Tianqi Jiangtang Capsule in the treatment of patients with diabetes: a systematic review and meta-analysis
Yanjiao Liu, Yifan Chen, Liuding Wang, Zhonghui Jiang, Zhuye Gao

TL;DR
Tianqi Jiangtang Capsule improves blood sugar control in diabetes patients and may offer additional health benefits, but more research is needed to confirm its safety and effectiveness.
Contribution
This study provides a systematic review and meta-analysis of TJC's glucose-lowering efficacy and multi-system benefits in diabetes.
Findings
TJC significantly reduced glycated hemoglobin, fasting blood glucose, and postprandial blood glucose levels.
TJC showed beneficial effects on lipid profiles, inflammatory markers, and renal function.
No significant difference in adverse events was observed between TJC and control groups.
Abstract
Tianqi Jiangtang Capsule (TJC) is a commercial Chinese polyherbal preparation (CCPP) commonly used as adjunctive therapy for glucose management in diabetes. While its potential multi-system effects have been observed, a systematic evaluation focusing on glycemic control remains limited. This study aims to primarily assess the glucose-lowering efficacy of TJC in diabetic patients. We conducted a comprehensive search for relevant randomized controlled trials (RCTs) across nine electronic databases from their inception to 1 September 2025. Two independent reviewers performed trial selection, data extraction, and risk-of-bias assessment. Meta-analyses of efficacy and safety outcomes were performed using RevMan 5.3 and Stata 17. Evidence quality was evaluated using GRADE methodology. 13 RCTs involving 1,298 diabetic patients were included. Compared with conventional treatment (CT) alone or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
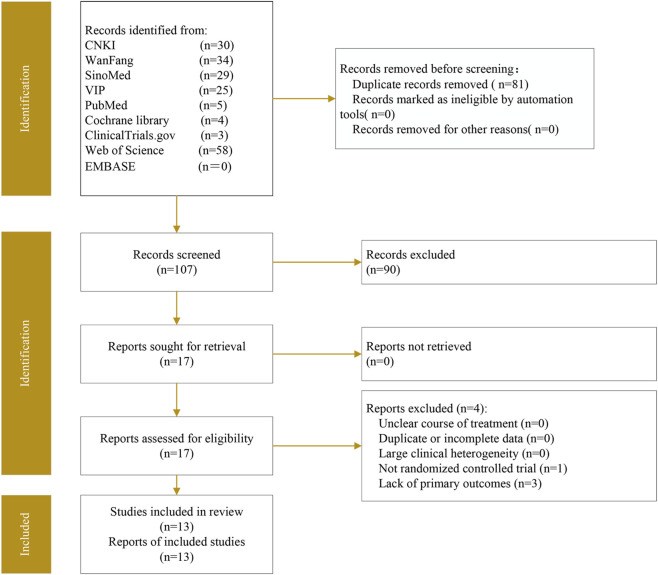 FIGURE 1
FIGURE 1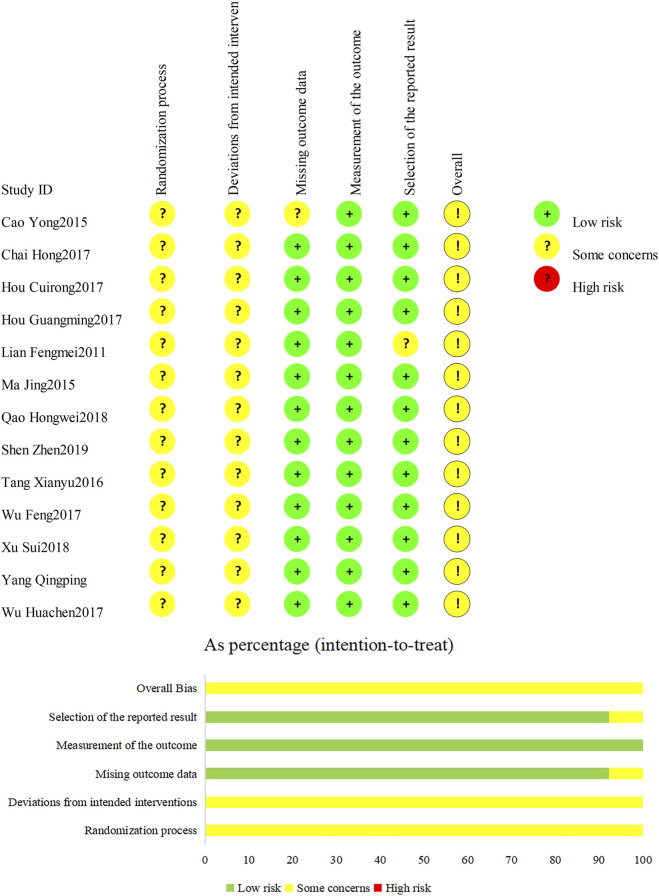 FIGURE 2
FIGURE 2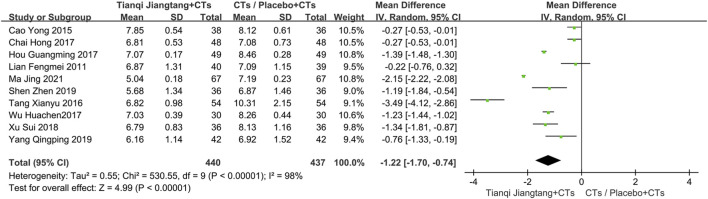 FIGURE 3
FIGURE 3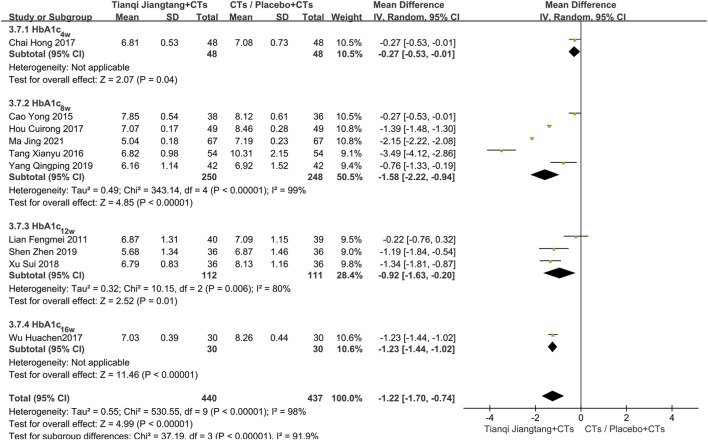 FIGURE 4
FIGURE 4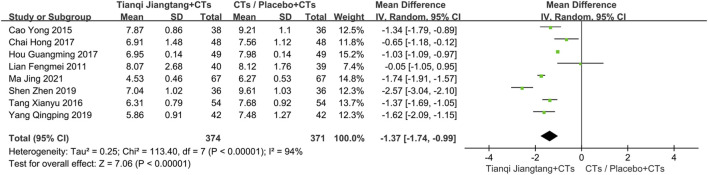 FIGURE 5
FIGURE 5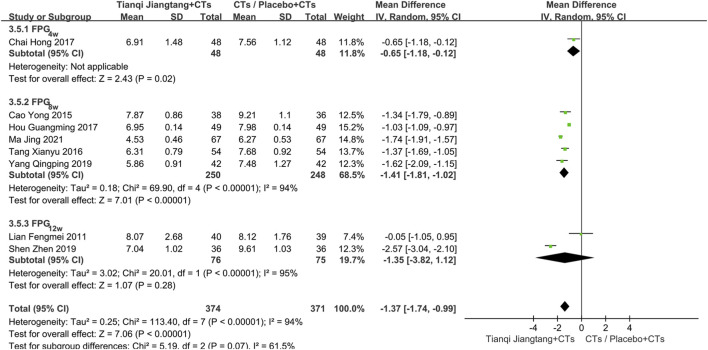 FIGURE 6
FIGURE 6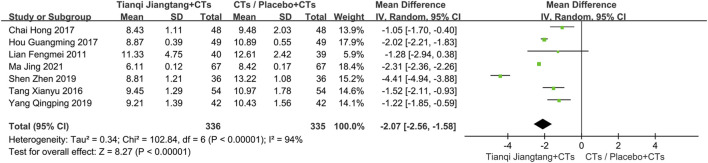 FIGURE 7
FIGURE 7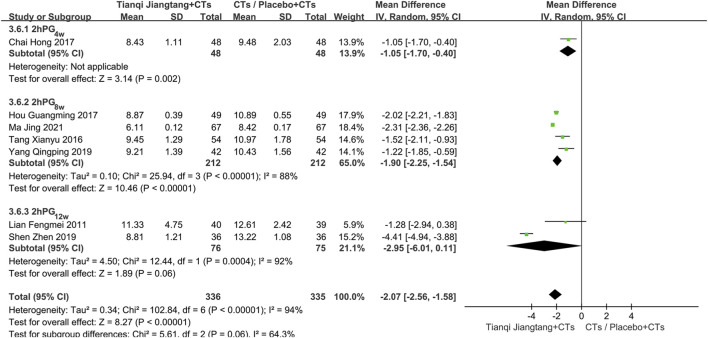 FIGURE 8
FIGURE 8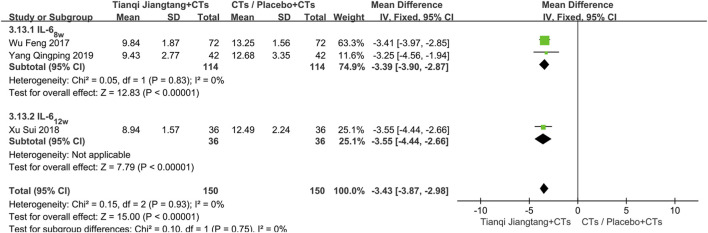 FIGURE 9
FIGURE 9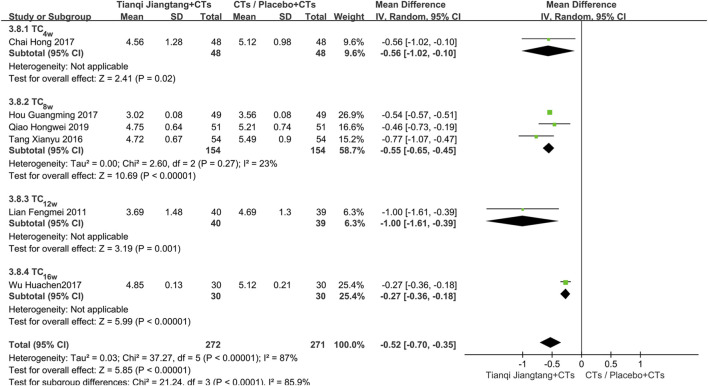 FIGURE 10
FIGURE 10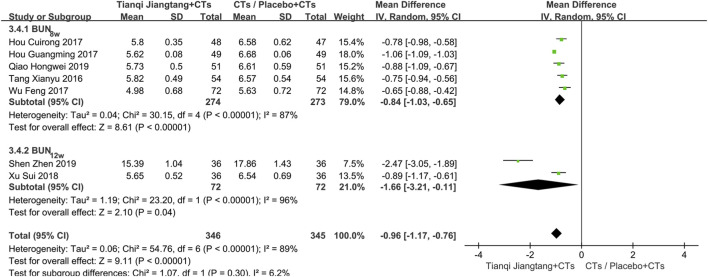 FIGURE 11
FIGURE 11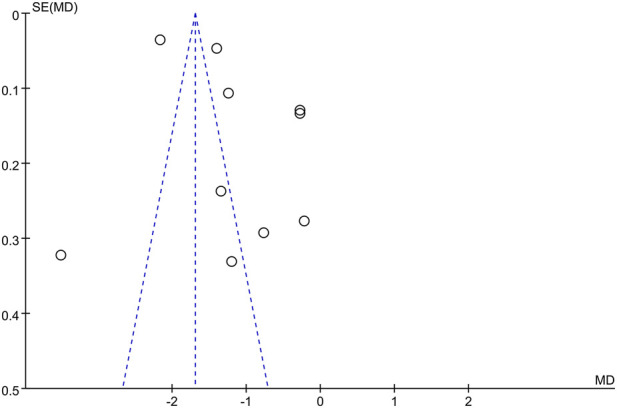 FIGURE 12
FIGURE 12| Study | Publication year | Sample size | Male/Female | Age (year) | Diabetes duration | BMI(kg/m2) | Intervention | Duration | Outcomes | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| E/C | E | C | E | C | E | C | E | C | E | C | ||||
|
| 2021 | 67/67 | 35/32 | 37/30 | 31–67 (54.89 ± 1.76) | 31–66 (54.57 ± 1.49) | 1–11 (7.457 ± 1.36) | 1–11 (7.29 ± 1.18) | −/− | −/− | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 8 weeks | ①②③⑫ |
|
| 2019 | 36/36 | 20/16 | 21/15 | 43–80 (65.11 ± 6.85) | 44–79 (63.45 ± 6.81) | 3–13 (6.76 ± 0.71) | 3–14 (6.73 ± 0.69) | 21–27 (24.55 ± 2.19) | 20–28 (24.34 ± 2.13) | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 12 weeks | ①②③⑩⑪ |
|
| 2019 | 42/42 | 25/17 | 22/20 | 39–70 (53.1 ± 7.0) | 37–69 (52.3 ± 7.5) | 0.75–5 (3.5 ± 1.1) | 0.5–5 (3.2 ± 1.4) | 20.5–30.9 (25.3 ± 1.8) | 20.9–31.6 (25.9 ± 2.3) | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 8 weeks | ①②③⑤⑥⑫ |
|
| 2019 | 51/51 | 27/24 | 28/23 | 62.64 ± 5.82 | 62.98 ± 6.02 | 7.28 ± 2.14 | 7.19 ± 2.24 | −/− | −/− | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 8 weeks | ⑦⑧⑩⑪⑫ |
|
