Age-related hearing loss and balance disorders: analysis of interactions and clinical implications in older persons. Systematic review and meta-analysis
Andrea Frosolini, Leonardo Franz, Leonardo Calvanese, Valeria Caragli, Daniela Parrino, Cristoforo Fabbris, Giulio Badin, Michael Negrisolo, Roberta Cenedese, Lisa Doretto, Giuseppe Brescia, Cosimo de Filippis, Elisabetta Genovese, Elisabetta Zanoletti, Gino Marioni

TL;DR
This paper reviews how age-related hearing loss is linked to balance issues and falls in older adults, suggesting that hearing aids and rehabilitation could help reduce fall risks.
Contribution
The study provides a systematic review and meta-analysis showing that hearing loss contributes to balance problems and fall risk in older adults.
Findings
ARHL is associated with slower mobility and higher odds of falls.
Hearing aid use improves balance in older adults with ARHL.
Age is a major factor in mobility decline, but ARHL adds modifiable risk.
Abstract
Age-related hearing loss (ARHL) frequently coexists with balance disorders in older persons, but the mechanisms and rehabilitative leverage of this association remain unsettled. We synthesized evidence on interactions between ARHL and vestibular/gait dysfunction, quantified mobility and fall outcomes, and appraised clinical implications for prevention. Following PRISMA and a registered PROSPERO protocol, we searched PubMed (MEDLINE), Scopus and Web of Science Core Collection. Inclusion required adults ≥65 years, ARHL and quantitative vestibular/balance outcomes. Forty studies met the criteria. Vestibular pooling was infeasible due to heterogeneous designs and metrics. In quantitative analysis, continuous outcomes were meta-analysed as standardized mean differences (SMD) (Hedges g) using random effects (REML) for ARHL–control contrasts and a fixed effect for within-participant Hearing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
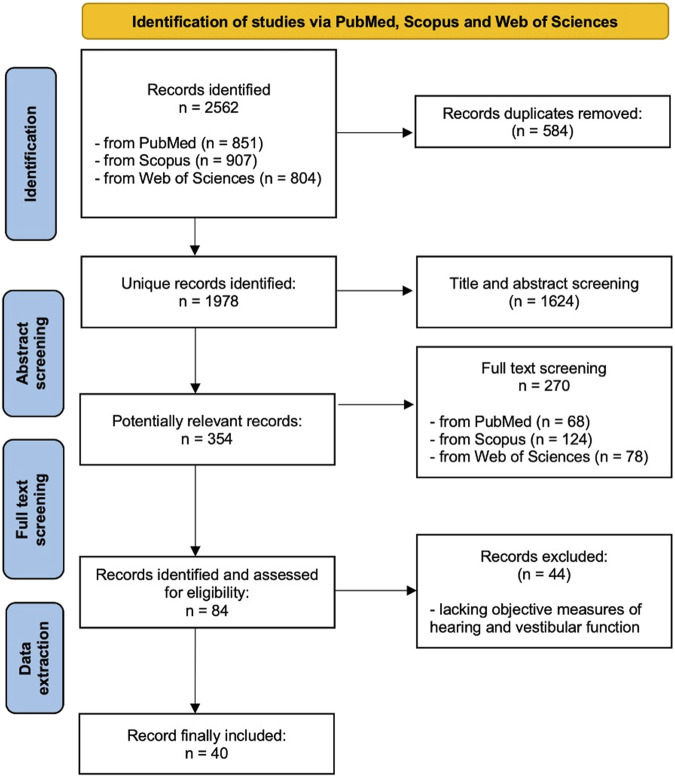 FIGURE 1
FIGURE 1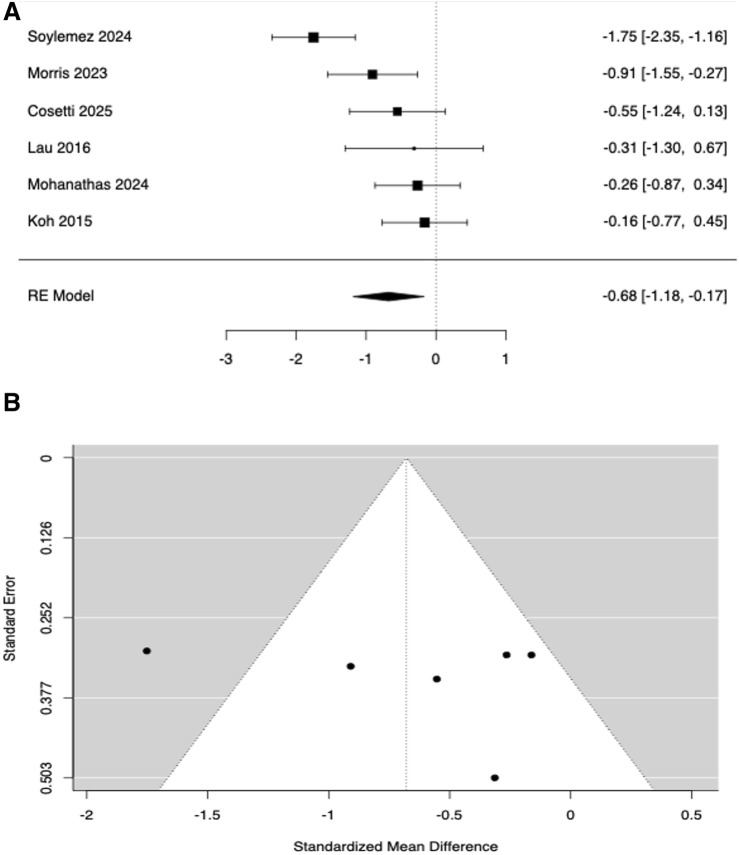 FIGURE 2
FIGURE 2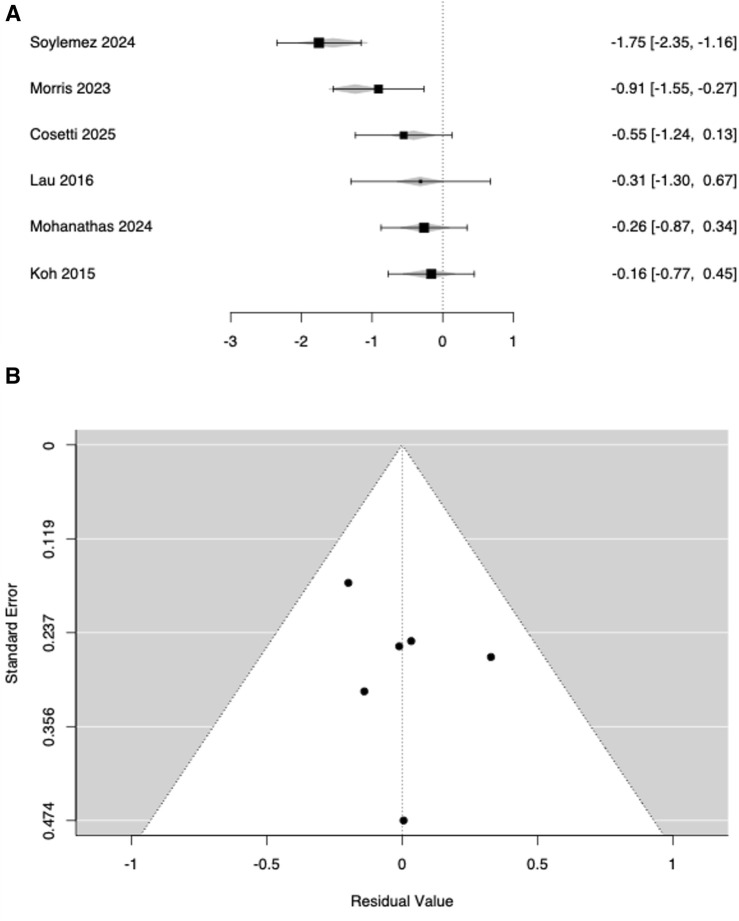 FIGURE 3
FIGURE 3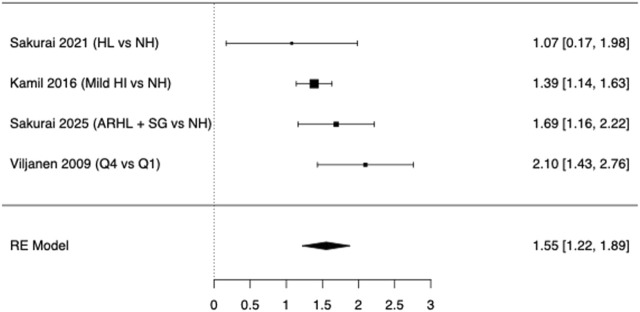 FIGURE 4
FIGURE 4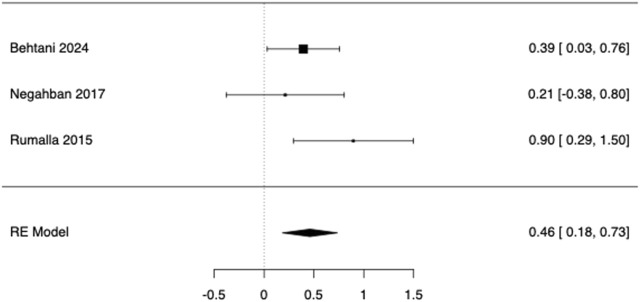 FIGURE 5
FIGURE 5| First author, year | Country | Design | Risk of Bias | Population (n; definition; mean age) | Comparison | Measure | Outcome |
|---|---|---|---|---|---|---|---|
|
| Portugal | RCS | M/S | 40; ENT patients; 70 | Young adults | TCR | No significant TCR differences between groups; significant correlation between PTA and TCR |
|
| Canada | CS | L | 37; healthy elderly; 70.4 | Young adults | vHIT; cVEMP; vestibular threshold | Older adults had higher heave and pitch detection thresholds |
|
| Turkey | CS | L | 63; HL patients; 67.2 | Age-matched non-HL | cVEMP | Significant differences between groups in VEMP latency and amplitude |
|
| United States | RCS | M | 149; CI candidates; 74.4 | NA | TCR | High prevalence of abnormal preoperative vestibular testing |
|
| Malaysia | CS | M | 135; ENT patients; 65.3 | NA | vHIT | Prevalence of vestibular dysfunction is independently associated with ageing and presbycusis |
|
| France | CS | L | 53; ARHL; 84.2 | Subgroup: Expected ARHL | VNG; vHIT | No significant associations between untimely ARHL and presby-vestibulopathy, or between the PTA high and presby-vestibulopathy |
|
| United States | CS | M | 51; Elderly volunteer; 77.1 (estimate) | NA | htDVA; cVEMP, oVEMP. | PTA correlated with saccular (not utricular) function |
| First author, year | Country | Design | Risk of Bias | Population (n; definition; mean age) | Comparison | Measures | Outcome |
|---|---|---|---|---|---|---|---|
|
| Germany | CS | M | 16; Elderly; 67.1 | NA | Sway during walking | Auditory information significantly improved postural control during walking |
|
| Canada | CS | M | 32; ARHL; 70.7 | Age-matched non-HL; young adults | DGI; Sit to stand Task; ABC scale; custom made perturbation plat- form | ARHL group demonstrated greater dual-task costs in noise leading to worst balance performer |
|
| United States | CS | M | 20; Elderly HL; 69) | Age-matched non-HL | TUG; DHI; ABC scale | Those with BHL performed slower on sub-component analysis of the instrumented TUG compared with age-matched control |
|
| Thailand | CS | M | 828; Elderly; 69.6 | Subgroup analysis | Survey | All age groups reported dizziness and vertigo but the elderly over 75 years reported more falls with a statistical significance |
|
| Brazil | CS | M | 247; ELLO Project: Study on Aging and Longevity; 68.4 | Subgroup: SNHL | Posturography | Elderly individuals with HL presented greater instabilities in the posturographic evaluation |
|
| Norway | CS | M | 42; MCI geriatric patients; 71.1 | Age-matched controls | OptoGait System | Demands on attentional control dependent on hearing acuity affects gait negatively in healthy older adults and aMCI individuals |
|
| United States | PCS | M | 1168; community-dwelling elderly HL; 74.3 (estimate) | Age-matched non-HL | Falls | HL is independently associated with greater odds of falling over time in older adults. |
|
| Republic of Korea | CS | M | 46; elderly; 76 | Subgroup: SNHL | TUG; OLST | Significant correlation between hearing loss and static balance |
|
| Norway | CS | L | 4101; HUNT4; | NA | SPPB | Increased hearing threshold is associated with poor physical performance |
