A historical review of mycosis fungoides: from Alibert to mogamulizumab
Nicholas A Johnson, Opeoluwa Fariyike, Khaylen Mistry, Zoe Venables, Nick J Levell

TL;DR
This paper reviews the history of mycosis fungoides, tracing its discovery and evolving understanding from the 19th century to modern treatments.
Contribution
The paper provides a historical perspective on the nomenclature, diagnosis, and treatment of mycosis fungoides over two centuries.
Findings
Mycosis fungoides was first described in 1806 by Alibert and misclassified as a fungal disease.
The term cutaneous T-cell lymphoma was established in 1975, clarifying the disease's origin.
Modern therapies now include monoclonal antibodies like mogamulizumab.
Abstract
In 1806, French physician Baron Jean-Louis Alibert saw a man with a desquamating rash and skin tumours. Alibert considered this to be a variant of yaws. In 1829 Alibert named the condition mycosis fungoides (MF), meaning ‘mushroom-like fungal disease’. Over 100 years later, French dermatologist Albert Sézary published papers from 1938 to 1949 detailing a mysterious disease containing ‘cellules monstrueuses’, describing cutaneous ‘monster cells’. In 1961, these clinical findings were collated together into ‘Sézary syndrome’. In the 1870s English dermatologist William Tilbury Fox published a dermatology atlas detailing cases similar to what we know now as MF, with the name ‘fibroma fungoides’. The atlas described MF as a type of fungus, before giving a description of yaws and painting a clinical picture that differed from that of a lymphoma. Over the twentieth century, our understandings…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
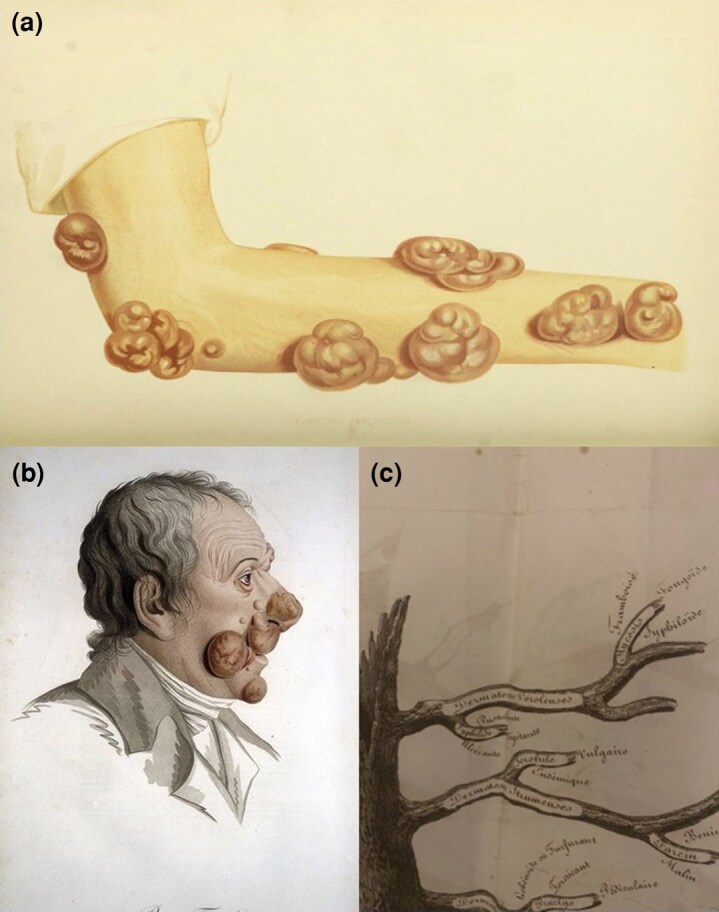 Figure 1
Figure 1| Patient number | Date of case | Author | Book | Sex/age (years) if disclosed | Key term(s) to describe lesions | Final diagnosis |
|---|---|---|---|---|---|---|
| Patient 1 (‘Lucas’) | 1806 | J.L. Alibert |
| Male, 56 | Small tubercles | Pian fongoide. Illustration available in |
| Patient 2 | 1871 | W. Tilbury Fox |
| Male, N/A | Without distinct granulations, fungal ‘excrescences’ Fibrocellular tissue | Fibroma fungoides |
| Patient 3 | Unknown | W. Tilbury Fox |
| Female, N/A | Fibromatous tumours Fibrocellular tissue | Fibroma fungoides/lymphadenoma/‘mycosis of the French’ |
| Patient 4 | Unknown | W. Tilbury Fox |
| N/A, child | Fibrocellular tissue Fleshy masses resembling half-ripe black grapes | Fibroma fungoides |
| Clinical variants | First clinical description of variant | Origin of term |
|---|---|---|
| Alibert–Bazin | 1806: Alibert, later commented upon by Bazin | Named from Alibert’s and Bazin’s contributions |
| Pagetoid reticulosis (Woringer–Kolopp disease) | 1939: Frederic Woringer (1903–1964) and Pierre Kolopp | 1973: term proposed by Otto Braun-Falco (1922–2018) |
| Folliculotropic | 1960: Hans-Georg Piper (1911–1969) | 1985: term ‘follicular’ mycosis fungoides proposed by Sun-Yong Kim |
| Granulomatous slack skin | 1973: Jacinto Convit (1913–2014) | 1978: term ‘granulomatous cutis laxa’ proposed by Albert Bernard Ackerman (1936–2008) |
