Pediatric severe sepsis: epidemiology and risk factors associated with acute kidney injury
Haibo Li, Ying Zhang, Hongyan Zhu, Ran Yu, Qi Zhou, Jiannan Song, Jiannan Wu, Wanli Ma, Zhanfei Hu, Jian Wang, Xuegao Yu, Hongyu Zhang

TL;DR
This study examines how acute kidney injury affects children with severe sepsis, finding that while AKI cases increased, mortality decreased due to better care.
Contribution
The study provides updated trends and risk factors for AKI in pediatric sepsis patients using a national database.
Findings
AKI incidence in pediatric sepsis rose from 2.7% in 2010 to 8.0% in 2019.
AKI was linked to a sevenfold higher mortality risk and longer hospital stays.
Mortality rates for PSS decreased from 32.4% to 17.9% between 2010 and 2019.
Abstract
Pediatric severe sepsis (PSS) is one of the leading causes of morbidity and mortality in children, incurring substantial social costs. Acute kidney injury (AKI) plays a critical role in determining PSS severity and prognosis. However, existing literature provides limited data regarding the risk factors associated with AKI in pediatric sepsis patients and the impact of AKI on hospital outcomes for these patients. This study aimed to analyze the temporal trends in incidence and outcomes of AKI among hospitalized PSS patients from 2010 to 2019, and identify associated risk factors; and assess the impact of AKI on in-hospital mortality and healthcare resource utilization. This study utilized the nationally representative National Inpatient Sample (NIS) database of the United States to conduct a retrospective analysis. All children aged 0 (infants) to 18 years who were diagnosed with severe…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
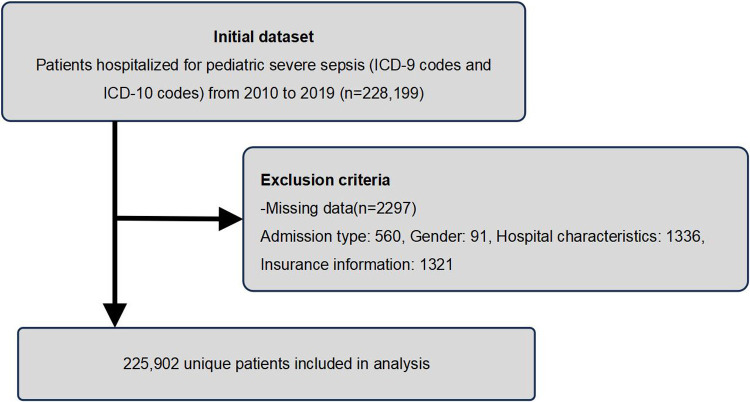 Figure 1
Figure 1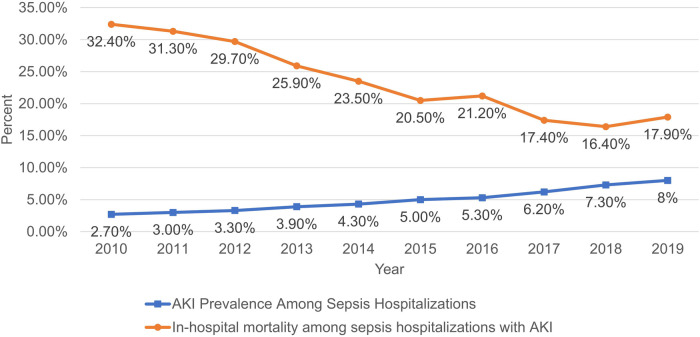 Figure 2
Figure 2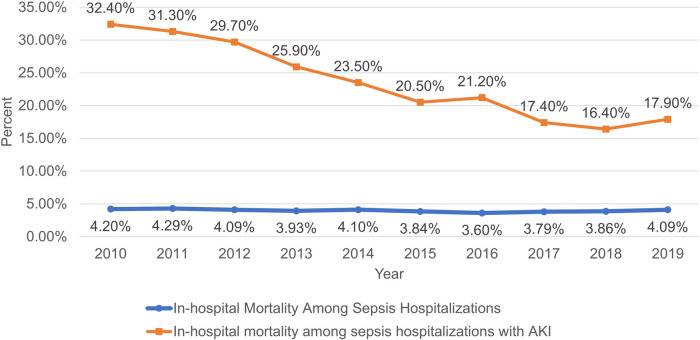 Figure 3
Figure 3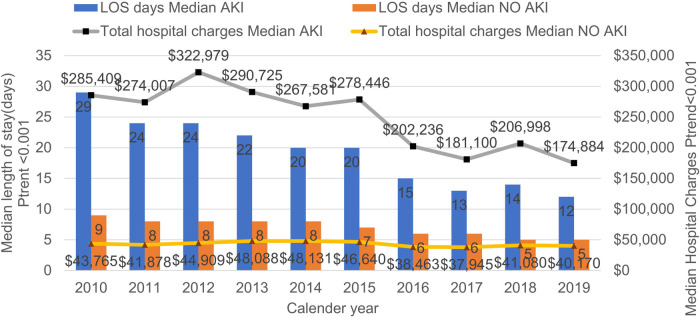 Figure 4
Figure 4| Characteristics | AKI | No AKI |
|
|---|---|---|---|
| Total ( | 10952 | 214,950 | |
| Total incidence (%) | 4.8 | ||
| Age (year) at admission Median (IQR) | 3 (0–17) | 0 (0–13) | <0.001 |
| Age group (%) | <0.001 | ||
| <1 year | 39.69 | 77.82 | |
| 1–3 | 11.47 | 7.83 | |
| 4–6 | 7.21 | 3.26 | |
| 7–10 | 9.75 | 3.60 | |
| 11–18 | 31.88 | 7.48 | |
| Gender (%) | <0.001 | ||
| Male | 53.64 | 55.23 | |
| Female | 46.36 | 44.77 | |
| Race (%) | <0.001 | ||
| White | 40.38 | 41.36 | |
| Black | 19.46 | 17.11 | |
| Hispanic | 20.90 | 21.99 | |
| Asian or Pacific Islander | 3.44 | 3.97 | |
| Native American | 0.99 | 0.88 | |
| Other | 14.84 | 14.69 | |
| Type of insure (%) | <0.001 | ||
| Medicare | 0.72 | 0.32 | |
| Medicaid | 57.39 | 56.38 | |
| Private insurance | 34.98 | 35.84 | |
| Self-pay | 1.92 | 3.13 | |
| No charge | 0.05 | 0.12 | |
| Other | 4.95 | 3.76 | |
| Bed size of hospital (%) | <0.001 | ||
| Small | 14.56 | 13.74 | |
| Medium | 21.38 | 26.81 | |
| Large | 64.05 | 59.46 | |
| Elective admission (%) | 6.59 | 3.46 | <0.001 |
| Type of hospital (teaching %) | 95.01 | 72.50 | <0.001 |
| Location of hospital | <0.001 | ||
| Urban (%) | 99.22 | 95.25 | |
| Rural (%) | 0.78 | 4.75 | |
| Region of hospital (%) | <0.001 | ||
| Northeast | 13.74 | 15.06 | |
| Midwest or North Central | 22.81 | 18.15 | |
