Case Report: IGFBP5-ALK fusion-positive case of high-grade endometrial stromal sarcoma with response to ALK-targeted therapy
Weiwei Zhang, Jinkun Wu, Shujie Song, Yu Cheng

TL;DR
A rare case of high-grade endometrial stromal sarcoma with an IGFBP5-ALK fusion responded to ALK-targeted therapy, showing the potential of molecular profiling in rare cancers.
Contribution
First reported case of ALK-rearranged HG-ESS responding to an ALK inhibitor, expanding treatment options for this rare cancer.
Findings
An IGFBP5-ALK fusion was identified in a patient with high-grade endometrial stromal sarcoma.
The patient achieved a partial response to iruplinalkib, a second-generation ALK inhibitor.
Molecular profiling enabled the identification of a targetable alteration in a rare and aggressive cancer.
Abstract
High-grade endometrial stromal sarcoma (HG-ESS) is a very rare and aggressive uterine malignancy. Although recurrent genetic alterations such as YWHAE-NUTM2 fusions and BCOR alterations are well recognized, ALK rearrangements have not been previously reported in HG-ESS, and the efficacy of ALK inhibitors in this context remains unknown. A 51-year-old woman presented with irregular vaginal bleeding and underwent a total abdominal hysterectomy with bilateral salpingo-oophorectomy (TLH/BSO) and omentectomy. Histopathological and immunohistochemical analyses following hysterectomy confirmed HG-ESS. Postoperative imaging revealed rapid disease progression with pulmonary and pelvic metastases. After failure of gemcitabine/docetaxel chemotherapy, next-generation sequencing identified an IGFBP5-ALK fusion (breakpoint: IGFBP5 exon 1 – ALK exon 19), a TERT promoter mutation, and a homozygous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
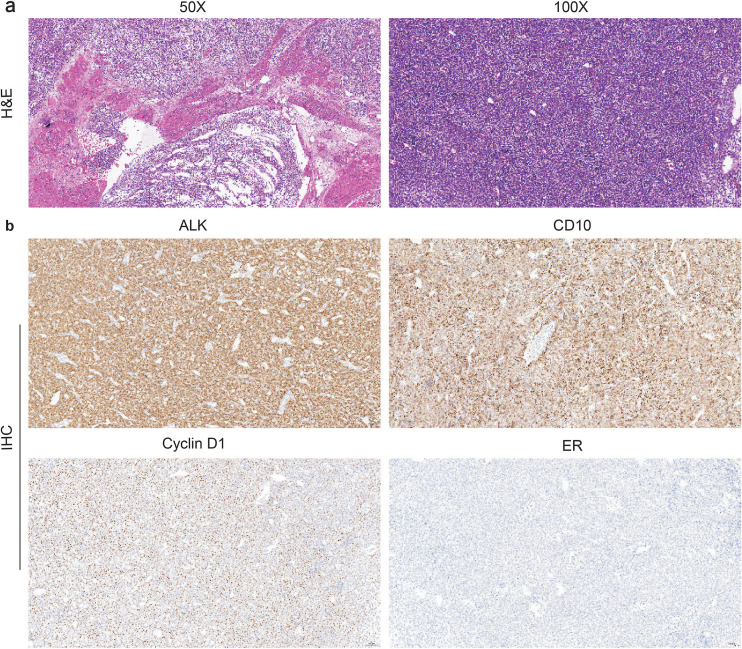 Figure 1
Figure 1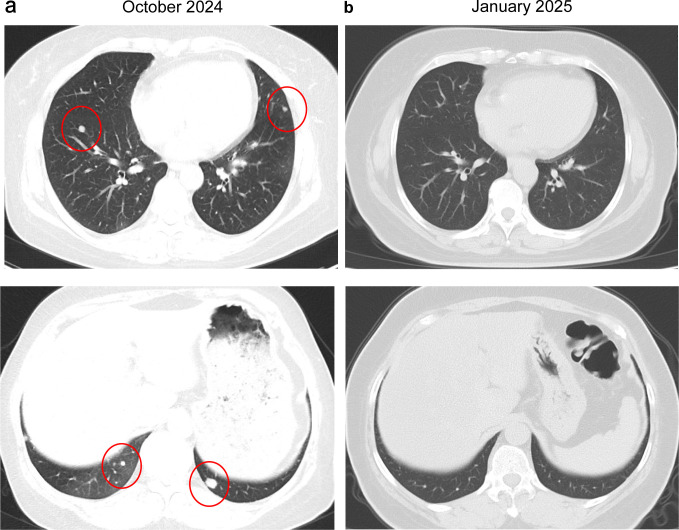 Figure 2
Figure 2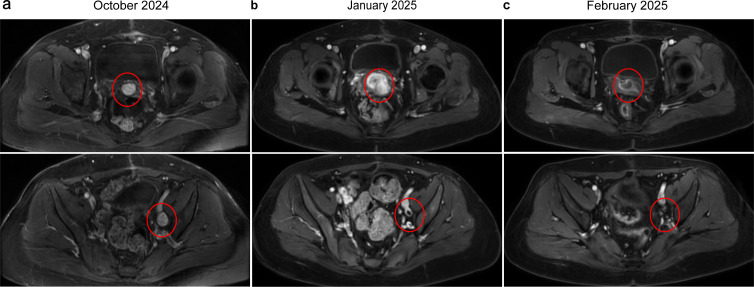 Figure 3
Figure 3| Microsatellite stable |
|---|
| Tumor Mutational Burden = 0 mutations/megabase |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Sarcoma Diagnosis and Treatment · Gastrointestinal Tumor Research and Treatment
Introduction
Endometrial stromal sarcomas (ESS) are rare mesenchymal malignancies accounting for less than 1% of all uterine malignancies and approximately 10% of uterine sarcomas (1). The World Health Organization (WHO) classifies ESS into low-grade endometrial stromal sarcoma (LG-ESS), high-grade endometrial stromal sarcoma (HG-ESS) and undifferentiated uterine sarcoma based on histopathological and molecular