detected in Stable and Exacerbated COPD in Patients in Asia-Pacific, ERJ Open Res. (September 2022) 8, no. 3, 00057–02022, 10.1183/23120541.00057-2022.36171985 PMC 9511156 · doi ↗ · pubmed ↗
- 7Yagyu K. , Ueda T. , Miyamoto A. , Uenishi R. , and Matsushita H. , Previous Moraxella catarrhalis Infection as a Risk Factor of COPD Exacerbations Leading to Hospitalization, COPD: Journal of Chronic Obstructive Pulmonary Disease. (December 2025) 22, no. 1, 10.1080/15412555.2025.2460808.39963887 · doi ↗ · pubmed ↗
- 8Wang C. , Hu J. , Gu Y. , Wang X. , Chen Y. , and Yuan W. , Application of Next-Generation Metagenomic Sequencing in the Diagnosis and Treatment of Acute Spinal Infections, Heliyon. (February 2023) 9, no. 3, 10.1016/j.heliyon.2023.e 13951.PMC 998484336879954 · doi ↗ · pubmed ↗