| South | 40.54 | 42.46 | |
| West | 22.91 | 24.32 | |
| Outcome | |||
| Died (%) | 21.89 | 3.07 | <0.001 |
| LOS, median (IQR), d | 17 (1–145) | 7 (1–85) | <0.001 |
| TOTCHE, median (IQR) | $235,912 ($14,327–2,383,936) | $43,077 ($4,513–755,247) | <0.001 |
| Comorbidities | AKI | No AKI |
|
|---|---|---|---|
| Cardiovascular | |||
| Hypertension | 13.51 | 1.76 | <0.001 |
| Congestive heart failure | 5.98 | 0.56 | <0.001 |
| Rheumatoid arthritis/collagen vascular diseases | 0.73 | 0.10 | <0.001 |
| Peripheral vascular disorders | 2.78 | 0.41 | <0.001 |
| Valvular disease | 6.92 | 1.76 | <0.001 |
| Pulmonological | |||
| Pulmonary circulation disorders | 4.52 | 1.11 | <0.001 |
| Chronic pulmonary disease | 7.52 | 3.06 | <0.001 |
| Psychiatric | |||
| Depression | 2.31 | 0.44 | <0.001 |
| Alcohol abuse | 0.09 | 0.01 | <0.001 |
| Drug abuse | 2.95 | 0.54 | <0.001 |
| Paralysis | 6.66 | 1.78 | <0.001 |
| Psychoses | 0.96 | 0.18 | <0.001 |
| Endocrinological | |||
| Acquired immune deficiency syndrome | 0.03 | 0.01 | 0.152 |
| Diabetes, uncomplicated | 1.61 | 0.30 | <0.001 |
| Diabetes with chronic complications | 0.76 | 0.22 | <0.001 |
| Hypothyroidism | 3.38 | 0.99 | <0.001 |
| Obesity | 3.75 | 0.67 | <0.001 |
| Weight loss | 8.83 | 1.88 | <0.001 |
| Neurologic | |||
| Other neurological disorders | 15.93 | 3.94 | <0.001 |
| Renal | |||
| Renal failure | 6.44 | 0.60 | <0.001 |
| Gastrointestinal | |||
| Peptic ulcer disease excluding bleeding | 0.13 | 0.03 | <0.001 |
| Liver disease | 6.58 | 0.98 | <0.001 |
| Blood | |||
| Deficiency anemias | 8.95 | 2.69 | <0.001 |
| Chronic blood loss anemia | 0.85 | 0.24 | <0.001 |
| Coagulopathy | 33.43 | 4.99 | <0.001 |
| Fluid and electrolyte disorders | 65.63 | 17.67 | <0.001 |
| Comorbidities | Multivariate logistic regression | ||
|---|---|---|---|
| OR | 95% CI |
| |
| Cardiovascular | |||
| Hypertension | 1.750 | 1.57–1.95 | <0.001 |
| Congestive heart failure | 2.169 | 1.46–3.23 | <0.001 |
| Acute myocardial infarction | 3.272 | 0.98–10.93 | 0.054 |
| Rheumatoid arthritis/collagen vascular diseases | 2.970 | 1.88–4.68 | <0.001 |
| Peripheral vascular disorders | 1.191 | 0.91–1.56 | 0.205 |
| Deep vein thrombosis | 1.891 | 1.57–2.27 | <0.001 |
| Valvular disease | 1.864 | 1.65–2.10 | <0.001 |
| Peripheral vascular disease | 1.313 | 1.01–1.71 | 0.044 |
| Cardiac arrest | 2.445 | 2.01–2.97 | <0.001 |
| Arrhythmia | 1.165 | 0.67–2.02 | 0.585 |
| Heart failure | 1.249 | 0.81–1.92 | 0.310 |
| Pulmonological | |||
| Pulmonary circulation disorders | 0.968 | 0.81–1.16 | 0.727 |
| Respiratory disease | 1.572 | 1.27–1.95 | <0.001 |
| Pneumonia | 1.281 | 1.18–1.40 | <0.001 |
| Chest pain | 2.221 | 1.33–3.72 | 0.002 |
| Respiratory failure | 1.038 | 0.93–1.16 | 0.521 |
| Continuous trauma ventilation | 0.781 | 0.71–0.86 | <0.001 |
| Chronic pulmonary disease | 1.093 | 0.98–1.22 | 0.117 |
| Pulmonary embolism | 1.119 | 0.77–1.63 | 0.555 |
| Psychiatric | |||
| Depression | 1.683 | 1.35–2.10 | <0.001 |
| Alcohol abuse | 3.816 | 0.97–15.15 | 0.057 |
| Drug abuse | 1.254 | 1.02–1.54 | 0.030 |
| Paralysis | 1.204 | 1.06–1.37 | 0.005 |
| Psychoses | 1.678 | 1.11–2.53 | 0.013 |
| Endocrinological | |||
| Acquired immune deficiency syndrome | 0.543 | 0.11–2.71 | 0.457 |