|
| Norway | CS | M | 50; ARHL and HA; 76.2 | Age-matched non-HL | SPPB; Posturography; DHI | HL was associated with worse physical performance as measured by SPPB, postural sway, and gait variability |
|
| Canada | CS | M | 8; bilateral HL and HA; 73.3 | Age-matched non-HL | Kinematic parameters (TUG) | HL group demonstrated more overall stride time variability than the NH group |
|
| United States | PCS | M | 144; PACE; 74 | NA | Falls | More falls over 3 years among participants with HL at baseline |
|
| United States | PCS | M | 637; OKLAHOMA Studies cohort; 73.9 (estimate) | Subgroup: no HL; mild; moderate; severe | Tinetti Balance Scale; 50 feet time walk | ARHL is associated with reduced life expectancy, probably mediated through an adverse impact on balance |
|
| United States | CS | M | 14; elderly BHL; | UHL; NH | TUG; ABC; Visual Vertigo Analog Scale; Four-Square Step Test | Adults with BHL demonstrated a pattern of balance impairment |
|
| Germany | PCS | L | 6480 | NA | Falls | The age-adjusted annual fall rate did not differ significantly by hearing category, nor did the risk of incident fracture |
|
| Japan | CS | M | 107; Elderly volunteers; 76.5 | Subgroup: HL; no HL | Gait speed stride length and stride time variability in walking; Falls | The association between HL and increased gait variability could jeopardize gait control during daily activities leading to increased risk of accidental falls |
|
| Japan | RCS | M/S | 810; Elderly (Otassha and REPRINTS studies); 74 (estimate) | Subgroup: normal; mild and moderate HL | Gait speed (m/s) in timed 5-meter walk; Falls | Interactions between gait performance and moderate hearing loss on both global cognition and the occurrence of falls |
|
| Japan | PCS | M | 786; Elderly (Otassha study); 72.9 | Subgroup: based on ARHL and Slow Gait | Gait speed (m/s) in timed 5 and 10 meters walk; Falls | Simultaneous presence of ARHL and SG significantly increased the risk of multiple falls, fall-induced fractures, and minor injuries |
|
| United States | CS | L | 80; ENT outpatients; 73.7 | NA | Gait parameters in 100m walking; DHI | Importance of auditory feedback for balance and coordination; right ear advantage for the influence of auditory feedback on gait |
|
| Finland | CS | L | 423; FITSA; 68.6 | Between female twins | Posturography; Falls | People with poor hearing acuity have a higher risk of falls, which is partially explained by their poorer postural control |
|
| Finland | PCS | L | 434; FITSA; 68.6 (Estimate) | Subgroup: BEHL 0.5–4 kHz <21dB; BEHL 0.5–4 kHz >21dB | Walking speed, endurance and difficulty | Hearing acuity correlated with mobility, which may be explained by the association between impaired hearing and poor balance |
|
| Germany; Australia | CS | M | 73; Elderly volunteers; 71.2 (estimate) | Subgroup: no HL; Mild HL; Moderate/severe HL | Gait parameters in 10m walk | Walking speed was reduced accompanied by decreased step length and increased cadence in people with more severe hearing loss |
| First Author, Year | Country | Study Design | Risk Of Bias | Population (n; definition; age in years) | Intervention: administration | Measure | Outcome |
|---|---|---|---|---|---|---|---|
|
| Canada | CS | L/M | 30; ARHL and HA; 69 | HA: ON | Posturography; modified clinical sensory integration in balance test (mCTSIB) | Beneficial impact on postural control when visual and somatosensory inputs were reduced. |
|
| Canada | CT | M | 42, Elderly; 68.05 | Cognitive and Aerobic Training: simultaneous | Sit-to-Stand task; Posturography | All participants improved on a measure of chair rises; there was no benefit to standing balance; advantage to Sequential training |
|
| Canada | CS | M | 22; ARHL and HA; 75.1 | HA: ON | Posturography | Did not remarkably improve balance |
|
| United States | CS | M | 14; Elderly HL and HA; 77 | HA: ON | Romberg; Tandem | Significant improvement in balance and decreased risk of falling |
|
| United States | CS | M | 299; Elderly HL and HA; 73.8 | HA: aided | Fall Risk Questionnaire (FRQ) | Lower odds of falling and reduction in fall risk |
|
| United States | RCS | M | 14109; Elderly HL and HA; 75.8 | HA: aided | Falls and fall-related injuries | Delay or prevention of fall-related injuries |
|
| Italy | CT | M | 15; ARHL and dizziness; 75.1 | HA: baseline | Conley Scale; DHI | Reduced the risk of falls and improved the spatial memory |
|
| Japan | CT | M | 10; ARHL; 81 | HA: baseline | Gait (speed, time, length) | Improved gait performance |
|
| Turkey | CS | M | 30; Outpatients HL and HA; 73 | HA: aided | TUG | Improved TUG in Dual task condition |
|
| IRAN | CS | L | 47; Outpatient Audiology; 67.4 | HA: ON | Posturography | Significant improvement in postural stability |
|
| Thailand | CT | L | 215; Elderly reporting dizziness; 67.4 | Cawthorne-Cooksey exercises: 20 weeks | Posturography | Helpful and acceptable: 90% satisfaction |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVestibular and auditory disorders · Hearing Loss and Rehabilitation · Hearing, Cochlea, Tinnitus, Genetics
Introduction
1
