A multiplex assay based on capillary electrophoresis to detect Mycobacterium tuberculosis complex: development and clinical validation
Yaocheng Wang, Zhen Li, Li Lai, Yiping Liu, Li Li, Yi Huang

TL;DR
A new test using capillary electrophoresis detects three tuberculosis-related genes at once, improving diagnostic accuracy and reducing errors.
Contribution
A novel multiplex capillary electrophoresis assay for simultaneous detection of three MTBC genes, enhancing diagnostic accuracy.
Findings
The assay detected MTBC genes IS6110, rpoB, and HSP65 with 100% analytical specificity and no cross-reactivity.
Clinical validation showed 77.4% sensitivity and 99.6% specificity in diagnosing tuberculosis.
Six MTBC strains with IS6110 deletions were identified, which would be missed by single-gene PCR tests.
Abstract
This study presents a novel multiplex assay based on capillary electrophoresis (CE) for the simultaneous detection of three Mycobacterium tuberculosis complex (MTBC) genes: IS6110, rpoB, and HSP65. Unlike conventional molecular diagnostic methods that target only a single gene, which may lead to misdiagnosis or missed diagnosis, this CE-based multiplex approach provides comprehensive detection to reduce diagnostic errors. Specificity testing with 76 microorganisms representing common respiratory pathogens confirmed 100% analytical specificity with no cross-reactivity, while sensitivity analysis demonstrated detection limits ranging from 10 to 20 copies/mL for all three target