| Diabetes, uncomplicated | 2.704 | 2.09–3.51 | <0.001 |
| Diabetes with chronic complications | 1.000 | 0.72–1.39 | 0.999 |
| Hypothyroidism | 1.188 | 0.99–1.42 | 0.060 |
| Obesity | 2.330 | 1.97–2.76 | <0.001 |
| Weight loss | 1.301 | 1.17–1.45 | <0.001 |
| Neurologic | |||
| Acute cerebrovascular disease | 1.375 | 1.08–1.75 | 0.010 |
| Other neurological disorders | 1.863 | 1.70–2.05 | <0.001 |
| Renal | |||
| Renal failure | 4.331 | 3.71–5.06 | <0.001 |
| Gastrointestinal | |||
| Gestrointestinal complication | 0.886 | 0.74–1.07 | 0.202 |
| Peptic ulcer disease excluding bleeding | 1.296 | 0.60–2.82 | 0.514 |
| Gastrointestinal bleeding | 1.916 | 1.41–2.60 | <0.001 |
| Liver disease | 1.904 | 1.67–2.17 | <0.001 |
| Blood | |||
| Deficiency anemias | 1.178 | 1.00–1.39 | 0.058 |
| Chronic blood loss anemia | 1.198 | 0.81–1.77 | 0.364 |
| Blood transfusion | 1.707 | 1.58–1.85 | <0.001 |
| Coagulopathy | 2.846 | 2.59–3.12 | <0.001 |
| Thrombocytopenia | 0.896 | 0.79–1.01 | 0.076 |
| Fluid and electrolyte disorders | 4.045 | 3.80–4.31 | <0.001 |
| Tumor | |||
| Lymphoma | 0.576 | 0.39–0.84 | 0.005 |
| Metastatic cancer | 1.023 | 0.74–1.42 | 0.890 |
| Solid tumor without metastasis | 0.628 | 0.50–0.79 | <0.001 |
| Variables | AKI | No AKI |
|
|---|---|---|---|
| Infection sites (%) | |||
| Gastrointestinal infection | 13.28 | 9.47 | <0.001 |
| Endocarditis infection | 0.66 | 0.08 | <0.001 |
| Skin tissue infection | 0.16 | 0.13 | 0.406 |
| Joint bone tissue infection | 0.02 | 0.01 | 0.163 |
| Intracranial infection | 0.11 | 0.04 | 0.003 |
| Bacterial infection (%) | |||
|
| 7.13 | 2.81 | <0.001 |
|
| 6.32 | 3.13 | <0.001 |
|
| 4.47 | 2.24 | <0.001 |
|
| 1.70 | 0.36 | <0.001 |
|
| 1.65 | 0.36 | <0.001 |
|
| 1.48 | 0.46 | <0.001 |
|
| 0.40 | 0.14 | <0.001 |
|
| 0.35 | 0.11 | <0.001 |
|
| 0.03 | 0.004 | 0.038 |
|
| 0.00 | 0.01 | 1.000 |
| Variable | Multivariate logistic regression | ||
|---|---|---|---|
| OR | 95% CI |
| |
| Infection sites | |||
| Urinary tract infection | 1.408 | 1.30–1.53 | <0.001 |
| Wound infection | 1.044 | 0.87–1.25 | 0.638 |
| Lung infection | 1.538 | 0.17–13.72 | 0.700 |
| Gastrointestinal infection | 0.972 | 0.91–1.04 | 0.412 |
| Skin tissue infection | 0.952 | 0.56–1.61 | 0.856 |
| Joint bone tissue infection | 0.923 | 0.18–4.73 | 0.924 |
| Endocarditis infection | 0.821 | 0.57–1.18 | 0.283 |
| Intracranial infection | 0.776 | 0.39–1.55 | 0.472 |
| Bacterial infection | |||
|
| 0.977 | 0.75–1.27 | 0.865 |
|
| 1.277 | 1.10–1.48 | 0.001 |
|
| 0.997 | 0.58–1.70 | 0.990 |
|
| 1.349 | 1.05–1.74 | 0.021 |
|
| 2.003 | 1.77–2.27 | <0.001 |
|
| 1.054 | 0.63–1.76 | 0.839 |
|
| 1.387 | 1.23–1.56 | <0.001 |
|
| 1.154 | 0.89–1.50 | 0.283 |
| Variable | Multivariate logistic regression | ||
|---|---|---|---|
| OR | 95% CI |
| |
| Age | |||
| <1 year | Ref | – | – |
| 1–3 | 1.394 | 1.29–1.50 | <0.001 |
| 4–6 | 2.205 | 2.01–2.42 | <0.001 |
| 7–10 | 2.616 | 2.40–2.85 | <0.001 |
| 11–18 | 4.317 | 4.05–4.61 | <0.001 |
| Female | 0.993 | 0.95–1.04 | 0.758 |
| Race | |||
| White | Ref | – | – |
| Black | 1.13 | 1.06–1.20 | <0.001 |
| Hispanic | 0.908 | 0.86–0.96 | 0.002 |
| Asian or Pacific Islander | 0.928 | 0.82–1.05 | 0.226 |
| Native American | 1.100 | 0.88–1.37 | 0.401 |
| Other | 1.017 | 0.95–1.09 | 0.611 |
| Number of Comorbidity | |||
