Comparative Efficacy and Safety of Conventional Dresden, Transepithelial, and Accelerated Corneal Collagen Cross-Linking Protocols for Progressive Keratoconus: A Systematic Review
Bradley A Nordin

TL;DR
This study compares three corneal cross-linking methods for treating keratoconus, finding conventional methods most effective for long-term results.
Contribution
The study provides a systematic review comparing three CXL protocols for progressive keratoconus, highlighting their efficacy and safety profiles.
Findings
Conventional epi-off CXL showed the best long-term keratometric stabilization and visual acuity preservation.
Accelerated CXL protocols had similar short-term outcomes but less durability over time.
Transepithelial approaches with enhancements achieved results closer to conventional methods in some cases.
Abstract
Objective: The objective of this study was to compare the efficacy and safety of conventional Dresden, transepithelial (epithelium-on), and accelerated corneal collagen cross-linking (CXL) protocols for the treatment of progressive keratoconus. Methods: A systematic review of 84 studies was conducted in accordance with Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines. Study screening and data extraction were supported by AI-assisted tools with full manual verification. Extracted outcomes included keratometric stabilization, visual acuity, endothelial cell density (ECD), complications, corneal thickness changes, and biomechanical or surrogate markers. Results: Conventional epithelium-off (epi-off) CXL demonstrated the most consistent long-term keratometric stabilization and visual acuity preservation, with mean Kmax flattening of approximately…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
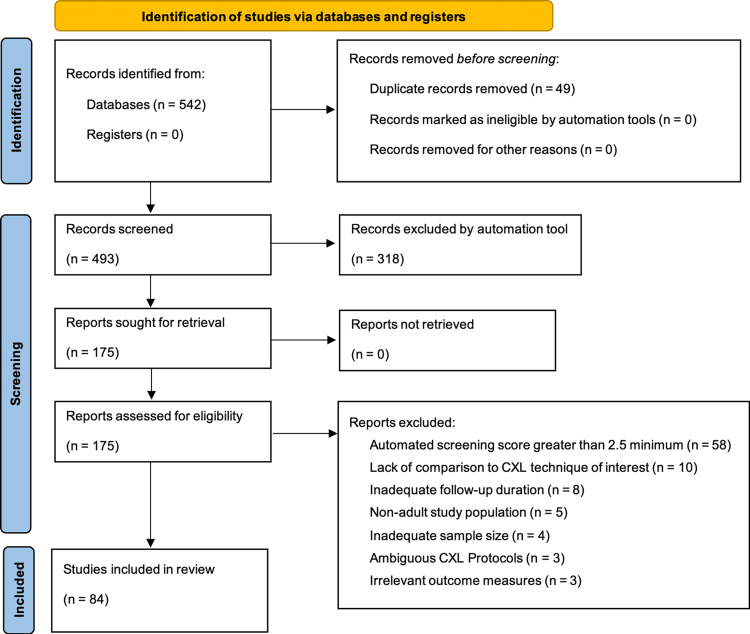 Figure 1
Figure 1| Database/Source | Search Query | Filters/Limits | Date Searched | Number of Results |
| PubMed/MEDLINE | (keratoconus[MeSH Terms] OR keratoconus[Title/Abstract] OR "keratoconus"[Title/Abstract]) AND ("Cross-Linking Reagents/therapeutic use"[MeSH Terms] OR "corneal collagen cross-linking"[Title/Abstract] OR "corneal cross-linking"[Title/Abstract] OR CXL[Title/Abstract] OR "cross linking"[Title/Abstract] OR "collagen cross linking"[Title/Abstract] OR "riboflavin UVA"[Title/Abstract] OR "riboflavin ultraviolet"[Title/Abstract] OR "photoactivated chromophore"[Title/Abstract]) AND (accelerated[Title/Abstract] OR conventional[Title/Abstract] OR Dresden[Title/Abstract] OR "transepithelial"[Title/Abstract] OR "epi-on"[Title/Abstract] OR "epi off"[Title/Abstract] OR "epithelium-off"[Title/Abstract] OR "epithelium-on"[Title/Abstract] OR pulsed[Title/Abstract] OR customized[Title/Abstract] OR iontophoresis[Title/Abstract] OR protocol*[Title/Abstract]) | Humans; Article types: Clinical Trial, Randomized Controlled Trial, Comparative Study, Observational Study; Publication dates: 2013 onward | January 1, 2013 to December 26, 2025 | 55 |
