Comparison of health economics in robot-assisted partial nephrectomy and CT-guided cryoablation for the management of T1 renal cell carcinoma: an analysis of a prospective Danish cohort
Theresa Junker, Mie Gaedt Thorlund, Tommy Kjærgaard Nielsen, Nessn Azawi, Signe Wang Bach, Jonathan Belsey, Jens Borgbjerg, Ole Graumann

TL;DR
A study in Denmark compared the cost-effectiveness of two treatments for early-stage kidney cancer and found that cryoablation is more cost-effective than surgery without affecting patient outcomes.
Contribution
The study provides real-world evidence on the cost-effectiveness of cryoablation versus robot-assisted surgery for T1 renal cell carcinoma using a Markov model and propensity score matching.
Findings
PCA and RAPN showed no significant differences in local recurrence, metastases, or major complications.
PCA had a significantly shorter hospital stay and provided a net monetary benefit of €9,045 at a €40,000/QALY threshold.
QALYs gained were nearly identical for both treatments, indicating similar health outcomes.
Abstract
This study used real-world outcomes data to compare the cost-effectiveness of percutaneous cryoablation (PCA) and robot-assisted partial nephrectomy (RAPN) in patients with T1 renal cell carcinoma (RCC). Prospective data from June 2019 to February 2021 from two Danish University hospitals, following patients with RCC stage T1 treated with either PCA or RAPN, were used to provide procedural and clinical outcome parameters. A Markov model was used to estimate quality-adjusted life years (QALYs) and costs, incorporating health states for stable disease, local recurrence, metastasis, and all-cause mortality. Propensity score matching using specific covariates was carried out to ensure that the two populations evaluated were matched. Analyses were conducted comparing time to local recurrence or metastases, duration of hospital stay, and postoperative complications. Treatment-specific…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