genes. In a prospective clinical validation study of 1067 patients suspected of pulmonary tuberculosis, the multiplex assay showed 77.4% sensitivity (CI 74.9%–79.9%), 99.6% specificity (CI 99.2%–100%), 96.0%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
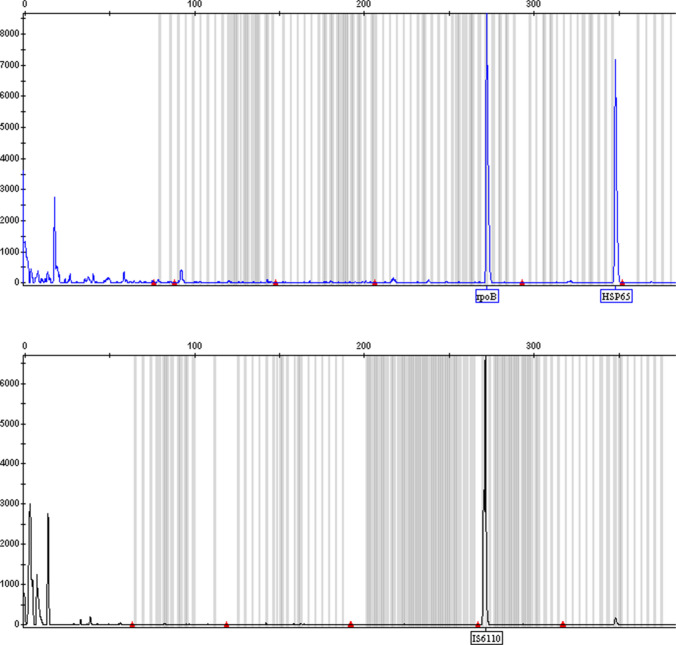 Figure 1
Figure 1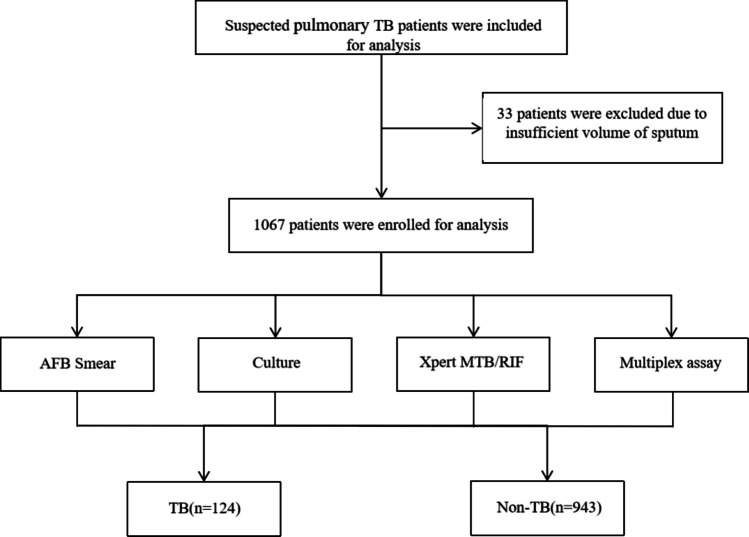 Figure 2
Figure 2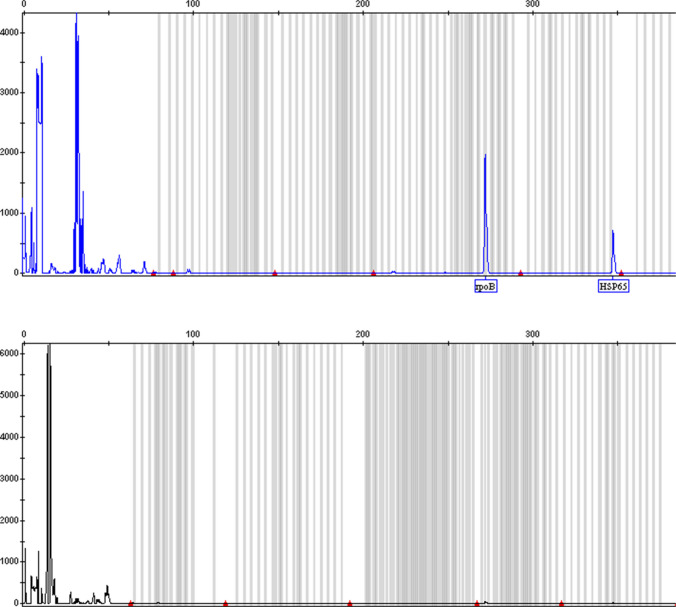 Figure 3
Figure 3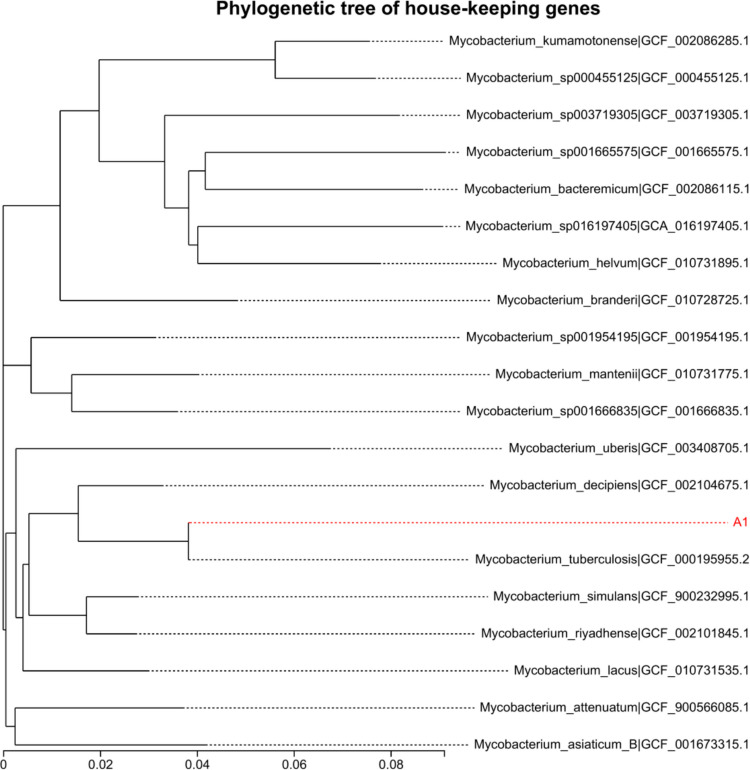 Figure 4
Figure 4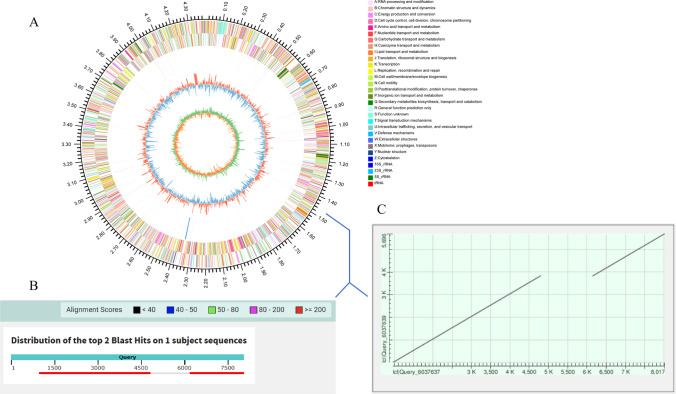 Figure 5
Figure 5- —Fujian Medical University, China
- —the Natural Science Foundation of Fujian Province, China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Mycobacterium research and diagnosis · Microfluidic and Capillary Electrophoresis Applications
Introduction
Tuberculosis (TB), which is caused by Mycobacterium tuberculosis complex (MTBC) infection, is still a global health epidemic, showing significant morbidity and mortality (WHO 2025). Indirect evidence suggests that one in four people is infected with MTBC worldwide, and 5%–10% of those develop TB (Houben et al. 2016). According to the World Health Organization (WHO), an alarming 10.7 million people were diagnosed with TB in 2024, and the number of TB-related deaths was about 1.23 million (WHO 2025). This highlights the need to take urgent action for TB prevention. Rapid identification of MTBC is of paramount importance towards early diagnosis of TB, leading to effective infection control.