| 2018 | 36/36 | 21/15 | 17/19 | 49–70 (59.1 ± 5.4) | 47–69 (60.2 ± 5.1) | 6–14 (9.2 ± 2.6) | 5–15 (9.5 ± 2.3) | −/− | −/− | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 12 weeks | ①④⑤⑥⑩⑪⑫ |
|
| 2017 | 48/48 | 30/18 | 28/20 | 65.47 ± 4.13 | 66.00 ± 4.25 | 6.59 ± 2.41 | 6.60 ± 2.36 | 24.57 ± 2.64 | 24.82 ± 1.95 | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 4 weeks | ①②③④⑦⑧⑨⑫ |
|
| 2017 | 48/47 | 26/22 | 27/20 | 47–78 (63.12 ± 4.42) | 48–79 (63.45 ± 4.53) | 5–9 (7.11 ± 2.38) | 5–10 (7.26 ± 2.41) | −/− | −/− | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 8 weeks | ⑩⑪ |
|
| 2017 | 49/49 | 25/24 | 26/23 | 49.8 ± 6.9 | 50.2 ± 7.3 | −/− | −/− | −/− | −/− | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 8 weeks | ①②③⑦⑧⑨⑩⑪⑫ |
|
| 2017 | 72/72 | 40/32 | 43/29 | 45–74 (58.4 ± 6.8) | 46–75 (57.7 ± 6.3) | 3–15 (6.8 ± 1.5) | 3–14 (6.2 ± 1.3) | 20–28 (23.9 ± 3.6) | 20–27 (23.6 ± 3.1) | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 8 weeks | ④⑥⑩⑪⑫ |
|
| 2017 | 30/30 | 16/14 | 18/12 | 58.94 ± 5.36 | 58.17 ± 4.89 | 8.44 ± 2.25 | 8.69 ± 2.48 | 22.36 ± 4.65 | 22.36 ± 4.65 | (1)Tianqi Jiangtang capsules 1.6 g three times daily | (1)Placebo | 16 weeks | ①⑦⑧⑨⑩⑪ |
|
| 2016 | 54/54 | 34/20 | 31/23 | 58.34 ± 8.03 | 59.47 ± 7.45 | 11.97 ± 2.60 | 12.58 ± 2.49 | −/− | −/− | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 8 weeks | ①②③⑦⑧⑨⑩⑪⑫ |
|
| 2015 | 40/40 | 19/19 | 19/17 | 33–63 (50.08 ± 7.21) | 34–62 (49.69 ± 7.12) | 1–7 (4.08 ± 1.58) | 1–7 (4.14 ± 1.55) | 24.08 ± 2.87 | 23.83 ± 2.87 | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)CTs | 8 weeks | ①③④⑤⑥ |
|
| 2011 | 40/39 | −/− | −/− | −/− | −/− | −/− | −/− | −/− | −/− | (1)Tianqi Jiangtang capsules 1.6 g three times daily. | (1)Placebo | 12 weeks | ①②③⑦⑧⑨ |
| Outcomes | Number of included studies | Heterogeneity test | Effect model | Results | |||
|---|---|---|---|---|---|---|---|
|
|
|
| (95% |
| |||
| Primary outcomes | |||||||
| HbA1c | 10 | 98 | P < 0.00001 | Random-effect model | −1.22 | −1.70–0.74 | P < 0.00001 |
| FPG | 8 | 94 | P < 0.00001 | Random-effect model | −1.37 | −1.74–0.99 | P < 0.00001 |
| 2hPG | 8 | 94 | P < 0.00001 | Random-effect model | −2.07 | −2.56–1.58 | P < 0.00001 |
| Secondary outcomes | |||||||
| hs-CRP | 3 | 96 | P < 0.00001 | Random-effect model | −2.51 | −3.71–1.30 | P < 0.0001 |
| IL-6 | 3 | 0 | P = 0.93 | Fixed-effect model | −3.43 | −3.87–2.98 | P < 0.00001 |
| TNF-α | 4 | 97 | P < 0.00001 | Random-effect model | −7.66 | −11.26–4.06 | P < 0.0001 |
| TC | 6 | 87 | P < 0.00001 | Random-effect model | −0.52 | −0.70–0.35 | P < 0.00001 |
| TG | 6 | 76 | P = 0.001 | Random-effect model | −0.24 | −0.34–0.15 | P < 0.00001 |
| LDL-C | 5 | 94 | P < 0.00001 | Random-effect model | −0.94 | −1.18–0.71 | P < 0.00001 |
| BUN | 7 | 89 | P < 0.00001 | Random-effect model | −0.96 | −1.17–0.76 | P < 0.00001 |
| Scr | 7 | 97 | P < 0.00001 | Random-effect model | −18.53 | −23.78–13.28 | P < 0.00001 |
| Outcomes | No. of participants (studies) | Anticipated absolute effects (95% | Certainty of the evidence | |
|---|---|---|---|---|
| Risk with CG | Risk difference with, E.G., | |||
| HbA1c | 877 (10) | The mean HbA1c ranged from 6.87 to 10.31 | The mean HbA1c in the, E.G., was 1.22 fewer (0.74 fewer to 1.70 fewer) | ⊕〇〇〇 |
| FPG | 745 (8) | The mean FPG ranged from 6.27 to 9.61 | The mean FPG in the, E.G., was 1.37 fewer (0.99 fewer to 1.74 fewer) | ⊕⊕〇〇 |
| 2hPG | 671 (7) | The mean 2hPG ranged from 8.42 to 13.22 | The mean 2hPG in the, E.G., was 2.07 fewer (1.58 fewer to 2.56 fewer) | ⊕⊕〇〇 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBerberine and alkaloids research · Natural Antidiabetic Agents Studies · Traditional Chinese Medicine Analysis
