Necrotizing Soft Tissue Infection at a Self-Administered Subcutaneous Etanercept Injection Site in an Immunosuppressed Patient With Rheumatoid Arthritis: A Case Report
Seigo Tai, Masaaki Takemoto, Yoshihiro Yamamoto, Takaaki Nakano, Toshitaka Ito

TL;DR
A patient with rheumatoid arthritis developed a severe infection at the site of a self-administered injection, highlighting the need for prompt diagnosis and treatment in immunosuppressed individuals.
Contribution
This case report emphasizes the risk of necrotizing soft tissue infection at biologic injection sites in immunosuppressed patients and underscores the importance of early intervention.
Findings
A patient with rheumatoid arthritis developed necrotizing soft tissue infection at a subcutaneous etanercept injection site.
The infection was confirmed via surgical exploration and led to a diagnosis of streptococcal toxic shock syndrome.
Prompt surgical debridement and antimicrobial therapy were critical for the patient's survival without amputation.
Abstract
Necrotizing soft tissue infection (NSTI) is rapidly progressive and can be fatal; outcomes depend on early recognition and prompt surgical debridement. In immunocompromised patients, local findings and inflammatory responses may be atypical, increasing the risk of delayed diagnosis. Although injections breach the skin barrier, NSTI originating at injection sites can be overlooked as a benign injection-site reaction; procedure-associated NSTI has been reported to have poor outcomes. A woman in her 60s with rheumatoid arthritis was receiving methotrexate, tacrolimus, and prednisolone and had started self-administered subcutaneous etanercept injections four months earlier. One week prior to presentation, she developed discomfort and mild pain in the medial right thigh at her usual injection site, and, presuming it was a routine injection-site reaction, delayed medical attention. She…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1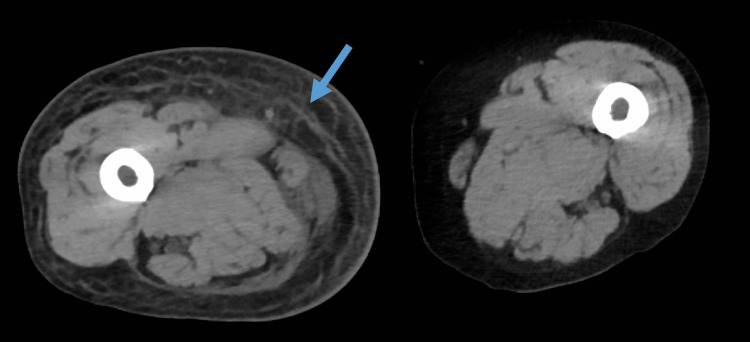 Figure 2
Figure 2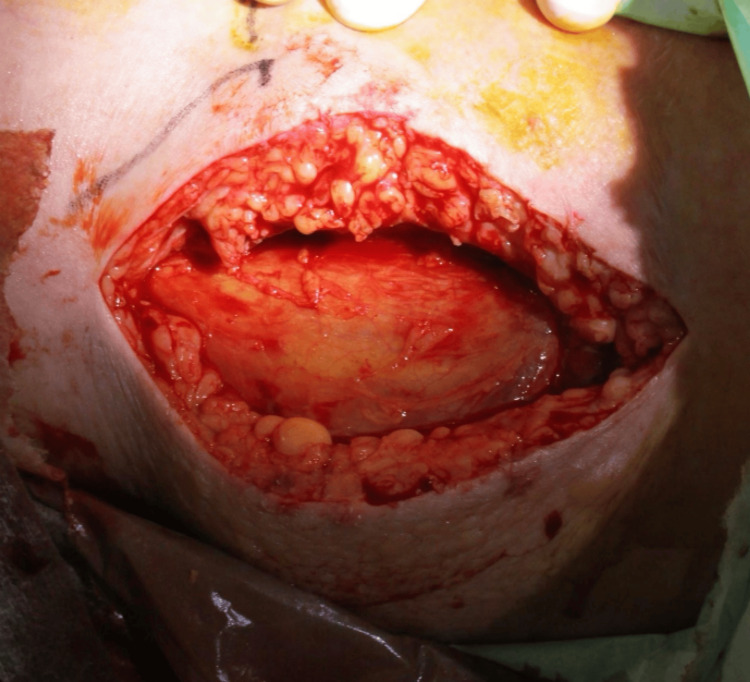 Figure 3
Figure 3| Parameter | Patient Value | Unit | Reference Range |
| WBC | 5,400 | /μL | 3,300–8,600 |
| Hemoglobin | 10.5 | g/dL | 11.6–14.8 |
| Platelets | 8.8×10^4 | /μL | 15.8–34.8×10^4 |
| Albumin | 1.600 | g/dL | 3.8–5.2 |
| Creatine kinase | 374 | U/L | 40–150 |
| Total bilirubin | 0.510 | mg/dL | 0.2–1.2 |
| AST | 29 | U/L | 10–40 |
| ALT | 18 | U/L | 7–40 |
| LDH | 264 | U/L | 120–230 |
| ALP | 54 | U/L | 106–322 |
| Amylase | 21 | U/L | 44–132 |
| Uric acid | 7.500 | mg/dL | 2.6–5.5 |
| BUN | 43.10 | mg/dL | 8–20 |
| Sodium | 142 | mEq/L | 138–145 |