| Embase | #1: 'keratoconus'/exp OR keratoconus:ti,ab,kw #2: ('corneal collagen cross linking'/exp OR 'cross linking'/exp OR cxl:ti,ab,kw OR "corneal cross-linking":ti,ab,kw OR "collagen cross linking":ti,ab,kw OR "riboflavin UVA":ti,ab,kw OR "riboflavin ultraviolet":ti,ab,kw OR "photoactivated chromophore":ti,ab,kw) #3: (accelerated:ti,ab,kw OR conventional:ti,ab,kw OR dresden:ti,ab,kw OR transepithelial:ti,ab,kw OR "epi-on":ti,ab,kw OR "epi off":ti,ab,kw OR "epithelium-off":ti,ab,kw OR "epithelium-on":ti,ab,kw OR pulsed:ti,ab,kw OR customized:ti,ab,kw OR iontophoresis:ti,ab,kw OR protocol*:ti,ab,kw) #4: #1 AND #2 AND #3 | Humans; Evidence-based medicine (e.g., RCTs, controlled trials); Publication types: articles, conference abstracts; Dates: 2013 to December 2025 | January 1, 2013 to December 26, 2025 | 65 |
| Cochrane CENTRAL | Adapted queries emphasizing comparative terms and protocol variants (similar to PubMed and Embase) | Humans; Clinical trials and comparative studies; Publication dates: 2013 onward | January 1, 2013 to December 26, 2025 | 28 |
| Scopus | Adapted queries emphasizing comparative terms and protocol variants (similar to PubMed and Embase) | Humans; Articles, reviews, conference papers; Publication dates: 2013 onward | January 1, 2013 to December 26, 2025 | 43 |
|
Grey Literature ( | Keywords: "keratoconus cross-linking comparison" | No specific filters; Focused on ongoing and completed trials | January 1, 2013 to December 26, 2025 | 4 |
| Hand-Searching |
Reviewing reference lists of recent reviews and meta-analyses (e.g., Deshmukh et al., 2023 [ | N/A | N/A | 5 |
| Deduplication | N/A | N/A | N/A | 34 duplicates removed |
| Overall (Post-Deduplication) | Combined from all databases, exported in NBIB format | N/A | N/A | 166 unique sources |
| Protocol Group | Study | Study Design | CXL Protocol(s) | Sample Size | Follow-up Duration |
| Conventional Dresden / Standard Epi-off |
Alqudah et al., 2025 [ | Retrospective observational cohort | Dresden vs I-CXL | 107 patients | 1 year |
|
Bhattacharyya et al., 2019 [ | Prospective observational cohort | Dresden vs Control | 78 eyes | 6 months | |
|
Choi et al., 2017 [ | Prospective RCT | Dresden vs A-CXL | 28 eyes | 6 months | |
|
Danesh et al., 2021 [ | Prospective observational cohort | Dresden | 31 eyes | 1 year | |
|
Dervenis et al., 2020 [ | Retrospective case series | Dresden vs A-CXL | 59 eyes | 7 months | |
|
Elghobaier et al., 2025 [ | Retrospective case series | Dresden | 223 eyes | 3 years | |
|
Elmassry et al., 2021 [ | Retrospective observational cohort | Dresden vs TE-CXL vs A-CXL | 6120 eyes | 10 years | |
|
Ferdi et al., 2019 [ | Systematic review and meta-analysis | Epi-off (various) | 41 studies | 1 year | |
|
Ferdi et al. (Registry), 2023 [ | Observational registry study | Dresden | 162 eyes | 5 years | |
|
Gustafsson et al., 2025 [ | Prospective RCT (non-inferiority) | Iso vs Hypo-osmolar RF | 54 patients | 1 year | |
|
Hallahan et al., 2014 [ | Prospective RCT | Dresden | 51 eyes | 3 months | |
|
Kandel et al. (Registry), 2024 [ | Observational registry study | Dresden | 176 eyes | 5 years | |
|
Kymionis et al., 2016 [ | Prospective NRCT | Dresden vs cCXL | 32 eyes | 1 month | |
|
Lindstrom et al., 2021 [ | Economic modeling study | Dresden vs no CXL | Simulated cohort | Lifetime | |
|
Marafon et al., 2020 [ | Retrospective comparative cohort | Dresden vs A-CXL | 113 eyes | Mean 37.6 months | |
|
Padmanabhan et al., 2014 [ | Prospective NRCT | Dresden vs T-CAT+CXL | 27 eyes | Mean 7.7 months | |