Introduction
1
Diabetes is a chronic disease mainly characterized by elevated blood sugar levels. This condition results from an absolute or relative insufficiency of insulin secretion, or an impaired utilization of insulin (Singh et al., 2025). It is estimated that by 2050, more than 1.31 billion people will have diabetes (GBD, 2023). The long-term management of diabetes continues to pose challenges due to limitations in current drug therapies. Particularly in type 2 diabetes, oral hypoglycemic agents often fail to achieve adequate glycemic control (Best et al., 2012). Moreover, with the exception of SGLT2 inhibitors, most oral hypoglycemic agents demonstrate no definitive benefits for patients’ cardio-renal outcomes. Some may even exacerbate conditions such as heart failure (Endocrinology, 2019). Exogenous insulin therapy remains essential in diabetes management. However, its use is associated with hypoglycemia risks and potential cardiovascular concerns (Peng et al., 2018; Kenny and Abel, 2019). Therefore, there is an urgent need for multifaceted glucose-lowering strategies that extend beyond glycemic control alone.
Traditional Chinese medicine therapy has unique therapeutic effects in preventing and treating diabetes and its complications (Li and Zhao, 2024). Tianqi Jiangtang Capsule (TJC) is a commercial Chinese polyherbal preparation (CCPP) widely used for patients with type 2 diabetes. It is the main intervention drug for the “11 th Five-Year Plan” science and technology project “Research on Traditional Chinese Medicine Treatment of Prediabetes Type 2”(He et al., 2018). Numerous studies have shown that TJC not only delays the progression of prediabetes, but also exerts a significant therapeutic effect in patients with diabetes, diabetes-related cerebrovascular disease and diabetic nephropathy (Cao et al., 2015; Chai et al., 2017; Hou G., 2017; Sun et al., 2019). However, the current evidence regarding the efficacy of TJC in diabetic patients predominantly relies on earlier clinical studies. They are considerably outdated compared to contemporary therapeutic standards. Our study therefore conducts an updated systematic review of TJC, incorporating recent clinical findings to comprehensively reassess its efficacy and safety profile.
Materials and methods
2
The protocol was registered in PROSPERO (CRD420251137368). Our study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 statement (Page et al., 2021).
Tianqi Jiangtang Capsule (TJC) is a Chinese patent medicine approved by the China National Medical Products Administration (NMPA, 2009). It is composed of ten botanical drugs: Astragalus membranaceus Fisch. ex Bunge [Fabaceae; Astragali Radix], Trichosanthes kirilowii Maxim. [Cucurbitaceae; Trichosanthis Radix], Ligustrum lucidum W.T.Aiton [Oleaceae; Ligustri Lucidi Fructus], Dendrobium nobile Lindl. [Orchidaceae; Dendrobii Caulis], Panax ginseng C.A.Mey. [Araliaceae; Ginseng Radix et Rhizoma], Lycium chinense Mill. [Solanaceae; Lycii Cortex], Coptis chinensis Franch. [Ranunculaceae; Coptidis Rhizoma], Cornus officinalis Siebold & Zucc. [Cornaceae; Corni Fructus], Eclipta prostrata (L.) L. [Asteraceae; Ecliptae Herba], Rhus chinensis Mill. [Anacardiaceae; Galla Chinensis]. All botanical drugs were verified using Plants of the World Online (POWO). We followed the ConPhyMP consensus reporting guidelines (Heinrich et al., 2022) and completed the ConPhyMP preparation as detailed in Supplementary null Appendix 1. A comprehensive summary of the botanical drugs compositions reported in the studies included in our meta-analysis is provided in Supplementary Table S3.
