Hashimoto’s thyroiditis is associated with reduced invasiveness in papillary thyroid carcinoma: a propensity score-matched retrospective cohort study
Rui Li, Xu Sun, Liai Hu, Zhiyuan Yu, Na Liu, Peiyu Li, Xudong Zhao, Wenquan Liang

TL;DR
This study finds that Hashimoto’s thyroiditis is linked to less aggressive papillary thyroid cancer, with reduced spread and fewer complications.
Contribution
The study demonstrates for the first time that Hashimoto’s thyroiditis is associated with reduced invasiveness in papillary thyroid carcinoma.
Findings
HT was associated with lower rates of extrathyroidal extension, multifocality, and bilateral carcinoma involvement.
HT was linked to increased pathological N0 stage tumors and reduced lymph node metastasis in specific patient groups.
Propensity score matching confirmed the association between HT and reduced cancer invasiveness.
Abstract
Papillary thyroid cancer (PTC), the predominant histologic subtype of thyroid cancer cases, has increased substantially over the past decades. In previous studies, Hashimoto’s thyroiditis (HT) exerts a paradoxical dual role in PTC. However, limited studies have specifically examined the association between HT and the invasion of PTC. In this retrospective study, 10329 PTC patients were selected, and the clinicopathological features were retrospectively analyzed. Propensity score matching (PSM) was employed to minimize confounding effects from baseline variables. Univariate analysis and multivariate analysis were performed using binary logistic regression to determine the predictive factor. Odds ratio (OR) and 95% confidence interval (CI) were calculated. Among 10329 PTC patients, 992 (9.6%) individuals were diagnosed with HT. Compared to the non-HT group, the HT group demonstrated…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
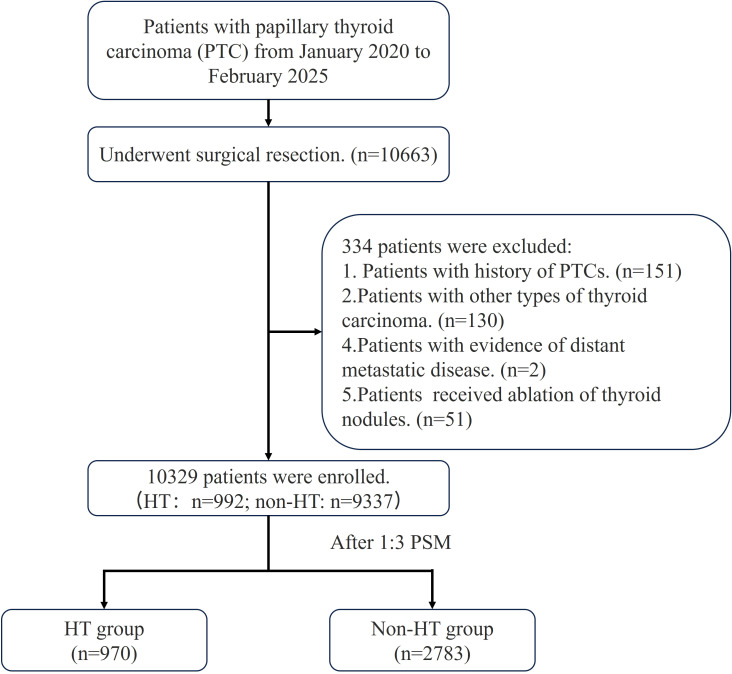 Figure 1
Figure 1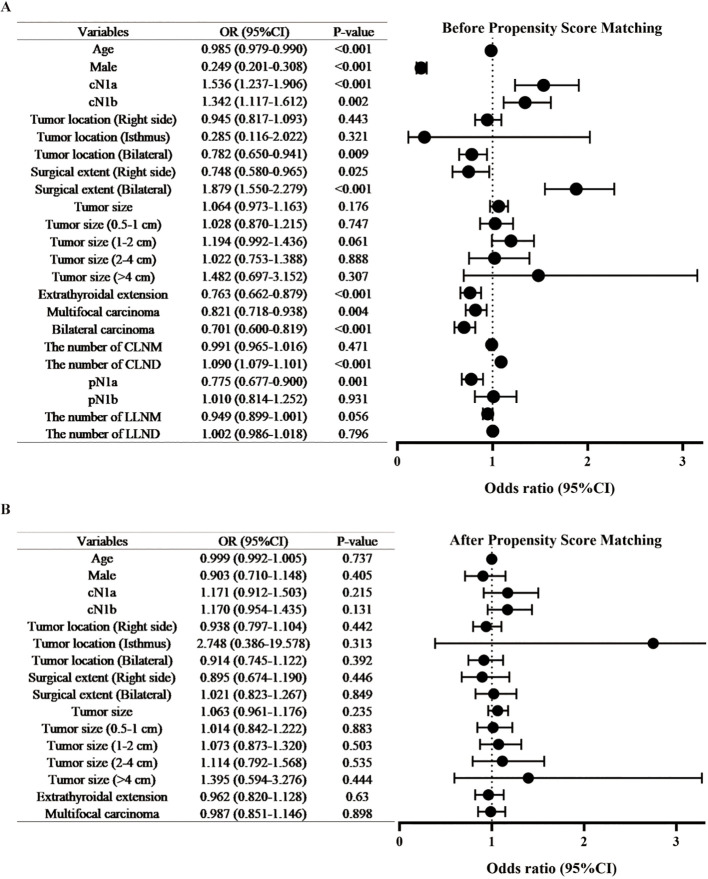 Figure 2
Figure 2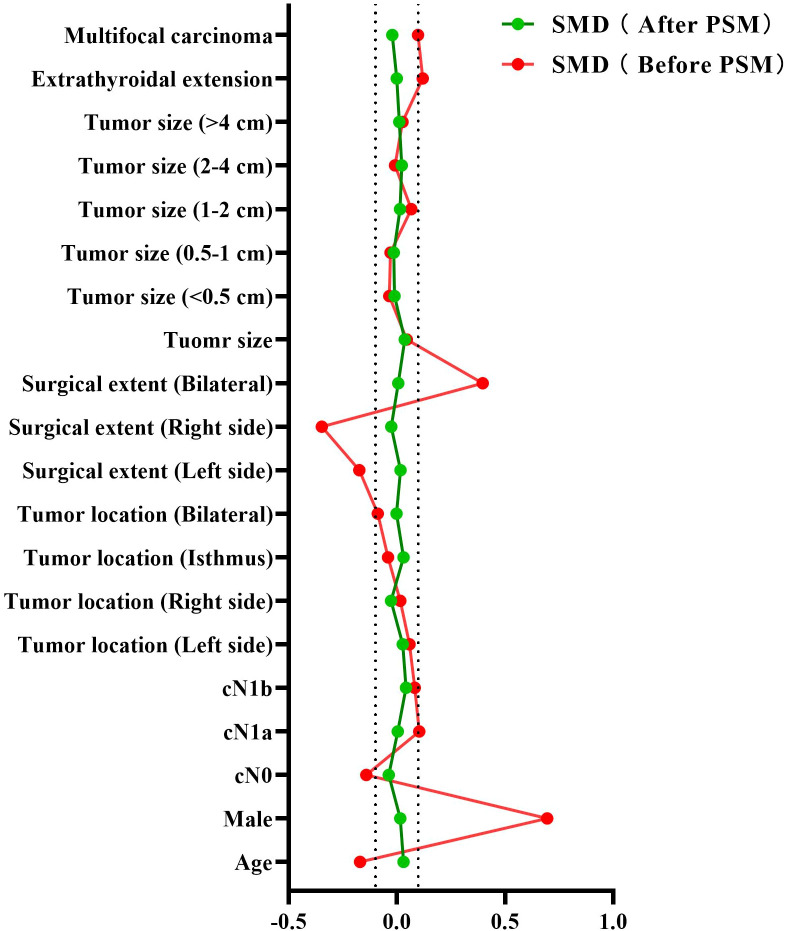 Figure 3
Figure 3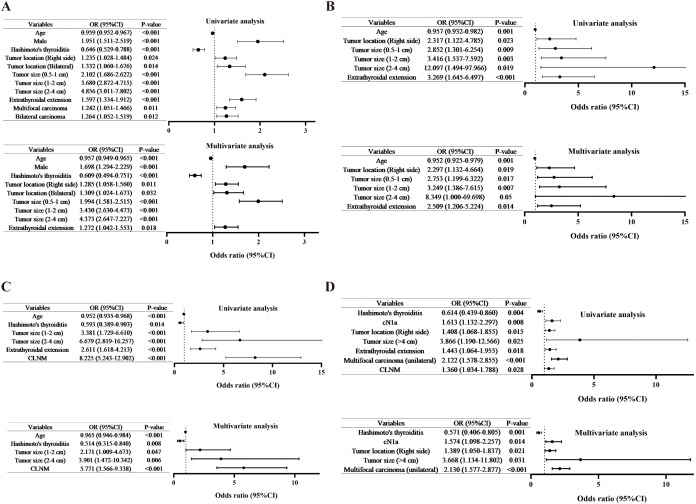 Figure 4
Figure 4| Characteristic | Patients (N = 10329) | OR (95%CI) | |||
|---|---|---|---|---|---|
| Total (n=10329) | HT absent (n = 9337) | HT present (n = 992) | |||
| Age | 43 (35-52) | 44 (35-52) | 41.5 (33-51) | <0.001 | 0.985 (0.979-0.990) |
| Gender, n (%) | <0.001 | 0.249 (0.201-0.308) | |||
| Female | 7376 (71.4) | 6482 (69.4) | 894 (90.1) | ||
| Male | 2953 (28.6) | 2855 (30.6) | 98 (9.9) | ||
| Clinical N stage, n (%) | <0.001 | ||||
| cN0 | 8160 (79.0) | 7432 (79.6) | 728 (73.4) | ||
| cN1a | 826 (8.0) | 718 (7.7) | 108 (10.9) | <0.001 | 1.536 (1.237-1.906) |
| cN1b | 1343 (13.0) | 1187 (12.7) | 156 (15.7) | 0.002 | 1.342 (1.117-1.612) |
| Clinical tumor location, n (%) | 0.051 | ||||
| Left side | 3746 (36.3) | 3361 (36.0) | 385 (38.8) | ||
| Right side | 4332 (41.9) | 3909 (41.9) | 423 (42.6) | 0.443 | 0.945 (0.817-1.093) |
| Isthmus | 38 (0.4) | 36 (0.4) | 2 (0.2) | 0.321 | 0.285 (0.116-2.022) |
| Bilateral | 2213 (21.4) | 2031 (21.8) | 182 (18.3) | 0.009 | 0.782 (0.650-0.941) |
| Surgical extent, n (%) | <0.001 | ||||
| Left side | 1926 (18.6) | 1794 (19.2) | 132 (13.3) | ||
| Right side | 2320 (22.5) | 2199 (23.6) | 121 (12.2) | 0.025 | 0.748 (0.580-0.965) |