Sensory function integrity reflects the nervous system’s ability to receive, process, organize and integrate the information recognized by multiple sensory modalities, including the senses of sight, hearing, smell, taste, touch, movement, gravity and posture (Kutlu et al., 2024). Sensory skills allow humans to experience and react to their surroundings; therefore, an optimal and effective multisensory integration is essential for strengthening environmental adaptation (Kutlu et al., 2024; Brown et al., 2001). Among higher-order functions relying on multisensory integration, postural control and balance are particularly sensitive to sensory decline. Accordingly, growing evidence has suggested that sensory impairments, such as hearing loss (HL), can compromise balance and postural stability and increase the risk of falls (Lavie et al., 2024; Jiam et al., 2016). Moreover, untreated HL negatively impact many aspects of life – cognitive status, loneliness, depression and reduced quality of life (Lavie et al., 2024).
Both HL and balance disorders (BD) are common among adults aged over 60 years, with a reported prevalence around 20%–30% and 60%, respectively (Roth et al., 2011; Semenov et al., 2016). Nonetheless there is limited knowledge about the complex interplay between HL and BD (Zuniga et al., 2012; Riska et al., 2022; Teplitxky et al., 2023), thus further investigation into proper audiological assessments and interventions for the older persons are required. Several theories have been proposed to explain the relationship between HL and BD. Primarily, HL and dizziness are the results of a common age-related deterioration of both anatomical and physiological cochlear-vestibular functions. The human auditory and vestibular systems are located in the inner ear; therefore, any deterioration of these structures due to aging could contribute to postural instability (Viljanen et al., 2009a; Kurtaran et al., 2016). From an embryological point of view, the cochlea and saccule develop from the same origin in the membranous labyrinth, which is innervated by the inferior portion of the vestibular nerve. Furthermore, the saccule plays the role of an acoustic-sensitive organ in lower species; therefore, as a vestibular-sensitive organ, it can be considered as a late development in humans (Kurtaran et al., 2016). Chronic noise exposure, along with molecular mechanisms such as inflammation, ototoxicity, oxidative stress and genetic factors have been proposed as common factors that link cochlear and vestibular pathophysiology (Paplou et al., 2023). Moreover, HL can directly affect balance by reducing the auditory input. Postural stability relies on sensory inputs, including visual, vestibular and somatosensory systems, and auditory information has been demonstrated to potentially contribute to balance by acting as auditory biofeedback (Kurtaran et al., 2016; Vitkovic et al., 2016). The decline in listening quality increases the ‘listening effort’ required to process and comprehend auditory signals reallocating cognitive resources toward auditory processing and thereby reducing those available for postural control, gait regulation, and other balance-related tasks (Wang et al., 2024; Kim et al., 2025). Therefore, patients with significant HL use much of their cognitive capacity for hearing, leaving less available for balance control (Kim et al., 2025). Furthermore, individuals with asymmetric hearing have a higher postural instability risk compared to those with symmetric hearing (Wang et al., 2024). Sound localization depends on interaural differences in signal timing and intensity. Thus, individuals with asymmetric hearing may experience greater difficulties in localizing sound sources, consequently impairing their postural stability (Wang et al., 2024).
The objective of this review is to systematically analyse the existing literature on auditory and vestibular functional decline in the older persons, investigating their mutual interactions, associated health outcomes, and implications for clinical management and preventive strategies. We aim to provide evidence-based recommendations for integrated clinical practice and public health policies.
Materials and methods
2
Protocol registration and research questions
2.1
This systematic review protocol was developed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and registered on the PROSPERO database (registry number PROSPERO 2025 CRD420251019918). The research question was formulated as follows: “What are the interactions between auditory and vestibular functional decline in older adults, their associated health outcomes, and implications for clinical management and preventive strategies?” and structured according to Patient/Population/Problem, Intervention, Comparison, and Outcome (PICO) criteria (Vallamchetla et al., 2025).
Search strategy and eligibility criteria
2.2
A comprehensive search was conducted in three bibliographic databases—PubMed (MEDLINE), Scopus, and Web of Science Core Collection (WOS) —from database inception to 31 March 2025 (final search conducted on 31 March 2025). These sources were selected a priori to maximize coverage while ensuring reproducibility. In addition, reference lists of included studies and relevant reviews were screened to identify any potentially eligible articles not captured by database indexing. Used keywords included “hearing loss,” “vestibular dysfunction,” “balance disorders,” “aging,” “elderly,” “falls,” and combinations thereof.