Inclusion and exclusion criteria
2.1
Inclusion and exclusion criteria based on the PICOS framework
2.1.1
Inclusion criteria
2.1.1.1
Population: Patients with a confirmed diagnosis of diabetes mellitus or those meeting the diagnostic criteria outlined in the 2024 American Diabetes Association’s Standards of Care in Diabetes (2024). Intervention: The control group received conventional therapy alone or in combination with a placebo. Conventional therapy may include treatments tailored to the patient’s underlying conditions, such as glucose-lowering or lipid-lowering agents. The observation group received TJCs in addition to the control regimen. Primary outcomes: Glycated hemoglobin (HbA1c), fasting plasma glucose (FPG), and 2 h postprandial glucose (2hPG); Secondary outcomes: High-sensitivity C-reactive protein (hs-CRP), tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), blood urea nitrogen (BUN), and serum creatinine (Scr); Safety outcomes: Adverse reactions (AR). Study Design: Randomized controlled trials (RCTs).
Exclusion criteria
2.1.1.2
Non-randomized controlled trials; Studies for which the full text could not be retrieved; Studies with incomplete, seriously erroneous, or biased data; Duplicated publications.
Search strategy
2.2
We conducted a computerized search of the following databases: China National Knowledge Infrastructure, WanFang, Chinese BioMedical Literature Database, China Science and Technology Journal Database, PubMed, Cochrane Library, ClinicalTrials.gov, Web of Science, and EMBASE. Studies on TJC for the treatment of patients with diabetes were collected. The search period spanned from the establishment of each database to 1 September 2025. Search terms included: “tianqijiangtang capsule”, “tianqijiangtang”, “tianqi jiangtang”, “tianqi”, “tianqi hypoglycemic capsule”, “Diabetes Mellitus”, “Diabetes Insipidus”, “Diabetic Diet”, “Gastroparesis”, “Glucose Intolerance”, “Advanced Glycation End Products”, “Prediabetic State”, and “Scleredema Adultorum” (Supplementary Table S1).
Study selection and data extraction
2.3
Two researchers (Liu Yanjiao and Chen Yifan) independently reviewed the titles and abstracts of each study. They then performed a full-text review of articles that were potentially eligible for inclusion in the meta-analysis. Literature screening and data extraction were conducted according to predefined eligibility criteria, after which the results were cross-verified. Any discrepancies were resolved through discussion or by consultation with a third researcher. Data were extracted using a standardized Excel form (Table 1), including, but not limited to: author(s), publication year, sample size, interventions, outcome measures, and participants’ baseline characteristics.
Risk of bias assessment
2.4
The risk of bias for each outcome was assessed using the Cochrane Risk of Bias tool (ROB2). Based on the descriptions provided in the articles regarding random sequence generation, allocation concealment, blinding, and other criteria, each included study was judged as having either a low, high, or unclear risk of bias.
Data analysis
2.5
Meta-analysis was performed using RevMan software (version 5.3) and Stata 17. For continuous variables measured with the same unit, the mean difference (MD) was used as the effect measure; for those with different units, the standardized mean difference (SMD) was applied. For dichotomous variables, the risk ratio (RR) was selected to summarize the results. All outcomes were expressed as effect estimates with their corresponding 95% confidence intervals (CI).
Heterogeneity among the included studies was assessed using the I ^ 2 ^ statistic. A fixed-effect model was applied when heterogeneity was not significant (I ^ 2 ^ < 50%), whereas a random-effect model was used when substantial heterogeneity was present (I ^ 2 ^ ≥ 50%), and the sources of heterogeneity were further explored. A significance level of α = 0.05 was set for the meta-analysis. We performed subgroup analyses to evaluate the impact of between-study heterogeneity, such as differences in follow-up duration, on the overall results. Additionally, sensitivity analysis was conducted to explore potential sources of statistical heterogeneity and to examine the robustness of the findings. If more than ten studies were included for a given outcome, potential publication bias was assessed by visually inspecting funnel plots and statistically using Begg’s and Egger’s tests.
Certainty assessment
2.6
Two independent reviewers (Liu Yanjiao and Jiang Zhonghui) rated the certainty of the evidence. The assessment used the GRADE framework. It covered risk of bias, imprecision, inconsistency, indirectness, and publication bias.
Results
3
Study selection
3.1
A total of 188 records were identified through database searches (CNKI n = 30, WanFang n = 34, SinoMed n = 29, VIP n = 25, PubMed n = 5, Cochrane Library n = 4, ClinicalTrials.gov n = 3, Web of Science n = 58, EMBASE n = 0) (Figure 1). After 81 duplicates were removed by using EndNote 20, we screened the titles and abstracts, and excluded an additional 90 records that did not meet the eligibility criteria. The remaining 17 records underwent full-text review. Among these, four studies were excluded due to reasons such as non-randomized controlled trials or lack of relevant outcome measures (Supplementary Table S2). Ultimately, 13 articles were included in the quantitative synthesis (Figure 1).
The preferred reporting items for systematic reviews and meta-analyses flow diagram for study selection.
Study characteristics
3.2
A total of 13 randomized controlled trials (Lian et al., 2011; Cao et al., 2015; Tang et al., 2016; Chai et al., 2017; Hou G., 2017; Hou C., 2017; Wu et al., 2017; Wu and Gao, 2017; Xu et al., 2018; Qiao, 2019; Shen, 2019; Yang et al., 2019; Ma et al., 2021) (RCTs) investigating TJC in the treatment of patients with diabetes were included. All studies were published in Chinese between 2011 and 2021, with a total sample size of 1,298 participants—650 in the intervention group and 648 in the control group. The smallest sample size was 60, and the largest was 144 (Table 1).
Methodological quality
3.3
The risk of bias in the included studies was assessed using the Cochrane ROB2 tool (Figure 2). Among the included studies, eight studies described the use of a random number table for allocation, while six only mentioned the term “randomized” without specifying the method. None of the included studies reported blinding or allocation concealment procedures. Lian et al. (2011) reported no pre-specified adverse reactions or adverse events, though all other trials included these outcomes. Two studies documented loss to follow-up and withdrawals. Cao et al. (2015) reported “4 cases lost to follow-up in the control group and 2 cases lost to follow-up in the treatment group”. Lian et al. (2011) noted that “2 participants dropped out, and 77 completed the study” (Figure 2).
Risk of bias graph: judgments about each risk of bias item presented across all included trials.
Primary outcomes
3.4
HbA1c
3.4.1
A total of 10 studies (Lian et al., 2011; Cao et al., 2015; Tang et al., 2016; Chai et al., 2017; Hou C., 2017; Wu and Gao, 2017; Xu et al., 2018; Shen, 2019; Yang et al., 2019; Ma et al., 2021) reported HbA1c levels (Figure 3), with significant heterogeneity observed among them (P < 0.00001, I ^ 2 ^ = 98%). Sensitivity analysis indicated that the results were robust. A random-effects model was therefore applied for meta-analysis, demonstrating significantly lower HbA1c levels in the observation group compared to the control group (MD = −1.22, 95% CI = −1.70 to −0.74, P < 0.00001) (Table 2).
Overall pooled results forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone on HbA1c.
Subgroup analysis based on intervention duration was performed. One study (Chai et al., 2017) with a 4 week intervention showed a significant difference in efficacy between the two groups (MD = −0.27, 95% CI = −0.53 to −0.01, P = 0.04). Five studies (Cao et al., 2015; Tang et al., 2016; Hou C., 2017; Yang et al., 2019; Ma et al., 2021) with an 8 week intervention exhibited significant heterogeneity (P < 0.01, I ^ 2 ^ = 99%). Differences in study populations and intervention methods across these trials were identified as potential sources of heterogeneity. Using a random-effects model, the pooled effect size indicated significantly lower HbA1c levels in the observation group (MD = −1.58, 95% CI = −2.22 to −0.94, P < 0.00001). Three studies (Lian et al., 2011; Xu et al., 2018; Shen, 2019) with a 12 week intervention showed substantial heterogeneity (P < 0.01, I ^ 2 ^ = 80%), and thus a random-effects model was used. The combined results demonstrated a significant difference between the groups (MD = −0.92, 95% CI = −1.63 to −0.20, P = 0.01). Excluding the study by Lian et al. (2011), between-study heterogeneity decreased significantly (P = 0.71, I ^ 2 ^ = 0%). A full-text review revealed that the study by Lian et al. (2011) involved patients with diabetes, while the other two studies focused on patients with diabetic kidney disease, suggesting that differences in study population may account for the heterogeneity. One study (Wu and Gao, 2017) with a 16 week intervention demonstrated a more pronounced reduction in HbA1c levels in the observation group (MD = −1.23, 95% CI = −1.44 to −1.02, P < 0.00001) (Figure 4).
