Preventing distal stent deflection using a sheath-assisted technique for malignant hilar biliary obstruction
Kenichi Haneda, Akihisa Kato, Yusaku Tomita, Yusuke Kito, Tadashi Toyohara, Yasuki Hori, Michihiro Yoshida

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
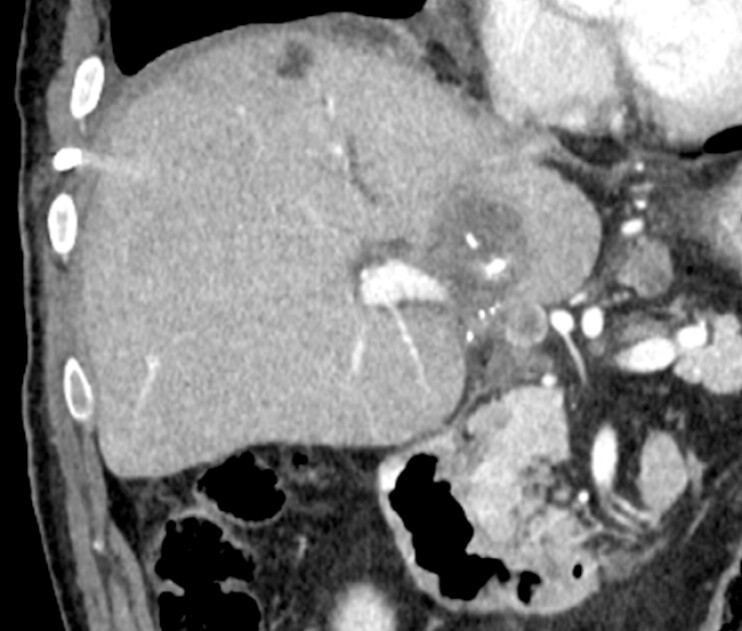 Fig. 1
Fig. 1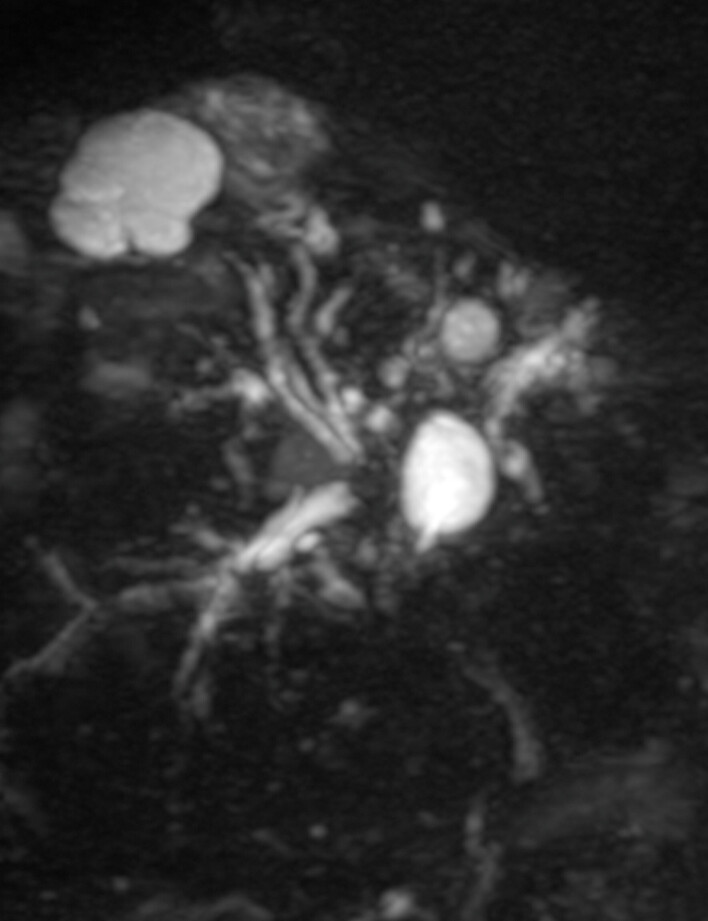 Fig. 2
Fig. 2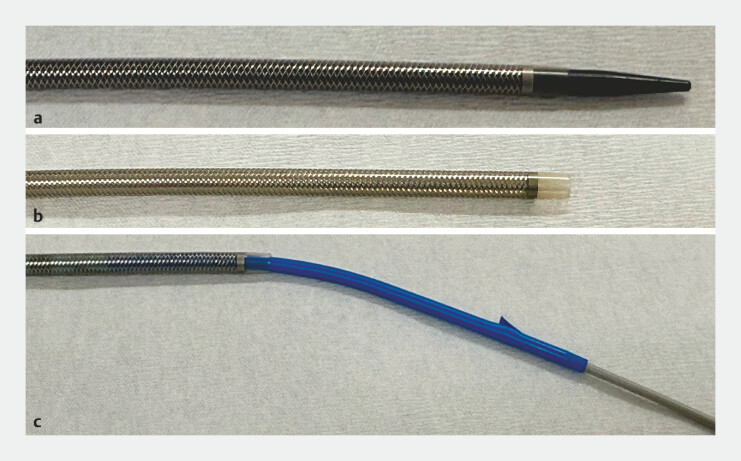 Fig. 3
Fig. 3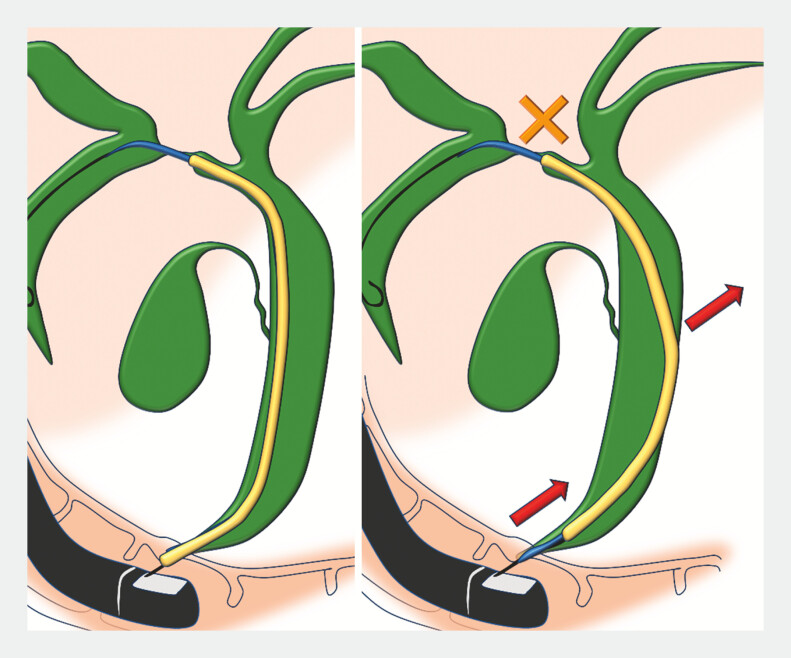 Fig. 4
Fig. 4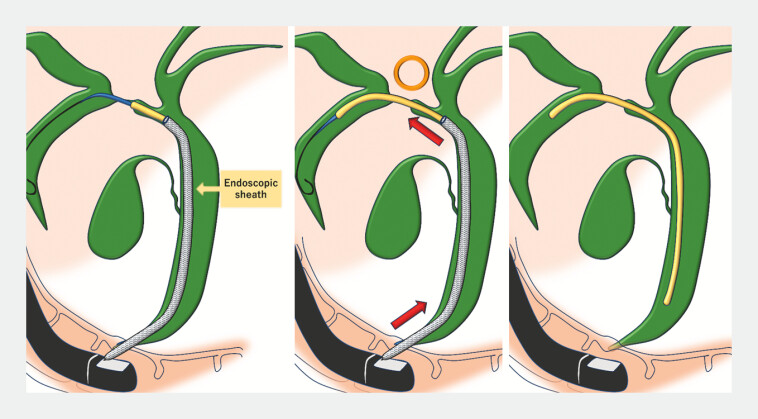 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Pediatric Hepatobiliary Diseases and Treatments
Endoscopic biliary stent placement for malignant hilar obstruction is a standard but often technically demanding procedure. Severe strictures can make the advancement of a stent difficult, particularly when multiple stents are required. Common strategies include exchanging for a stiffer guidewire or dilating the stricture with a dilator or balloon catheter 1 2 ; however, these may not always be successful. In particular, when inserting a plastic stent, stent deflection in the distal bile duct can dissipate the pushing force, preventing the stent from crossing the stricture.