| 0 | Ref | – | – |
| 1 | 2.471 | 2.29–2.67 | <0.001 |
| ≥2 | 3.120 | 2.80–3.48 | <0.001 |
| Type of insurance | |||
| Medicare | Ref | – | – |
| Medicaid | 1.903 | 1.42–2.56 | <0.001 |
| Private insurance | 1.798 | 1.34–2.42 | <0.001 |
| Self-pay | 1.463 | 1.05–2.04 | 0.025 |
| No charge | 0.546 | 0.21–1.45 | 0.226 |
| Other | 2.014 | 1.48–2.75 | <0.001 |
| Bed size of hospital | |||
| Small | Ref | – | – |
| Medium | 0.800 | 0.74–0.86 | <0.001 |
| Large | 1.047 | 0.98–1.12 | 0.156 |
| Elective admission | 0.833 | 0.76–0.91 | <0.001 |
| Teaching hospital | 3.015 | 2.73–3.33 | <0.001 |
| Urban hospital | 1.269 | 1.00–1.61 | 0.051 |
| Region of hospital | |||
| Northeast | Ref | – | – |
| Midwest or North Central | 1.226 | 1.14–1.32 | <0.001 |
| South | 1.169 | 1.09–1.25 | <0.001 |
| West | 1.181 | 1.10–1.27 | <0.001 |
- —National Natural Science Foundation of China10.13039/501100001809
- —Natural Science Foundation of Inner Mongolia Autonomous Region10.13039/501100004763
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Kidney Injury Research · Sepsis Diagnosis and Treatment · Central Venous Catheters and Hemodialysis
Introduction
Sepsis is a condition characterized by a malfunctioning immune reaction to infection, the dysregulation between the pro—coagulant and anticoagulant systems within the body is acknowledged as one of the pathogenic reasons underlying sepsis, resulting in potentially fatal organ dysfunction (1, 2). And the global health equity gap is particularly detrimental to children, increasing their susceptibility to infectious diseases. Studies have pointed out that each year, 50 million people worldwide are infected with sepsis, of whom half are newborns and children under the age of 19 (3). Pediatric severe sepsis (PSS) is a life-threatening condition and one of the leading causes of mortality in children worldwide. The prevalence of severe sepsis has been reported to be increasing in recent years (4), due to rising complications (5, 6), more frequent multidrug—resistant and opportunistic infections (7, 8), and improved surveillance and diagnosis (9, 10). Among the series of pathological changes caused by severe sepsis, the kidneys are among the most frequently affected organs. However, the diagnosis of AKI relies on changes in serum creatinine and urine output—indicators that are often lagging and non-specific, making early recognition and timely intervention particularly challenging (11, 12). In addition to insufficient renal perfusion, microvascular dysfunction, inflammation, and the response of cells to inflammatory injury can all contribute to sepsis-related acute kidney injury, which may progress to chronic kidney disease, imposing a substantial long-term health burden—a sequela often more significant than that of resolved dysfunction in other organ systems (13, 14). Children suffering from this severe illness generally face a heightened risk of sepsis-associated acute kidney injury (SA—AKI) (15, 16), which further elevates morbidity and mortality (17). Nevertheless, data on AKI's impact on hospital outcomes in PSS inpatients and its associated factors remain scarce.