| Bilateral | 6083 (58.9) | 5344 (57.2) | 739 (74.5) | <0.001 | 1.879 (1.550-2.279) |
| Tumor size | 0.8 (0.6-1.2) | 0.8 (0.5-1.2) | 0.8 (0.6-1.2) | 0.176 | 1.064 (0.973-1.163) |
| Tumor size, stratified, n (%) | 0.259 | ||||
| <0.5 cm | 2575 (24.9) | 2341 (25.1) | 234 (23.6) | ||
| 0.5-1 cm | 2583 (44.4) | 4156 (44.5) | 427 (43.0) | 0.747 | 1.028 (0.870-1.215) |
| 1-2 cm | 2505 (24.3) | 2238 (24.0) | 267 (26.9) | 0.061 | 1.194 (0.992-1.436) |
| 2-4 cm | 604 (5.8) | 548 (5.9) | 56 (5.6) | 0.888 | 1.022 (0.753-1.388) |
| >4 cm | 62 (0.6) | 54 (0.6) | 8 (0.8) | 0.307 | 1.482 (0.697-3.152) |
| Extrathyroidal extension, n (%) | <0.001 | 0.763 (0.662-0.879) | |||
| Absence | 2732 (26.4) | 2420 (25.9) | 312 (31.5) | ||
| Presence | 7597 (73.6) | 6917 (74.1) | 680 (68.5) | ||
| Multifocal carcinoma, n (%) | 0.004 | 0.821 (0.718-0.938) | |||
| Absence | 5777 (55.9) | 5179 (55.5) | 598 (60.3) | ||
| Presence | 4552 (44.1) | 4158 (44.5) | 394 (39.7) | ||
| Bilateral carcinoma, n (%) | <0.001 | 0.701 (0.600-0.819) | |||
| Absence | 7386 (71.5) | 6616 (70.9) | 770 (77.6) | ||
| Presence | 2943 (28.5) | 2721 (29.1) | 222 (22.4) | ||
| The number of CLNM | 0 (0-2) | 0 (0-2) | 0 (0-2) | 0.471 | 0.991 (0.965-1.016) |
| The number of CLND | 4 (2-8) | 4 (1-7) | 7 (3-12) | <0.001 | 1.090 (1.079-1.101) |
| Pathological N stage, n (%) | 0.003 | ||||
| N0 | 5942 (57.5) | 5331 (57.1) | 611 (61.6) | ||
| N1a | 3336 (32.3) | 3064 (32.8) | 272 (27.4) | 0.001 | 0.775 (0.677-0.900) |
| N1b | 1051 (10.2) | 942 (10.1) | 109 (11.0) | 0.931 | 1.010 (0.814-1.252) |
| Patients with LLND, n=1343 | |||||
| The number of LLNM | 2 (1-5) | 2 (1-5) | 2 (0-4) | 0.056 | 0.949 (0.899-1.001) |
| The number of LLND | 14 (9-20) | 13 (9-20) | 14 (10-21) | 0.796 | 1.002 (0.986-1.018) |
| Characteristic | Patients (N = 3753) | SMD | ||||
|---|---|---|---|---|---|---|
| Total (n=3753) | HT absent (n = 2783) | HT present (n = 970) | Before PSM | After PSM | ||
| Age | 42 (34-50) | 42 (34-50) | 42 (33-51) | 0.737 | -0.170 | 0.031 |
| Gender, n (%) | 0.405 | |||||
| Female | 3347 (89.2) | 2475 (88.9) | 872 (89.9) | 0.694 | 0.016 | |
| Male | 406 (10.8) | 308 (11.1) | 98 (10.1) | -0.694 | -0.016 | |
| Clinical N stage, n (%) | 0.187 | |||||
| cN0 | 2859 (76.2) | 2141 (76.9) | 718 (74.0) | -0.141 | -0.038 | |
| cN1a | 344 (9.2) | 247 (8.9) | 97 (10.0) | 0.215 | 0.103 | 0.004 |
| cN1b | 550 (14.7) | 395 (14.2) | 155 (16.0) | 0.131 | 0.083 | 0.042 |
| Clinical tumor location, n (%) | 0.540 | |||||
| Left side | 1413 (37.6) | 1036 (37.2) | 377 (38.9) | 0.058 | 0.027 | |
| Right side | 1607 (42.8) | 1198 (43.0) | 409 (42.2) | 0.442 | 0.016 | -0.027 |
| Isthmus | 4 (0.1) | 2 (0.1) | 2 (0.2) | 0.313 | -0.041 | 0.031 |
| Bilateral | 729 (19.4) | 547 (19.7) | 182 (18.8) | 0.392 | -0.088 | -0.002 |
| Surgical extent, n (%) | 0.507 | |||||
| Left side | 511 (13.6) | 379 (13.6) | 132 (13.6) | -0.174 | 0.017 | |
| Right side | 509 (13.6) | 388 (13.9) | 121 (12.5) | 0.446 | -0.347 | -0.026 |
| Bilateral | 2733 (72.8) | 2016 (72.4) | 717 (73.9) | 0.849 | 0.397 | 0.006 |
| Tumor size | 0.8 (0.6-1.2) | 0.8 (0.6-1.2) | 0.8 (0.6-1.2) | 0.235 | 0.046 | 0.036 |
| Tumor size, stratified, n (%) | 0.863 | |||||
| <0.5 cm | 908 (24.2) | 679 (24.4) | 229 (23.6) | -0.035 | -0.011 | |
| 0.5-1 cm | 1648 (43.9) | 1228 (44.1) | 420 (43.3) | 0.883 | -0.030 | -0.015 |