features (2). HG-ESS is a distinct entity that typically exhibits more aggressive behavior, characterized by high-grade cytological features, frequent recurrence, and metastasis (3). Molecularly, HG-ESS is heterogeneous, with recurrent genetic alterations including YWHAE-NUTM2 fusions, BCOR genetic alterations (rearrangements or internal tandem duplications), and many more being revealed as the next-generation sequencing (NGS) technique is being advanced (4, 5).
Conventional treatment for localized HG-ESS involves surgical resection, but management of advanced or metastatic disease remains challenging. Chemotherapy regimens, such as doxorubicin-based regimens or gemcitabine/docetaxel, are often used but with limited efficacy and significant toxicity. Given the poor outcomes with conventional chemotherapy, targeted therapies directed against specific molecular alterations represent a promising approach.
ALK inhibitors, such as crizotinib, alectinib, iruplinalkib and lorlatinib, have demonstrated remarkable efficacy in ALK-rearranged non-small cell lung cancer (NSCLC) (6–9). There is emerging evidence that ALK inhibitors may also be active in ALK-rearranged inflammatory myofibroblastic tumors (IMTs) and other sarcomas (10, 11). However, experience with ALK inhibitors in *ALK-*rearranged HG-ESS is limited. Iruplinalkib is a novel, potent second-generation ALK tyrosine kinase inhibitor approved by the Chinese National Medical Products Administration for ALK-positive NSCLC that has shown high overall response rates and improved outcomes compared with crizotinib in clinical trials (6). However, its use in ALK-rearranged sarcomas, particularly uterine sarcomas, has not been reported.
Herein, we present a case of metastatic HG-ESS harboring an IGFBP5-ALK fusion that demonstrated a dramatic and rapid response to iruplinalkib after progression on chemotherapy, highlighting the importance of molecular profiling and the therapeutic potential of ALK inhibitors in this rare malignancy.
Methods
Written consent was obtained from the patient and results from genetic profiling and clinical data can be published.
Histological analysis
Surgical resection specimens of uterine HG-ESS were fixed in 10% neutral buffered formalin, embedded in paraffin, and sectioned at a thickness of 5 μm. The sections were subsequently subjected to hematoxylin and eosin (H&E) staining and immunohistochemically evaluated using antibodies against ALK, CD10, H-caldesmon, Vimentin, ER, PR, P53, WT-1, CyclinD1, BRG1, INI-1, SMA, Desmin, CD117, S-100 and Ki67.