Subgroup analysis forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone on HbA1c.
FPG
3.4.2
A total of eight studies (Lian et al., 2011; Cao et al., 2015; Tang et al., 2016; Chai et al., 2017; Hou C., 2017; Shen, 2019; Yang et al., 2019; Ma et al., 2021) reported FPG levels (Figure 5), with significant heterogeneity among them (P < 0.00001, I ^ 2 ^ = 94%). Sensitivity analysis suggested that the results were robust. A random-effects model was therefore employed for meta-analysis, which indicated that the observation group had significantly lower FPG levels than the control group after treatment (MD = −1.37, 95% CI = −1.74 to −0.99, P < 0.00001) (Table 2).
Overall pooled results forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone on FPG.
Subgroup analysis based on intervention duration was conducted. One study (Chai et al., 2017) with a 4 week intervention period showed a statistically significant difference between the two groups (MD = −0.65, 95% CI = −1.18 to −0.12, P = 0.02). In the five studies (Cao et al., 2015; Tang et al., 2016; Hou C., 2017; Yang et al., 2019; Ma et al., 2021) with an 8 week intervention, significant heterogeneity was observed (P < 0.01, I ^ 2 ^ = 94%). After excluding the study by Hou G. (2017) (Hou C., 2017), the heterogeneity decreased substantially (P = 0.13, I ^ 2 ^ = 48%). A full-text review indicated that the study by Hou G. (2017) involved patients with early-stage diabetes, while the other four studies included patients who met diagnostic criteria for diabetes (with one study specifically focusing on diabetic kidney disease). Differences in study populations were identified as a potential source of heterogeneity. Using a random-effects model, the pooled effect size showed significantly lower FPG levels in the observation group (MD = −1.41, 95% CI = −1.81 to −1.02, P < 0.00001). Two studies (Lian et al., 2011; Shen, 2019) with a 12 week intervention exhibited significant heterogeneity (P < 0.01, I ^ 2 ^ = 95%). A random-effects model was applied, and the meta-analysis results showed no significant difference in efficacy between the two groups (MD = −1.35, 95% CI = −3.82 to 1.12, P = 0.28). After careful review of the full texts, it was found that the included populations differed between the two studies, which may explain the observed heterogeneity (Figure 6).
Subgroup analysis forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone on FPG.
2hPG
3.4.3
Seven studies (Lian et al., 2011; Tang et al., 2016; Chai et al., 2017; Hou C., 2017; Shen, 2019; Yang et al., 2019; Ma et al., 2021) reported 2hPG levels (Figure 7), with significant heterogeneity among the studies (P < 0.00001, I ^ 2 ^ = 94%). A random-effects model was therefore employed for meta-analysis. The results indicated that the observation group had significantly lower 2hPG levels than the control group after treatment (MD = −2.07, 95% CI = −2.56 to −1.58, P < 0.00001) (Table 2).
Overall pooled results forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone on 2hPG.
Subgroup analysis based on intervention duration was conducted. One study (Chai et al., 2017) with a 4 week intervention showed a significant difference between the two groups (MD = −1.05, 95% CI = −1.70 to −0.40, P = 0.002). Among the four studies (Tang et al., 2016; Hou C., 2017; Yang et al., 2019; Ma et al., 2021) with an 8 week intervention, significant heterogeneity was observed (P < 0.01, I ^ 2 ^ = 88%). After reviewing the full texts, variations in study populations and intervention protocols were identified as potential sources of heterogeneity. Using a random-effects model, the pooled effect size demonstrated significantly lower 2hPG levels in the observation group (MD = −1.90, 95% CI = −2.25 to −1.54, P < 0.00001). Two studies (Lian et al., 2011; Shen, 2019) with a 12 week intervention exhibited significant heterogeneity (P < 0.01, I ^ 2 ^ = 92%). A random-effects model was applied, and the meta-analysis results showed no significant difference between the two groups (MD = −2.95, 95% CI = −6.01 to 0.11, P = 0.06). Differences in the enrolled populations were considered a possible source of heterogeneity (Figure 8).
Subgroup analysis forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone on 2hPG.
Secondary outcomes
3.5
hs-CRP
3.5.1
Three studies (Cao et al., 2015; Chai et al., 2017; Wu et al., 2017) used hs-CRP as an outcome measure (Supplementary Figure S1). Sensitivity analysis indicated robust results, while significant heterogeneity was observed among the studies (P < 0.00001, I ^ 2 ^ = 91%). A random-effects model was therefore applied for meta-analysis. The results demonstrated that, compared with conventional therapy alone or combined with placebo, the addition of TJC led to a statistically significant improvement in hs-CRP levels (MD = −2.51, 95% CI = −3.71 to −1.30, P < 0.0001) (Table 2).
Subgroup analysis based on intervention duration showed that one study (Chai et al., 2017) with a 4 week treatment period reported a significant difference between the two groups (MD = −1.15, 95% CI = −1.62 to −0.68, P < 0.00001). Two studies (Cao et al., 2015; Wu et al., 2017) with an 8 week intervention showed low heterogeneity (P = 0.28, I ^ 2 ^ = 13%). The results indicated that the observation group was superior to the control group (MD = −3.08, 95% CI = −3.32 to −2.84, P < 0.00001) (Supplementary Figure S2).
IL-6
3.5.2
Three studies (Wu et al., 2017; Xu et al., 2018; Yang et al., 2019) used IL-6 as an outcome measure (Supplementary Figure S3). Sensitivity analysis indicated robust results, with low heterogeneity observed among the studies (P = 0.93, I ^ 2 ^ = 0%). A fixed-effect model was therefore applied for meta-analysis. The results demonstrated a statistically significant reduction in IL-6 levels in the observation group compared to the control group (MD = −3.43, 95% CI = −3.87 to −2.98, P < 0.00001) (Table 2).
Subgroup analysis was performed based on treatment duration. Two studies had a treatment duration of 8 weeks (Wu et al., 2017; Yang et al., 2019), showing no significant heterogeneity (P = 0.83, I ^ 2 ^ = 0%). The meta-analysis results indicated a statistically significant difference in efficacy between the two groups (MD = −3.55, 95% CI = −4.44 to −2.66, P < 0.00001). One study with a 12 week treatment duration (Xu et al., 2018) also demonstrated a significant difference between groups (MD = −3.08, 95% CI = −3.32 to −2.84, P < 0.00001) (Figure 9).
Subgroup analysis forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone on IL-6.
TNF-α
3.5.3
Four studies (Cao et al., 2015; Wu et al., 2017; Xu et al., 2018; Yang et al., 2019) used TNF-α as an outcome measure (Supplementary Figure S4). Sensitivity analysis indicated robust results, with significant heterogeneity observed among the studies (P < 0.00001, I ^ 2 ^ = 97%). A random-effects model was therefore applied for meta-analysis. The results demonstrated that the addition of Tianqi Jiangtang Granule to conventional therapy led to a statistically significant improvement in TNF-α levels compared to conventional treatment alone or combined with placebo (MD = −7.66, 95% CI = −11.26 to −4.06, P < 0.0001) (Table 2).