Studies were eligible for inclusion if they met all the following criteria: i) Included adults aged ≥65 years (either in the whole population or in identifiable subgroups [this age represents the internationally accepted definition of “older adults” in geriatric medicine (e.g., WHO guidelines]) experiencing age-related HL (presbycusis) diagnosed through pure tone audiometry; ii) original clinical articles with quantitative data; iii) explicit investigation of the interaction or association between auditory functions, and their impact on vestibular function, balance performance or fall risk; iv) English as publication language. Interventions or exposures of interest included audiological rehabilitation strategies such as hearing aids (HA), cochlear implants (CIs) and auditory training; vestibular rehabilitation programmes; and combined auditory-vestibular or sensory integration therapies. Studies were also considered if they examined relevant exposures such as underlying audiological pathologies. When present, the controls included healthy older adults without hearing or balance disorders, no intervention or standard care, or alternative rehabilitative interventions.
Studies were excluded if they met any of the following criteria: i) Population aged <65 years or no subgroups’ data to be isolated from over-65 patients; ii) focused on acute conditions or neurological diseases unrelated to aging; iii) studies based on animal models or other preclinical investigations, reviews, editorials, commentaries, or case reports, conference abstracts without full data and other qualitative studies without quantitative measurements; iv) interventions not of interest: studies involving surgical, pharmacological, or rehabilitative interventions unrelated to auditory or vestibular function; investigations focused on acute trauma, inflammatory disease, or non-sensory medical conditions.
Study selection and eligibility criteria
2.3
Four independent reviewers (LC; VC; MN; AF) conducted the initial screening based on titles and abstracts, applying pre-defined inclusion and exclusion criteria. Articles selected underwent full-text screening to confirm eligibility. Studies without clear methodological rigour, lacking relevant outcomes, or with incomplete data were ruled out. Disagreements during the screening process were resolved by consensus or consultation with a senior author.
Data extraction and quality assessment
2.4
Data extraction was independently performed by the same 4 independent reviewers (LC; VC; MN; AF) using a standardized extraction form. Extracted data included: authors, publication year, study design, demographic details with focus on tendency and dispersion measures of age, methods of auditory and vestibular/gait assessment, key outcomes, findings and clinical implications. If manuscripts lacked sufficient data, they were excluded during this phase and the reasons have been reported within the Results section. The quality of studies was evaluated using appropriate Cochrane risk-of-bias tools based on study design (Sandoval-Lentisco et al., 2024). Discrepancies were settled through consensus.
Data synthesis and analysis
2.5
Extracted data were synthesized using a structured narrative synthesis: studies were grouped a priori by outcome domain (vestibular function, balance/gait performance, fall outcomes, and rehabilitative interventions), and findings were summarized in terms of direction, consistency, and clinical relevance. Where appropriate, a quantitative summary was performed. For continuous outcomes, time up and go (TUG), we used standardized mean differences (SMD) as the summary effect. Between-group comparisons (HL vs. controls) were pooled with a random-effects model using the Restricted Maximum Likelihood (REML) estimator to account for between-study variability; effects were coded so that negative values indicated worse performance in the HL group. For falls (binary outcomes), when studies reported falls by hearing status, we used reported odds ratios (ORs) and 95% confidence intervals where available; otherwise, we reconstructed ORs and standard errors from 2 × 2 tables. To preserve independence, we retained one contrast per study a priori. We prioritized “any fall” over alternative endpoints and 12-month recall. Effects were coded so that OR>1 indicates higher odds of falling in the age-related hearing loss (ARHL) group. As robustness checks, we repeated the model after excluding the non-12-month window and the ≥2-falls endpoint. For within-participant ON–OFF hearing-aid contrasts, the primary model was fixed-effect (inverse-variance weighting) because k was small (k = 3) and τ^2^ was poorly estimable. Effects were coded so that positive values indicated better performance with HA ON (ON–OFF). For ON–OFF studies reporting multiple stances/metrics, we pre-specified a single challenging static stance (eyes-closed on foam or closest analogue) and one primary posturography metric per study to minimize multiplicity. A two-sided p < 0.05 was considered statistically significant. Heterogeneity was assessed with the Q-test, I^2^, and τ^2^. Outlier/influence diagnostics used studentized residuals and Cook’s distance. To explore the influence of age imbalance between groups in the HL-vs-control synthesis, we performed a mixed-effects meta-regression using the mean age difference (HL–control) as a continuous moderator. For the ON–OFF analysis (k = 3), meta-regression was considered exploratory only. Potential small-study effects were examined visually (funnel plots) and statistically (Egger’s regression, Begg–Mazumdar rank correlation, Rosenthal’s fail-safe N). Analyses were conducted in jamovi (version 2.3; The jamovi project, Sydney, Australia; accessed 29 July 2025).
Results
3
Search results, general characteristics and quality assessment of included studies
3.1
The initial database search yielded a total of 2,562 records across three major sources: Scopus (n = 907), WOS (n = 804), and PubMed (n = 851). After removing duplicates, a total of 1,978 unique records were identified. These entries underwent title and abstract screening to assess relevance according to the predefined inclusion and exclusion criteria outlined in the PROSPERO protocol, thus identifying 354 potentially relevant studies. After full-text screening, 270 articles (124 from Scopus, 78 from WOS, and 68 from PubMed) were excluded due to the following reasons. Irrelevant outcomes [e.g., did not assess hearing, vestibular, or gait parameters): 71 articles (26.3%)]; wrong population [e.g., non-elderly subjects, paediatric cohorts, or undefined age groups: 48 articles (17.8%)]; inadequate study design [e.g., narrative reviews, editorials, case reports, or conference abstracts: 44 articles (16.3%)]; missing or unclear methodology [e.g., small sample size, no control group, or lacking statistical analysis: 29 articles (10.7%)]; non-English language or full text not accessible [22 (8.1%)]; cognitive or psychosocial focus without audiological/vestibular relevance [18 (6.7%)]; combined populations without age-stratified data [16 (5.9%)]; other reasons (e.g., focused solely on device engineering, occupational noise, or unrelated imaging findings: 22 (8.1%)]. The final pool of articles that underwent data extraction consisted of 84 manuscripts. After data extraction additional 44 manuscripts were excluded as lacking objective measures on hearing or vestibular function. Figure 1 presents the PRISMA flow diagram, while Tables 1-3 summarize the general characteristics of the 40 included studies based on the PICO criteria and their assessed risk of bias.
Prisma flow diagram.
Qualitative synthesis
3.2
Hearing function was assessed using pure tone audiometry across all studies, with some research groups complementing it with speech audiometry (Teplitxky et al., 2023), tympanometry (Picciotti et al., 2024), or self-perceived measures such as the Hearing Handicap Inventory for the Elderly (Mohanathas et al., 2024) and the Speech, Spatial and Qualities of Hearing Scale (G et al., 2022; Morris et al., 2023). ARHL was operationalized in two ways: i) Age-normative thresholds benchmarked against age- and sex-specific percentiles, classifying hearing as “worse than expected for age” when ear-specific thresholds exceed the >90th, an approach used in 1/40 studies (Teplitxky et al., 2023); ii) absolute definition according to HL grading, an approach used in 39/40 studies (Zuniga et al., 2012; Viljanen et al., 2009a; Kurtaran et al., 2016; Picciotti et al., 2024; Mohanathas et al., 2024; G et al., 2022; Morris et al., 2023; Azevedo et al., 2022; Nayak et al., 2022; Onn et al., 2021; Basta et al., 2023; Bruce et al., 2019a; Bruce et al., 2019b; Cosetti et al., 2025; Chongvisal et al., 2019; Ciquinato et al., 2020; Gorecka et al., 2021; Kamil et al., 2016; Koh et al., 2015; Kolasa et al., 2023; Kolasa et al., 2024; Lau et al., 2016; Mamo et al., 2023; Mold et al., 2024; Purchase-Helzn et al., 2004; Sakurai et al., 2021; Sakurai et al., 2022; Sakurai et al., 2025a; Sakurai et al., 2025b; Szeto et al., 2021; Viljanen et al., 2009b; Wollesen et al., 2018; Behtani et al., 2024; Rumalla et al., 2015; Campos et al., 2023; Mahmoudi et al., 2019; Soylemez et al., 2024; Negahban et al., 2017; Prasansuk et al., 2004).