For the advantages over conventional diagnostic methods like mycobacterial culture, which is time-consuming and acid-fast bacilli (AFB) smear with low sensitivity, nucleic acid amplification tests (NAATs) have been widely applied for rapid diagnosis of TB, among which the Xpert MTB/RIF assay, endorsed by the World Health Organization (WHO) in 2010, has been a significant advancement offering rapid detection of Mycobacterium tuberculosis and rifampicin resistance in less than 2 h. These techniques are based on the amplification of unique mycobacterial target sequences. Several appropriate genes, such as 16SrRNA, IS6110, IS1081, HSP65, and rpoB, have been utilized for these molecular methods. However, most of the molecular assays that are currently in use only target one gene, which can lead to the misdiagnosis of tuberculosis (Comín et al. 2022; Huang et al. 2022; Pang et al. 2017; Jin et al. 2023; Chin et al. 2020). Meanwhile, due to point mutations in primer binding regions, low bacterial load, sample inhibitors, and assay limitations, false-negative results may occur, resulting in a missed diagnosis of tuberculosis (Phyu et al. 2018; Moradiya et al. 2020).
Capillary electrophoresis (CE) can separate charged macromolecules, such as DNA, which separates molecules based on their differential migration in an electric field. CE can separate DNA fragments of up to 1000 nucleotides with single-nucleotide resolution. It is a robust analytical technique with several potential advantages, such as short analysis time, low sample volume requirements (nanoliter or less), and high efficiency. For the most part, it has multianalyte capability, which allows it to assay multiple targets simultaneously. Furthermore, with flexible applications of parallel operation, CE has the potential for high-throughput analysis.
We therefore developed a CE-based multiplex molecular detection assay capable of detecting three MTBC genes: IS6110, rpoB, and HSP65. The selection of target genes was based on their established roles in MTBC identification and diagnostic utility. IS6110 is a highly specific and multi-copy insertion sequence within the MTBC, widely used for molecular detection. rpoB encodes the β-subunit of RNA polymerase and is associated with rifampicin resistance; its inclusion allows for potential simultaneous detection of drug resistance. HSP65 is a conserved heat shock protein gene frequently used for mycobacterial species differentiation. We then evaluated this method’s analytical performance and conducted clinical validation. By targeting these three genes simultaneously, we aim at enhancing diagnostic robustness, particularly in cases where one target may be absent or mutated.
Materials and methods
Primer design
Three pairs of oligonucleotides were required to detect the target genes of MTBC. Briefly, they were designed as follows: first, gene sequences were retrieved from NCBI for the following mycobacterium: M. tuberculosis (ATCC 27294), M. marinum (ATCC 927), M. gordonae (ATCC 14470), M. scrofulaceum (ATCC 19981), M. terrae (ATCC 15755), M. fortuitum subsp. fortuitum (ATCC 6841), M. asiaticum (ATCC 25276). Second, comparative analysis was performed through sequence alignment using Clustal Omega to obtain the conserved regions of the three target genes. Third, Primer Premier 5 software was used to design the primers according to the conserved regions. Then, the specificity of these forward primers was tested in silico using the BLAST tools from NCBI. To discriminate the three targets, these three forward primers were labelled with fluorophores, 6-FAM and TAMRA, respectively, at the 5′-end to be subsequently detectable by electrophoresis. Additionally, cross-reaction of these reverse primers should be avoided.
DNA extraction
The Chelex-100 method was modified for DNA extraction. Specifically, two loops of freshly grown mycobacterial cultures from L-J medium were added to 300 μl of water containing Chelex resin. To improve the efficiency of DNA extraction, 10 μl proteinase K (10 mg/ml) was added to the DNA extraction process, considering the high lipid content in the MTBC membrane. Incubate at 56 °C for 20 min and then boil at 100 °C for 5 min to release DNA. Following this, the sample was centrifuged to pellet cellular debris and Chelex resin, and the supernatant was used as the DNA template. Then, DNA concentration and purity were determined by spectrophotometer (NanoDrop One, Thermo Scientific, USA).