| Potassium | 4.700 | mEq/L | 3.6–4.8 |
| Chloride | 104 | mEq/L | 101–108 |
| Glucose | 75 | mg/dL | 70–109 |
| Creatinine | 3.230 | mg/dL | 0.46–0.79 |
| eGFR | 12 | mL/min/1.73m² | ≥60 |
| CRP | 27.76 | mg/dL | 0–0.3 |
| pH | 7.453 | 7.35–7.45 | |
| PaCO2 | 19.50 | mmHg | 35–45 |
| PaO2 | 59.20 | mmHg | 80–100 |
| HCO3- | 13.50 | mEq/L | 22–26 |
| Base excess | -8.700 | mEq/L | -2–2 |
| Lactate | 2.500 | mmol/L | 0.5–2 |
| Procalcitonin | >100 | ng/mL | <0.05 |
| PT | 13.70 | sec | 10–13 |
| PT activity | 79 | % | 70–130 |
| PT-INR | 1.180 | 0.85–1.15 | |
| APTT | 32.70 | sec | 25–35 |
| FDP | 14.80 | µg/mL | 0–5 |
| D-dimer | 11.90 | µg/mL | 0–1 |
| Fibrinogen | 556 | mg/dL | 200–400 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsStreptococcal Infections and Treatments · Orthopedic Infections and Treatments · Dermatological and COVID-19 studies
Introduction
Necrotizing soft tissue infection (NSTI) is a life-threatening infection involving the skin, subcutaneous tissue, fascia, and sometimes muscle. Mortality remains substantial, and prognosis depends strongly on early diagnosis and prompt surgical debridement. Delayed recognition and delayed source control are consistently associated with worse outcomes [1-4].
The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score was developed to support risk stratification [5]; however, a subsequent systematic review and meta-analysis demonstrate limited sensitivity [6], and LRINEC should not be used to exclude NSTI. Because time to definitive surgery is a critical determinant of outcomes, early diagnosis and prompt debridement remain fundamental [7,8].
Portals of entry for NSTI are diverse, including minor trauma and surgical wounds; procedure-related entry points such as injections and other invasive procedures are also recognized [1-4,9]. Necrotizing soft tissue infections following injection therapy have been reported to have higher mortality and poorer outcomes compared with other entry mechanisms [9].
Biologic agents (e.g., anti-tumor necrosis factor (anti-TNF) agents) are effective for rheumatoid arthritis. Several case reports have described necrotizing fasciitis in patients receiving etanercept, highlighting that anti-TNF therapy can predispose to severe soft-tissue infections and that early recognition is critical [10-12]. Anti-TNF therapy is also associated with an increased risk of serious infections in rheumatoid arthritis [13-16]. Streptococcus pyogenes (group A Streptococcus) can cause fulminant NSTI, and clinical deterioration may be complicated by streptococcal toxic shock syndrome (STSS) [17,18].