The primary objectives of our study were as follows: (1) to evaluate the temporal trends in incidence and outcomes of PSS patients with concurrent AKI, as well as the associated factors; and (2) to determine the impact of AKI on sepsis patients during the same time period.
Methods
Study plan and source of data
The data was sourced from the National Inpatient Sample (NIS), which is part of the Healthcare Cost and Utilization Project. The NIS contains patient demographics, medical conditions, treatments, duration of stay, costs, insurance types, and mortality information. We conducted a retrospective analysis using a large sample spanning 2010–2019. As the study involved secondary analysis of de-identified data, institutional review board approval was not required. All patient data were anonymized, waiving the need for informed consent.
Study population
The study included pediatric patients (0–18 years) hospitalized for sepsis between 2010 and 2019. To avoid potential bias from repeated measures, only the first recorded hospitalization for sepsis within the study period was included for each unique patient. To examine demographic features, we excluded patients with missing information on sex, insurance type, elective admission, and hospital profile (including patients with duplicate missing data). Given that there are many patients lacking racial data, we were classify these patients into the “Other” category to preserve sample size. After exclusions, 225,902 PSS inpatients were included (Figure 1). For the purpose of this analysis, patients under 1 year of age were categorized in the “<1 year” group. Since this study did not assess AKI severity and in consideration of the administrative nature of the NIS database, AKI and sepsis was defined by the presence of any relevant diagnostic code (ICD-9-CM and ICD-10-CM) in the primary or secondary position during the hospitalization (Supplementary Tables 1–3).
Flow chart of the patient selection process in this study.
Outcome measures
The primary objective was to analyze epidemiological characteristics of PSS patients with and without AKI from 2010 to 2019, focusing on hospitalization status and mortality. In-hospital mortality was the primary outcome. Secondary outcomes were medical resource utilization, assessed by median length of stay and inflation-adjusted hospitalization costs. Comorbidities and infection-related data (site and pathogen) were also analyzed.
Statistical analysis
Categorical variables will be described as proportions and percentages, while continuous variables will be presented as medians and interquartile ranges. The χ^2^ test compared categorical variables; the Mann–Whitney U test compared quantitative data. Given the large sample size of this study (n = 225,902), to identify the most robust and clinically relevant predictors for the multivariate model and to mitigate the risk of model overfitting, we employed a more stringent entry criterion of p ≤ 0.001 from univariate analyses. Variables meeting this threshold were subsequently entered into a multivariate model, which will be adjusted for age, sex, race, median household income, payer status, type of admission, hospital characteristics including bed size, location/teaching status, and regions, and all baseline comorbidities. This adjustment is intended to significantly reduce the impact of other confounding factors.