Polymerase chain reaction
In brief, the PCR reaction was carried out in a 50-μL mixture each containing 1.0 μL dNTP (10 mmol/L) (Invitrogen, USA), 2.0 μL AmpliTaq Gold™ DNA polymerase (5U/μL) (ABI, USA), 5.0 μL PCR Buffer(without Mg^2+^) (ABI, USA), 8.0 μL MgCl_2_(25 mmol/L) (ABI, USA), 26.0 μL amplification-grade water (Promega, USA), 0.5 μL each primer, and 5.0 μL DNA template. The reaction was performed using an automated thermal cycler (Verity, ABI, USA). The following PCR protocol was used: predenaturation of 94 ℃ for 5 min, 35 cycles of 94 ℃ for 30 s, 55 ℃ for 1 min, and 72 ℃ for 1 min, then a final extension step of 72 ℃ for 1 min.
Capillary electrophoresis
The 3130 genetic analyzer (ABI, USA) was utilized. The procedures were briefly as follows: first, a 9.0-μL mixture of LIZ 500 (Promega, USA) and HiDi buffer (Promega, USA) in a 1:130 ratio was added to a 96-well plate. A 1.0-μL multiplex PCR product was then pipetted into each well, followed by a pre-denaturation process with heating the plate to 99 ℃ for 3 min. Then, capillary electrophoresis was performed according to the manufacturer’s instructions.
Whole-genome and Sanger sequencing
Genomic DNA from MTBC isolates with discordant or irregular molecular assay results was sent to Majorbio (Shanghai, China) for whole-genome sequencing. To increase the accuracy and integrity of genome assembly, we employed a dual-platform strategy using both next-generation sequencing (Illumina) for high-depth short-read data and third-generation sequencing (PacBio) for long-read data. The raw Illumina reads were first quality-checked using FastQC and then filtered and trimmed. For long-read data, quality control was performed using the SMRT Analysis suite. Assembly was conducted using hybrid assembly approaches with SOAPdenovo and unicycler, which allowed us to leverage the strengths of both sequencing technologies. The assembled genomes were annotated using Prokka, and sequence alignments were performed with BLAST. For phylogenetic analysis, a set of 31 housekeeping genes was extracted from the assemblies, and the evolutionary relationships were constructed using MEGA 6.0 via the neighbor-joining method.
Analytical evaluation
The analytical sensitivities of the multiplex assay were evaluated by determining the limit of detection (LOD). The LOD was measured using spiked samples with ATCC 27294. Twenty replicates were evaluated at five concentrations around LOD, and the LOD was determined using probit analysis. Then, studies were performed to determine the analytical specificity. Seventy-six (76) microorganisms (Table 1), which represent common respiratory pathogens, were tested at the following concentrations: DNA at 1 × 10^7^ copies/mL for bacteria and fungi, nucleic acid at 2 × 10^9^ copies/mL for viruses, DNA at 1 × 10^5^ copies/mL for nontuberculous mycobacteria, and a concentration of 10^6^ elementary bodies (EB) per mL for Chlamydia. All specificity and sensitivity assays were tested in duplicate.
Table 1. Microorganisms tested for analytical evaluationMicroorganismsOriginMicroorganismsOriginMycobacterium gastriATCC15754Haemophilus influenzaeClinical isolatesMycobacterium terraeATCC15755Haemophilus parainfluenzaeClinical isolatesMycobacterium xenopiATCC19250Klebsiella oxytocaClinical isolatesMycobacterium smegmatisATCC19420Klebsiella pnenmoniaeClinical isolatesMycobacterium ulceransATCC19423Legionella pneumophilaClinical isolatesMycobacterium thermoresistibileATCC19527Micrococcus luteusClinical isolatesMycobacterium abscessusATCC19977Morganella morganiiClinical isolatesMycobacterium scrofulaceumATCC19981Mycobacterium fortuitumClinical isolatesMycobacterium simiaeATCC25275Mycobacterium gordonaeClinical isolatesEscherichia coliATCC25922Mycobacterium intracellulareClinical isolatesStaphylococcus aureusATCC25923Mycobacterium kansassiClinical isolatesPseudomonas aeruginosaATCC27853Neisseria meningitidisClinical isolatesMycobacterium haemophilumATCC29548Nocardia asteroidesClinical isolatesMycobacterium malmoenseATCC29571Nocardia brasiliensisClinical isolatesShigella flexneriATCC29903Nocardia farcinicaClinical