We report a case of fulminant streptococcal NSTI developing at the site of self-administered subcutaneous etanercept injection in an immunosuppressed patient with rheumatoid arthritis, initially misattributed to an injection-site reaction and resulting in delayed presentation.
Case presentation
Patient information
A woman in her 60s with rheumatoid arthritis presented with fever and difficulty ambulating. Her past medical history included chronic kidney disease (stage 3), hypertension, dyslipidemia, and a cerebral aneurysm treated by endovascular embolization.
Medications and treatment history
She was receiving methotrexate 12 mg weekly, tacrolimus 1 mg daily, prednisolone 5 mg daily, and folic acid 5 mg daily. Self-administered subcutaneous etanercept 50 mg weekly was initiated approximately four months prior to presentation.
Social history
She reported long-term tobacco use (approximately 25-60 cigarettes/day for about 40 years) and regular alcohol consumption (approximately half a bottle of champagne nearly daily).
History of present illness
She typically injected etanercept into the medial thigh region. Approximately one week prior to admission, she noticed discomfort and mild pain in the medial aspect of the right thigh at her usual injection site. Assuming this was a routine injection-site reaction, she used over-the-counter medication and did not seek care. The pain progressively worsened, and she developed difficulty walking. One day prior to admission, she experienced decreased appetite, generalized fatigue, diarrhea, and mild abdominal pain. On the day of admission, persistent fever and worsening systemic symptoms prompted presentation to emergency services. At the referring facility, examination revealed erythema, swelling, and severe tenderness of the medial right thigh, and septic shock due to severe soft tissue infection was suspected; therefore, she was transferred to our hospital.
Initial assessment and vital signs
On arrival, she was alert (Japan Coma Scale I-1; Glasgow Coma Scale (GCS) E4V5M6). At the referring facility, she had hypotension and tachycardia (blood pressure (BP) 88/49 mmHg, heart rate (HR) 101 beats/minute). At our hospital arrival, her vital signs were respiratory rate 29 breaths/minute, saturation of peripheral oxygen (SpO₂) 97%, BP 110/58 mmHg (norepinephrine 0.2 µg/kg/minute), HR 108 beats/minute, temperature 37.3°C, and GCS E4V5M6.
Physical examination
The medial right thigh showed ill-defined erythema and swelling with focal vesiculation and purpuric changes without overt skin necrosis. Lesion dimensions were recorded as erythema/induration 10 cm × 15 cm, with a maximum bulla diameter of 3 cm. Pain was severe and clearly disproportionate to the skin findings (Figure 1).
Cutaneous findings on presentation.Ill-defined erythema and swelling on the medial aspect of the right thigh with focal vesiculation and purpuric changes, without overt skin necrosis. The patient reported severe pain disproportionate to the visible findings.
Laboratory findings
Initial laboratory values are summarized in Table 1. Coagulation studies suggested sepsis-associated coagulopathy. The LRINEC score was 8. Renal dysfunction was evident at presentation (blood urea nitrogen (BUN) 43.10 mg/dL, creatinine 3.230 mg/dL, estimated glomerular filtration rate (eGFR) 12 mL/minute/1.73 m²), consistent with acute kidney injury on chronic kidney disease.
Imaging
Contrast-enhanced CT demonstrated fascial thickening, increased attenuation of subcutaneous fat, fluid tracking along muscle bundles, and obscuration of intermuscular fat planes, consistent with deep soft-tissue inflammation centered at the fascial level (Figure 2). No gas was detected. Absence of gas did not exclude NSTI. Despite renal dysfunction, contrast-enhanced CT was performed after risk-benefit assessment because rapid delineation of deep soft-tissue involvement was considered critical for time-sensitive decision-making in septic shock.
CT on arrival at hospitalCT shows fascial thickening and deep soft-tissue edema with fluid tracking along fascial planes in the right medial thigh, without subcutaneous emphysema or gas formation.