| 1-2 cm | 967 (25.8) | 710 (25.5) | 257 (26.5) | 0.503 | 0.066 | 0.014 |
| 2-4 cm | 205 (5.5) | 149 (5.4) | 56 (5.8) | 0.535 | -0.009 | 0.022 |
| >4 cm | 25 (0.7) | 17 (0.6) | 8 (0.8) | 0.444 | 0.026 | 0.011 |
| Extrathyroidal extension | 0.630 | |||||
| Absence | 1107 (29.5) | 815 (29.3) | 292 (30.1) | 0.119 | -0.0003 | |
| Presence | 2646 (70.5) | 1968 (70.7) | 678 (69.9) | -0.119 | 0.0003 | |
| Multifocal carcinoma | 0.898 | |||||
| Absence | 1107 (29.5) | 1647 (59.2) | 577 (59.5) | 0.098 | -0.021 | |
| Presence | 2646 (70.5) | 1136 (40.8) | 393 (40.5) | -0.098 | 0.021 | |
| pLN (-) N=2050 (%) | pLN (+) N=809 (%) | Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|---|---|
| OR (95%CI) | OR (95%CI) | |||||
| Age | 45 (36-53) | 38 (32-48) | <0.001 | 0.959 (0.952-0.967) | <0.001 | 0.957 (0.949-0.965) |
| Gender, n (%) | <0.001 | 1.951 (1.511-2.519) | <0.001 | 1.698 (1.294-2.229) | ||
| Female | 1891 (92.2) | 695 (85.9) | ||||
| Male | 159 (7.8) | 114 (14.1) | ||||
| HT, n (%) | <0.001 | 0.646 (0.529-0.788) | <0.001 | 0.609 (0.494-0.751) | ||
| Absence | 1490 (72.7) | 651 (80.5) | ||||
| Presence | 560 (27.3) | 158 (19.5) | ||||
| Clinical tumor location, n (%) | 0.037 | 0.05 | ||||
| Left side | 802 (39.1) | 273 (33.7) | ||||
| Right side | 880 (42.9) | 370 (45.7) | 0.024 | 1.235 (1.028-1.484) | 0.011 | 1.285 (1.058-1.560) |
| Isthmus | 2 (0.1) | 0 (0) | 0.999 | 0.999 | ||
| Bilateral | 366 (17.9) | 166 (20.5) | 0.014 | 1.332 (1.060-1.676) | 0.032 | 1.309 (1.024-1.673) |
| Surgical extent, n (%) | 0.091 | |||||
| Left side | 357 (17.4) | 119 (14.7) | ||||
| Right side | 335 (16.3) | 153 (18.9) | ||||
| Bilateral | 1358 (66.2) | 537 (66.4) | ||||
| Tumor size | <0.001 | <0.001 | ||||
| <0.5 cm | 685 (33.4) | 131 (16.2) | ||||
| 0.5-1 cm | 965 (47.1) | 388 (48.0) | <0.001 | 2.102 (1.686-2.622) | <0.001 | 1.994 (1.581-2.515) |
| 1-2 cm | 351 (17.1) | 247 (30.5) | <0.001 | 3.680 (2.872-4.715) | <0.001 | 3.430 (2.630-4.473) |
| 2-4 cm | 42 (2.0) | 39 (4.8) | <0.001 | 4.856 (3.011-7.802) | <0.001 | 4.373 (2.647-7.227) |
| >4 cm | 7 (0.3) | 4 (0.5) | 0.084 | 0.155 | ||
| Extrathyroidal extension, n (%) | <0.001 | 1.597 (1.334-1.912) | 0.018 | 1.272 (1.042-1.553) | ||
| Absence | 751 (36.6) | 215 (26.6) | ||||
| Presence | 1299 (63.4) | 594 (73.4) | ||||
| Multifocal carcinoma, n (%) | 0.011 | 1.242 (1.051-1.466) | 0.260 | |||
| Absence | 1304 (63.6) | 473 (58.5) | ||||
| Presence | 746 (36.4) | 336 (41.5) | ||||
| Bilateral carcinoma, n (%) | 0.012 | 1.264 (1.052-1.519) | 0.307 | |||
| Absence | 1562 (76.2) | 580 (71.7) | ||||
| Presence | 488 (23.8) | 229 (28.3) | ||||
| pLN (-) N=53 (%) | pLN (+) N=291 (%) | Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|---|---|
| OR (95%CI) | OR (95%CI) | |||||
| Age | 45 (34-55) | 38 (32-46) | 0.001 | 0.957 (0.932-0.982) | 0.001 | 0.952 (0.925-0.979) |
| Gender, n (%) | 0.152 | |||||
| Female | 47 (88.7) | 234 (80.4) | ||||
| Male | 6 (11.3) | 57 (19.6) | ||||
| HT, n (%) | 0.495 | |||||
| Absence | 36 (67.9) | 211 (72.5) | ||||
| Presence | 17 (32.1) | 80 (27.5) | ||||
| Clinical tumor location, n (%) | 0.058 | 0.128 | ||||
| Left side | 24 (45.3) | 98 (33.7) | ||||
| Right side | 13 (24.5) | 123 (42.3) | 0.023 | 2.317 (1.122-4.785) | 0.019 | 2.297 (1.132-4.664) |