|
Price et al., 2018 [ | Prospective interventional case series | Dresden vs A-CXL | 644 eyes | Median 3.5 years | |
|
Rosenblat et al., 2014 [ | Prospective NRCT | Standard vs hypotonic RF | 39 patients | 1 year | |
|
Rosenblat et al., 2016 [ | Prospective RCT | Standard vs hypotonic RF | 48 eyes | 1 year | |
|
Seyedian et al., 2015 [ | Prospective RCT | Dresden vs Control | 52 eyes | 1 year | |
|
Soeters et al., 2014 [ | Retrospective observational cohort | Dresden | 119 eyes | 1 year | |
|
Soeters et al., 2015 [ | Prospective RCT | Dresden vs TE-CXL | 39 eyes | 1 year | |
|
Strmeňová et al., 2015 [ | Retrospective observational cohort | Dresden | 88 eyes | 2 years | |
|
Vandevenne et al., 2023 [ | Prospective RCT (non-inferiority) | Dresden vs cCXL | 124 patients | 1 year | |
|
Wittig-Silva et al., 2014 [ | Prospective RCT | Dresden vs Control | 100 eyes | 3 years | |
| Transepithelial / Epi-on |
Al Fayez et al., 2015 [ | Prospective RCT | TE-CXL vs Dresden | 70 eyes | Mean 40 months |
|
APRICITY-A, 2023 [ | Prospective RCT | EpiSmart vs Sham | 400 subjects | 1 year | |
|
APRICITY-B, 2023 [ | Prospective RCT | EpiSmart vs Sham | 400 subjects | 1 year | |
|
Bikbova et al., 2016 [ | Prospective RCT | I-CXL vs Dresden | 149 eyes | 2 years | |
|
Caruso et al., 2016 [ | Prospective NRCT | TE-CXL | 25 eyes | 2 years | |
|
Caruso et al., 2021 [ | Prospective RCT | TA-CXL vs Dresden | NR | 2 years | |
|
Cassagne et al., 2014 [ | Prospective interventional case series | I-CXL | NR | NR | |
|
Cifariello et al., 2018 [ | Prospective RCT | TE-CXL vs Dresden | 40 eyes | 2 years | |
|
Epstein et al., 2022 [ | Prospective RCT | EpiSmart vs Control | 1922 subjects | 1 year | |
|
Ferrini et al., 2023 [ | Prospective observational cohort | TE-CXL vs Dresden | NR | NR | |
|
Gatzioufas et al., 2016 [ | Prospective observational cohort | TE-CXL | 26 eyes | 1 year | |
|
Lesniak et al., 2014 [ | Prospective RCT | TE-CXL | 30 eyes | 6 months | |
|
Lombardo et al., 2016 [ | Prospective RCT | I-CXL vs Dresden | 34 eyes | 6 months | |
|
Lombardo et al., 2017 [ | Prospective RCT | I-CXL vs Dresden | 34 eyes | 2 years | |
|
Mastropasqua et al., 2014 [ | Experimental laboratory (ex vivo) study | I-CXL vs TE-CXL vs Dresden | 10 donor corneas | Immediate (procedural) | |
|
Mazzotta et al., 2020 [ | Prospective interventional case series | ATE-CXL + O2 | 27 eyes | 6 months | |
|
Mazzotta et al., 2022 [ | Prospective NRCT | EFPL-M-TECXL + eRF | 40 eyes | 3 years | |
|
Rechichi et al., 2021 [ | Prospective NRCT | STARE-X | 100 eyes | ≥2 years | |
|
Shao et al., 2020 [ | Prospective observational cohort | TE-CXL | 46 eyes | 6 months | |
|
Shetty et al., 2014 [ | Retrospective case series | TE-CXL vs Dresden vs A-CXL (epi-off) | 2350 patients | ≥6 months | |
|
Smith et al., 2025 [ | Prospective RCT | Epioxa™ vs Sham | 312 eyes | 1 year | |
|
Stojanovic et al., 2014 [ | Prospective RCT | TE-CXL vs Epi-off | 40 eyes | Median 2 years | |
|
Stulting et al., 2018 [ | Prospective observational cohort | TE-CXL | 512 eyes | 2 years | |
|
Sun et al., 2018 [ | Prospective NRCT | TE-CXL + O2 | 26 eyes | 1 year | |
|
Vinciguerra et al., 2016 [ | Prospective NRCT | I-CXL vs Dresden | 34 eyes | 1 year | |