Seven studies, as shown in Table 1, explored vestibular dysfunction in individuals with ARHL (Zuniga et al., 2012; Teplitxky et al., 2023; Kurtaran et al., 2016; G et al., 2022; Azevedo et al., 2022; Nayak et al., 2022; Onn et al., 2021; Mold et al., 2024). The majority of these studies - five out of seven - concluded that ARHL was associated with poorer vestibular outcomes (Zuniga et al., 2012; Kurtaran et al., 2016; G et al., 2022; Azevedo et al., 2022; Nayak et al., 2022): two studies reported significant correlations between pure tone average (PTA) and caloric tests (Azevedo et al., 2022) or VEMPS (Viljanen et al., 2009a). Three research groups found significant differences in terms of VEMPS (Kurtaran et al., 2016; G et al., 2022) and vHIT (Onn et al., 2021) when comparing ARHL with age matched subjects with normal hearing. Instead, two studies did not find significant associations between ARHL and caloric responses or vHIT (Teplitxky et al., 2023; Onn et al., 2021).
A total of 22 articles examined the impact of ARHL on static and dynamic gait, as resembled in Table 2. Functional mobility was primarily evaluated through standardized assessments such as the TUG test (Mohanathas et al., 2024; Morris et al., 2023; Cosetti et al., 2025; Koh et al., 2015; Lau et al., 2016; Soylemez et al., 2024) and gait analysis (Basta et al., 2023; Bruce et al., 2019a; Gorecka et al., 2021; Kamil et al., 2016; Kolasa et al., 2023; Lau et al., 2016; Mold et al., 2024; Sakurai et al., 2021; Sakurai et al., 2022; Sakurai et al., 2025a; Szeto et al., 2021; Viljanen et al., 2009b; Wollesen et al., 2018). These evaluations consistently demonstrated that individuals with HL showed slower walking speeds, prolonged transition times and impaired dynamic balance compared to age-matched controls. Complementing these mobility-focused assessments, eight investigations also incorporated dual-task paradigms which explored the additional cognitive load imposed by concurrent auditory processing tasks during ambulation (Morris et al., 2023; Basta et al., 2023; Bruce et al., 2019a; Cosetti et al., 2025; Gorecka et al., 2021; Kolasa et al., 2024; Lau et al., 2016; Wollesen et al., 2018). These studies revealed that ARHL exacerbated cognitive-motor interference, leading to diminished postural control under complex task conditions. To further characterize postural stability, static and dynamic posturography is frequently employed (Marioni et al., 2013). These analyses frequently included measures such as centre of pressure (CoP) displacement and sway area, which consistently revealed greater instability in individuals with ARHL, especially when visual or somatosensory cues were limited (Bruce et al., 2019a; Ciquinato et al., 2020; Kolasa et al., 2024; Viljanen et al., 2009b). In addition to instrumented tests, clinical balance scales were applied to quantify equilibrium and fall risk in everyday contexts such as the Activities-Specific Balance confidence scale (Morris et al., 2023; Bruce et al., 2019a; Cosetti et al., 2025) and the Dynamic Gait Index (Bruce et al., 2019a). Lastly, fall events were captured using the Falls Efficacy Scale International (FES-I) and self-reported fall frequency (Viljanen et al., 2009a; Chongvisal et al., 2019; Kamil et al., 2016; Mamo et al., 2023; Purchase-Helzn et al., 2004; Sakurai et al., 2021; Sakurai et al., 2022; Sakurai et al., 2025a). Excluding Purchase-Helzner (Purchase-Helzn et al., 2004) who reported that the age-adjusted annual fall rate did not differ significantly by hearing category, all the other research groups (Viljanen et al., 2009a; Chongvisal et al., 2019; Kamil et al., 2016; Mamo et al., 2023; Sakurai et al., 2021; Sakurai et al., 2022; Sakurai et al., 2025a) found a correlation between ARHL and risk of falls.
The most frequently investigated intervention for ARHL was HA, as reported by nine studies (Picciotti et al., 2024; Mohanathas et al., 2024; Sakurai et al., 2025b; Behtani et al., 2024; Rumalla et al., 2015; Campos et al., 2023; Mahmoudi et al., 2019; Soylemez et al., 2024; Negahban et al., 2017) (see also Table 3). The majority of the available studies (Picciotti et al., 2024; Sakurai et al., 2025b; Behtani et al., 2024; Rumalla et al., 2015; Campos et al., 2023; Soylemez et al., 2024; Negahban et al., 2017) reported positive effects of HA on postural stability, gait performance, or fall risk reduction, using a variety of outcome measures including instrumented posturography, the TUG, and standardized fall-risk scales. Notably, Rumalla (Rumalla et al., 2015), Negahban (Negahban et al., 2017) and Behtani (Behtani et al., 2024) demonstrated an improved postural control in HA-ON vs. HA-OFF experimental conditions. In contrast, Mohanathas (Mohanathas et al., 2024) failed to observe significant balance improvements in the same experimental setting. Campos (Campos et al., 2023) and Mahmoudi (Mahmoudi et al., 2019) - the latter with over 14,000 participants - reported lower fall risk and delayed fall-related injuries among HA users. Picciotti (Picciotti et al., 2024) and Sakurai (Sakurai et al., 2025b) further indicated longitudinal improvements following 1 year of HA use.
Two studies investigated non–HA interventions aimed at improving balance in older adults with hearing impairment (Bruce et al., 2019a; Prasansuk et al., 2004). Prasansuk (Prasansuk et al., 2004) conducted a clinical trial involving 215 older adults who underwent a 20-week Cawthorne-Cooksey vestibular rehabilitation programme, first reported in the 1940s (Marioni, 2022). The intervention demonstrated high acceptability and was associated with notable improvements in posturographic measures of balance, supporting its utility in managing age-related balance deficits. In a clinical trial of 42 participants, Bruce (Bruce et al., 2019a) evaluated the effects of cognitive and aerobic training, delivered either simultaneously or sequentially. While both intervention paradigms led to improvements in chair rise performance, no significant benefit on standing balance was observed, and the sequential training protocol was slightly more advantageous.
Quantitative analysis
3.3
Six studies (Mohanathas et al., 2024; Morris et al., 2023; Cosetti et al., 2025; Koh et al., 2015; Lau et al., 2016; Soylemez et al., 2024) compared TUG performance in subjects with HL vs. controls without HL. Study-level SMDs ranged from −1.75 to −0.16, with all estimates favouring the control group (i.e., worse performance in HL). The random-effects model yielded a statistically significant average effect size of SMD = −0.679, indicating that individuals with HL exhibited worse dynamic balance than controls (Figure 2). Substantial heterogeneity was observed (Q (5) = 18.15, p = 0.003; I^2^ = 70.8%; Tau^2^ = 0.2771). The 95% prediction interval was −1.83 to 0.47, indicating that, although the mean effect was negative, true effects might vary and could be near zero or positive in some populations. Studentized residuals suggested one potential outlier (Soylemez et al., 2024) exceeding the Bonferroni-adjusted threshold (±2.64), whereas Cook’s distance showed no undue influence. To examine confounding by age, a mixed-effects meta-regression including the mean age difference (HL–control) as a moderator showed a significant association (estimate = −0.0363; Z = −4.07; p < 0.001; 95% confidence interval −0.054 to −0.019; Figure 3). Thus, for each 1-year increase in age imbalance (HL older than controls), the effect became ∼0.036 SMD units more negative, indicating systematic bias due to age differences. Clinically, this corresponded to ∼0.9 s slower TUG per 10-year age imbalance (assuming a representative pooled TUG SD ˜ 2.5 s). After adjusting for age difference, the intercept was not significant (SMD = −0.196, p = 0.294) and residual heterogeneity was eliminated (Tau^2^ = 0; I^2^ = 0%; Q (5) = 1.61, p = 0.808; R^2^ = 100%). No significant evidence of publication bias was detected (Begg–Mazumdar p = 0.71; Egger p = 0.937; Rosenthal’s fail-safe N = 49, p < 0.001). Trim-and-fill did not impute missing studies.