isolatesMycobacterium chelonaeATCC35752Proteus mirabilisClinical isolatesMycobacterium szulgaiATCC35799Proteus vulgarisClinical isolatesMycobacterium celatumATCC51131Pseudomonas aeruginosaClinical isolatesMycobacterium genavenseATCC51234Pseudomonas fluorescensClinical isolatesMycobacterium marinumATCC927Pseudomonas putidaClinical isolatesMycobacterium colombienseCIP108962Serratia marcescensClinical isolatesMycobacterium paraintracellulareJCM30622Shigella boydiiClinical isolatesMycobacterium MassilienseCIP108297Staphylococcus capitisClinical isolatesMycobacterium bolletiiDSM45149Staphylococcus epidermidisClinical isolatesMycobacterium aviumClinical isolatesStaphylococcus haemolyticusClinical isolatesAcinetobacter baumanniiClinical isolatesStaphylococcus saprophyticusClinical isolatesAcinetobacter calcoaceticusClinical isolatesStenotrophomonas maltophiliaClinical isolatesAcinetobacter haemolyticusClinical isolatesStreptococcus agalactiaeClinical isolatesAcinetobacter juniiClinical isolatesStreptococcus midisClinical isolatesAlcaligenes faecalisClinical isolatesStreptococcus salivariusClinical isolatesBranhamella catarhalisClinical isolatesAdenovirusNIFDC 370057-202001Candida albicansClinical isolatesCoronavirusNIFDC 370057-202001Citrobacter freundiiClinical isolatesHuman metapneumovirusNIFDC 370057-202001Corynebacterium diphtheriaeClinical isolatesInfluenza B VirusNIFDC 370057-202001Enterobacter aerogenesClinical isolatesParainfluenza virusNIFDC 370057-202001Enterobacter cloacaeClinical isolatesRespiratory syncytial virusNIFDC 370057-202001Enterococcus faecalisClinical isolatesRhinovirusNIFDC 370057-202001Enterococcus faeciumClinical isolatesRubella virusNIFDC 370057-202001ATCC: American Type Culture Collection; CIP: Collection of Institut Pasteur, France; JCM: Japan Collection of Microorganisms; DSM: Deutsche Sammlung von Mikroorganismen und Zellkulturen, German; NIFDC: National Institutes for Food and Drug Control, China
Clinical performance
A prospective cohort study was conducted to evaluate the performance characteristics of the multiplex assay. Inclusion criteria: Subjects 18 years or older were eligible for the study if they were suspected of pulmonary tuberculosis (based on symptoms such as persistent cough, fever, weight loss, night sweats, and/or abnormal chest radiography findings) in Fujian Provincial Hospital, China, and on no TB treatment or with less than 3 days of TB treatment. Exclusion criteria: insufficient sputum volume. Then, we estimated that a sample size of 1100 patients is needed to obtain a between-group difference with more than 99% power. Meanwhile, this is an adequate sample size for evaluating the sensitivity and specificity according to the CLSI guideline. Testing should continue until results from at least 50 positive specimens, as a minimum guideline, are obtained with both the test and comparative method. The Institutional Ethics Committee of Fujian Provincial Hospital approved the study.
Sputum specimens collected from subjects were tested using AFB smear, culture, and Xpert MTB/RIF. Also, a single leftover sputum sample was tested using the multiplex assay. All the participants were at least independently diagnosed by two doctors based on clinical and laboratory findings. If the diagnosis is different, another doctor is required. Then, the sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) of the four methods were calculated, respectively.
Discordant results for MTBC culture positive and molecular assay negative, irrespective of Xpert MTB/RIF or multiplex assay, were further evaluated using bi-directional sequencing of the corresponding region of the genome. If needed, WGS was used for further validation.
Data analysis
Statistical analyses were performed using SPSS Statistics 24, including the sensitivity, specificity, NPV, and PPV of the four methods adopted in this study, and their corresponding 95% confidence interval (CI). Probit analysis was used to determine the LOD of the multiplex assay. The LOD was defined as the lowest DNA concentration detected in 95% of 20 replicates for every target gene.