| Accelerated |
Abdel-Radi et al., 2023 [ | Prospective interventional case series | A-CXL | 45 eyes | 6 months |
|
Adapted Fluence Study, 2015 [ | Prospective RCT | A-CXL (7 vs 10 min) | 40 patients | 1 year | |
|
Ang et al., 2025 [ | Retrospective observational study | A-CXL | 70 eyes | 1 year | |
|
Asgari et al., 2018 [ | Prospective NRCT | A-CXL (18 vs 9 mW) | 60 eyes | 1 year | |
|
Avni-Zauberman et al., 2021 [ | Retrospective cohort | A-CXL vs Dresden | 124 eyes | 1 year | |
|
Badawi, 2021 [ | Retrospective cohort | A-CXL vs TE-CXL vs Dresden | 104 eyes | 1 year | |
|
Bunin et al., 2025 [ | Retrospective cohort | A-CXL vs A-CACXL | 62 eyes | 3 years | |
|
Dina et al., 2025 [ | NRCT (non-inferiority) | A-CXL vs Dresden | 41 eyes | 1 year | |
|
Dongre et al., 2024 [ | Retrospective case series | A-CXL vs Dresden | 964 eyes | 1 year | |
|
Gupta et al., 2024 [ | Retrospective comparative cohort | CACXL vs TE-CXL vs Dresden | 94 eyes | 1 year | |
|
Hagem et al., 2017 [ | Prospective RCT | A-CXL vs Dresden | 40 eyes | 1 year | |
|
Hagem et al., 2019 [ | Prospective RCT | A-CXL vs Dresden | 40 eyes | 2 years | |
|
Hashemi et al., 2015 [ | Prospective RCT | A-CXL vs Dresden | 62 eyes | 6 months | |
|
Hashemi et al., 2017 [ | Prospective interventional case series | A-CXL (18 vs 9 mW) | 62 eyes | 1 year | |
|
Herber et al., 2018 [ | Retrospective case series | A-CXL (beam profiles) | 45 eyes | 1 year | |
|
Iqbal et al., 2019 [ | Prospective NRCT | A-CXL+PRK vs Dresden | 125 eyes | 2 years | |
|
Ishii et al., 2022 [ | Prospective NRCT | ATE-CXL | 34 eyes | 3 years | |
|
Kandel et al., 2021 [ | Observational registry study | A-CXL vs Dresden | 684 eyes | 1 years | |
|
Karotkar et al., 2022 [ | Prospective RCT | pl-ACXL vs cl-ACXL | 100 eyes | 1 year | |
|
Kobashi et al., 2020 [ | Systematic review and meta-analysis | A-CXL vs Dresden | 6 RCTs | 1 year | |
|
Kortuem et al., 2017 [ | Retrospective comparative cohort | A-CXL vs Dresden | 286 eyes | 3 years | |
|
Males et al., 2018 [ | Retrospective comparative cohort | A-CXL vs Dresden | 42 eyes | ≥1 years | |
|
Manumuraleekrishna et al., 2024 [ | Prospective interventional case series | A-CXL (hypo- vs iso-osmolar RF) | 100 eyes | 1 year | |
|
Mazzotta et al., 2021 [ | Prospective NRCT | A-CXL | 156 eyes | 5 years | |
|
Ng et al., 2016 [ | Prospective NRCT | A-CXL vs Dresden | 26 eyes | Mean 13.9 months | |
|
Ozsaygili et al., 2021 [ | Retrospective comparative cohort | A-CXL | 64 eyes | 1 year | |
|
Recalde et al., 2019 [ | Prospective observational cohort | A-CXL | 22 eyes | 1 year | |
|
Rehnman et al., 2015 [ | Prospective RCT | CRXL vs Dresden | 60 eyes | 6 months | |
|
Sherif et al., 2016 [ | Prospective interventional case series | pl-ACXL | 20 eyes | Intraoperative | |
|
Šklebar et al., 2025 [ | Prospective observational cohort | A-CXL vs Dresden | 38 eyes | 9 months | |
|
Tomita et al., 2014 [ | Prospective NRCT | A-CXL vs Dresden | 48 eyes | 1 year | |
|
Turhan et al., 2019 [ | Prospective interventional case series | A-CXL | 52 eyes | NR | |
|
Turunç et al., 2025 [ | Prospective interventional case series | A-CXL | 113 eyes | 6 months | |
|
Yousif et al., 2023 [ | Retrospective comparative cohort | pl-ACXL vs cl-ACXL | 200 eyes | 1 year |