Forest (A) and funnel (B) plots for Timed Up to Go comparing age-related hearing loss (ARHL) vs. normal-hearing controls. Effects are Hedges g (negative = worse/slower in ARHL) pooled with a random-effects model.
Meta-regression of Timed Up and Go effect sizes comparing ARHL vs. normal-hearing controls as a function of between-group age difference. Forest (A) and funnel (B) plots.
Regarding fall risk in HL patients, we pooled k = 4 independent contrasts: three studies reporting 12-month “any fall” (Kamil et al., 2016; Sakurai et al., 2021; Viljanen et al., 2009b); one using a 5-year window (Sakurai et al., 2025a). Older adults with ARHL had 55% higher odds of falling than their normal-hearing counterparts, as shown in Figure 4 (OR = 1.55, 95% confidence interval 1.22–1.89, Z = 9.16, p < 0.001). Between-study heterogeneity was moderate (τ^2^ = 0.0458 [SE 0.0963], τ = 0.214; I^2^ = 39.6%; Q (3) = 5.25, p = 0.154). Small-study effects were not evident (Egger’s p = 0.897; Kendall’s τ p = 0.750), and the Rosenthal fail-safe N was 242, suggesting the result is unlikely to be explained by unpublished null findings.
Forest Plot for fall at 12–60 months comparing ARHL with normal hearing (or, where quartiles were reported, the poorest hearing category vs. the best one).
Three within-participant contrasts comparing static balance with HA ON vs. OFF were synthesized (Behtani et al., 2024; Rumalla et al., 2015; Negahban et al., 2017). Study-level Hedges’ g ranged from 0.21 to 0.90, with all estimates favouring the ON condition (Rumalla (Rumalla et al., 2015) g = 0.895, SE = 0.307; Behtani (Behtani et al., 2024): g = 0.394, SE = 0.185; Negahban (Negahban et al., 2017): g = 0.212, SE = 0.302). The REML indicated a moderate improvement with hearing aids ON (pooled Hedges g = 0.459, SE = 0.140; 95% confidence interval 0.184–0.734; Z = 3.27; p = 0.001; k = 3; Figure 5). Between-study heterogeneity was not detected (Q (2) = 2.81, p = 0.245; I^2^ = 0%; τ^2^ = 0.00 [SE = 0.066]), so the REML summary coincided with the fixed-effect estimate. Given k = 3, small-study bias tests were treated cautiously and were not informative (Egger p = 0.743; Kendall’s tau p = 1.000; Rosenthal fail-safe N = 10). A two one-sided tests (TOST) procedure with pre-specified bounds of ±0.50 SMD was non-significant (Z = −0.290, p = 0.386), indicating that equivalence to ≤|0.50| SMD could not be concluded; the null-hypothesis test was significant (Z = 3.274, p = 0.001). With so few studies, prediction intervals and funnel/asymmetry diagnostics were not informative; meta-regression on age did not converge and was not interpreted.
Forest plot of posturography outcomes in ARHL comparing Hearing Aid (HA) ON vs. OFF (within-participant). Effects are Hedges g (positive = better with HA ON) pooled with a random-effects model; stance pre-specified as eyes-closed on foam (or closest analogue).
Discussion
4
The WHO defines active aging as ‘the process of optimizing opportunities for health, participation, and security to enhance the quality of life as people age, allowing individuals to realize their potential for physical, social, and mental wellbeing throughout the life course’ (de Lima et al., 2024). Reduced mobility may lead to limitations in spatial awareness, depression and social isolation. ARHL, beside accelerating cognitive decline, appears to affect balance and ultimately fall risk, thus reducing the chances of retaining an active aging (Cosetti et al., 2025; Ivanenko and Gurfinkel, 2018; Rafoul et al., 2025; Wunderlich et al., 2024; Berge et al., 2019; Agmon et al., 2017; Foster et al., 2022; Ferrucci et al., 2012).
The available evidence that patho-physiologically and clinically correlates of such associations is discussed in detail below.
ARHL effects on vestibular system
4.1
A meta-analysis for ARHL and vestibular outcomes was not feasible due to substantial methodological heterogeneity (6, 8, 10, 19, 21- 23; see Table 1), therefore a narrative synthesis has been provided. Available studies examined the association between HL and vestibular subsites degeneration. HL on high frequencies seemed to be significantly related to saccular dysfunction (Agrawal et al., 2009). As previously reported, cochlea and saccule embryologically develop in the membranous labyrinth from the same origin and the inferior vestibular nerve innervates this anatomical area: a similar pattern of degeneration in cells of spiral and vestibular ganglions has also been found (Gluth and Nelson, 2017).
In clinical practice, lots of patients with different types of presbycusis suffer from vestibular dysfunction. However, it is unclear whether there is an actual causative association, or just a coexistence of age-related changes in the central nervous system, leading to an impairment of both systems. In the Kurtaran et al. (Kurtaran et al., 2016) population, HL was associated with reduction of amplitudes and prolonged P1 and N1 latency periods in VEMPs, thus suggesting a possible correlation between ARHL and peripheral vestibular deficit (Kurtaran et al., 2016). This supported the hypothesis that vestibular weakness can accompany HL, even without predisposing factors for vestibular diseases (Kurtaran et al., 2016). On the contrary, Onn et al. (Onn et al., 2021) and Teplitxky et al. (Teplitxky et al., 2023) did not find a significant association between vestibular dysfunction and presbycusis. Thus, we highlight the need for further research with standardized protocols to shed light on the interplay between ARHL and age-related vestibular loss (Paplou et al., 2023).
ARHL effects on gait and falls
4.2
ARHL has been increasingly recognized as a factor that might negatively influence gait and balance in older adults. Hearing contributes to spatial orientation and environmental awareness, both of which are essential for static and adaptive gait (Lin and Ferrucci, 2012).