| Treatment | Inception and first clinical use | First use in MF |
|---|---|---|
| Radiotherapy | 1896: Used to treat malignancy, a year after the discovery of X-rays | 1951: TSEBT used in MF |
| NM gas and mechlorethamine | 1946: Clinical pharmacologists Louis Goodman and Alfred Gilman used NM-based compounds such as methyl-bis (beta-chloroethyl) amine to manage Hodgkin lymphoma, leukaemia and other malignancies | 1959: MF treated with topical mechlorethamine at Cleveland clinic by John R. Haserick and Joseph H. Richardson: |
| Photochemotherapy | 1948: A.M. el-Moft used purified 8-MOP for vitiligo. | 1976: Fitzpatrick treated MF. |
| Interferons | 1957: First named and described. | 1984: Paul A. Bunn Jr described efficacy of high-dose recombinant IFN-α in patients with CTCL |
| VAD | 1962: Topical tretinoin and other VAD compounds were used in malignancies and hyperkeratotic disorders | 1983: John F. Kessler uses isotretinoin in CTCL. |
| HDACi | 1969: Akira Inoue isolated histone deacetylases. | 2006: Vorinostat (SAHA) was approved by the FDA for CTCL, |
| Monoclonal antibodies | 1986: The first monoclonal antibody, orthoclone OKT3, was used to reduce rejection in kidney transplantation. | 2002: Alemtuzumab, an anti-CD52, monoclonal antibody, was first trialled in CTCL. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Lymphoma Diagnosis and Treatment · Histiocytic Disorders and Treatments
First understandings of mycosis fungoides, and its clinical diagnosis
Since its first description in 1806 by French dermatologist Baron Jean-Louis Alibert (1768–1837), there has been confusion about the classification and diagnosis of mycosis fungoides (MF). A 56-year-old man named ‘Lucas’ was treated by Alibert for a desquamating rash and skin tumours, which Alibert termed as ‘pian fongoide’.^1^ The term ‘pian’ was used by European physicians to describe yaws (Treponema pallidum subspecies pertenue),^2^ while ‘fongoide’ described mushroom-like growth. Alibert detailed an ailment that developed small tubercles like a potato or mushroom.^3^ Alibert first used the term ‘mycosis fungoides’ in ‘Monographe des Dermatoses’ in 1835 for the same patient (Figure 1).^4^ This terminology may have caused confusion regarding a possible infective, either fungal or treponemal, aetiology of MF.
(a) Early illustration of fibroma fungoides taken from Tilbury Fox’s Atlas of Skin Disease, 1872, which may represent mycosis fungoides (MF). Credit: Wellcome Library, London, under the Public Domain Universal Licence (https://creativecommons.org/publicdomain/mark/1.0/). (b) Early drawings of MF termed ‘pian fongoide’, taken from skin observed in ‘Description des maladies de la peau observées à l'Hôpital Saint-Louis. Et exposition des meilleures méthodes suivies pour leur traitement / par’, J.L. Alibert 1806. Credit: Wellcome Library, London, under the Creative Commons Attribution Lisence (https://creativecommons.org/licenses/by/4.0/). (c) In J.L. Alibert, Arbre Des Dermatoses in ‘Monographie des Dermatoses’, 1835, MF is grouped with syphilis. Credit: Reproduced from a copy of Monographie des Dermatoses gifted to author N.J.L.