We report a case in which an endoscopic sheath was used to prevent distal stent deflection and facilitate the successful plastic stent placement across a tight hilar stricture.
A 70-year-old man with a history of left hepatic lobectomy for hepatocellular carcinoma developed recurrent diseases in segment 1 of the liver ( Fig. 1 ). Magnetic resonance cholangiopancreatography demonstrated hilar bile duct obstruction due to the tumor in S1, resulting in dilatation of the anterior and posterior segmental ducts ( Fig. 2 ).
Contrast-enhanced CT revealed recurrent hepatocellular carcinoma in the liver S1. CT, computed tomography.
MRCP showed that the anterior and posterior segments of the bile duct were dilated and separated due to HCC in S1. HCC, hepatocellular carcinoma; MRCP, magnetic resonance cholangiopancreatography.
Endoscopic biliary stenting was performed. Guidewires were successfully placed in both segmental ducts, and a 7-Fr plastic inside stent was inserted into the posterior duct. However, attempts to place another 7-Fr plastic stent into the anterior duct failed because of distal stent deflection, even after exchanging the guidewire from 0.025-inch to 0.035-inch.
To overcome this, a large-caliber version of EndoSheather (Piolax, Inc., Yokohama, Japan, Fig. 3 ) 3 4 5 was advanced over the guidewire to the hilar bile duct. After removing the inner catheter, the 7-Fr plastic stent was inserted through the outer sheath. This approach prevented distal stent deflection and enabled the stent to cross the stricture smoothly for successful deployment ( Fig. 4 , Fig. 5 , Video 1 ).
a An appearance of the modified EndoSheather with an enlarged sheath diameter (an inner diameter of 8.4 Fr and an outer diameter of 10 Fr). b Outer sheath of EndoSheather. c The 7-Fr integrated plastic stent in the outer sheath of EndoSheather.
The 7-Fr plastic stent deflected in the distal bile duct, preventing it from transmitting enough forces to penetrate the stricture.
EndoSheather was advanced over the guidewire to the hilar bile duct. The sheath prevented the plastic stent from bending in the distal bile duct, allowing the force required to insert the 7-Fr stent to be transmitted sufficiently to the stricture, enabling the stent to be placed beyond the stricture.
The endoscopic sheath assisted in preventing the distal deflection of the plastic stent and enabled its smooth insertion across the tight hilar stricture.Video 1
When plastic stent deflection in the distal bile duct impedes insertion during hilar stenting, the use of an endoscopic sheath can provide effective axial support, reduce deflection, and facilitate smooth stent placement.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee TH Techincal Tips and Issues of biliary Stenting,Fosusing on Malignat Hilar Obstruction Clin Endosc 20134626026610.5946/ce.2013.46.3.26023767037 PMC 3678064 · doi ↗ · pubmed ↗
- 2Alfieri D Delogu C Mazza S The Role and Appropriate Selection of Guidewires in Biliopancreatic Endoscopy Medicina 20256191310.3390/medicina 61050913.40428871 PMC 12113394 · doi ↗ · pubmed ↗
- 3Kito Y Kato A Yoshida M Facile and secure deployment of plastic stent through an endoscopic tapered sheath for endoscopic ultrasound-guided drainage Endoscopy 202254 E 674E 67510.1055/a-1747-316235168275 · doi ↗ · pubmed ↗
- 4Matsumori T Uza N Okada H Innovative method for the diagnosis of bile duct lesions using a novel tapered-tip sheath system to facilitate biliary biopsies Gastrointest Endosc 2023984350036775209 10.1016/j.gie.2023.02.005 · doi ↗ · pubmed ↗
- 5Kato A Yoshida M Hori Y The novel technique of drainage stenting using a tapered sheath dilator in endoscopic ultrasound-guided biliary drainage DEN Open 20234 e 30310.1002/deo 2.30337873053 PMC 10590603 · doi ↗ · pubmed ↗