Result
CE-based multiplex assay
Specific primers (Table 2) targeted IS6110, rpoB, and HSP65 were designed based on their conserved regions, respectively. Then, the specificity of these forward primers was examined in silico. Compared with the core nucleotide BLAST database, which consists of 108,970,392 sequences, the number of hits for the forward primer targeted IS6110 is 101, 99 for MTBC, and 2 for Mycobacterium avium complex. For rpoB, the number of hits is 109, which includes 2 for Pontimonas sp. and 107 for MTBC. The number of hits for the forward primer targeted HSP65 is 101, which is all for MTBC. Moreover, the identity of all these hits above is 100%. Table 2. Oligonucleotides used for amplification by PCRGeneOligonucleotideSequenceFluorophoresSizeIS6110**IS6110-F5’-TACGGTGCCCGCAAAGTG-3’5'-TAMRA271bpIS6110-R5’-AGGCGTCGGTGACAAAGG-3’/rpoB**rpoB-F5'-CCAATTCATGGACCAGAACAA-3'5'−6-FAM270 bprpoB-R5'-TACACGATCTCGTCGCTAACC-3'/HSP65**HSP65-F5'-AGCGATTTCGGCGGGTGA-3'5'−6-FAM346 bpHSP65-R5'-TCTTGTTGACGACCAGGGTG-3'/
The result of Mycobacterium tuberculosis H37Rv (ATCC 27294) using this multiplex assay is in line with expectations (Fig. 1). After targeted DNA sequencing and alignment with reference sequence, the identity is 99.3% (269/271), 99.3% (268/270), and 98.8% (342/346) for IS6110, rpoB, and HSP65, respectively (Fig. S1).Fig. 1. The result of Mycobacterium tuberculosis H37Rv (ATCC 27294) using multiplex assay
Analytical evaluation
Three target genes were all successfully detected by the multiplex assay with an LOD ranging from 10 to 20 copies/mL (Table 3). Irrespective of the type of microorganisms, genomic DNA extracts from 76 respiratory pathogens were not detected by the multiplex method. So, the analytical specificity of the multiplex assay is 100% at the given concentration regarding bacteria, fungi, viruses, Chlamydia, and nontuberculous mycobacteria.
Table 3. Detection limit of Multiplex assay for three target genesGeneMultiplex assayLimit of detection (copies/mL)^a^Number of replicatesNumber detected% detectedIS6110102020100rpoB20201995HSP65202020100^a^ The limit of detection (LOD) was defined as the lowest DNA concentration that was detected in 95% of 20 replicates
Clinical performance
A total of 1100 patients were enrolled between January 2023 and December 2023, excluding 33 patients due to insufficient sputum volume. The final enrollment of 1067 patients was performed by AFB smear, culture, Xpert MTB/RIF, and the multiplex assay. Figure 2 shows the classification of patients included in this study. In total, 124 patients were diagnosed with pulmonary tuberculosis. The overall positive rates of AFB smear, culture, Xpert MTB/RIF, and the multiplex assay, not taking the diagnosis into account, were 4.9%, 11.8%, 10.0%, and 9.4%, respectively (Table 4). However, for the TB patients, the positive rates were 25.8%, 75.0%, 79.8%, and 77.4%, respectively.Fig. 2. The flowchart of patients included in this study
Table 4. Performance of different methods to diagnose TB in the cohortDetection Methods Test ResultsRateDiagnosisSensitivitySpecificityPPVNPVTBNon-TBCICICICIAFB smearPositive4.9%32(25.8%)21(2.2%)25.8%97.7%60.4%90.9%Negative95.1%92(74.2%)922(97.7%)23.2%−28.4%96.9%−98.7%57.4%−63.3%89.2%−92.7%CulturePositive11.8%93(75.0%)32(3.3%)75.0%96.7%74.4%96.7%Negative88.2%31(25.0%)911(96.7%)72.4%−77.6%95.5%−97.7%71.8%−77.0%95.6%−97.8%Xpert MTB/RIFPositive10.0%99(79.8%)8(0.8%)79.8%99.2%92.5%97.4%Negative90.0%25(20.2%)935(99.2%)77.4%−82.3%98.6%−99.7%91.0%−94.1%96.4%−98.4%Multiplex assayPositive9.4%96(77.4%)4(0.4%)77.4%99.6%96.0%97.1%Negative90.6%28(22.6%)939(99.6%)74.9%−79.9%99.2%−100%94.8%−97.2%96.1%−98.1%PPV, Positive Predictive Value. NPV, Negative Predictive Value. CI, 95% upper and lower confidence interval
Comparisons of the four methods for the MTBC are given in Table 4. In total, 93 patients tested positive for multiplex assay, all of which were culture-positive. However, 31 patients who were not finally diagnosed with TB were culture-positive, all of which were multiplex assay–negative. Conversely, other 4 non-TB patients, who were diagnosed as obsolete pulmonary tuberculosis, were Xpert MTB/RIF positive and multiplex assay–positive, none of which was culture-negative. The overall sensitivity of AFB smear for all 1067 patients was 25.8% (CI 23.2%–28.4%), specificity 97.7% (CI 96.9%–98.7%), PPV 60.4% (CI 57.4%–63.3%), and NPV 90.9% (CI 89.2%–92.7%). The corresponding values for culture were 75.0% (CI 72.4%–77.6%), 96.7% (CI 95.5%–97.7%), 74.4% (CI 71.8%–77.0%), and 96.7% (CI 95.6%–97.8%). Meanwhile, the multiplex assay showed 77.4% (CI 74.9%–79.9%) sensitivity, 99.6% (CI 99.2%–100%) specificity, 96.0% (CI 94.8%–97.2%) PPV, and 97.1% (CI 96.1%–98.1%) NPV.