In addition, annual percentage changes in PSS morbidity and mortality (with/without AKI) were calculated. The distributions of length of stay and hospitalization costs were positively skewed and contained extreme outliers—typical for healthcare utilization data—we therefore used medians to analyze trends, which are resistant to the influence of extreme values. We used time series analysis for evaluating trends of incidence rate, length of stay, and hospitalization charges during the study period.
Results
Baseline characteristics
Table 1 summarizes the basic characteristics of these patients. The overall incidence of acute kidney injury (AKI) in PSS patients was 4.8% (n = 10,952). Of 225,902 sepsis patients, 171,622 (75.97%) were infants <1 year. A higher proportion of PSS—AKI patients were male (53.64% vs. 46.36%, P < 0.001) and White (40.38%, P < 0.001). In addition, the median age of admission for PSS—AKI patients was 3 years (IQR: 0–17 years, P < 0.001), and most patients were covered by Medicaid (57.39%). At the same time, PSS—AKI patients were mainly admitted to urban medical institutions (99.22%) and were mostly treated in hospitals with larger beds (64.05%).
Trend analysis
The incidence of AKI among PSS in—patients has demonstrated a remarkable upward tendency. It rose from 2.7% in 2010 to 8% in 2019 (P < 0.001). Conversely, mortality declined from 32.4% to 17.9% (P < 0.001) (Figure 2). Annual in-hospital mortality was lower in PSS patients without AKI (3.07% vs. 21.89%, P < 0.001), though both groups showed decreasing mortality over time (Figure 3). Supplementary Table 4 shows the demographic data of PSS—AKI patients from 2010 to 2019. The total number of pediatric sepsis-related AKI hospitalizations gradually increased. As shown in Table 1 and Figure 4, PSS—AKI patients had significantly longer median hospital stays (17 vs. 7 days) and higher median costs (43,077) (P < 0.001).
Incidence and mortality of AKI in hospitalized patients with PSS from 2010 to 2019.
Annual mortality with and without AKI in hospitalized patients with PSS.
The median length of hospital stay and the median total hospital costs of hospitalized PSS patients with and without AKI from 2010 to 2019.
Comorbidities
The research findings indicate that PSS—AKI patients had a significantly higher associations of developing hypertension, encompassing both simple and complex types (13.51% vs. 1.76%), congestive heart failure (5.98% vs. 0.56%), rheumatoid arthritis/collagen vascular diseases (0.73% vs. 0.10%), peripheral vascular diseases (2.78% vs. 0.41%), and valvular diseases (6.92% vs. 1.76%) (P < 0.001) (Table 2).
Compared with non—AKI patients hospitalized for sepsis, AKI patients may also have potential associations with the following comorbidities: pulmonary circulatory disorders (4.52% vs. 1.11%), chronic lung diseases (7.52% vs. 3.06%), uncomplicated diabetes (1.61% vs. 0.30%), chronic complications of diabetes (0.76% vs. 0.22%), hypothyroidism (3.38% vs. 0.99%), other neurological disorders (15.93% vs. 3.94%), digestive ulcers without bleeding (0.13% vs. 0.03%), liver diseases (6.58% vs. 0.98%), anemia deficiency (8.95% vs. 2.69%), chronic hemorrhagic anemia (0.85% vs. 0.24%), and electrolyte disturbances (65.63% vs. 17.67%), and the like (Table 2).
As presented in Table 3, the correlation between AKI and comorbid conditions spanning from 2010 to 2019 is depicted. The odds ratio (OR) associated with the comorbidity of fluid and electrolyte imbalances within the PSS—AKI group was the greatest, followed by rheumatoid arthritis/collagen vascular diseases (OR 2.970; 95% CI 1.88–4.68) and coagulation disorders (OR 2.846; 95% CI 2.59–3.12) (all P < 0.001). Other common comorbidities included uncomplicated diabetes (OR, 2.704; 95% CI, 2.09–3.51), cardiac arrest (OR, 2.445; 95% CI, 2.01–2.97), obesity (OR, 2.330; 95% CI, 1.97–2.76), congestive heart failure (OR, 2.169; 95% CI, 1.46–3.23) (P < 0.001), etc. (Table 3).