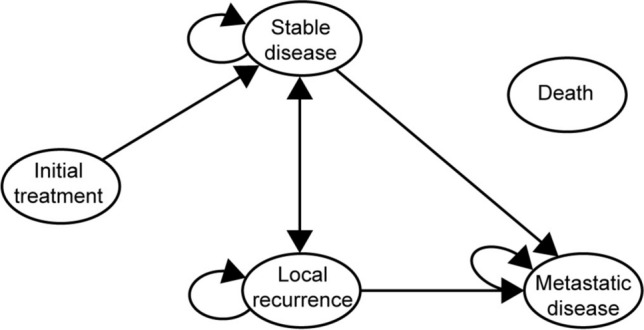 Figure 1
Figure 1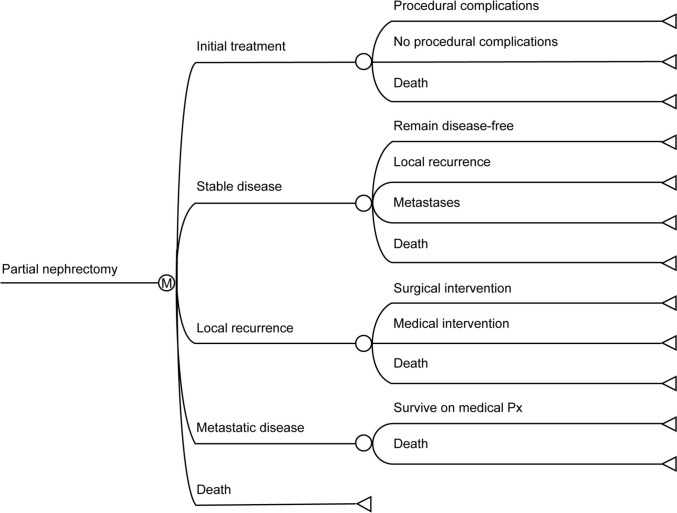 Figure 2
Figure 2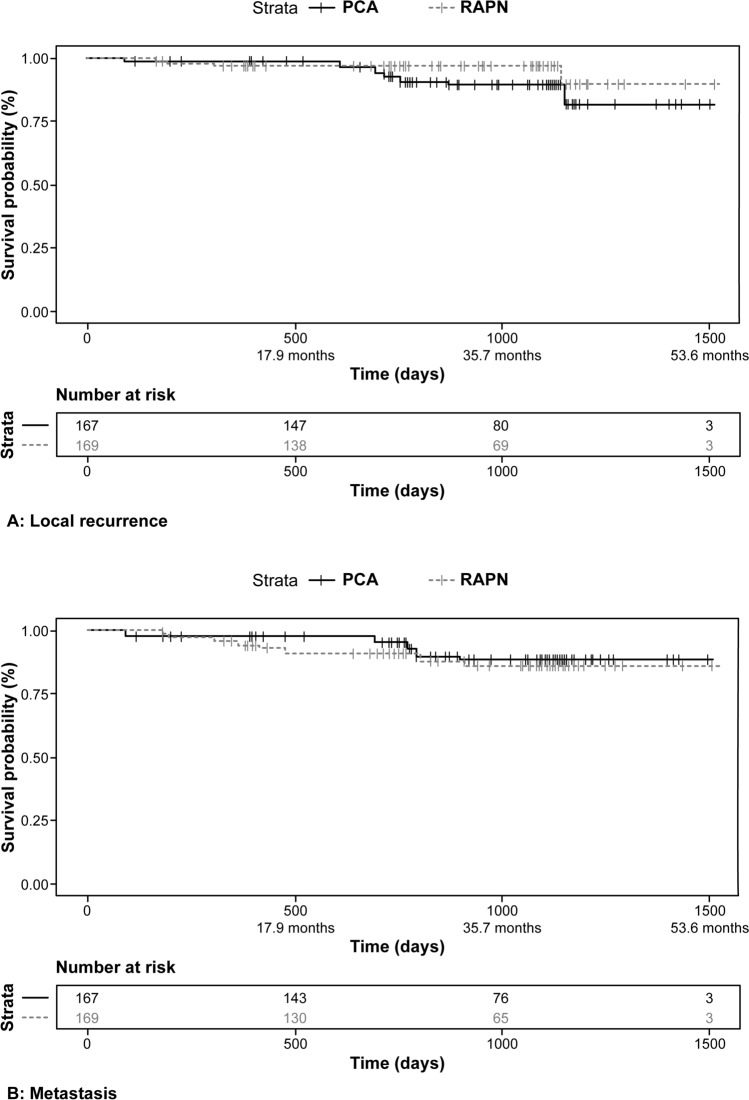 Figure 3
Figure 3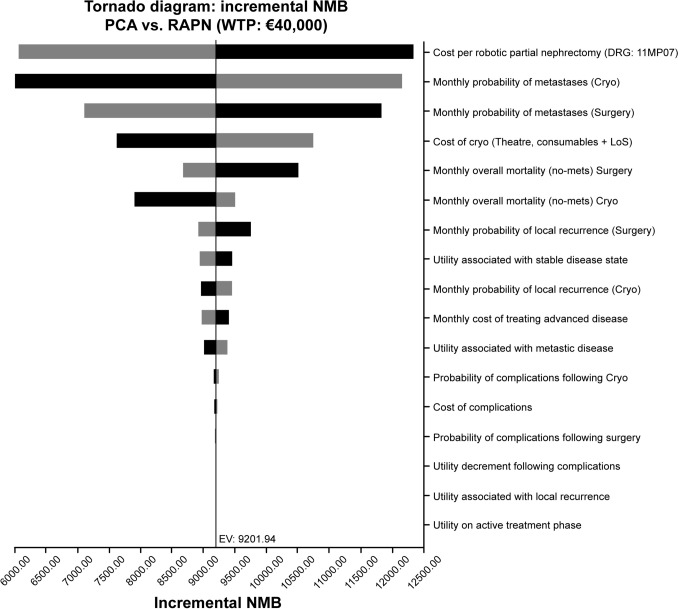 Figure 4
Figure 4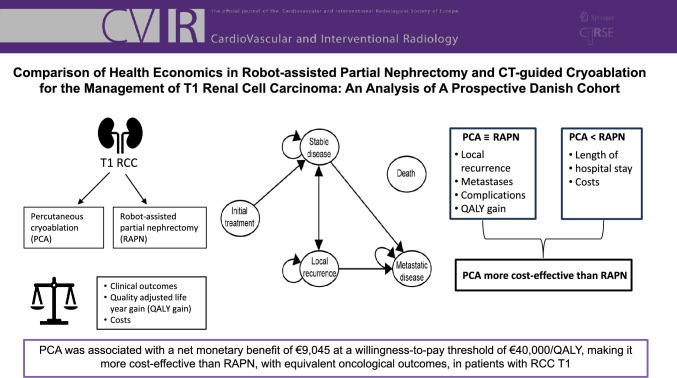 Figure 5
Figure 5- —http://dx.doi.org/10.13039/100008497Boston Scientific Corporation
- —University of Southern Denmark
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal cell carcinoma treatment · Pancreatic and Hepatic Oncology Research · MRI in cancer diagnosis
Introduction
Renal cell carcinoma (RCC) accounts for 90–95% of all renal malignancies. In 2020, there were around 400,000 incident cases and 130,000 deaths globally [1, 2]. A 2019 publication estimated that new cases of RCC in Denmark would rise from 922 in 2020 to 1,017 by 2030 [3]. In 2022–2023, the Danish Renal Cancer database documented 1,091 new cases, suggesting that the rise in incidence has already exceeded the predicted rate for 2030 [4].
A 5-year survival following diagnosis of RCC ranges from 97% for stage I to 27% for stage IV [5]. Effective containment of stage I tumors, around two-thirds of all new cases [5], is a high therapeutic priority. The standard treatment for early-stage localized RCC is robot-assisted partial nephrectomy (RAPN) [6, 7] to maximize the preservation of renal parenchyma without sacrificing cancer control.
Percutaneous cryoablation (PCA) is an alternative method in which cryoprobes are inserted into the tumor under computed tomography (CT) guidance. A double freeze–thaw cycle destroys the tumor cells through intracellular ice formation, osmotic cell membrane rupture, and delayed local vascular injury. This approach is associated with oncological outcomes similar to RAPN’s regarding local recurrence, metastatic disease, and cancer-specific mortality, with a low complication rate [8–10].