Subgroup analysis based on intervention duration showed that three studies (Cao et al., 2015; Wu et al., 2017; Yang et al., 2019) with an 8 week intervention exhibited substantial heterogeneity (P < 0.01, I ^ 2 ^ = 97%). A random-effects model was used, and the results indicated a significant difference between the two groups (MD = −6.33, 95% CI = −9.90 to −2.75, P = 0.0005). After excluding the study by Wu F. (2017) (Wu et al., 2017), heterogeneity decreased significantly (P = 0.36, I ^ 2 ^ = 0%). A full-text review revealed that the study by Wu F. (2017) (Wu et al., 2017) involved patients with early-stage diabetic kidney disease, while the other two studies included general patients with diabetes, suggesting that differences in population characteristics may have contributed to the heterogeneity. One study (Xu et al., 2018) with a 12 week intervention showed superior efficacy in the observation group compared to the control group (MD = −12.11, 95% CI = −15.24 to −8.98, P < 0.00001) (Supplementary Figure S5).
TC
3.5.4
Six studies (Lian et al., 2011; Tang et al., 2016; Chai et al., 2017; Hou C., 2017; Wu and Gao, 2017; Qiao, 2019) used TC as an outcome measure (Supplementary Figure S6). Sensitivity analysis indicated robust results, with significant heterogeneity observed among the studies (P < 0.00001, I ^ 2 ^ = 87%). A random-effects model was therefore employed for meta-analysis. The results demonstrated a statistically significant reduction in TC levels in the observation group compared to the control group (MD = −0.52, 95% CI = −0.70 to −0.35, P < 0.00001) (Table 2).
Subgroup analysis based on intervention duration was performed. One study (Chai et al., 2017) with a 4 week intervention period showed a significant difference between the two groups (MD = −0.56, 95% CI = −1.02 to −0.10, P = 0.02). Three studies (Tang et al., 2016; Hou C., 2017; Qiao, 2019) with an 8 week intervention exhibited low heterogeneity (P = 0.27, I ^ 2 ^ = 23%). The pooled effect size indicated significantly lower TC levels in the observation group (MD = −0.55, 95% CI = −0.65 to −0.45, P < 0.00001). One study (Lian et al., 2011) with a 12 week intervention showed a significant difference between the groups (MD = −1.00, 95% CI = −1.61 to −0.39, P = 0.001). One study (Wu and Gao, 2017) with a 16 week intervention also demonstrated lower TC levels in the observation group (MD = −0.27, 95% CI = −0.36 to −0.18, P < 0.00001) (Figure 10).
Subgroup analysis forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone on TC.
TG
3.5.5
Six studies (Lian et al., 2011; Tang et al., 2016; Chai et al., 2017; Hou C., 2017; Wu and Gao, 2017; Qiao, 2019) reported TG levels as an outcome measure (Supplementary Figure S7). Sensitivity analysis suggested robust findings, with significant heterogeneity detected among the studies (P = 0.001, I ^ 2 ^ = 76%). A random-effects model was therefore used for meta-analysis. The results indicated a statistically significant reduction in TG levels in the observation group compared to the control group (MD = −0.24, 95% CI = −0.34 to −0.15, P < 0.00001) (Table 2).
Subgroup analysis based on intervention duration showed that one study (Chai et al., 2017) with a 4 week intervention period reported significantly lower TG levels in the observation group after treatment (MD = −0.17, 95% CI = −0.29 to −0.05, P = 0.004). Three studies (Tang et al., 2016; Hou C., 2017; Qiao, 2019) with an 8 week intervention showed no significant heterogeneity (P = 0.83, I ^ 2 ^ = 0%). The pooled effect size demonstrated a significant difference between the two groups (MD = −0.32, 95% CI = −0.34 to −0.30, P < 0.00001). One study (Lian et al., 2011) with a 12 week intervention found no significant difference between the observation and control groups (MD = −0.19, 95% CI = −0.53 to 0.15, P = 0.27). Another study (Wu and Gao, 2017) with a 16 week intervention showed lower TG levels in the observation group, with a result approaching statistical significance (MD = −0.11, 95% CI = −0.22 to 0.00, P = 0.05) (Supplementary Figure S8).
LDL-C
3.5.6
Five studies (Lian et al., 2011; Tang et al., 2016; Chai et al., 2017; Hou C., 2017; Wu and Gao, 2017) reported LDL-C levels (Supplementary Figure S9). Significant heterogeneity was observed among these studies (P < 0.00001, I ^ 2 ^ = 94%), and a random-effects model was therefore applied for meta-analysis. The results indicated that the observation group had significantly lower LDL-C levels than the control group after treatment (MD = −0.94, 95% CI = −1.18 to −0.71, P < 0.00001) (Table 2).
Subgroup analysis based on intervention duration showed that one study (Chai et al., 2017) with a 4 week intervention period demonstrated a significant difference between the two groups (MD = −1.09, 95% CI = −1.22 to −0.96, P < 0.00001). Two studies (Tang et al., 2016; Hou C., 2017) with an 8 week intervention exhibited significant heterogeneity (P < 0.01, I ^ 2 ^ = 97%). After comparing the studies, it was noted that one study involved patients with diabetic kidney disease, while the other included individuals with early-stage diabetic kidney disease—suggesting that differences in study populations may explain the heterogeneity. Using a random-effects model, the pooled effect size showed significantly lower LDL-C levels in the observation group (MD = −1.09, 95% CI = −1.78 to −0.41, P = 0.002). One study (Lian et al., 2011) with a 12 week intervention showed a statistically significant difference between the groups (MD = −0.80, 95% CI = −1.26 to −0.34, P < 0.01). Another study (Wu and Gao, 2017) with a 16 week intervention also demonstrated lower LDL-C levels in the observation group (MD = −0.63, 95% CI = −0.76 to −0.50, P < 0.00001) (Supplementary Figure S10).
BUN
3.5.7
Seven studies (Tang et al., 2016; Hou G., 2017; Hou C., 2017; Wu et al., 2017; Xu et al., 2018; Qiao, 2019; Shen, 2019) reported BUN levels (Supplementary Figure S11), with significant heterogeneity among them (P < 0.00001, I ^ 2 ^ = 89%). Sensitivity analysis indicated robust results. A random-effects model was therefore employed for meta-analysis, which showed that the observation group had significantly lower BUN levels than the control group after treatment (MD = −0.96, 95% CI = −1.17 to −0.76, P < 0.00001) (Table 2).
Subgroup analysis based on intervention duration was performed. Among the five studies (Tang et al., 2016; Hou G., 2017; Hou C., 2017; Wu et al., 2017; Qiao, 2019) with an 8 week intervention period, significant heterogeneity was observed (P < 0.01, I ^ 2 ^ = 87%). After excluding the study Hou G. (2017) (Hou C., 2017), heterogeneity decreased markedly (P = 0.54, I ^ 2 ^ = 0%). A detailed review of the full texts suggested that differences in intervention protocols and study populations may have contributed to the heterogeneity. Using a random-effects model, the meta-analysis demonstrated a significant difference between the two groups (MD = −0.84, 95% CI = −1.03 to −0.65, P < 0.00001). Two studies (Xu et al., 2018; Shen, 2019) with a 12 week intervention exhibited significant heterogeneity (P < 0.01, I ^ 2 ^ = 96%). Comparative review revealed that one study enrolled patients with stage II–III diabetic kidney disease, while the other included participants with diabetic kidney disease without stage restrictions. Differences in population characteristics were identified as a potential source of heterogeneity. A random-effects model was applied, and the pooled effect size indicated significantly lower BUN levels in the observation group (MD = −1.66, 95% CI = −3.21 to −0.11, P = 0.04) (Figure 11).
Subgroup analysis forest plot comparing Tianqi Jiangtang Capsule plus conventional treatments (CTs) to placebo plus CTs or CTs alone BUN.
Scr
3.5.8
Seven studies (Tang et al., 2016; Hou G., 2017; Hou C., 2017; Wu et al., 2017; Xu et al., 2018; Qiao, 2019; Shen, 2019) reported Scr levels (Supplementary Figure S12), with significant heterogeneity observed among them (P < 0.00001, I ^ 2 ^ = 97%). Sensitivity analysis indicated that the results were robust. A random-effects model was therefore applied for meta-analysis, which showed significantly lower Scr levels in the observation group compared to the control group after treatment (MD = −18.53, 95% CI = −23.78 to −13.28, P < 0.00001) (Table 2).