Infections associated with PSS—AKI hospitalizations
Regarding infection sites (Table 4), gastrointestinal infections (13.28% vs. 9.47%) and endocarditis (0.66% vs. 0.08%) were more common in PSS-AKI hospitalizations (P < 0.001). Among pathogens, Staphylococcus aureus (7.13% vs. 2.81%), Escherichia coli (6.32% vs. 3.13%), Streptococcus (4.47% vs. 2.24%), Candida (1.70% vs. 0.36%), Pseudomonas (1.65% vs. 0.36%), Enterococcus (1.48% vs. 0.46%), anaerobic bacteria (0.40% vs. 0.14%), and Salmonella (0.35% vs. 0.11%) were relatively common (P < 0.001). The results of Table 5 indicate that, in the correlation analysis of PSS complicated by AKI and the sites of infection, only the factor of urinary tract infection exhibits statistical significance (OR = 1.408; 95% CI: 1.30–1.53; P < 0.001). For pathogens, Escherichia coli (E. coli) (OR = 2.003; 95% CI: 1.77–2.27; P < 0.001) and Staphylococcus aureus (OR = 1.387; 95% CI: 1.23–1.56; P < 0.001) were the most predominant pathogenic bacteria.
Multivariate predictors of in-hospital mortality in PSS—AKI patients
Table 6 compares predictors of mortality in PSS—AKI patients. The highest in-hospital mortality rate occurred in patients aged 11–18 years (OR, 4.317; 95% CI: 4.05–4.61; P < 0.001), and among black individuals (OR, 1.13; 95% CI: 1.06–1.20; P < 0.001). In addition, multiple comorbidities significantly increased the risk of mortality during hospitalization for patients with sepsis and acute kidney injury.
Discussion
Epidemiological characteristics of pediatric severe sepsis vary across studies, likely due to differences in populations, observation periods, and diagnostic criteria. We analyzed 225,902 associated hospitalizations of patients with sepsis aged 0–18 years between 2010 and 2019. Key findings included: (1) The incidence of AKI in PSS patients increased nearly three times (from 2.7% to 8.0%), while in-hospital mortality decreased by nearly half (from 32.4% to 17.9%); (2) PSS—AKI patients had significantly longer hospital stays (17 vs. 7 days) and higher hospitalization costs (43,077) than non—AKI patients, though both metrics showed a downward trend over time; (3) AKI risk was strongly associated with specific comorbidities (e.g., fluid-electrolyte disturbances, coagulation disorders), infection sites (e.g., gastrointestinal infections), and pathogens (e.g., Escherichia coli, Staphylococcus aureus); (4) We observed that among patients with PSS—AKI, the most common age groups were infants <1 year (39.69%) and 11–18 years (31.88%), and the incidence rate was higher in male patients (53.64% vs. 46.36%); (5) Those with multiple comorbidities had the highest in-hospital mortality.
Our study highlights a rising incidence of AKI in PSS inpatients over a decade, alongside declining mortality—a trend consistent with other studies, including in adults (4, 18, 19). This trend may reflect increased global attention to pediatric sepsis, promoting earlier and more aggressive management. Advances in diagnosis, monitoring, and treatment may also have mitigated disease severity. Thus, while overall AKI incidence increased, mortality declined. We also found that hospital stays and costs were substantially higher for PSS—AKI patients, though both decreased over time. Optimizing management to prevent AKI progression may help reduce length of stay and costs.
In the European Children's Infectious Disease Study (EUCLIDS), half of the children were confirmed to have invasive bacterial infections, and one-third of the survivors were discharged with disabilities (20). Numerous studies have shown that early identification of pathogens and timely administration of antibiotics are crucial and have beneficial effects on prognosis (21–23). In our study, Staphylococcus aureus, Escherichia coli and Streptococcus were prevalent; however, it should be noted that these pathogen-specific findings are based on clinical diagnosis codes rather than laboratory-confirmed microbiology. While this may not fully capture the true etiologies, the patterns observed can still offer valuable references for clinical prevention and intervention. Among all infection sites, gastrointestinal infections showed the closest association with PSS—AKI. It has been reported that factors such as a younger age, blood—related or immunological comorbidities, malignancies, and abdominal infections are linked to severe AKI (24), and in our study we noted an increased proportion of AKI in patients with water and electrolyte disorders, coagulation disorders, other neurological disorders, hypertension, chronic lung disease, valvular disease, paralysis, congestive heart failure. Among them, fluid and electrolyte imbalance, which is a recognized risk factor, usually reflects the cumulative effects of capillary leakage, active resuscitation and potential disease severity in sepsis. Coagulation dysfunction is also prominent in our model. It is a known component of organ dysfunction caused by sepsis and can exacerbate renal microvascular damage (25, 26). Reducing these risk factors and implementing early interventions may slow PSS—AKI progression.