Current guidelines from the European Association of Urology and the American Urological Association recommend PCA as an alternative to RAPN in patients with T1a tumors, particularly in those with frailty or comorbidities [6, 7]. This restricted range of indications reflects the relatively limited published evidence base for PCA.
PCA is currently used in a minority of patients with RCC; however, a recent analysis from Germany and the USA shows that its use grew threefold between 2006 and 2019 [11]. Drivers for adopting PCA were improved safety and a shorter procedure time than other focal therapies [12]. While primarily seen in older patients, 15% of PCA patients in the German analysis were under 65, indicating an overlap with the PN target group [11].
One aspect of PCA that merits consideration is the relative cost performance versus RAPN. While long-term costs are likely similar, the costs of the procedure and the postoperative care can vary considerably. However, potentially significant differences between the patient populations undergoing the two treatments could impact the analysis and bias the conclusions. Several recent studies have explored the costs of PCA versus surgical treatment of T1a RCC**,** with mixed results depending on methodology, healthcare setting, and inclusion criteria [12–15]. However, the evidence is sparse, especially prospective data regarding the cost-effectiveness of PCA versus RAPN in a publicly funded healthcare system, including both T1a and T1b tumors with long-term follow-up. Therefore, this study used real-world prospective clinical data from two centers in Denmark to assess the cost-effectiveness of PCA compared to RAPN in patients with stage T1 RCC, using propensity score matching to allow assessment of the impact of the treatment modality independently of patient characteristics.