In 1852, William James Erasmus Wilson (1809−1884) from England described Alibert’s comments on MF. Wilson disagreed with Alibert, classifying MF with molluscum contagiosum, then known as molluscum of Bateman.^5,6^
In 1862, Alibert’s student, Pierre-Antioine-Ernest Bazin (1807–1878), described three progressive stages of MF: eczematoid, infiltrative and tumoural, which later became known as the ‘Alibert–Bazin’ type.^7^ By 1874, Wilson had given the condition the name ‘eczema tuberculatum’.^8^
In 1877, English dermatologist William Tilbury Fox (1836–1879) published in Atlas of Skin Diseases four cases of ‘fibroma fungoides’.^9^ Fox gave the opinion that fibroma fungoides existed separately from lymph adenomas, epitheliomas, contractile keloids and MF of the French, as described by Alibert. A summary of these cases, and their key descriptions, can be found contrasted against Alibert’s ‘pian fongoide’ in Table 1.
Confusion about the cause and origin of MF was widespread in the early and mid-nineteenth century as diagnosis was by visual examination. In the absence of precise diagnostic criteria and confusing nomenclature, many cases of MF were likely misdiagnosed.
Diagnosis of MF improved in the late nineteenth century with innovation of histopathological techniques. Louis-Antoine Ranvier (1835–1922) demonstrated reticular lymphoid tissues in MF in 1875.^7^ In 1887, French dermatologist Jean Ferdinand Darier (1856−1938) described ‘Darier’s epidermal nests’, later renamed ‘petits nids cellulaires’.^10^
In 1885, Émile Charles Achille Vidal (1825–1893) and Louis-Anne-Jean Brocq (1856–1928) documented MF ‘d’emblee’, in which tumours were the first cutaneous manifestation – instead of being preceded by eruptions or infiltrations.^7^ In 1892, François Henri Hallopeau (1842–1919) and Ernest Henri Besnier (1831–1909) described erythroderma before the appearance of tumours.^7^ Pautrier microabscesses were credited to French dermatologist Lucien Marie Pautrier (1876–1959) in 1927, at the New York Society of Dermatology.^10–12^
French dermatologist Albert Sézary (1880–1956) published papers from 1938 to 1949 detailing a variant of MF with erythroderma and ‘cellules monstrueuses’, or ‘monster cells’, in the blood.^13^ In 1961, these clinical findings were collated together into ‘Sézary syndrome’ (SS) and the cutaneous presence of ‘mononuclear cells’ was identified.^14^
Marvin A. Lutzner (unknown dates) and Richard L. Edelson (1944–) coined the term and classification of cutaneous T-cell lymphoma (CTCL) in 1975, allowing for unity as the term encompassed both MF and SS.^15^ However, MF diagnosis is often still delayed due to similarities in clinical presentation to common conditions such as psoriasis, eczema and tinea infections.^16^
Advancement and evolution of diagnosing and understanding the aetiology of mycosis fungoides
The distinct yet progressive stages of MF, coupled with limited diagnostic techniques, led to further confusion about its origin. Potential triggers of MF such as environmental and/or occupational exposure to solvents, genetic malformations and infectious causes, such as truncated human T-cell lymphotropic virus (HTLV)-1, have been proposed and rejected.^17–21^
In the mid-twentieth century, the advent of flow cytometry and immunohistochemistry revolutionized MF diagnosis by identifying its T-cell origin and demonstrating antigen markers. In 1968, Lutzner used electron microscopy to comment on the irregularity of SS and MF cell nuclei, and the serpentine nature of SS nuclei, leading to the naming of Lutzner cells in the 1970s.^22,23^ Electron microscopy in 1980 was used to visualize the morphology of viruses such as HTLV, then thought to be involved in MF pathogenesis.^24^ In 1985 the Southern blot test demonstrated the monoclonality of MF cells, and by 1987 immunohistology had helped identify the presence of CD30 antigens on MF cells.^25,26^ The 1990s saw the polymerase chain reaction identify T-cell receptor arrangements specific to MF cells.^27^ However, the laboratory diagnosis of MF remains challenging.^28,29^
In MF, malignant T cells express cutaneous lymphocyte-associated antigen (CLA) and C-C chemokine receptors (CCRs). CLA^+^ T cells migrate to the skin through the help of cytokines, from sources such as keratinocytes.^30^ One of the important CCRs seen in MF is CCR4 and its ligand CCL17. They are involved in the apprehension of T cells and increasing prosurvival factors such as phosphatidylinositol-3-kinase, allowing these T cells to become resistant to apoptosis.^31^ MF cells can lack receptors such as CD7, CD5 and CD2, and malignant T cells congregate around Langerhans cells – seen as Pautrier microabscesses.^30^ Patients with MF have higher serum interleukin (IL)-7 and IL-15, which have roles in memory T-cell proliferation.^32^
In 2018, the World Health Organization and European Organisation for Research and Treatment of Cancer officially recognized four variants of MF (Table 2).^33^
How has mycosis fungoides management evolved?