In summary, integrating these data-driven strategies into clinical practice is crucial. This entails enhanced monitoring of high-risk patients—clinicians should maintain a heightened suspicion for AKI in neonates, male patients, and those with specific comorbidities such as fluid-electrolyte imbalances, coagulation disorders, or hypertension. Concurrently, focused attention on high-risk pathogens and infection sites necessitates proactive preventive measures and the prompt administration of appropriate antibiotic therapy. Implementing such a targeted approach may help mitigate the progression of PSS—AKI, thereby potentially alleviating its substantial healthcare burden and reducing associated mortality.
We utilized a large, nationally representative database to accurately capture real-world trends in morbidity and mortality. However, this study has several potential limitations. First, the retrospective, administrative nature of the data introduces the possibility of recording bias due to inconsistent identification and coding practices, which may lead to an underestimation of AKI incidence. Moreover, the database contains only in-hospital information, lacking post-discharge follow-up and out-of-hospital mortality data, thus providing an incomplete clinical picture. Second, we lacked data on specific exposures such as nephrotoxic medications and radiocontrast agents, which are known risk factors for AKI. Third, important treatment variables that influence sepsis outcome—including mechanical ventilation and renal replacement therapy—were not available for adjustment in our multivariate models, potentially confounding the observed association between AKI and mortality. Fourth, we could not fully address the interplay between comorbidities and pre-existing chronic kidney disease (CKD); excluding patients with pre-existing CKD or a history of AKI can mitigate such bias and enhance the validity of the findings. Fifth, although immunocompromised children were included in the cohort, we did not perform a dedicated subgroup analysis for this population, so our results may not fully reflect their distinct risk profile and outcomes. An additional limitation is the granularity of age data within this group; the use of a single “<1 year” category, necessitated by the database structure, precludes a more nuanced analysis distinguishing neonates from older infants. What's more, the risk factors, prevalence, clinical and microbiological etiology of newborns and infants (<1 year old) are significantly different from those of older children and adolescents, and their pathophysiological mechanisms are also quite distinct (27, 28), but we do not exclude them.
Conclusion
Between 2010 and 2019, the incidence of PSS with or without AKI increased among hospitalized children. AKI was associated with higher mortality, morbidity, longer hospital stays, and greater resource use, increasing public health burden. However, with the deepening of pediatric sepsis research and the improvement of medical level, the overall mortality rate of PSS has decreased, especially the mortality rate of PSS patients with AKI has shown a significant decreasing trend. Therefore further research and technological innovation are necessary to improve early diagnosis of AKI, identification of risk factors, and timely implementation of preventive treatment, This is of crucial significance for improving children's health and reducing the risk of adverse consequences caused by infections and related diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Levi M van der Poll T. Coagulation and sepsis. Thromb Res. (2017) 149:38–44. 10.1016/j.thromres.2016.11.00727886531 · doi ↗ · pubmed ↗
- 2Singer M Deutschman CS Seymour CW Shankar-Hari M Annane D Bauer M The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. (2016) 315(8):801–10. 10.1001/jama.2016.028726903338 PMC 4968574 · doi ↗ · pubmed ↗
- 3Watson RS Carrol ED Carter MJ Kissoon N Ranjit S Schlapbach LJ. The burden and contemporary epidemiology of sepsis in children. Lancet Child Adolesc Health. (2024) 8(9):670–81. 10.1016/S 2352-4642(24)00140-839142741 · doi ↗ · pubmed ↗
- 4Hartman ME Linde-Zwirble WT Angus DC Watson RS. Trends in the epidemiology of pediatric severe sepsis*. Pediatr Crit Care Med. (2013) 14(7):686–93. 10.1097/PCC.0b 013e 3182917 fad 23897242 · doi ↗ · pubmed ↗
- 5Wen SW Smith G Yang Q Walker M. Epidemiology of preterm birth and neonatal outcome. Semin Fetal Neonatal Med. (2004) 9(6):429–35. 10.1016/j.siny.2004.04.00215691780 · doi ↗ · pubmed ↗
- 6Magee JC Krishnan SM Benfield MR Hsu DT Shneider BL. Pediatric transplantation in the United States, 1997–2006. Am J Transplant. (2008) 8(4 Pt 2):935–45. 10.1111/j.1600-6143.2008.02172.x 18336697 · doi ↗ · pubmed ↗
- 7Kunz AN Brook I. Emerging resistant gram-negative aerobic bacilli in hospital-acquired infections. Chemotherapy. (2010) 56(6):492–500. 10.1159/00032101821099222 · doi ↗ · pubmed ↗
- 8Gudiol C Bodro M Simonetti A Tubau F González-Barca E Cisnal M Changing aetiology, clinical features, antimicrobial resistance, and outcomes of bloodstream infection in neutropenic cancer patients. Clin Microbiol Infect. (2013) 19(5):474–9. 10.1111/j.1469-0691.2012.03879.x 22524597 · doi ↗ · pubmed ↗