| Isthmus | 1 (1.9) | 1 (0.3) | 0.326 | 0.900 | ||
| Bilateral | 15 (28.3) | 69 (23.7) | 0.744 | 0.487 | ||
| Surgical extent, n (%) | 0.188 | |||||
| Left side | 4 (7.5) | 24 (8.2) | ||||
| Right side | 0 (0) | 17 (5.8) | ||||
| Bilateral | 49 (92.5) | 250 (85.9) | ||||
| Tumor size | 0.006 | 0.027 | ||||
| <0.5 cm | 15 (28.3) | 31 (10.7) | ||||
| 0.5-1 cm | 19 (35.8) | 112 (38.5) | 0.009 | 2.852 (1.301-6.254) | 0.017 | 2.753 (1.199-6.322) |
| 1-2 cm | 17 (32.1) | 120 (41.2) | 0.003 | 3.416 (1.537-7.592) | 0.007 | 3.249 (1.386-7.615) |
| 2-4 cm | 1 (1.9) | 25 (8.6) | 0.019 | 12.097 (1.494-97.966) | 0.050 | 8.349 (1.000-69.698) |
| >4 cm | 1 (1.9) | 3 (1.0) | 0.755 | 0.662 | ||
| Extrathyroidal extension, n (%) | <0.001 | 3.269 (1.645-6.497) | 0.014 | 2.509 (1.206-5.224) | ||
| Absence | 16 (30.2) | 34 (11.7) | ||||
| Presence | 37 (69.8) | 257 (88.3) | ||||
| Multifocal carcinoma, n (%) | 0.498 | |||||
| Absence | 28 (52.8) | 139 (47.8) | ||||
| Presence | 25 (47.2) | 152 (52.2) | ||||
| Bilateral carcinoma, n (%) | 0.481 | |||||
| Absence | 31 (58.5) | 185 (63.6) | ||||
| Presence | 22 (41.5) | 106 (36.4) | ||||
| pLN (-) N=128 (%) | pLN (+) N=422 (%) | Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|---|---|
| OR (95%CI) | OR (95%CI) | |||||
| Age | 44 (34-52) | 36 (30-43) | <0.001 | 0.952 (0.935-0.968) | <0.001 | 0.965 (0.946-0.984) |
| Gender, n (%) | 0.488 | |||||
| Female | 114 (89.1) | 366 (86.7) | ||||
| Male | 14 (10.9) | 56 (13.3) | ||||
| HT, n (%) | 0.014 | 0.593 (0.389-0.903) | 0.008 | 0.514 (0.315-0.840) | ||
| Absence | 81 (63.3) | 314 (74.4) | ||||
| Presence | 47 (36.7) | 108 (25.6) | ||||
| Clinical tumor location, n (%) | 0.228 | |||||
| Left side | 58 (45.3) | 158 (37.4) | ||||
| Right side | 44 (34.4) | 177 (41.9) | ||||
| Isthmus | 0 (0) | 0 (0) | ||||
| Bilateral | 26 (20.3) | 87 (20.6) | ||||
| Tumor size | <0.001 | 0.004 | ||||
| <0.5 cm | 20 (15.6) | 26 (6.2) | ||||
| 0.5-1 cm | 55 (43.0) | 109 (25.8) | 0.215 | 0.855 | ||
| 1-2 cm | 43 (33.6) | 189 (44.8) | <0.001 | 3.381 (1.729-6.610) | 0.047 | 2.171 (1.009-4.673) |
| 2-4 cm | 10 (7.8) | 88 (20.9) | <0.001 | 6.679 (2.819-16.257) | 0.006 | 3.901 (1.472-10.342) |
| >4 cm | 0 (0) | 10 (2.4) | NA | NA | ||
| Extrathyroidal extension, n (%) | <0.001 | 2.611 (1.618-4.213) | 0.427 | |||
| Absence | 36 (28.1) | 55 (13.0) | ||||
| Presence | 92 (71.9) | 367 (87.0) | ||||
| Multifocal carcinoma, n (%) | 0.074 | |||||
| Absence | 74 (57.8) | 206 (48.8) | ||||
| Presence | 54 (42.2) | 216 (51.2) | ||||
| Bilateral carcinoma, n (%) | 0.970 | |||||
| Absence | 85 (66.4) | 281 (66.6) | ||||
| Presence | 43 (33.6) | 141 (33.4) | ||||
| CLNM, n (%) | <0.001 | 8.225 (5.243-12.902) | <0.001 | 5.771 (3.566-9.338) | ||
| Absence | 70 (54.7) | 54 (12.8) | ||||
| Presence | 58 (45.3) | 368 (87.2) | ||||
| Unilateral N=1318 (%) | Bilateral N=256 (%) | Univariate analysis | Multivariate analysis | |||
|---|---|---|---|---|---|---|
| OR (95%CI) | OR (95%CI) | |||||
| Age | 45 (36-52) | 43 (36-53) | 0.727 | |||
| Gender, n (%) | 0.913 | |||||
| Female | 1182 (89.7) | 229 (89.5) | ||||
| Male | 136 (10.3) | 27 (10.5) | ||||
| HT, n (%) | 0.004 | 0.614 (0.439-0.860) | 0.001 | 0.571 (0.406-0.805) | ||
| Absence | 958 (72.7) | 208 (81.3) | ||||
| Presence | 360 (27.3) | 48 (18.7) | ||||