Subgroup analysis based on intervention duration revealed that among the five studies (Tang et al., 2016; Hou G., 2017; Hou C., 2017; Wu et al., 2017; Qiao, 2019) with an 8 week intervention, heterogeneity was not significant (P = 0.36, I ^ 2 ^ = 8%). The analysis demonstrated a statistically significant difference between the two groups (MD = −10.39, 95% CI = −10.96 to −9.82, P < 0.00001). Two studies (Xu et al., 2018; Shen, 2019) with a 12 week intervention showed substantial heterogeneity (P < 0.01, I ^ 2 ^ = 99%). A comparative review indicated that differences in the enrolled populations may have contributed to the heterogeneity. Using a random-effects model, the pooled results indicated a non-significant reduction in Scr levels in the observation group (MD = −76.08, 95% CI = −185.01 to 32.85, P = 0.17) (Supplementary Figure S13).
Safety outcomes
3.6
Eight studies (Tang et al., 2016; Chai et al., 2017; Hou C., 2017; Wu et al., 2017; Xu et al., 2018; Qiao, 2019; Yang et al., 2019; Ma et al., 2021) reported on adverse events. Among these, six studies explicitly reported that no adverse drug reactions (ADRs) occurred. The remaining two studies (Xu et al., 2018; Yang et al., 2019) reported specific ADRs. One study (Xu et al., 2018) indicated that during the treatment period, one case of dizziness occurred in the control group, and one case of nausea and one case of gastric discomfort were reported in the treatment group. Another study (Yang et al., 2019) reported one case of hypoglycemia and one case of headache in the control group, and one case of abdominal pain, one case of vomiting, and one case of hypoglycemia in the treatment group. The remaining studies did not report any information regarding the occurrence of adverse drug reactions. Meta-analysis showed no statistically significant difference in the incidence of adverse reactions between the two groups (RR = 1.71, 95% CI = 0.39 to 7.44, P = 0.47). None of the studies reported any occurrence of serious adverse events (Table 2).
Sensitivity analysis
3.7
Sensitivity analysis was performed using the leave-one-out method. The results indicated that the significance of the outcomes remained unchanged regardless of which individual study was omitted. This suggests that the findings of this meta-analysis are robust.
Publication bias
3.8
Since the number of studies was fewer than 10 for all other outcome measures, publication bias was evaluated only for HbA1c using a funnel plot. The results suggested the presence of potential publication bias (Figure 12). Further assessment using Egger’s and Begg’s tests confirmed significant statistical evidence (p < 0.001 and p = 0.002, respectively), suggesting potential small-study effects (Supplementary Figure S14). However, the trim-and-fill method did not detect any missing studies requiring imputation, and the adjusted effect size remained identical to the original estimate (SMD = −2.47, 95% CI: −4.46 to −0.49, Supplementary Figure S15). The adjusted forest plot is presented in Supplementary Figure S16, and the Egger’s regression plot is shown in Supplementary Figure S17.
Funnel plot of HbA1c.
Certainty assessment
3.9
The certainty of the evidence was rated using the GRADE method (Table 3). The overall certainty was low to very low. This was mainly due to a high risk of bias, imprecision and inconsistency.
Discussion
4
Our study primarily evaluated the glucose-lowering efficacy of Tianqi Jiangtang Capsule in diabetic patients. Additionally, we evaluated the capsule’s ability to suppress systemic inflammation, regulate lipid metabolism, and improve renal function.
Our findings demonstrate that TJC significantly reduces HbA1c, FPG, and 2hPG levels in diabetic patients. HbA1c serves as a reliable indicator of long-term glycemic status, being less affected by short-term physiological fluctuations (Wang et al., 2023). The marked reduction in HbA1c indicates TJC’s effectiveness in stabilizing glucose metabolism. Although no statistically significant improvements in FPG and 2hPG were observed in the 12 week subgroup (likely due to substantial heterogeneity and limited sample size), the observed downward trend still supports TJC’s regulatory effect on glucose metabolism. Furthermore, our results show that TJC substantially improves lipid metabolism, inflammatory markers, and renal function. These systemic benefits are interconnected through two key pathophysiological factors: insulin resistance and chronic inflammation.
Proteomic and metabolomic studies suggest that TJC exerts multi-targeted improvement in insulin resistance. In animal models following TJC intervention, alterations in key serum protein levels were observed, manifested as increased apolipoprotein E (ApoE), apolipoprotein A1 (ApoA1), and transthyretin (TTR) alongside decreased haptoglobin (Hp) and serum amyloid P-component (SAP) (Zhang et al., 2010). Additionally, upregulation was noted in insulin-independent pathways including glucose transporter type 4 (GluT-4) and mitogen-activated protein kinase (MAPK) signaling, as well as the lipid metabolism pathway mediated by upregulation of perixisome proliferator-activated receptor alpha (PPAR-α) (Zhang et al., 2009). Human metabolomic studies on adipose tissue indicate that TJC may participate in the restoration of metabolic processes involving phospholipids, glycolipids, nucleosides, and carnitines (Yu et al., 2011). In contrast to Western medications like metformin, which primarily act on Adenosine 5′-monophosphate (AMP)-activated protein kinase (AMPK) and GluT-4 signaling pathways (Herman et al., 2022), TJC exerts multiple therapeutic benefits by targeting a broader range of molecular pathways. These mechanisms collectively enhance glucose uptake and utilization, improve insulin resistance, and regulate lipid profiles.
Another crucial aspect of TJC’s mechanism lies in its impact on chronic inflammation. Previous studies have confirmed that systemic chronic inflammation serves as a key driver in the development and progression of diabetes and its complications. It can not only perpetuate insulin resistance but also directly contribute to end-organ damage (Yaribeygi et al., 2019). Elevated hs-CRP levels are closely associated with an increased risk of T2DM in middle-aged and elderly Chinese populations (Yang et al., 2021). Furthermore, longitudinal changes in hs-CRP show a significant association with all-cause mortality risk (Wang et al., 2024). IL-6 inhibits SLC39A5 expression, leading to hyperglucagonemia-associated hyperglycemia, which is closely linked to the development of diabetic kidney disease and diabetes-related cardiovascular complications (Kreiner et al., 2022; Chen et al., 2023). TNF-α may mediate inflammatory responses by activating transcription factors such as kappa B kinase beta (IKKβ), c-Jun N-terminal kinase (JNK), and nuclear factor kappa-B (NF-κB) (Akash et al., 2018). Its upregulation of TNF-related apoptosis-inducing ligand (TRAIL) and death receptor 5 (DR5) expression exacerbates the progression of diabetic nephropathy (Lv et al., 2025). By concurrently alleviating insulin resistance and inflammatory levels, TJC disrupts this vicious cycle between metabolic dysregulation and tissue injury, suggesting potential ameliorative effects against a spectrum of diabetic complications.
Our study reveals that TJC’s renoprotective effects further corroborate the aforementioned perspective (significant reductions in BUN and Scr levels). Animal experiments demonstrated that diabetic kidney disease (DKD) rats treated with high dose TJC exhibited significant reductions in blood glucose, lipid levels, proteinuria, and the pro-fibrotic factor serum transforming growth factor-β1 (TGF-β1), along with enhanced activities of antioxidant enzymes superoxide dismutase (SOD) and glutathione peroxidase (GSH-Px). Histopathological examination of renal tissue showed a decreased number of sclerotic glomeruli and alleviated edema in renal tubular epithelial cells (Chen et al., 2017). This confirms that TJC ameliorates the progression of diabetic kidney disease through its antioxidant and anti-fibrotic functions. Additional studies have reported that TJC can improve blood viscosity, inhibit platelet aggregation, and enhance cognitive function in elderly diabetic patients with cerebral microangiopathy, as well as improve peripheral vascular elasticity in early-stage diabetes (Cheng and Yin, 2017; Wu and Gao, 2017). These effects may represent downstream manifestations of its synergistic actions on glucose homeostasis, lipid metabolism, and inflammatory pathways.