Identification of IS6110-like element in MTBC
Among the 93 patients who were culture, Xpert MTB/RIF and multiplex assay triple positive, we could not detect IS6110 element in 6 TB patients using the multiplex assay (Fig. 3). Due to the possibility of misdiagnosis, a more careful analysis of the 6 isolates was carried out using WGS. The evolutionary relationship of the 6 isolates, based on dnaG, frr, infC, nusA, pgk, pyrG, rplA, rplB, rplC, rplD, rplE, rplF, rplK, rplL, rplM, rplN, rplP, rplS, rplT, rpmA, rpoB, rpsB, rpsC, rpsE, rpsI, rpsJ, rpsK, rpsM, rpsS, smpB, and tsf 31 housekeeping genes, is displayed in Fig. 4 (take A1 isolate as an example). Phylogenetic analysis revealed that the 6 isolates most likely belonged to Mycobacterium tuberculosis.Fig. 3. Example of the result of TB patients (IS6110 deletion) using multiplex assayFig. 4Phylogenetic tree of A1 isolate. The phylogenetic analysis was conducted based on dnaG*, frr, infC, nusA, pgk, pyrG, rplA, rplB,rplC, rplD, rplE, rplF, rplK, rplL, rplM, rplN, rplP, rplS, rplT, rpmA, rpoB, rpsB, rpsC, rpsE, rpsI, rpsJ, rpsK, rpsM, rpsS, *smpB, and tsf 31 housekeeping genes, using MEGA 6.0 by neighbor-joining method
Furthermore, the whole genomes were obtained after genome assembly (Fig. 5A). As expected, we could not find the oligonucleotide sequence designed for IS6110 in these genomes. Neither did we find the reverse complementary sequence. Since IS6110 was multicopy and belonged to mobile genetic elements, we attempted to position one deletion in these genomes. Then, sequence alignment with Mycobacterium tuberculosis H37Rv reference sequence (accession ID NC_000962) was carried out using BLAST tools. Finally, we positioned one deletion at location: 1463537 (Fig. 5B, C). In comparison with the reference sequence, we found an approximate 1500-bp deletion did exist in the IS6110 corresponding region.Fig. 5. The location of IS6110 deletion. A Circos plot of the genome of A1 strain. B Alignment of sequence in the location of IS6110 deletion with Mycobacterium tuberculosis H37Rv reference sequence. C Dot plot of the alignment
Discussion
About a quarter of the population is globally estimated to have been infected with MTBC (Cohen et al. 2019). Rapid and accurate detection of MTBC is of great significance in controlling the TB spread, a devastating infectious disease (Naidoo et al. 2022). Nowadays, various commercially available NAATs kits are adopted in clinical laboratories worldwide (Mousavi-Sagharchi et al. 2024). Also, various novel NAATs methods are developed for MTBC detection (Wang et al. 2024; Batuer et al. 2024; Svensson et al. 2021; Yee et al. 2020; Huang et al. 2022; Homann et al. 2021; Shan et al. 2022). However, most of these molecular kits only target one gene. This can lead to the misdiagnosis and missed diagnosis of TB. Misdiagnosis of TB can bring about substantial negative consequences (Houben RMGJ et al. 2019). Firstly, a treatment course that lasts at least 6 months will be falsely recommended. Also, patients will incur substantial costs for clinical services and nonclinical expenses, like transportation, food, childcare, and lost wages (Laurence et al. 2015). Meanwhile, missed diagnosis of TB can result in the delay of treatment for patients, which can do harm to TB prevention (Medrano et al. 2014). Here, we propose a novel, rapid, and multi-target method that can detect three genes of MTBC simultaneously, aiming to provide a more comprehensive method for MTBC to reduce the misdiagnosis and missed diagnosis of TB.