| Clinical N stage, n (%) | 0.008 | 1.613 (1.132-2.297) | 0.014 | 1.574 (1.098-2.257) | ||
| cN0 | 1153 (87.5) | 208 (81.3) | ||||
| cN1a | 165 (12.5) | 48 (18.8) | ||||
| Clinical tumor location, n (%) | 0.015 | 1.408 (1.068-1.855) | 0.021 | 1.389 (1.050-1.837) | ||
| Left side | 598 (45.4) | 95 (37.1) | ||||
| Right side | 720 (54.6) | 161 (62.9) | ||||
| Tumor size | 0.101 | 0.134 | ||||
| <0.5 cm | 341 (25.9) | 63 (24.6) | ||||
| 0.5-1 cm | 587 (44.5) | 103 (40.2) | 0.767 | |||
| 1-2 cm | 323 (24.5) | 69 (27.0) | 0.447 | |||
| 2-4 cm | 60 (4.6) | 16 (6.3) | 0.241 | |||
| >4 cm | 7 (0.5) | 4 (2.0) | 0.025 | 3.866 (1.190-12.566) | 0.031 | 3.668 (1.134-11.802) |
| Extrathyroidal extension, n (%) | 0.018 | 1.443 (1.064-1.955) | 0.141 | |||
| Absence | 434 (32.9) | 65 (25.4) | ||||
| Presence | 884 (67.1) | 191 (74.6) | ||||
| Multifocal carcinoma (unilateral), n (%) | <0.001 | 2.122 (1.578-2.855) | <0.001 | 2.130 (1.577-2.877) | ||
| Absence | 1075(81.6) | 173 (67.6) | ||||
| Presence | 243 (18.4) | 83 (32.4) | ||||
| CLNM, n (%) | 0.028 | 1.360 (1.034-1.788) | 0.470 | |||
| Absence | 872 (66.2) | 151 (59.0) | ||||
| Presence | 446 (33.8) | 105 (41.0) | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Thyroid Disorders and Treatments · Thyroid and Parathyroid Surgery
Introduction
The incidence of thyroid cancer (TC) has increased substantially over the past decades, ranking as the seventh most prevalent cancer globally and the fifth most prevalent malignancy in females (1–3). Papillary thyroid cancer (PTC), the predominant histologic subtype of TC cases, represents the primary driver of this observed epidemiological rise (4). Updated in 2025, the American Thyroid Association (ATA) Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer further mandate precise risk stratification and personalized treatment planning for PTC patients (5).
Hashimoto’s thyroiditis (HT), one of the most prevalent autoimmune thyroid disorders, arises from complex interactions among genetic susceptibility, environmental triggers, and epigenetic modifications (6). It is serologically characterized by elevated anti-thyroglobulin (TgAb) and anti-thyroid peroxidase (TPOAb) antibodies. Histopathologically, HT manifests as lymphoplasmacytic infiltration, germinal center formation within lymphoid follicles, and progressive parenchymal atrophy (7). The relationship between HT and PTC remains contentious. On the one hand, chronic inflammation-driven oncogenic transformation and TSH-mediated follicular epithelial proliferation may promote PTC development (8, 9). Conversely, Anil et al. prospectively demonstrated no increased risk in HT patients with thyroid nodules (10). However, few studies have examined the association between HT and PTC invasion.
In this study, we systematically evaluated the association between clinicopathological characteristics and HT status in PTC patients. Propensity score matching (PSM) was employed to minimize confounding effects from baseline variables. Primary endpoints included lymph node metastasis status and incidence of bilateral carcinomas (initially diagnosed as unilateral disease preoperatively). Our comprehensive analysis provides clinically actionable evidence for refining risk-adapted management strategies in HT-associated PTC.