Methods
The objective was to compare patients with cT1N0M0 RCC undergoing primary treatment, using either RAPN or PCA, as part of a prospective cohort study in two Danish university hospitals. A Markov model was constructed in TreeAge Pro (TreeAge Software, 2024) to estimate medium-term quality-adjusted life years (QALYs) and direct medical costs from the perspective of the Danish healthcare system over a 5-year time horizon. QALYs and costs were discounted at 3% per year. The Danish Data Protection Agency approved the project and was deemed exempt from ethics notification obligations. The study was reported following the CHEERS guidelines [16]
Model Structure
The Markov model consisted of three post-treatment health states (stable disease, local recurrence, and metastatic disease) and a further state capturing death (Figs. 1 and 2).Fig. 1. Health state transition diagramFig. 2Cost-utility model structure (partial nephrectomy shown)
Input Parameters
Table 1 shows the input parameters and sources used. All variables were included in a deterministic sensitivity analysis, with testing being carried out across a range of ± 20% from the central estimate. Table 1. Input parameters used in the modelParameterValueSourceTransition probabilitiesPostoperative complications: RAPN (Clavien grade III +)2.5%Analysis of NEPHSPARE data^^Postoperative complications: PCA (Clavien grade III +)5.5%Analysis of NEPHSPARE data^^Local recurrence0.18% per monthWeighted analysis of NEPHSPARE data^^Same rate applied in both groupsMetastatic recurrence0.35% per monthWeighted analysis of NEPHSPARE data^^Same rate applied in both groupsOverall mortality0.12% per monthWeighted analysis of NEPHSPARE data^^Same rate applied in both groupsMortality in metastatic stateParameterised survival curveHawkins et al. [19] – survival following targeted systemic therapy in metastatic RCCUtilitiesIntervention0.058 in month of procedureWu et al. [13] (assumes local recurrence state for month of treatment)Postoperative complications0.05 in month of procedureWu et al. 2023 [13]Stable disease0.76Wu et al. 2023 [13]Local recurrence0.70Wu et al. 2023 [13]Metastatic recurrence0.66Wu et al. 2023 [13]Health care resource use & costsCost of PCA procedure€7,427Bottom-up costing based on clinician inputCost of RAPN procedure€15,293Health Data Agency DRG Rates 2024: DRG 11MP07Cost of post-op complications€4,332Health Data Agency DRG Rates 2024: DRG 21MA03Cost/month of advanced disease state€2,500Estimated based on published literatureBuja et al.; Ronconi et al.; Cholley et al.; Redig et al. [30–33]^^Data from the NEPHSPARE cohort have previously been published regarding adverse events and health-related quality of life [17, 18]
Clinical Inputs
Procedural and clinical outcomes were derived from the results based on the NEPHSPARE cohort [17, 18]. This prospective cohort of 187 patients with cT1N0M0 RCC underwent primary treatment between June 2019 and February 2021 at two university hospitals in Denmark. All PCA procedures were conducted at one hospital specializing in the technique. Both centers performed RAPN. The present analysis is on a subset of 171 patients from the NEPHSPARE cohort, excluding open partial nephrectomy (PN). The median duration of follow-up was 30 months. Patients were treated with either RAPN (n = 80) or PCA (n = 91), as decided by a multidisciplinary team. PCA patients tended to be older and have smaller tumors, more comorbidities, poorer renal function, and a lower performance status than those treated with RAPN (Table 2). Table 2. Covariate distributions in crude population and propensity-adjusted pseudopopulationCovariateCrude populationIPTW-adjusted populationPCARAPNpPCARAPNpNumber of patients9180167167Age at surgery Mean (sd)67.3 (12.0)62.3 (10.9)0.00165.0 (12.8)65.0 (10.9)0.987SexN Female (%)25 (27%)21 (26%)0.90046 (27%)49 (29%)0.808CCI N (%)01234567897(7.7%)8(8.8%)18(20%)17(19%)16(18%)12(13%)6(6.6%)3(3.3%)3(3.3%)1(1.1%)10(13%)14(18%)25(31%)19(24%)5(6.3%)3(3.8%)3(3.8%)1(1.3%)-- < 0.00114(8%)21(13%)46(28%)33(20%)20(12%)16(10%)8(5%)4(3%)3(2%)1(1%)16(10%)21 (12%)47(28%)35(21%)17(10%)18(11%)5(3%)8(5%)--0.966ASA N (%)0126 (7%)43 (47%)42 (46%)8 (10%)45 (56%)27 (34%)0.20017 (10%)87(52%)63(38%)13(8%)85(51%)69(41%)0.867BMI Mean (sd)29.6 (6.07)28.7 (5.58)0.30030.0 (6.32)28.7 (5.20)0.174eGFR Mean (sd)70.9 (20.2)78.4 (15.3)0.02373.8 (18.9)73.1 (19.1)0.870Tumor size (mm)Mean (sd)31.2 (9.3)37.3 (12.6) < 0.00133.1 (9.4)34.6 (11.5)0.394RENAL scoreN (%)456789101110(11%)5(5.5%)12(13%)15(16%)23(25%)14(15%)12(13%)–8(10%)6(7.5%)13(16%)21(26%)11(14%)15(19%)5(6.3%)1(1.3%)0.30016(10%)9(5%)24(14%)27(16%)39(23%)28(17%)25(15%)–22(13%)14(8%)23(14%)54(32%)21(12%)28(17%)7(4%)1(1%)0.067ECOG Performance status N (%)012354(59%)24(26%)12(13%)1(1.1%)68(85%)10(13%)2(2.5%)– < 0.001118(71%)34(21%)14(8%)1(1%)123(73%)31(18%)15(9%)–0.879
To derive comparable outcomes data for the comparison, propensity score-weighted analyses (inverse probability of treatment weighting; IPTW) were carried out for two outcomes: time to local recurrence and time to metastasis. Sufficient data were available to carry out the propensity score matching for 80 patients undergoing RAPN and 91 patients undergoing PCA. There was only one death attributed to metastatic RCC and eight other deaths, which were insufficient to allow mortality analysis.
Analytical Method
Potential outcome confounders (age, gender, tumor size, RENAL score, ECOG-PS, and age-adjusted Charlson comorbidity index) were included in the propensity score models. Scores were estimated by fitting a logistic regression model with stabilized IPTW, which was then used to derive pseudo-populations for analysis.
Survival analyses were based on time to local recurrence or metastasis. Patients who did not experience the event of interest or were lost to follow-up were right-censored at the last observed date. A Cox proportional regression model generated estimates of the hazard ratio.
The two pseudo-populations were well-matched (Table 2). Analysis demonstrated no significant differences between PCA and RAPN for either time to local recurrence (HR = 0.80; 95% CI = 0.34–1.85; p = 0.72) or time to metastasis (HR = 2.09; 95% CI = 0.69–6.26; p = 0.19) (Fig. 3). All analyses were conducted in R (R Foundation for Statistical Computing, Vienna, Austria).Fig. 3. Time to event curves. Results of propensity score-matched analysis of patient databases. A = Local recurrence; B = Metastasis
Although the PCA group showed a trend toward earlier recurrence and later metastases, no statistically significant difference was seen for either of these two parameters. Thus, each group had identical transition probabilities for all oncological outcomes based on the 5-year event rates in the pseudo-populations. Mortality estimates for patients with metastatic disease were based on published 5-year survival data [19].
The 90-day postoperative complication rates for each treatment group were taken directly from the dataset: 2.5% in the RAPN group and 5.5% in the PCA group. Only complications with a Clavien-Dindo score of III or above were included, as lesser degrees would have been expected to impact costs and QALYs only modestly [20, 21].
The mean length of stay in the RAPN group was 1.90 nights. For PCA, 85/91 patients were treated as day cases, while the mean length of stay in the six remaining patients was 3.0 nights.
Utilities
The utilities for stable and metastatic diseases were based on published results from the Netherlands [22]. The utility for recurrent disease was assumed to fall midway between stable and metastatic disease, in line with the approach used in a recent economic analysis [13]. The utility for postoperative complications was taken from Casciano et al. [23].
Costs
All costs were expressed as Euros (€), using an exchange rate of DKK 1 = €0.134.