This is the first study that developed a multiplex assay to detect MTBC based on the CE platform. To ensure the specificity of this method, a two-step strategy was employed to design PCR primers. First, the conserved regions of the MTBC were identified through sequence alignment with several common NTM. Then, the BLAST tools from NCBI were utilized to test the specificity of these primers, which were designed based on the conserved regions. Specifically, compared with the core nucleotide BLAST database, it showed probable cross-reactivity with *Pontimonas *sp. for rpoB and Mycobacterium avium complex for IS6110, proving no cross-reaction occurred by follow-up experiments. Also, here we report the performance of this method in a cohort, with 1067 patients finally enrolled, compared with AFB smear, culture, and Xpert MTB/RIF. The multiplex assay exhibited a sensitivity of 77.4% vs. 25.8% of AFB smear, 75.0% of culture, and 79.8% of Xpert MTB/RIF. The increment in sensitivity of the multiplex assay over AFB smear was significant, whereas the increment in sensitivity of the multiplex assay over culture was marginal. Also, we observed a low increment in specificity and NPV of the multiplex assay over AFB smear, culture, and Xpert MTB/RIF (specificity 99.6% vs. 97.7%, 96.7%, and 99.2%, respectively, NPV 97.1% vs. 90.9%, 96.7%, and 97.4%, respectively). However, regarding PPV, the corresponding value of the multiplex assay was 96.0% vs. 60.4%, 74.4%, and 92.5% for AFB smear, culture, and Xpert MTB/RIF, respectively. Xpert MTB/RIF is acknowledged to be an excellent method to detect MTBC (WHO 2020). In this context, it is worth noting that, with more target genes to be detected simultaneously, the multiplex assay performed at least as well as Xpert MTB/RIF.
Compared to the Xpert MTB/RIF assay, which is a fully integrated, cartridge-based system suitable for point-of-care settings, our CE-based approach is more suitable for centralized laboratories with existing capillary electrophoresis infrastructure. In terms of cost per test, our method may be more economical in high-throughput settings, though it requires an initial investment in CE equipment. A detailed comparison of key characteristics between our assay and the Xpert MTB/RIF system is provided in Table S1. The primary advantage of our assay lies in its multi-target design, which enhances diagnostic accuracy, particularly in regions with circulating IS6110-deficient strains.
During the clinical evaluation of the multiplex assay, we discovered 6 strains of MTBC with suspected IS6110 deletion. First, we adopted Sanger sequencing for IS6110, rpoB, and HSP65, three genes, to identify these strains. Regarding rpoB and HSP65, the results were in line with the reference sequence of Mycobacterium tuberculosis (data not shown). Nevertheless, we could only obtain the IS6110 sequence result if we designed these primers. Then, the whole genomes were obtained using WGS based on the Illumina and Pacbio platforms. According to the phylogenetic analysis based on 31 housekeeping genes, these 6 strains belonged to Mycobacterium tuberculosis. Moreover, after the genome assembly, an approximate 1500-bp deletion did exist in the IS6110 corresponding region. Owing to this finding, we could also recognize that the long gap was why we failed to get the results by Sanger sequencing. Certainly, in this regard, it would lead to a false negative result for any commercial PCR kits targeted at IS6110. Although we just discovered 6 IS6110 deletion strains (4.8%, 6/124) in our study, it was reported that the corresponding frequency was about 8% and 11% in Viet Nam and India, respectively (Chauhan et al. 2007). This indicates the necessity of the multiplex assay we developed here to reduce the missed diagnosis of TB.
The study has limitations. First, clinical validation of this multiplex assay was performed on just one site, which may lead to bias. Second, considering sputum volume, we select Xpert MTB/RIF targeted rpoB as a comparison in the cohort, endorsed by WHO (WHO 2020). So, in this regard, another two molecular assays, targeted IS6110 and HSP65, respectively, were needed. Third, although 76 microorganisms, which represent common respiratory pathogens, were selected for analytical specificity, we did not take *Pontimonas *sp., which showed 100% identity aligned with the oligonucleotide designed for rpoB, into evaluation, since the corresponding strain was not available in our library.
In conclusion, the multiplex assay simultaneously provides one-run results for IS6110, rpoB, and HSP65, maintaining adequate sensitivity, specificity, PPV, and NPV for TB diagnosis. We present a more comprehensive method to detect MTBC. Although this is only a small fraction of the overall endeavor for accurate diagnosis, the multiplex assay has the potential to reduce misdiagnosis and missed diagnosis of TB. To achieve the global end TB goals, the multiplex assay, a comprehensive alternative to methods currently used, deserves further field evaluation.
Supplementary Information
Below is the link to the electronic supplementary material.ESM 1(DOCX 13.5 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chin, K, Sarmiento, M, Mustapha, Z, Acosta, A (2020) Identification of a Rothia mucilaginosa strain in a clinical specimen based on PCR-sequencing with mycobacterium hsp 65 primers J CLIN DIAGN RES, 10.7860/jcdr/2020/44942.13975