| Study | CXL Protocol | Kmax Change | Comparison | Timepoint | Stabilization Rate |
| Wittig-Silva et al., 2014 [ | Dresden | -1.03 ± 0.19 D (p < 0.001) | vs Control: +1.75 (p < 0.001) | 3 years | 100% vs 60% |
| Strmeňová et al., 2015 [ | Dresden | -0.97 D (p < 0.01) | NR | 2 years | 97% |
| Seyedian et al., 2015 [ | Dresden | -0.22 ± 0.6 D (p < 0.05) | vs Control: +0.41 D (p < 0.01) | 1 year | 88% vs 62% |
| Choi et al., 2017 [ | Dresden | -0.55 ± 0.89 D (p < 0.05) | vs A-CXL: no change (p < 0.05) | 6 months | 100% vs 100% |
| Bhattacharyya et al., 2019 [ | Dresden | -1.63 D (NS) | vs Control: increased (NS) | 6 months | 90% vs 0% |
| Ferdi et al. (Registry), 2023 [ | Dresden | -3.7 D (p < 0.001) | NR | 5 years | 93% |
| Stojanovic et al., 2014 [ | Dresden | -1.8 ± 1.4 D (p < 0.05) | vs A-CXL: +1.2 D (p < 0.05) | 5 years | 88% vs 74% |
| Study | TE-CXL Protocol | Kmax Change | Comparison | Timepoint | Stabilization Rate |
| Al Fayez et al., 2015 [ | Standard TE-CXL | +1.1 D (p < 0.05) | vs Dresden: -2.4 D (p < 0.0001) | 3 years | 41% vs 100% |
| Bikbova et al., 2016 [ | I-CXL | -0.9 D (p < 0.05) | vs Dresden: -1.8 D (p < 0.05) | 2 years | 100% vs 100% |
| Caruso et al., 2016 [ | Vitamin E-TPGS | -1.01 ± 1.22 D (p < 0.001) | NR | 2 years | 80% |
| Vinciguerra et al., 2016 [ | I-CXL | -0.31 ± 1.87 D (NS) | vs Dresden: -1.05 D (p < 0.01) | 1 year | NR |
| Stulting et al., 2018 [ | Enhanced RF | -0.48 D (p < 0.001) | NR | 2 years | 100% |
| Epstein et al., 2022 [ | EpiSmart | -0.76 D (p < 0.001) | NR | 1 year | 75% |
| Smith et al., 2025 [ | Epioxa™ + O2 | ≤ -1.0 D (p < 0.05) | vs sham: increased (p < 0.0001) | 1 year | NR |
| Study | A-CXL Protocol | Kmax Change | Comparison | Timepoint | Stabilization Rate |
|
Iqbal et al., 2019 [ | 30 mW/cm2 × 8 min pulsed + PRK | -2.40 ± 0.69 D (p < 0.001) | vs Dresden: -1.62 D (p < 0.05) | 1 year | 100% vs 100% |
|
Iqbal et al., 2019 [ | 30 mW/cm2 × 8 min pulsed + PRK | -2.23 ± 0.56 D (p < 0.001) | vs Dresden: -2.03 D (NS) | 2 years | 100% vs 100% |
|
Marafon et al., 2020 [ | 30 mW/cm2 × 8 min pulsed | -0.90 ± 3.12 D (p < 0.001) | vs Dresden: -0.68 D (NS) | 6 months | 96% vs 90% |
|
Badawi, 2021 [ | 10 mW/cm2 × 9 min | -1.87 ± 0.32 D (p < 0.0001) | vs Dresden: -2.74 D (NS) | 1 year | NR |
|
Badawi, 2021 [ | 10 mW/cm2 × 9 min | -1.87 ± 0.32 D (p < 0.0001) | vs TE-CXL: -0.36 D (p < 0.0001) | 1 year | NR |
|
Ishii et al., 2022 [ | ATE-CXL | –0.48 D (NS) | NR | 3 years | 88% |
|
Yousif et al., 2023 [ | pl-ACXL | -0.61 ± 3.73 D (NS) | vs cl-ACXL: -0.36 D (NS) | 1 year | NR |
|
Kandel et al., 2024 [ | 9 mW/cm2 × 10 min | +1.2 ± 2.7 (NS) | vs Dresden: -1.8 D (p < 0.05) | 5 years | 73% vs 88% |
| Study | Protocol | UDVA Change | CDVA/BCVA Change | Timepoint |
|
Wittig-Silva et al., 2014 [ | Dresden | -0.15 ± 0.06 logMAR (p < 0.01) | -0.09 ± 0.03 logMAR ( p < 0.01) | 3 years |
|
Strmeňová et al., 2015 [ | Dresden | NR | -0.048 logMAR (p < 0.01) | 2 years |
|
Bikbova et al., 2016 [ | I-CXL | NS | -0.07 logMAR (p < 0.05) | 2 years |
|
Bikbova et al., 2016 [ | Dresden | NS | -0.02 logMAR (p < 0.05) | 2 years |
|
Choi et al., 2017 [ | Dresden | -0.09 ± 0.09 (p < 0.01) | NR | 6 months |
|
Choi et al., 2017 [ | A-CXL | NS | NR | 6 months |