Procedural costs for RAPN were based on the 2024 tariff for Diagnosis-Related Group (DRG) 11MP07 (operations on kidney, renal pelvis, and ureter, malignant disease, patient aged > 18, with robot): €15,293. No specific DRG for PCA is currently approved in Denmark. The estimated per-procedure cost of €7,427 was consequently based on local resource use assessments of staff costs, length of stay, and costs of major single-use equipment.
Results
Results (Table 3) demonstrate a near equality of efficacy outcome: both interventions yield a similar discounted 5-year QALY gain (3.323 vs 3.315). Over 5 years, total costs associated with PCA were 32% lower than those incurred in the RAPN group (€18,795 vs €27,520). This suggests that PCA marginally dominates RAPN, although the minimal incremental QALY makes this an uncertain conclusion. More informative in this situation is the net monetary benefit (NMB), which places the assumed value of the QALY gain alongside the difference in resource use in a single metric. A positive value for the NMB implies a cost-effective treatment at the stated willingness-to-pay threshold. The base case demonstrates an NMB of +€9,045 for this model, at a willingness-to-pay threshold of €40,000/QALY, confirming that PCA is a cost-effective intervention. Table 3. Results of base case analysis—5-year time horizon; costs and benefits discounted at 3% per annum, with a willingness to pay = €40,000/QALYTreatment groupAbsoluteIncrementalICERNMBCostQALYsCost**QALYsRAPN€27,5203.315PCA€18,7953.323€-8,7250.008Dominant€ 9,045ICER = Incremental cost-effectiveness ratio; NMB = Net monetary benefit
Deterministic sensitivity analysis (Fig. 4) shows that the NMB is most sensitive to variations in the probability of metastases for the two treatment strategies, with procedural cost parameters also significantly affecting the outcome. Other factors, such as local recurrence risk and the cost of downstream treatments, are less essential drivers of NMB. All explored ranges showed positive NMB, indicating robust cost-effectiveness for PCA.Fig. 4. Tornado plot showing the impact of the deterministic sensitivity analysis on net monetary benefit. Top 17 parameters listed based on the magnitude of effect on NMB Black bars = NMB based on high parameter estimate; Gray bars = NMB based on low parameter estimate
Discussion
This study uses prospective real-world data from two Danish centers to demonstrate that PCA has comparable oncological outcomes to RAPN in patients with stage T1 RCC. Using these data in a cost-effectiveness model yields near-identical health benefits over five years. However, the overall cost of PCA treatment is lower, making PCA the economically dominant treatment over RAPN. The finding of a positive NMB indicates that PCA represents a more efficient use of resources and is consequently the preferred choice from a health economic perspective.
The lower costs for PCA are driven by the index procedure's costs—principally lower theater costs and shorter postoperative length of stay. The 90-day rate of postoperative complications at Clavien-Dindo grade III and above was non-significantly higher in the PCA group vs the RAPN group (5.5% vs 2.5%). Analysis of the complication rates in this dataset has been previously published [17], with the authors noting that the observed rates in the PCA group are higher than rates seen in an earlier retrospective case series that also used the Clavien-Dindo classification [24]. This appears to reflect significantly different durations of postoperative follow-up for complications in the two studies (90 days vs 30 days). In the current dataset, the principal driver of the excess severe complication rate for PCA was six cases of delayed abscess formation diagnosed after 30 days. In the Schmit et al. case series, only one abscess occurred out of 398 cases analyzed [24]. When a 30-day limit was applied to the current dataset, the observed complication rates were similar between the two studies. Additionally, sensitivity analysis shows these costs are relatively unimportant determinants of overall health economic outcomes [Fig. 4]. Consequently, this is unlikely to have influenced the result of the current analysis.
Previously published health economic analyses exist comparing nephron-sparing surgery with percutaneous localized treatments [13, 14, 25–29], although in the absence of randomized controlled trials, these are typically derived from retrospective case series. The conclusions of a recent literature-based cost-utility analysis carried out by Wu et al. were very similar to those of our analysis, with 5-year efficacy outcomes being nearly identical between the two groups (3.68 vs 3.67 QALYs). Costs in the PCA group were 23% lower (26,478 ~ €18,278 vs €23,618) [13]. It should be noted that the primary data source in Wu et al.’s model came from patients treated before 2011, and the PN group pertains to open surgery instead of laparoscopic or robot-assisted procedures. Additionally, although propensity score matching was carried out, limited information was available to characterize the tumor complexity, so it is uncertain how well-matched the two treatment groups were [13].