Next-generation sequencing analysis
Genomic profiling was performed on DNA extracted from the patient’s formalin-fixed, paraffin-embedded (FFPE) tumor tissue sample. Targeted NGS was carried out using the BGI-T7 platform and a 506-gene panel encompassing cancer-related genes. Raw sequencing data in BCL format were converted to FASTQ files using bcl2fastq (v2.19). Quality control was performed with Trimmomatic to remove low-quality reads and reads containing N bases. Clean reads were then aligned to the hg19 human reference genome using BWA. Subsequent variant calling and annotation were performed using bioinformatics pipelines to detect point mutations, insertions/deletions, copy number alterations, and gene fusions, as well as tumor mutation burden (TMB) and microsatellite instability (MSI) status.
Case description
A 51-year-old woman presented in September 2024 with irregular vaginal bleeding for one month. On 4 September 2024, she underwent a total abdominal hysterectomy with bilateral salpingo-oophorectomy (TLH/BSO) and omentectomy. The excised mass measured 15 × 11 × 9 cm and was located predominantly within the myometrium, with serosal penetration and lymphovascular invasion. No adnexal involvement was identified. Histopathological examination revealed a multinodular growth pattern with destructive invasion of the myometrium. The neoplastic cells were arranged in solid sheets, exhibited a high nuclear-to-cytoplasmic ratio, and possessed ovoid to plump spindle-shaped nuclei with prominent nucleoli; intravascular tumor emboli were also observed (Figure 1a). Immunohistochemically, the tumor cells demonstrate positivity for CD10, Cyclin D1, Vimentin and ALK (D5F3 clone), negativity for Desmin, CD117, ER, PR, and S-100, and a high proliferative index (Ki-67: 60%) (Figure 1b). These morphological and immunohistochemical features are consistent with a diagnosis of HG-ESS. According to the intraoperative findings and final postoperative pathology report from the hysterectomy specimen, the patient’s disease was classified as FIGO (2023) stage IVB.
Morphologic features and immunohistochemical stains of the HG-ESS samples. (a) Representative pictures of H&E staining. (b) IHC showing expression of ALK, CD10, Cyclin D1, and ER. HG-ESS, high-grade endometrial stromal sarcoma; H&E, hematoxylin and eosin; IHC, immunohistochemistry.
Approximately one month (October 25, 2024) after surgery, surveillance imaging confirmed disease progression. Chest CT demonstrated multiple bilateral pulmonary metastases (Figure 2a). Contrast-enhanced abdominal and pelvic MRI revealed a new metastatic pelvic mass posterior to the bladder and progressive enlargement of pelvic lymphadenopathy, suggestive of metastatic nodal involvement (Figure 3a). The patient was subsequently treated with docetaxel and gemcitabine with progression of disease after two cycles. Follow-up chest CT (January 13, 2025) demonstrated a reduction in pulmonary metastases (Figure 2b). However, contrast-enhanced abdominal and pelvic MRI showed shrinkage of pelvic lymph node metastases but a 90% enlargement of the pelvic metastatic lesion posterior to the bladder, indicating localized disease progression (Figures 3b). Chemotherapy-induced anemia and fatigue made further chemotherapy intolerable. NGS was performed using a targeted 506-gene panel. The results identified an IGFBP5-ALK gene fusion, a TERT promoter mutation, and a homozygous deletion at chromosome 9p21.3 affecting the CDKN2A/CDKN2B/MTAP gene cluster (Table 1). No canonical molecular alterations typically associated with HG-ESS, such as YWHAE-NUTM2 fusions or BCOR rearrangements/internal tandem duplications, were detected. Additionally, the tumor was found to be microsatellite stable and exhibited a TMB of 0 mutations per megabase.
Chest CT scans before and after first-line chemotherapy. (a) Pre-chemotherapy CT image (October 25, 2024) demonstrates multiple bilateral pulmonary metastases. (b) Post-chemotherapy CT scan (January 13, 2025) shows significant remission of the pulmonary metastases. CT, computed tomography.
Baseline and follow-up contrast-enhanced MRI of the abdomen and pelvis. (a) Pre-chemotherapy images (October 25, 2024) reveal a new metastatic pelvic mass posterior to the bladder along with pelvic lymphadenopathy. (b) After chemotherapy (January 13, 2025), the pelvic lymph node metastases show shrinkage; however, the metastatic lesion behind the bladder exhibits 90% enlargement. (c) Following the initiation of Iruplinalkib treatment, both the pelvic metastatic lesion and lymph node metastases demonstrate a significant radiographic response (February 24, 2025).