As MF was confused as a variant of yaws/syphilis in the early nineteenth century, treatments may have included various herbal compounds, arsenic, atoxyl, sodium casodylate, potassium iodide and mercury.^37^
Fox’s nineteenth-century treatments for MF (as fibroma fungoides) included hygienic regimens, nutritious diets and nourishment, unspecified tonics and astringents applied directly to the sores.^9^
The twentieth and twenty-first centuries brought many advancements in the management of MF (Table 3). Many treatments listed in Table 3 are still used in 2025.^68^ Psoralen and ultraviolet A, total skin electron beam therapy and topical nitrogen mustards are still indicated in both early- and advanced-stage management, as monotherapy or in conjunction.^30^
In recent years monoclonal antibodies such as mogamulizumab have improved progression-free survival rates in MF.^69^ Mogamulizumab targets the CCR4 receptor, which – with its complementary CCL17 ligand – inhibits dermal migration of MF cells.^70^ Treatments for MF continue to improve, and although it is understood that MF is not an infectious disease, infections such as Staphylococcus aureus can promote MF.^71^
Summary
Reflection on the past two centuries from Alibert to mogamulizumab offers insight into the challenges that accompany the aetiology, diagnosis, classification and management of MF. While MF management has improved, diagnosis is often delayed due to clinician and patient confusion caused by the similarities in presentation with common benign dermatoses. Further patient and clinician education must be done to optimize patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alibert JL . Second genre: dermatoses contagieuses. In: Descriptions de la maladie de la peau observée à l'Hôpital Saint-Louis (Alibert JL, ed.). Paris: Baillière, 1837; 200–4.
- 2Radolf JD. Treponema. In: Medical Microbiology (Albrecht T, Baron S, Castro G et al, eds), 4th edn. The University of Texas Medical Branch at Galveston, 1996; chapter 36.21413263 · pubmed ↗
- 3Wallach D, Tilles G. Dermatology in France. Paris: Pierre Fabre Dermo-Cosmétique, 2002.
- 4Funk Warsaw of . Clinical studies on sarcomata of the skin. In: The British Journal of Dermatology (Morris M, Brooke HG, eds), vol. 1. H.K. Lewis, 1888-9; 143–156.
- 5Wilson E . On Diseases of the Skin. Philadelphia: Blanchard and Lea, 1852.
- 6Machado FM, Salvador RB. Why avoid naming diseases after animals? The case of “Molluscum contagiosum”. Trop Med Health 2024; 52:21.38448972 10.1186/s 41182-024-00586-4PMC 10916272 · doi ↗ · pubmed ↗
- 7Block JB, Edgcomb J, Eisen A et al Mycosis fungoides. Natural history and aspects of its relationship to other malignant lymphomas. Am J Med 1963; 34:228–35.13971694 10.1016/0002-9343(63)90056-1 · doi ↗ · pubmed ↗
- 8Sequeira JH . Discussion on mycosis fungoides. Proc R Soc Med 1914; 7:190–204.10.1177/0035915714007003110 PMC 200397719977643 · doi ↗ · pubmed ↗