Materials and methods
Patients’ selection
Consecutive PTC patients who underwent surgical resection for treatment at the First Medical Center of the Chinese People’s Liberation Army (PLA) General Hospital from January 2020 to February 2025 were screened. Related patients meeting the following criteria were selected: (1) an obvious pathologic diagnosis of PTC; (2) primary cases without a history of thyroid tumors; (3) underwent surgical resection. The exclusion criteria were as follows: (1) patients with a history of thyroid tumors; (2) patients with other types of thyroid tumors, including follicular thyroid cancer, medullary thyroid cancer, and anaplastic thyroid cancer; (3) patients with evidence of distant metastatic disease; (4) patients who received ablation of thyroid nodules. This study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of the First Medical Center of the Chinese PLA General Hospital.
Data collection
The preoperative and postoperative clinicopathological features were retrospectively studied. Baseline variables, such as patient age and gender, were obtained from medical records. The clinical N stage and tumor location were determined from preoperative ultrasound and computed tomography scans. The surgical strategy for PTC, including thyroid lobectomy/total thyroidectomy, central compartment neck dissection, and lateral neck dissection (for cN1b patients), was determined by the surgeon based on preoperative staging. The presence of HT was diagnosed postoperatively by histopathological examination of paraffin-embedded sections, characterized by diffuse lymphoplasmacytic infiltration, and the presence of lymphoid follicles with reactive germinal centers in the background thyroid tissue, irrespective of preoperative antibody status (11). Tumor size, extrathyroidal extension, multifocal carcinoma, bilateral carcinoma, central lymph node metastasis (CLNM) count, central lymph node dissection (CLND) yield, pathological N stage (pN), lateral lymph node metastasis (LLNM) count, and lateral lymph node dissection (LLND) yield were determined through postoperative histopathological examination.
Statistical analysis
IBM SPSS Statistics 26.0 software (SPSS Inc, Chicago, IL, USA) and R software (ver. 4.2.1, R Development Core Team) were adopted for statistical analyses in this study. Numerical data with normal distribution were expressed as the mean ± standard deviation (SD), and numerical data without normal distribution were expressed as median (interquartile range, IQR). Categorical data are presented as absolute numbers and percentages. The MatchIt package was used to conduct the PSM, with a matching ratio of 1:3 between the HT and non-HT groups and a matching capacity of 0.02 (12). The standardized mean differences (SMD) of covariate balance before and after PSM were subsequently calculated. Univariate and multivariate analyses were performed using binary logistic regression to identify the predictive factors for CLNM, LLNM, and bilateral cancer. Odds ratio (OR) and 95% confidence interval (CI) were calculated. P-values were two-tailed, and P < 0.05 was considered statistically significant. Data visualization was performed using GraphPad Prism 8 Software.
Results
Patient selection and characteristics
Initially, a cohort of 10663 PTC patients who underwent thyroidectomy was included. Of these, 151 patients had a history of PTCs, 130 patients had other types of thyroid carcinoma, 2 patients had evidence of distant metastatic disease, and 51 patients had received ablation of thyroid nodules. After rigorous screening, 10329 patients were selected for further analysis, and 992 (9.6%) were diagnosed with HT (Figure 1). Compared with the non-HT group, the HT group exhibited a significantly younger age (p<0.001), greater female predominance (p<0.001), higher rates of clinical N1a and N1b disease (p<0.001), and more frequent bilateral thyroidectomy (p<0.001). Conversely, the HT group demonstrated lower rates of extrathyroidal extension (p<0.001), reduced multifocality (p=0.004), and decreased bilateral carcinoma involvement (p<0.001). Additionally, the HT group had higher numbers of CLND (p<0.001) and a greater proportion of pathological N0 stage tumors (p=0.003) (Table 1; Figure 2A).
The flow chart for patient selection PTC, papillary thyroid carcinoma; HT, Hashimoto’s thyroiditis; PSM, propensity score matching.
Comparison of clinical characteristics in papillary thyroid carcinoma patients with versus without Hashimoto’s thyroiditis before and after propensity score matching. (A) Pre-matching cohort; (B) Post-matching cohort. CLNM, central lymph node metastasis, CLND, central lymph node dissection, LLNM, lateral lymph node metastasis, LLND, lateral lymph node dissection.
Covariates, including age, gender, clinical N stage, clinical tumor location, surgical extent, tumor size, extrathyroidal extension, and multifocal carcinoma, were well-balanced through PSM. Following a 1:3 ratio PSM, the final cohort comprised 970 patients with HT and 2783 non-HT controls. All covariates demonstrated non-significant intergroup differences (P > 0.05; Figure 2B; Supplementary Table 1) with SMD below the 0.1 threshold (Table 2; Figure 3). The propensity score distribution and matching methodology are detailed in Supplementary Figures 2, 3.
The assessment of standardized mean differences (SMD) for covariate balance before and after propensity score matching (PSM).
HT independently associates with lower CLNM in cN0 PTC
After propensity score matching, 3753 patients were included in the final analysis. Among them, 2859 patients (76.2%) were clinically node-negative (cN0), of whom 809 (28.3%) had pathologically confirmed CLNM. Univariate analysis identified male gender (p<0.001; OR = 1.951), right-sided tumors (p=0.024; OR = 1.235), bilateral tumors (p=0.014; OR = 1.332), larger tumor size (p < 0.001), extrathyroidal extension (p<0.001; OR = 1.597), multifocal carcinoma (p=0.011; OR = 1.242), and bilateral carcinoma (p=0.012; OR = 1.264) as potential risk factors for CLNM. In contrast, increasing age (p<0.001; OR = 0.959) and HT (p < 0.001; OR = 0.646) showed potential protective effects. Furthermore, a multivariate analysis was conducted using binary logistic regression to identify the predictive factors for CLNM in cN0 PTC patients (Table 3; Figure 4A). Male gender (p<0.001; OR = 1.698), right-sided tumors (p=0.011; OR = 1.285), bilateral tumors (p=0.032; OR = 1.309), larger tumor size (p<0.001), and extrathyroidal extension (p=0.018; OR = 1.272) as significant risk factors for CLNM, while increasing age (p<0.001; OR = 0.957) and HT (p<0.001; OR = 0.609) were significant associated with lower CLNM rate in cN0 PTC.