In December 2024, the patient was started on an oral ALK inhibitor, iruplinalkib, at a dose of 180 mg once daily after a 7-day lead-in period at 60 mg once daily. After 6 weeks of treatment, follow-up abdominal and pelvic MRI (February 24, 2025) showed significant regression of all lesions (both the pelvic metastatic lesion posterior to the bladder and pelvic lymph node metastases) (Figure 3c). A partial response was observed based on RECIST 1.1 criteria, with the sum of the longest diameters of target lesions decreasing by more than 47.2%. The most recent follow-up examination on August 6, 2025, revealed further shrinkage of the metastatic lesion behind the bladder on contrast-enhanced abdominal and pelvic MRI. Local therapy for the pelvic recurrence was evaluated and administered. Following discussion by our multidisciplinary tumor board, the patient received a course of definitive intensity-modulated radiotherapy (IMRT) to the pelvis, targeting the recurrent pelvic lesion and involved pelvic lymph nodes. The treatment was delivered from September 22 to October 29, 2025. The planning target volumes and prescribed doses were as follows: the gross tumor volume of nodal disease (GTVn) with a 5-mm margin (PGTVn) received 61.6 Gy in 28 fractions, and the clinical target volume (CTV) encompassing the pelvic nodal drainage areas with a 5-mm margin (PTV) received 50.4 Gy in 28 fractions. The patient continues to receive iruplinalkib and remains under routine clinical surveillance. The treatment was generally well-tolerated, with only grade 1 hypertriglyceridemia reported.
Discussion
In this case report, we present a case of a 51-year-old patient diagnosed with a HG-ESS and a very rare IGFBP5-ALK fusion. This report provides the first evidence of successful ALK-directed therapy in ALK-rearranged HG-ESS, achieving a significant and sustained response (>8 months and ongoing) following failure of conventional chemotherapy. This finding provides critical clinical evidence that ALK-rearranged HG-ESS represents a distinct molecular subtype for which targeted therapy with ALK inhibitors can be highly effective, mirroring the paradigm established in ALK-positive lung cancer.
ALK inhibitors, such as crizotinib, alectinib, iruplinalkib and lorlatinib, have demonstrated remarkable efficacy in ALK-rearranged NSCLC (6–9). There is a paucity of data on the incidence of ALK rearrangements and the role of ALK-directed tyrosine kinase inhibitors (TKIs) in the management of HG-ESS. Of note, the IGFBP5-ALK fusion identified in this HG-ESS (Table 1) differs from canonical NSCLC ALK rearrangements (e.g., EML4-ALK). NGS results also revealed the rearrangement breakpoint was between IGFBP5 exon 1 and ALK exon 19. The finding of this atypical IGFBP5-ALK breakpoint (the majority of ALK gene fusions occur at exon 20 of ALK) suggests that it may not be an isolated event, and highlights the great diversity of fusion events involving HG-ESS. The activity of ALK fusions may differ depending on the fusion partner and rearrangement breakpoints (12). Kyi et al. reported a patient with uterine inflammatory myofibroblastic tumor (IMT) positive for IGFBP5-ALK was shown to respond to crizotinib, however the rearrangement breakpoint was between IGFBP5 exon 1 and ALK exon 20 (13). Another patient with uterine IMT achieved a complete response to crizotinib, although the rearrangement breakpoint was unknown (14). This patient’s response to iruplinalkib suggests that the IGFBP5-ALK (I1; A19) fusion is likely ALK inhibitor–sensitive. ALK fusions are exceedingly rare in HG-ESS, and this case identifies a novel initial driver event as demonstrated by the presence of IGFBP5-ALK fusion in this patient’s hysterectomy specimen and a paucity of other genetic alterations in the NGS results.
The genomic landscape was further defined by a homozygous deletion at the CDKN2A/CDKN2B/MTAP locus, which is recurrent alterations in HG-ESS and is strongly associated with aggressive clinical behavior and poor prognosis (15, 16). A retrospective molecular analysis of NSCLC patients with ALK rearrangements revealed that CDKN2A/B copy number loss was the second most frequent concomitant genetic alteration after TP53 mutation (17). In addition to CDKN2A/B copy number loss, co-occurring TERT gene mutations have been identified in the study (17). Interestingly, this patient-who was found to have CDKN2A/B copy number loss-exhibited a low TMB (0 mutations/Mb), which is inconsistent with the study showing that co-occurrence of CDKN2A/B copy number loss is associated with a higher TMB (17), indicating CDKN2A/B loss might be a late event in tumor evolution of HG-ESS. The aggressive clinical course, marked by rapid postoperative recurrence, aligns with a separate study linking co-occurring CDKN2A/B loss to poorer progression-free and overall survival, underscoring its role in driving aggressive tumor biology in ALK-rearranged HG-ESS (18).