Treatment and clinical course
Given septic shock and high clinical suspicion for NSTI, aggressive fluid resuscitation and continuous norepinephrine infusion were initiated. Empiric broad-spectrum antibiotics (meropenem, vancomycin, and clindamycin) were started in accordance with severe SSTI/NSTI management principles [2]. Emergency surgical exploration was performed for diagnostic confirmation and source control. A finger test under local anesthesia revealed gray, dishwater-like fluid. The fascia was friable and easily separated by blunt dissection with minimal bleeding, consistent with NSTI (Figure 3).
Intraoperative findings (finger test).Exploration reveals gray, dishwater-like fluid. The fascia is friable and easily separated by blunt dissection with minimal bleeding, consistent with NSTI. Necrotic subcutaneous tissue and fascia were debrided, and the wound was left open.
Extensive debridement of necrotic subcutaneous tissue and fascia was performed, the wound was irrigated, and left open. The patient was managed postoperatively in the intensive care unit.
Histopathology was not performed because emergent source control was prioritized. Group A β-hemolytic streptococcus (S. pyogenes) was isolated from wound and blood cultures. With hypotension and multiorgan dysfunction, the clinical picture was consistent with STSS. Molecular typing (e.g., emm typing) and laboratory assays proving toxin production were not performed; toxin production was not proven, and STSS was diagnosed clinically.
After susceptibility results became available, antimicrobial therapy was de-escalated to penicillin G plus clindamycin in line with guidance for invasive group A streptococcal infection/toxin-mediated disease. Residual necrosis was suspected clinically, and additional debridement was performed on hospital day 2. Thereafter, necrosis did not progress, and granulation tissue developed. Shock, coagulopathy, and acute kidney injury improved, and limb amputation was avoided. After prolonged wound management and rehabilitation, the patient was discharged ambulatory without assistance on hospital day 105.
Discussion
This case underscores three clinically important points: (i) NSTI may arise at injection sites, (ii) immunosuppression and injection-site reactions can delay recognition, and (iii) early surgical evaluation remains essential even when skin findings appear mild.
Portals of entry and injection-associated NSTI
NSTI typically follows disruption of the skin barrier, enabling pathogens to invade deep tissues and spread rapidly along fascial planes [1,3,4]. While minor trauma and surgical wounds are common portals of entry, procedure-related entry points such as injections, punctures, and other invasive procedures are recognized [1-4,9]. Injections breach the skin barrier and can theoretically introduce pathogens into subcutaneous tissue or near the fascia [3,9]. Procedure-associated NSTI has been reported to have poorer outcomes compared with other entry mechanisms [9]. In the present case, early symptoms localized to the patient’s usual etanercept injection site, supporting injection-site entry as the most plausible portal.
Comparison with prior etanercept-associated necrotizing fasciitis reports
Several case reports have described necrotizing fasciitis in patients receiving etanercept, including a dermatomyositis patient in whom MRI facilitated early diagnosis and timely debridement with a favorable outcome [10], a pediatric patient receiving etanercept and cyclosporine for macrophage activation syndrome [11], and a rheumatoid arthritis patient with shoulder involvement while on etanercept [12]. These reports collectively emphasize that anti-TNF therapy can predispose to severe soft-tissue infections and that early recognition is critical. Our case differs in that the suspected portal of entry was the self-injection site itself, the pathogen was S. pyogenes with a clinical course consistent with STSS, and the patient delayed seeking care for approximately one week after localized symptoms, culminating in septic shock requiring urgent surgical source control.
Injection-site selection, rotation, and patient education
The Japanese package insert for etanercept states that injection sites (thigh, abdomen, or upper arm) should be rotated and that patients should not self-administer until they receive proper training; importantly, it does not specify medial versus lateral thigh [19]. In this case, the exact reason for medial-thigh injections could not be verified retrospectively; however, family members consistently reported habitual injections into the same medial-thigh area. This uncertainty was acknowledged as a limitation. Nevertheless, this case suggests that clinicians should reinforce injection-site rotation and advise patients, especially those immunosuppressed, to seek prompt evaluation if injection-site pain is progressive or disproportionate, or if systemic symptoms develop.