Univariate and multivariate logistic regression analyses of risk factors for: (A) CLNM in cN0 PTC patients; (B) CLNM in cN1a PTC patients; (C) LLNM in cN1b PTC patients; (D) bilateral carcinoma identified in clinically unilateral PTC lesions. CLNM, central lymph node metastasis, LLNM, lateral lymph node metastasis, PTC, papillary thyroid cancer.
Among 344 cN1aPTC patients, 291 (84.6%) had pathologically confirmed CLNM. After univariate and multivariate analysis, right-sided tumors (p=0.019; OR = 2.297), larger tumor size (p=0.027), and extrathyroidal extension (p=0.014; OR = 2.509) were identified as significant risk factors for CLNM, while increasing age (p=0.001; OR = 0.952) was a significant protective factor (Table 4; Figure 4B).
HT independently associates with lower LLNM in CN1b PTC
Of the 550 cN1b PTC patients studied, 422 (76.7%) developed pathologically proven LLNM, among whom 54 (12.8%) presented with skip metastasis (Table 5; Figure 4C). Univariate analysis revealed significant associations for LLNM risk: tumor size 1–2 cm (p<0.001, OR = 3.381); tumor size 2–4 cm (p<0.001, OR = 6.679); extrathyroidal extension (p<0.001, OR = 2.611); and CLNM (p<0.001, OR = 8.225). Protective effects were observed for age (p<0.001, OR = 0.952) and HT (p=0.014, OR = 0.593). Multivariate analysis confirmed independent predictors: tumor size 1–2 cm (p=0.047, OR = 2.171); tumor size 2–4 cm (p=0.006, OR = 3.901); CLNM (p<0.001, OR = 5.771); with persistent protection from age (p<0.001, OR = 0.965).HT (p=0.008, OR = 0.514) was significantly associated with lower LLNM rate in cN1b PTC.
HT independently associates with reduced bilateral pathological involvement
In our cohort, 1574 patients had clinically unilateral lesions and underwent bilateral thyroidectomy, involving 1361 cN0 patients and 213 cN1a patients. Among them, 256 patients (16.2%) were pathologically confirmed to have bilateral thyroid carcinoma (Table 6; Figure 4D). Univariate analysis identified cN1a metastasis (p=0.008, OR = 1.613), right-sided tumors (p=0.015, OR = 1.408), tumor size >4cm (p=0.025, OR = 3.866), extrathyroidal extension (p=0.018, OR = 1.443), unilateral multifocal carcinoma (p<0.001, OR = 2.122), and CLNM (p=0.028, OR = 1.360) as potential risk factors for bilateral carcinoma, while HT showed a protective association (p=0.004, OR = 0.614). Multivariate analysis confirmed cN1a (p=0.014, OR = 1.574), right-sided location (p=0.021, OR = 1.389), tumor size >4cm (p=0.031, OR = 3.668), and unilateral multifocal carcinoma (p<0.001, OR = 2.130) as independent risk factors, with HT remaining a significant negative correlate (p=0.001, OR = 0.571).
Discussion
The imperative for precision risk stratification in PTC management is substantial, which is complicated by concomitant HT. This complexity arises not only from HT-induced diagnostic pitfalls in fine-needle aspiration biopsy (FNAB), but more critically from the paradoxical oncologic implications of HT itself (13, 14). In our cohort, HT coexisted with PTC in 9.6% of cases, demonstrating significant female predominance, consistent with prior epidemiological reports (11, 15–17). Crucially, the presence of HT prompted more aggressive preoperative management, evidenced by significantly higher rates of clinically suspected nodal metastases (cN1a and cN1b stage) and consequent performance of bilateral thyroidectomy. However, postoperative pathological assessment revealed a paradoxical protective association: HT was independently associated with reduced tumor invasiveness, with significantly lower frequencies of extrathyroidal extension, multifocality, and bilateral carcinoma involvement, and a higher proportion of pN0 stage tumors. After PSM to control for key confounders, HT consistently demonstrated an association with reduced PTC invasiveness. This was evidenced by significantly reduced CLNM rates in cN0 patients, lower incidence of LLNM in cN1b cases, and decreased bilateral tumor detection among preoperatively diagnosed unilateral tumors. These robust findings establish a significant association between HT and diminished invasive potential of PTC.
The protective association between HT and attenuated PTC invasiveness observed in our PSM analysis aligns with robust existing evidence. A multicenter cohort of 9210 PTC patients demonstrated HT’s negative correlation with aggressive features, including primary tumors larger than 4 cm, gross extrathyroidal extension, extranodal extension, and distant metastasis, and concurrently correlated with superior 10-year disease-specific and recurrence-free survival (11). This is further substantiated by a meta-analysis of 10648 cases across 38 studies, which found that HT co-occurrence significantly predicted reduced extrathyroidal extension, fewer positive lymph nodes, and improved long-term recurrence-free survival (17). Single-institutional data from 435 surgically treated PTC patients corroborated these findings, showing that PTC-HT cases had smaller tumor dimensions, less lymph node involvement, and earlier-stage disease than HT-negative counterparts (18). Collectively, these findings reinforce HT’s role in contributing to its less aggressive clinicopathological presentation in PTC.
Notwithstanding the predominant protective patterns, certain studies report conflicting associations between Hashimoto’s thyroiditis and papillary thyroid carcinoma behavior. Lee et al.’s aforementioned meta-analysis paradoxically identified HT as a risk factor for multifocal tumor involvement (17), a finding corroborated by Cappellacci et al. in their cohort of 839 PTC patients, in which the HT group demonstrated significantly higher multifocal rates (40.5% vs. 29.6%) (19). Although the latter study confirmed HT’s association with smaller tumor diameters, their multivariate analysis unexpectedly established HT as an independent risk factor for thyroid cancer development. This aligns with Apostolou et al.’s investigation of 3233 patients with multinodular thyroid disease, in which HT independently predicted malignant histopathology (20). Most strikingly, Chen et al.’s cohort demonstrated an 11.8-fold increased thyroid cancer risk in HT patients after full adjustment for demographic and comorbidity confounders (21). Danis et al. similarly reported that HT was associated with elevated PTC risk and consequently recommended more aggressive diagnostic approaches for HT patients with thyroid nodules (22). These contradictory observations suggest HT’s dual role in thyroid carcinogenesis, potentially promoting initial malignant transformation while simultaneously constraining progression through immunomodulatory mechanisms.