|
Stulting et al., 2018 [ | TE-CXL | -0.146 logMAR (p < 0.0001) | -0.108 logMAR (p < 0.0001) | 2 years |
|
Kobashi et al., 2020 [ | Dresden | NS | -0.02 logMAR (p < 0.0001) | 1 year |
|
Kobashi et al., 2020 [ | A-CXL | NS | NS | 1 year |
|
Ferdi et al. (Registry), 2023 [ | Dresden | -0.074 logMAR (p < 0.001) | NR | 1 year |
|
Ferdi et al. (Registry), 2023 [ | Dresden | -0.138 logMAR (p < 0.001) | NR | 5 years |
|
Kandel et al. (Registry), 2024 [ | Dresden | -0.204 logMAR (95% CI: -0.158 to -0.25) | -0.114 logMAR (95% CI: -0.07 to -0.156) | 5 years |
|
Kandel et al. (Registry), 2024 [ | A-CXL | -0.098 logMAR (95% CI: -0.032 to -0.164) | -0.004 logMAR (95% CI: -0.044 to +0.05) | 5 years |
| CXL Protocol | Mean Baseline ECD (Range) | Mean Follow-up ECD (Range) | Mean Change (Range) | Mean Follow-Up (Range) | Statistical Significance |
|
Dresden
[ | 2697.8 cells/mm2 (2690–2846) | 2682 cells/mm2 (2672–2805) | -15.8 cells/mm2 (-33 to +3) | 17.5 months (6–40) | No significant differences in ECD were observed within or between protocols (p > 0.05). |
|
TE-CXL
[ | 2663 cells/mm2 (2545–2750) | 2651.6 cells/mm2 (2532–2738) | -13.2 cells/mm2 (-100 to -12) | 21.1 months (12–40) | No significant differences in ECD were observed within or between protocols (p > 0.05). |
|
A-CXL
[ | 2772.3 cells/mm2 (2485–2854) | 2742.9 cells/mm2 (2468–2821) | -29.4 cells/mm2 (-15 to -12) | 11.5 months (6–24) | No significant differences in ECD were observed within or between protocols (p > 0.05). |
| Study | CXL Protocol | Haze Rate | Severity | Resolution |
|
Kortuem et al., 2017 [ | Dresden | 70.5% | Variable | Progressive improvement |
|
Kortuem et al., 2017 [ | A-CXL | 46.9% | Variable | Progressive improvement |
|
Bhattacharyya et al., 2019 [ | Dresden | All patients | Transient | Resolved by 3 months |
|
Ferdi et al. (Registry), 2023 [ | Dresden | 15.1% at 1 year | Variable | NR |
|
Ferdi et al. (Registry), 2023 [ | Dresden | 1.9% at 5 years | Variable | NR |
|
Kandel et al. (Registry), 2024 [ | Dresden | 3% at 5 years | Variable | Resolution in 77% |
|
Kandel et al. (Registry), 2024 [ | A-CXL | 2% at 5 years | Variable | Resolution in 88% |
|
Alqudah et al., 2025 [ | I-CXL | 7% | Mild | NR |
|
Alqudah et al., 2025 [ | Dresden | 54% mild | Mild | NR |
| Complication | Study | CXL Protocol | Rate | Notes |
| Corneal scarring |
Ferdi et al., 2019 [ | Dresden | 3.0% at 1 year | Declining over time |
| Endothelial cell loss |
Manumuraleekrishna et al., 2024 [ | A-CXL (Hypo-osmolar RF) | 1 eye | Significant ECD loss |
| Microbial keratitis |
Kandel et al. (Registry), 2024 [ | A-CXL | 1 case | Led to scarring |
| Need for re-treatment |
Ishii et al., 2022 [ | ATE-CXL | 2 eyes | Due to progression |
| Persistent epithelial defect |
Ferdi et al., 2019 [ | TE-CXL | 1.40% | Overall rate |
| Sterile infiltrates |
Kandel et al. (Registry), 2024 [ | A-CXL | Reported | Resolved with treatment |
| Stromal edema |
Bikbova et al., 2016 [ | Dresden | Observed | Resolved 6-12 months |
| Study | CXL Protocol | Baseline CCT/TCT | Change | Timepoint | Significance |
|
Wittig-Silva et al., 2014 [ | Dresden | NR | -19.52 ± 5.06 μm | 3 years | p < 0.001 |
|
Wittig-Silva et al., 2014 [ | Control | NR | -17.01 ± 3.63 μm | 3 years | p < 0.001 |