In the meta-analysis of six studies, ARHL appeared associated with poorer TUG performance (see Figure 2) but meta-regression indicated that age imbalance fully explained this pattern (Figure 3), leaving no residual association. Moreover, according to Figure 4, a robust, clinically relevant association between ARHL and incident falls was found. It should be noted that our retrieved OR of 1.55 corresponds to RR ≈ 1.35 when the baseline 1-year fall risk is 27.6% (community-dwelling older adults) and RR ≈ 1.25 when the baseline risk is 43% (higher-risk cohorts), still consistent with a meaningful contribution of hearing status to fall propensity (Mahmoudzadeh Khalili et al., 2024; World Health Organization, 2007). Overall, the included studies have shown that subjects with ARHL had slower walking speeds, shorter stride lengths, and increased gait variability, in comparison to age-matched controls (Sakurai et al., 2021; Viljanen et al., 2009b; Li et al., 2013); these conditions were all associated with a higher risk of falls (Viljanen et al., 2009a; Chongvisal et al., 2019; Kamil et al., 2016; Mamo et al., 2023; Sakurai et al., 2021; Sakurai et al., 2022; Sakurai et al., 2025a; Lin and Ferrucci, 2012). In 2009, a prospective cohort-study firstly explored the relationship between hearing acuity and walking difficulties in older women, by measuring walking speed, walking endurance and self-report difficulties over a 2-km distance (Viljanen et al., 2009b). Poorer hearing levels were significantly associated with reduced balance and higher risk of falls, which could have a direct effect on mobility decline and hence on quality of life of aging people (Viljanen et al., 2009b). Other studies strengthen the association between HL and gait impairment by gait speed analysis (Kolasa et al., 2024; Sakurai et al., 2021; Sakurai et al., 2022; Sakurai et al., 2025a; Wollesen et al., 2018). Sakurai et al. (Sakurai et al., 2021) explored the relationship between ARHL and gait variability: poorer hearing acuity was significantly associated with slower gait speed and increased stride length variability, whereas stride time variability was not significantly affected. Among subjects with HL, those reporting multiple falls had higher stride length variability, but not necessarily slower gait or changes in stride time variability compared to non-fallers. These findings suggested that auditory deficits might compromise spatial consistency in gait (i.e., stride length), increasing the risk of falls, even in the absence of marked reductions in temporal gait variability (i.e., stride time) (Sakurai et al., 2021). Moreover, Sakurai (Sakurai et al., 2022) reported how ARHL and gait performance interacted to affect both global cognition and the risk of fall among the older persons. Slow gait in combination with moderate HL exhibited significantly lower cognitive assessment scores (Montreal Cognitive Assessment-MoCA test) and higher incidence of falls (Sakurai et al., 2022). Conversely, older adults with moderate HL but preserved gait speed did not show these deficits (Sakurai et al., 2022). In addition, the simultaneous presence of ARHL and slow gait markedly increased the risk of single and recurrent falls as well as fall-induced fractures and minor injuries, compared to when these risk factors were present separately (Sakurai et al., 2025a).
Additionally, the TUG test (Podsiadlo and Richardson, 1991) was used to evaluate dynamic balance abilities in older adults. Koh et al. (Koh et al., 2015) observed that the TUG time increased as age increased, even if the comparison of the results between the normal hearing and HL groups revealed there was no significant difference in the TUG times. However, in daily life, balance and walking function mostly occur in the form of multi-tasking phenomena, thus the TUG itself can be misleading in assessing effective functional mobility. Cosetti et al. (Cosetti et al., 2025) applied a dual-task paradigm to the instrumented TUG (iTUG) test, to investigate differences in dynamic balance between older adults with bilateral HL and age-matched normal hearing controls. The total duration of iTUG test did not differ significantly between the two groups, whereas the sub-component analysis of the test did. ARHL subjects showed prolonged sit-to-stand and stand-to-sit times in comparison to the normal hearing cohort (Cosetti et al., 2025). These findings suggested that, while overall mobility might appear comparable, there could be differences in anticipatory balance control in older adults with HL, who also showed specific impairment at the conclusion phase of the task, particularly under cognitive load (dual task). This might reflect a reduced attentional capacity, where added cognitive demand due to the HL disproportionately affected components of gait, potentially impacting on the risk of falling (Cosetti et al., 2025). Furthermore, in the dual-task TUG test combined with cognitive forward and backward digit span tasks, Söylemez et al. (Soylemez et al., 2024) found that HL severity was significantly associated with reduced working memory, and the performance was impaired in presbycusis cases compared to younger controls. Notably, when presbycusis subjects were divided into HA-users and non-users, the former performed significantly better on the cognitive components of the dual-task tests than the latter, suggesting that amplification may reduce listening-related cognitive load and help to preserve cognitive-motor integration during gait.
The Oklahoma Longitudinal Assessment of the Health Outcomes of Mature Adults (OKLAHOMA) prospective studies cohort (Mold et al., 2024) highlighted that participants with moderate or severe ARHL and those with peripheral neuropathy (PN) showed significantly poorer balance and increased gait time, indicating impaired locomotor performance among affected older patients. ARHL and PN independently predict earlier mortality, but their combination reduces survival time more than either sensory deficit alone. This additive effect of ARHL and PN can be mediated in part through impaired balance and gait and underscores the importance of evaluating both sensory systems in older persons people, in order to promptly identify the conditions and pursue prevention and treatment strategies that may help improve longevity in this population (Mold et al., 2024).
Kolasa et al. (2024) examined if HL was independently associated with physical performance, postural sway and gait variability. By using the Short Physical Performance Battery (SPPB) – that evaluates lower-body strength, balance and gait speed–the force platform and the accelerometer, Kolasa et al. (2024) provided a comprehensive and multidimensional assessment of physical function which is essential for everyday activities. They confirmed the previously reported (Kolasa et al., 2023) significant negative association between HL and SPPB total score, suggesting that people with HL had a worse physical performance and could face an increased risk of falls (Kolasa et al., 2023; Kolasa et al., 2024). A significant association between HL and increased postural sway on a firm surface with open and closed eyes, as well as on a foam surface with eyes closed, was found (Kolasa et al., 2024), in line with what has already been reported by other studies (Berge et al., 2019; Agmon et al., 2017). The Kolasa et al. (2024) study also showed that patients with HL had a greater gait variability during dual-task walking across all directions in comparison to individuals with normal hearing, supporting the Sakurai et al. (2021) findings.
Evaluating the effects of HL on dual-task performance while walking, Lau et al. (2016), found that older adults with bilateral HL showed more overall stride time variability than the normal-hearing group. Again, these findings suggested that ARHL might compromise standing balance and walking performance, particularly under cognitively demanding conditions like daily activities, and might serve as an early marker for mobility decline and fall risk in the aging population. The association between ARHL and risk of falls was also assessed and confirmed by other studies (Viljanen et al., 2009a; Chongvisal et al., 2019; Kamil et al., 2016; Mamo et al., 2023; Sakurai et al., 2021; Sakurai et al., 2022; Sakurai et al., 2025a) using appropriate clinical scales, such as the Activities-Specific Balance confidence scale (Morris et al., 2023; Bruce et al., 2019a; Cosetti et al., 2025), the Dynamic Gait Index (Bruce et al., 2019a), the Falls Efficacy Scale International (FES-I), and a self-reported fall frequency (Viljanen et al., 2009a; Chongvisal et al., 2019; Kamil et al., 2016; Mamo et al., 2023; Sakurai et al., 2021; Sakurai et al., 2022; Sakurai et al., 2025a). On the contrary, Purchase-Helzner (Purchase-Helzn et al., 2004) found that neither the age-adjusted annual fall rate nor the risk of incident fracture differed significantly by hearing category.
As already mentioned, besides the improvement of postural stability by a fixed sound source, Basta et al. (2023) observed that continuous auditory information at low or moderate intensities seemed to be significantly helpful in maintaining postural control during easy and challenging walking. This could further promote the importance of auditory rehabilitation in people with ARHL for improving static and dynamic gait control, as discussed in the subsequent section.
Effects of hearing rehabilitation on vestibular system and gait
4.3
Available results supported the hypothesis that HA could positively influence balance and postural control, as shown in Table 2. In line with the well-known effective role of auditory input on dynamic balance and gait, the studies showed that HA-users exhibited better dual-task walking performance and visual working memory, thus indicating the auditory rehabilitation’s protective effect against falls in cognitively demanding situations (Soylemez et al., 2024).