Advancements in research methodologies have progressively elucidated the molecular mechanisms underlying HT’s influence on PTC pathogenesis. In vitro experiments by Kim et al. demonstrated that HT attenuates PTC cell invasiveness by upregulated of E-cadherin and TGF-β, key regulators of epithelial-mesenchymal transition (23). Complementarily, Sun et al.’s metabolomic profiling of PTC patients revealed dysregulated aminoacyl-tRNA biosynthesis and serine/threonine metabolism in HT-associated tumors, suggesting metabolic reprogramming as a contributory mechanism (24). Multi-omics analyses further identified HT-specific genetic signatures via The Cancer Genome Atlas, including DMBT1, MET, FAM20A, SERPINA1, CD53, FCER1G, and TYROBP (25–28). Most notably, Ma et al.’s single-cell RNA sequencing identified HT-associated cell clusters that establish a TSH-suppressive microenvironment through interactions among mTE3, nTE0, and nTE2 subpopulations. This immunomodulatory network is functionally mediated by the MIF-(CD74+CXCR4) signaling axis, facilitating stromal-immune communication that may concurrently promote carcinogenesis yet restrain progression (29).
Notably, our study identified preoperative misdiagnosis of contralateral PTC in 16.2% of presumed unilateral cases, with HT emerging as a negative correlate of bilateral involvement, a finding that diverged from the prevailing literature. This contrasts with Lv et al.’s analysis of 1442 patients undergoing total thyroidectomy for unilateral PTC with benign-appearing contralateral nodules, where HT was classified as a risk factor alongside multifocality and capsular invasion (30). Similarly, Wang et al.’s meta-analysis (23% contralateral malignancy misdiagnosis rate) implicated HT as a significant risk predictor (31). Conversely, Wu et al. reported no association between HT and contralateral cancer in their cohort (28.9% misdiagnosis rate) (32). Our large-scale propensity-matched cohort demonstrates HT’s negative correlation against contralateral malignancies, aligning with its established inhibitory roles in protection against CLNM in cN0 patients and LLNM in cN1b patients.
While this study demonstrates an inverse association between HT and markers of PTC aggressiveness, several limitations warrant consideration. Firstly, the retrospective nature inherently introduces selection bias. Secondly, although PSM mitigated major confounders, residual bias persists from unmeasured factors. Besides, the cohort’s restriction to established PTC cases precludes assessment of HT’s impact on de novo carcinogenesis risk, which requires prospective comparison between HT and non-HT populations. Further, our histopathology-based HT diagnosis, while the gold-standard, limits clinical practice where serological criteria (TPOAb/TgAb) or ultrasound features guide preoperative decisions. This methodological discordance may partially explain divergent findings in the literature regarding HT’s dual roles. Finally, while the results may suggest a potentially protective immune microenvironment in HT, the hypothesis remains unproven and requires validation by future molecular and immunopathological studies.
Conclusion
This study demonstrates an inverse association between HT and markers of PTC aggressiveness, evidenced by reduced extrathyroidal extension, multifocality, and bilateral involvement alongside increased node-negative disease. After rigorous PSM, HT demonstrated inverse associations across key clinical scenarios: lowering CLNM rates in clinically node-negative patients, decreasing LLNM in cN1b subgroups, and reducing bilateral tumor detection among preoperatively diagnosed unilateral lesions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhou T Wang X Zhang J Zhou E Xu C Shen Y . Global burden of thyroid cancer from 1990 to 2021: a systematic analysis from the Global Burden of Disease Study 2021. J Hematol Oncol. (2024) 17:74. doi: 10.1186/s 13045-024-01593-y, PMID: 39192360 PMC 11348565 · doi ↗ · pubmed ↗
- 2Li M Dal Maso L Pizzato M Vaccarella S . Evolving epidemiological patterns of thyroid cancer and estimates of overdiagnosis in 2013–17 in 63 countries worldwide: a population-based study. Lancet Diabetes Endocrinol. (2024) 12:824–36. doi: 10.1016/S 2213-8587(24)00223-7, PMID: 39389067 · doi ↗ · pubmed ↗
- 3Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I . Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024) 74:229–63. doi: 10.3322/caac.21834, PMID: 38572751 · doi ↗ · pubmed ↗
- 4Filetti S Durante C Hartl D Leboulleux S Locati LD Newbold K . Electronic address: [email protected]. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. (2019) 30:1856–83. doi: 10.1093/annonc/mdz 400, PMID: 31549998 · doi ↗ · pubmed ↗
- 5Ringel MD Sosa JA Baloch Z Bischoff L Bloom G Brent GA . 2025 American thyroid association management guidelines for adult patients with differentiated thyroid cancer. Thyroid. (2025) 35:841–985. doi: 10.1177/10507256251363120, PMID: 40844370 PMC 13090833 · doi ↗ · pubmed ↗
- 6Ragusa F Fallahi P Elia G Gonnella D Paparo SR Giusti C . Hashimotos’ thyroiditis: Epidemiology, pathogenesis, clinic and therapy. Best Pract Res Clin Endocrinol Metab. (2019) 33:101367. doi: 10.1016/j.beem.2019.101367, PMID: 31812326 · doi ↗ · pubmed ↗
- 7Ralli M Angeletti D Fiore M D’Aguanno V Lambiase A Artico M . Hashimoto’s thyroiditis: An update on pathogenic mechanisms, diagnostic protocols, therapeutic strategies, and potential Malignant transformation. Autoimmun Rev. (2020) 19:102649. doi: 10.1016/j.autrev.2020.102649, PMID: 32805423 · doi ↗ · pubmed ↗
- 8Dailey M Lindsay S Skahen R . Relation of thyroid neoplasms to Hashimoto disease of the thyroid gland. AMA Arch Surg. (1955) 70:291–7. doi: 10.1001/archsurg.1955.01270080137023, PMID: 13227748 · doi ↗ · pubmed ↗