Diagnostic strategy and the importance of early surgery
NSTI is primarily a clinical diagnosis [1-4]. Imaging can support diagnosis, but the absence of gas does not exclude NSTI [1-4,6]. LRINEC may support risk stratification but should not be used to rule out NSTI [5,6]. Because the patient had septic shock and pain disproportionate to examination findings, prompt surgical exploration was prioritized, and the finger test rapidly confirmed NSTI, enabling immediate debridement [1-4,7,8].
Streptococcal toxic shock syndrome and adjunctive therapy
In this case, S. pyogenes was isolated from wound and blood cultures, and the clinical picture was consistent with STSS [17,18]. Molecular typing (e.g., emm typing) and laboratory assays proving streptococcal toxin production were not performed; therefore, toxin production was not proven, and STSS was diagnosed clinically. Adjunctive intravenous immunoglobulin (IVIg) has been investigated for streptococcal toxin-mediated disease and NSTI; however, the evidence remains mixed [20,21].
Limitations
First, molecular typing and laboratory assays proving toxin production were not performed. Second, the exact rationale for medial-thigh injection and the content of injection-site education could not be fully verified retrospectively, although family members consistently reported habitual injections into the same area. Third, histopathology was not performed due to clinical urgency.Finally, because the patient was immunosuppressed with comorbidities, spontaneous skin infection unrelated to the injection cannot be completely excluded; however, the temporal and anatomic association makes the injection site the most plausible portal of entry.
Conclusions
NSTI can occur at injection sites and may be misinterpreted as a benign injection-site reaction, particularly in immunosuppressed patients. When pain is disproportionate to skin findings or systemic symptoms develop, clinicians should promptly evaluate for NSTI and prioritize early surgical consultation and exploration, even if the cutaneous appearance is subtle.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Necrotizing soft-tissue infections N Engl J Med Stevens DL Bryant AE 2253226537720172921167210.1056/NEJ Mra 1600673 · doi ↗ · pubmed ↗
- 2Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the infectious diseases society of America Clin Infect Dis Stevens DL Bisno AL Chambers HF 1471595920142494753010.1093/cid/ciu 296 · doi ↗ · pubmed ↗
- 3Necrotizing soft tissue infections: review and current concepts in treatment, systems of care, and outcomes Curr Probl Surg Hakkarainen TW Kopari NM Pham TN Evans HL 3443625120142506971310.1067/j.cpsurg.2014.06.001PMC 4199388 · doi ↗ · pubmed ↗
- 4Necrotizing soft tissue infections: a focused review of pathophysiology, diagnosis, operative management, antimicrobial therapy, and pediatrics Surg Infect (Larchmt) Tessier JM Sanders J Sartelli M 81932120203158434310.1089/sur.2019.219 · doi ↗ · pubmed ↗
- 5The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections Crit Care Med Wong CH Khin LW Heng KS Tan KC Low CO 153515413220041524109810.1097/01.ccm.0000129486.35458.7d · doi ↗ · pubmed ↗
- 6Necrotizing soft tissue infection: diagnostic accuracy of physical examination, imaging, and LRINEC score: a systematic review and meta-analysis Ann Surg Fernando SM Tran A Cheng W 586526920192967240510.1097/SLA.0000000000002774 · doi ↗ · pubmed ↗
- 7Influence of surgical treatment timing on mortality from necrotizing soft tissue infections requiring intensive care management Intensive Care Med Boyer A Vargas F Coste F 8478533520091909928810.1007/s 00134-008-1373-4 · doi ↗ · pubmed ↗
- 8Time is of the essence when treating necrotizing soft tissue infections: a systematic review and meta-analysis World J Emerg Surg Nawijn F Smeeing DP Houwert RM Leenen LP Hietbrink F 41520203192133010.1186/s 13017-019-0286-6PMC 6950871 · doi ↗ · pubmed ↗