|
Vinciguerra et al., 2016 [ | Dresden | NR | -41.1 ± 35.3 μm | 1 year | p < 0.001 |
|
Vinciguerra et al., 2016 [ | I-CXL | NR | +1.0 ± 7.2 μm | 1 year | NS |
|
Kortuem et al., 2017 [ | Dresden | 457.75 μm | Progressive thinning | 3 years | p < 0.05 |
|
Kandel et al. (Registry), 2024 [ | Dresden | NR | -3.0 μm | 5 years | NS |
|
Kandel et al. (Registry), 2024 [ | A-CXL | NR | -11.8 μm | 5 years | p < 0.001 |
|
Ferdi et al. (Registry), 2023 [ | Dresden | 459 μm | -17 μm | 1 year | p < 0.001 |
|
Ferdi et al. (Registry), 2023 [ | Dresden | 459 μm | -11 μm | 5 years | p < 0.05 |
| Study | CXL Protocol | Demarcation Line Depth (via AS-OCT) | Comparison |
|
Bikbova et al., 2016 [ | I-CXL | 172 ± 16 μm | vs Dresden: 292 μm (p < 0.001) |
|
Dervenis et al., 2020 [ | Dresden | 322.50 μm | vs pl-ACXL: 319.95 μm (NS) |
|
Kobashi et al., 2020 [ | Dresden | Deeper than A-CXL (actual values NR) | WMD vs A-CXL: -102.25 μm 95% CI: -157.16 to -47.35 (p < 0.001) |
|
Mazzotta et al., 2022 [ | TE-EFPL ACXL | 282.6 ± 23.6 μm | NR |
|
Karotkar et al., 2022 [ | pl-ACXL | 251.13 ± 18.28 μm | vs cl-ACXL: 245.28 μm (NS) |
|
Manumuraleekrishna et al., 2024 [ | A-CXL (Iso-osmolar RF) | 252 μm | vs hypo-osmolar: 210 μm (NS) |
|
Dina et al., 2025 [ | A-CXL | 278.9 ± 31.71 μm | vs Dresden: 280.42 μm (NS) |
| Study | CXL Protocol | Parameter | Timepoint | Change | Significance |
|
Hashemi et al., 2015 [ | A-CXL vs Dresden | CH | 6 months | No significant difference | NS |
|
Hashemi et al., 2015 [ | A-CXL vs Dresden | CRF | 6 months | No significant difference | NS |
|
Shao et al., 2020 [ | TE-CXL | Brillouin shift | 6 months | +25 MHz cone region | p < 0.01 |
|
Karotkar et al., 2022 [ | cl-ACXL | DAI | 1 year | -0.19 mm (1.04→0.85) | p < 0.05 |
|
Karotkar et al., 2022 [ | pl-ACXL | DAI | 1 year | -0.28 mm (1.12→0.84) | p < 0.01 |
|
Manumuraleekrishna et al., 2024 [ | A-CXL (Iso- vs Hypo-osmolar RF) | CH | 1 year | Greater in iso-osmolar RF | p < 0.05 |
|
Manumuraleekrishna et al., 2024 [ | A-CXL (Iso- vs Hypo-osmolar RF) | CRF | 1 year | Greater in iso-osmolar RF | p < 0.05 |
|
Ang et al., 2025 [ | A-CXL | DAR | 6 months | -1.447 | p < 0.01 |
|
Ang et al., 2025 [ | A-CXL | IR | 6 months | -1.753 | p < 0.05 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCorneal surgery and disorders · Corneal Surgery and Treatments · Ocular Surface and Contact Lens
Introduction and background
Background on keratoconus
Keratoconus is a progressive, non-inflammatory ectatic disorder of the cornea characterized by thinning and conical protrusion, leading to irregular astigmatism, myopia, and significant visual impairment. Epidemiologically, the condition typically manifests in adolescence or early adulthood, with a pooled global prevalence of 289.1 cases per 100,000 individuals (0.29%) and an incidence of 4.0 per 100,000 person-years, affecting over 23.7 million people worldwide and showing increasing trends over time, particularly post-2020. The highest prevalence and incidence are observed in the 20-29 age group, with rates of 525.5 per 100,000 and 20.8 per 100,000 person-years, respectively, highlighting a substantial burden in young adults aged 18-39 years across diverse regions [1].