In a cost-consequences analysis, Garcia et al. demonstrated a 36% cost difference favoring PCA vs RAPN in a single-center setting in Brazil (19,399 ~ €10,545 vs €16,450) [14]. This analysis was based on a relatively recent dataset, but the data were not corrected for baseline differences in the treated populations. As our study showed, patients treated with PCA tend to be older, with more comorbidities and higher RENAL scores than those treated with RAPN. The absence of matching in the study by Garcia et al. introduces uncertainty to the quantitative results [14].
Although other, older economic analyses exist, they generally reflect technologies and outcomes that are not representative of current practice and which, consequently, are of limited relevance to the current research question and clinical practice [25–29].
Limitations
Patient data for this analysis were drawn from two University Hospitals in Denmark. All patients undergoing PCA were treated at a single hospital with the appropriate experience and expertise, while both centers undertook RAPN. This imbalance may yield relevant organizational issues that we have been unable to consider in our analysis.
As discussed, baseline differences in the two patient populations also present a source of potential bias. Patients treated with PCA tended to be older and had a higher RENAL score, reflecting more advanced tumors with higher case complexity and, consequently, surgical and oncological risk. Furthermore, patients in the PCA group had a greater prevalence of life-limiting non-renal comorbidities, as evidenced by a higher Charlson comorbidity index. We undertook a propensity score weighting approach to generate matched pseudo-populations to minimize the impact of these differences on the clinical outcome results. However, even though we achieved a high level of matching for the parameters under consideration, it is possible that there remained unmatched confounders.
Additionally, the analysis included both T1a and T1b tumors. However, subgroup analysis by stage was not performed due to limited statistical power, especially within the cryoablation subgroup. This should be considered when comparing our findings to studies that included only T1a tumors, as differences in tumor stage may influence outcomes and generalizability.
The approach for assigning costs to the treatment options is a limiting factor to the analysis. For RAPN, a specific DRG is identified within the Danish tariff (11MP07) with a value of €15,293. There is no specified DRG for PCA, so a bottom-up estimate was used based on known materials costs and clinician-estimated healthcare resource use. In the absence of contemporaneously collected resource use data, it is possible that either estimate could be an inaccurate representation of the actual costs. Infrastructure costs were not captured, nor were costs for potential additional procedures, such as inserting a JJ stent before PCA of a complex tumor, included. However, the relative costs of RAPN and PCA are consistent with the values used in other published comparisons [14, 28, 29].
Structural issues within the model may have impacted the results. A 5-year time horizon was used to maintain the modeled outcomes within the evidence’s timeframe, avoiding the need for extrapolation, which could have introduced bias. Given that most of the between-group differences observed in the model accrue in the perioperative period, with minimal differences in long-term oncological outcomes expected, extrapolation would have been unlikely to produce a more informative result.
Conclusion
The present study reported comparable oncological outcomes following PCA and RAPN, utilizing prospectively collected real-world data from patients with RCC T1, leading to near-identical QALYs for the two treatment options. Additionally, a 32% cost reduction was found for PCA compared to RAPN. This study suggests that PCA may offer cost savings for RCC T1 patients without compromising oncological outcomes, making it a cost-effective treatment option over a 5-year time horizon.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World cancer research fund international. Kidney cancer statistics. 2020. Available at: https://www.wcrf.org/cancer-trends/kidney-cancer-statistics/
- 2Dansk Renal Cancer database (Da Ren Ca Data) Dansk Urologisk Cancergruppe Årsrapport 2023. Available at: https://www.sundhed.dk/content/cms/86/15686_darencadata_aarsrapport-2023_offentliggjort.pdf
- 3EAU Guidelines. Edn. presented at the EAU Annual Congress Paris 2024. Available at: https://d 56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Renal-Cell-Carcinoma-2024.pdf