This case report describes a rare instance of HG-ESS harboring an IGFBP5 -ALK gene fusion—a genetic alteration with major therapeutic and prognostic implications. To our knowledge, this specific fusion has not been previously reported in HG-ESS and is more characteristically associated with uterine IMT (19, 20). The use of NGS for fusion detection and the patient’s marked response to ALK-targeted therapy represent significant strengths of this study. A limitation of our molecular analysis is that the sequencing data were processed using a customized bioinformatics pipeline designed to detect a predefined set of variants and fusions. Although this targeted approach ensures high sensitivity for known alterations, it may lack the breadth to identify novel or unexpected genetic events that could further inform the tumor’s biology or clinical behavior. As a single case report, our study has inherent limitations. The findings describe the experience of one patient and therefore cannot establish the general efficacy of ALK inhibitors in ALK-rearranged HG-ESS.
In conclusion, this case strengthens the rationale for molecular testing, including ALK immunohistochemistry and/or NGS, in patients with HG-ESS. The identification of an ALK rearrangement can transform the treatment strategy from ineffective chemotherapy to a highly effective, well-tolerated targeted therapy. Iruplinalkib, as demonstrated here, represents a promising treatment option for this molecularly defined subset of patients. Further clinical trials are warranted to formally establish the efficacy of ALK inhibitors in ALK-rearranged HG-ESS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D’Angelo E Prat J . Uterine sarcomas: a review. Gynecol. Oncol. (2010) 116:131–9. doi: 10.1016/j.ygyno.2009.09.023, PMID: 19853898 · doi ↗ · pubmed ↗
- 2Höhn AK Brambs CE Hiller GGR May D Schmoeckel E Horn L-C . 2020 WHO classification of female genital tumors. Geburtshilfe Frauenheilkd. (2021) 81:1145–53. doi: 10.1055/a-1545-4279, PMID: 34629493 PMC 8494521 · doi ↗ · pubmed ↗
- 3Lee C-H Mariño-Enriquez A Ou W Zhu M Ali RH Chiang S . The clinicopathologic features of YWHAE-FAM 22 endometrial stromal sarcomas: a histologically high-grade and clinically aggressive tumor. Am J Surg Pathol. (2012) 36:641–53. doi: 10.1097/PAS.0b 013e 31824 a 7b 1a, PMID: 22456610 · doi ↗ · pubmed ↗
- 4Chiang S Lee C-H Stewart CJR Oliva E Hoang LN Ali RH . BCOR is a robust diagnostic immunohistochemical marker of genetically diverse high-grade endometrial stromal sarcoma, including tumors exhibiting variant morphology. Mod Pathol Off J U. S. Can Acad Pathol Inc. (2017) 30:1251–61. doi: 10.1038/modpathol.2017.42, PMID: 28621321 PMC 5916794 · doi ↗ · pubmed ↗
- 5Mariño-Enriquez A Lauria A Przybyl J Ng TL Kowalewska M Debiec-Rychter M . BCOR internal tandem duplication in high-grade uterine sarcomas. Am J Surg Pathol. (2018) 42:335–41. doi: 10.1097/PAS.0000000000000993, PMID: 29200103 · doi ↗ · pubmed ↗
- 6Shi Y Chen J Yang R Wu H Wang Z Yang W . Iruplinalkib (WX-0593) versus crizotinib in ALK TKI-naive locally advanced or metastatic ALK-positive NSCLC: interim analysis of a randomized, open-label, phase 3 study (INSPIRE). J Thorac Oncol Off Publ. Int Assoc Study Lung Cancer. (2024) 19:912–27. doi: 10.1016/j.jtho.2024.01.013, PMID: 38280448 · doi ↗ · pubmed ↗
- 7Solomon BJ Mok T Kim D-W Wu Y-L Nakagawa K Mekhail T . First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med. (2014) 371:2167–77. doi: 10.1056/NEJ Moa 1408440, PMID: 25470694 · doi ↗ · pubmed ↗
- 8Peters S Camidge DR Shaw AT Gadgeel S Ahn JS Kim D-W . Alectinib versus crizotinib in untreated ALK-positive non-small-cell lung cancer. N Engl J Med. (2017) 377:829–38. doi: 10.1056/NEJ Moa 1704795, PMID: 28586279 · doi ↗ · pubmed ↗