As a matter of fact, Picciotti et al. (2024) found that, after 12 months of HA fitting, patients with presbycusis and presby-vestibulopathy improved in their balance scales and dizziness-related handicap scores, reducing their fall risk. Similar results were later reproduced by Sakurai et al. (2025b). Moreover, a dose-response relationship between HA use and fall prevention was suggested by Campos et al. (2023), who detected significantly lower odds of falling in consistent HA-users. Overall, the current evidence suggests that HA provides measurable benefits in postural control by restoring auditory spatial cues, improving sensory integration, and facilitating vestibular compensation. Nonetheless, the heterogeneity across investigations (Table 3) reflects the different study design and patient-level moderators: balance gains from HA are related to HL severity, coexisting vestibular dysfunction, and device use/adherence. Nevertheless, the overall evidence supports incorporating auditory assessment and rehabilitation within multifactorial fall-prevention programmes for older adults. Accordingly, our meta-analysis indicated small-to-moderate, consistent improvements in posturography with HA ON vs. OFF, particularly when visual and somatosensory cues were impoverished, supporting a role for auditory input in sensory reweighting (See Figure 5).
Concerning cochlear implantation, we found no specific study addressing its impact on posture, gait and risk of falls. Nayak et al. (Nayak et al., 2022) performed CI ipsilateral to the reduced vestibular response in 67.4% of cases and contralateral in 32.6%, with no significant difference observed in postoperative dizziness rates between these groups, highlighting that vestibular dysfunction was more strongly associated with abnormal preoperative videonystagmography results or existing vestibular conditions. Although it is plausible that CI, as well as HA, may have a positive effect on posture, gait and risk of falls protection, this hypothesis needs to be confirmed in future research. In CI candidates, a thorough preoperative vestibular assessment and individualized risk evaluation remain essential in order to optimize hearing rehabilitation outcomes while safeguarding vestibular health.
Regarding non-auditory rehabilitation interventions, Bruce et al. (2019b) and Prasansuk et al. (2004) showed how training specificity shapes balanced outcomes in ARHL. In Bruce’s clinical trial (Bruce et al., 2019a), combined cognitive plus aerobic training sequentially improved chair-rise performance but did not enhance standing balance on posturography. By contrast, Prasansuk’s clinical trial applied a 20-week Cawthorne–Cooksey vestibular programme and demonstrated posturographic balance gains with high acceptability (Prasansuk et al., 2004). Consequently, when the clinical target is postural stability and fall risk, interventions should prioritize task-specific vestibular and sensory-integration training, with general aerobic/cognitive conditioning used as an adjunct rather than a substitute.
Strengths, limits, and future directions
4.4
The main limitation of this systematic review and meta-analysis may reside in the heterogeneity of study designs, measures and evaluation methods across the included articles.
Instead, the primary strength lies in the article selection process, with circumscribed inclusion/exclusion criteria, allowing for the inclusion of original articles with an overall low-to-moderate risk of bias (see also Tables 1-3). Moreover, beside a comprehensive qualitative evaluation of the state of knowledge on the relationship between ARHL and vestibular impairment, a quantitative meta-analysis regarding TUG performance between individuals with ARHL and controls was performed (also formally investigating the possible confounding effects) as well as a meta-analysis of fall risk in ARHL vs. age-matched NH. In addition, the within-participant analysis allowed us to quantitatively explore the effect of HA in terms of posturography outcomes. Further studies are mandatory to elucidate in detail the possible clinical implications of further acoustic rehabilitation strategies (e.g., incorporating auditory cues in rehabilitation or training programmes) on gait in older persons, to possibly enhance postural stability and reduce fall risk.
Conclusion
5
In this systematic review, a qualitative synthesis showed frequent associations between ARHL and vestibular dysfunction. In quantitative analysis, ARHL was linked to impaired balance and mobility, but that part of the observed deficit reflected residual confounding by age. A greater gait variability in dual-task conditions and heightened fall risk among the ARHL population was also reported. Moreover, HA intervention may lead to better static posturography measures. Taken together, these findings suggested that while chronological age remained a powerful driver of mobility outcomes, ARHL contributed additional, modifiable risk through sensory and cognitive-motor pathways, and that rehabilitation may offer clinically meaningful gains in postural control within multimodal fall-prevention strategies.
The importance of balance in impacting the quality of life of individuals with HL should not be underestimated, as balance is essential for most daily activities. By 2060, nearly a quarter of the U.S. population will be aged over 65 years, emphasizing the growing public health concerns related to falls and associated injuries (Riska et al., 2022). Balance impairments and resulting falls significantly impact morbidity and mortality, increasing hospitalization risk tenfold and accounting for over 50% of accidental deaths among the older persons (Paplou et al., 2023). The economic burden associated with falls due to sensory decline further underscores the importance of early detection and multidisciplinary interventions involving various specialists such as audiologists, ENT, neurologists, cardiologists, geriatricians, including combined audiological and vestibular rehabilitation programmes to enhance functional independence and reduce healthcare costs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agmon M. Lavie L. Doumas M. (2017). The association between hearing loss, postural control, and mobility in older adults: a systematic review. J. Am. Acad. Audiology 28 (6), 575–588. 10.3766/jaaa.16044 28590900 · doi ↗ · pubmed ↗
- 2Agrawal Y. Carey J. P. Della Santina C. C. Schubert M. C. Minor L. B. (2009). Disorders of balance and vestibular function in US adults: data from the national Health and Nutrition Examination Survey, 2001-2004. Arch. Intern Med. 169 (10), 938–944. 10.1001/archinternmed.2009.66 19468085 · doi ↗ · pubmed ↗
- 3Azevedo C. Vilarinho S. Sousa Menezes A. Milhazes Mar F. Dias L. (2022). Vestibular and cochlear dysfunction in aging: two sides of the same coin? World J. Otorhinolaryngol. Head. Neck Surg. 8 (4), 308–314. 10.1002/wjo 2.59 36474668 PMC 9714048 · doi ↗ · pubmed ↗
- 4Basta D. Borsellino L. Anton K. Ernst A. (2023). Influence of auditory information on postural control during different gait tasks in the elderly. J. Int. Adv. Otol. 19, 22–27. 10.5152/iao.2023.22671 36718032 PMC 9984904 · doi ↗ · pubmed ↗
- 5Behtani L. Paromov D. Moïn-Darbari K. Houde M. S. Bacon B. A. Maheu M. (2024). Hearing aid amplification improves postural control for older adults with hearing loss when other sensory cues are impoverished. Trends hear. 28, 23312165241232219. 10.1177/23312165241232219 38356376 PMC 10868491 · doi ↗ · pubmed ↗
- 6Berge J. E. Nordahl S. H. G. Aarstad H. J. Goplen F. K. (2019). Hearing as an independent predictor of postural balance in patients evaluated for dizziness. Otolaryngol. Head. Neck Surg. 161 (3), 478–484. 10.1177/0194599819844961 31013210 · doi ↗ · pubmed ↗
- 7Brown C. Tollefson N. Dunn W. Cromwell R. Filion D. (2001). The adult sensory profile: measuring patterns of sensory processing. Am. J. Occup. Ther. 55 (1), 75–82. 10.5014/ajot.55.1.75 11216370 · doi ↗ · pubmed ↗
- 8Bruce H. Lai L. Bherer L. Lussier M. St-Onge N. Li K. Z. H. (2019 a). The effect of simultaneously and sequentially delivered cognitive and aerobic training on mobility among older adults with hearing loss. Gait Posture 67, 262–268. 10.1016/j.gaitpost.2018.10.020 30390596 · doi ↗ · pubmed ↗