In summary, the integrated evidence presented in this paper indicates that TJC contributes to the improvement of glucose homeostasis in diabetic patients. Its glucose-lowering effect is not an isolated action, but rather reflects its role as a multi-target therapeutic agent acting on an interconnected network of metabolic, inflammatory, and oxidative stress pathways. Beyond TJC, various other Chinese botanical drugs and proprietary Chinese patent medicines have demonstrated advantages in the long-term management of diabetes. For instance, Shenqi Jiangtang Capsule, which shares similarities with TJC, has been reported to reduce levels of inflammatory markers such as TNF-α, IL-1β, CRP, and IL-6 (Cheng et al., 2025). This effect may be associated with its modulation of pathways such as mitogen-activated protein kinases (MAPK) and AKT serine/threonine kinase (AKT) (Chen et al., 2025). This mechanism partially overlaps with that of TJC. Additionally, other preparations such as Qigui Didang Formula (Wang et al., 2022), Jinqi Jiangtang Capsule (Hao et al., 2025), and Wumei Pill (Huang et al., 2025) have been shown to confer additional benefits beyond glucose-lowering, including suppression of inflammation, improvement of renal function, and regulation of lipid metabolism. A recent systematic review evaluated the efficacy of 23 Chinese botanical drugs for type 2 diabetes. The results demonstrated that the combination of Chinese botanical drugs with conventional Western medications yielded superior therapeutic efficacy in improving insulin resistance and dyslipidemia compared to Western medications alone (Ni et al., 2025). The comprehensive mechanism of action of TJC and similar Chinese medicines effectively compensates for the limitations of conventional diabetes treatments, which include the single-target focus of oral hypoglycemic agents and insulin therapy, the potential risks of target organ damage, and other adverse effects. Therefore, we propose that an integrated therapeutic approach combining Chinese botanical drugs with conventional hypoglycemic agents represents a more holistic strategy for managing type 2 diabetes and mitigating its associated complications.
Due to the limited number of included studies, publication bias was assessed only for the HbA1c outcome. The funnel plot suggested the possible presence of publication bias. Subsequent Egger’s and Begg’s tests yielded statistically significant results. However, the trim-and-fill method did not identify any missing studies requiring imputation, and the adjusted effect size remained unchanged. This phenomenon may be attributed to the substantial heterogeneity among the included studies and their relatively small sample sizes. Although the adjusted results remained statistically significant, there remains a possibility that small-scale studies may overestimate the magnitude of the effect. Thus, the findings warrant further validation through larger-scale, high-quality studies. Sensitivity analysis showed that the significance of the overall results did not change substantially with the omission of any individual study. Therefore, we consider the study findings to be robust. None of the included studies reported the implementation of blinding or allocation concealment, which may introduce potential bias. Although the use of objective outcome measures thus reduces the likelihood of measurement bias, the presence of selection bias and performance bias may still have led to an overestimation of the intervention effects.
No significant adverse reactions were reported in most studies during the treatment period. Mild gastrointestinal symptoms such as nausea, vomiting, and abdominal pain were occasionally observed but did not require special intervention. However, five studies did not report the occurrence of ADRs, and none of the included studies established predefined indicators for AEs. Therefore, the safety profile of TJC requires further confirmation. Future studies should provide more detailed reporting on the side effects, drug interactions, and overall safety profile of TJC.
This study has several limitations. First, all included RCTs were of low to moderate quality, and the lack of large high-quality RCTs may introduce bias. Second, the study populations were exclusively Chinese, limiting generalizability to other ethnicities, climates, and regions. Additionally, most studies did not clearly describe blinding methods, reducing the quality of evidence. Future studies should emphasize allocation concealment and strict double-blind designs to enhance standardization and credibility. The studies included in this systematic review exhibited considerable heterogeneity. We only performed subgroup analyses based on treatment duration. Due to constraints including incomplete baseline data reporting, unclear population classifications, and heterogeneous control medications in the original studies, it was not feasible to form meaningful subgroups for other analyses such as those based on type of control therapy, disease subtype, baseline HbA1c level, duration of diabetes, or study quality. Consequently, the inability to fully account for the sources of heterogeneity represents a limitation of this review. Finally, the short treatment and follow-up durations in the included studies preclude conclusions regarding the long-term effects of TJC. Extended observation periods are recommended in future research.
Conclusion
5
Our meta-analysis mainly evaluated the glucose-lowering efficacy of TJC. We discovered its additional benefits in inhibiting inflammation responses, improving lipid metabolism and protecting renal function. These findings suggest that beyond glycemic control, TJC may possess broader clinical significance by ameliorating inflammatory markers in diabetic patients. This supports its potential application for diabetic complications, such as diabetic kidney disease. However, the safety profile and scope of application of TJC require further investigation to be substantiated.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Akash M. S. H. Rehman K. Liaqat A. (2018). Tumor necrosis factor-alpha: Role in development of insulin resistance and pathogenesis of type 2 diabetes mellitus. J. Cell. Biochem. 119 (1), 105–110. 10.1002/jcb.26174 28569437 · doi ↗ · pubmed ↗
- 2American Diabetes Association Professional Practice Committee (2024). 2. Diagnosis and classification of diabetes: standards of care in Diabetes-2024. Diabetes Care 47 (Suppl. 1), S 20–s 42. 10.2337/dc 24-S 002 38078589 PMC 10725812 · doi ↗ · pubmed ↗
- 3Best J. D. Drury P. L. Davis T. M. Taskinen M. R. Kesäniemi Y. A. Scott R. (2012). Glycemic control over 5 years in 4,900 people with type 2 diabetes: real-world diabetes therapy in a clinical trial cohort. Diabetes Care 35 (5), 1165–1170. 10.2337/dc 11-1307 22432105 PMC 3329812 · doi ↗ · pubmed ↗
- 4Cao Y. Wang H. Xu C. (2015). The effects of Tianqi Jiangtang Capsule combined with metformin on the levels of interleukin-6,tumor necrosis factorαand C-reactive protein in patients with type 2 diabetes mellitus. Chin. J. Diabetes 23 (08), 739–741. 10.3969/j.issn.1006-6187.2015.08.012 · doi ↗
- 5Chai H. Lu Y. Xiao H. Li Y. Cui K. Zhang Y. (2017). Clinical observation of Tianqi Jiangtang Capsules combined with metformin in the treatment of elderly patients with type 2 diabetes mellitus complicated with cerebral microvascular lesions. China Pharm. 28 (15), 2053–2057. 10.6039/j.issn.1001-0408.2017.15.11 · doi ↗
- 6Chen K. Xu S. Chen G. Mao X. Cao M. Huang H. (2017). Effects of Tianqi Jiangtang Capsule on renal function in rats with diabetic kidney disease. Chin. J. Diabetes 9 (11), 714–719. 10.3760/cma.j.issn.1674-5809.2017.11.010 · doi ↗
- 7Chen W. Cui W. Wu J. Zheng W. Sun X. Zhang J. (2023). Blocking IL-6 signaling improves glucose tolerance via SLC 39A 5-mediated suppression of glucagon secretion. Metabolism 146, 155641. 10.1016/j.metabol.2023.155641 37380017 · doi ↗ · pubmed ↗
- 8Chen N. Lei W. Shi Y. He T. Tian N. Yu R. (2025). Mechanism of action of Shenqi Jiangtang capsules in treatment of diabetic nephropathy: a study based on network pharmacology, machine learning, and Mendelian randomization. Hunan J. Traditional Chin. Med. 41 (01), 155–162. 10.16808/j.cnki.issn 1003-7705.2025.01.032 · doi ↗