In terms of progression, keratoconus advances with increasing corneal steepening, as evidenced by an average increase in maximum keratometry (Kmax) of 0.7 diopters (D) over 12 months, with faster rates in younger patients and those with baseline Kmax steeper than 55 D. This natural history leads to deteriorating visual acuity and quality of life, often culminating in severe disability if unchecked [2]. The need for stabilization is critical to halt this progression, prevent the requirement for advanced interventions like corneal transplantation, and preserve vision, particularly in high-risk groups where closer monitoring and early treatments like corneal cross-linking are recommended [1,2].
Overview of CXL
Corneal collagen cross-linking (CXL) represents a paradigm shift in keratoconus management, as it is the only minimally invasive treatment proven to halt disease progression by biomechanically strengthening the corneal stroma [3]. The mechanism involves the application of riboflavin (vitamin B2) as a photosensitizer, followed by ultraviolet-A (UV-A) irradiation at a wavelength of 365-370 nm to generate reactive oxygen species, which induce covalent bonds between collagen fibrils and proteoglycans through oxidative (Type 1 and Type 2) and glycosylation pathways, thereby increasing corneal rigidity and resistance to ectatic changes [3,4]. Oxygen plays a crucial role in this photochemical reaction, and riboflavin also acts as an optical buffer by absorbing UV-A photons and converting them into harmless chemical energy (via photochemical excitation and subsequent reactive oxygen species generation), thereby protecting posterior ocular structures like the endothelium, lens, and retina from UV damage during the procedure [3,5].
The procedure evolved from foundational studies in the late 1990s at the University of Dresden, where initial experiments demonstrated increased corneal rigidity through riboflavin/UV-A-induced cross-links [5,6]. The conventional "Dresden protocol," an epithelium-off (epi-off) approach introduced in 2003, involves epithelial debridement of the central 7-9 mm cornea, riboflavin (0.1% in 20% dextran) instillation every two to five minutes for 30 minutes, and UV-A exposure at 3 mW/cm² for 30 minutes, delivering a total energy dose of 5.4 J/cm² [3,4]. Transepithelial (epi-on) protocols preserve the epithelium to minimize complications, enhancing riboflavin penetration via chemical enhancers (e.g., benzalkonium chloride), iontophoresis, or supplemental oxygen, offering reduced discomfort but potentially lower long-term efficacy compared to epi-off methods unless modified [3,7]. To address limitations such as prolonged treatment time, postoperative pain, and infection risk, accelerated variants emerged, increasing UV-A irradiance (e.g., 9-30 mW/cm²) while shortening duration (e.g., 9 mW/cm² for 10 minutes) based on Bunsen-Roscoe's law of reciprocity (which posits that the photochemical effect is proportional to light intensity × exposure time, applicable at moderate but not extreme intensities), though efficacy may vary due to reduced oxygen availability at higher intensities [3,5].
Rationale and scope
Despite numerous systematic reviews on CXL, significant gaps persist, including limited head-to-head comparisons of protocols, inconsistent long-term data beyond five years, and heterogeneous definitions of progression and stabilization [8,9]. Prior syntheses often focus on short-term efficacy in isolation, with fewer addressing comprehensive safety profiles or biomechanical surrogates in diverse patient groups, such as non-pediatric populations, where most studies emphasize pediatric cases due to aggressive progression [8,10]. With emerging 2025 data from registries and trials, an updated review is warranted to guide clinical decision-making amid evolving protocols [9].
The objective of this systematic review is to address the following PICO question: In patients with progressive keratoconus (P), what is the comparative efficacy and safety (O) of accelerated CXL, conventional (Dresden protocol) CXL, and transepithelial (epi-on) CXL (I) versus each other (C) with respect to stabilization of keratometric indices, improvement in uncorrected and corrected distance visual acuity, preservation of endothelial cell density, and rates of serious complications (haze, persistent edema, infection, scarring) at ≥12 months follow-up?
Review
Materials and methods
Study Design
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [11]. A qualitative synthesis was performed, including randomized controlled trials (RCTs), prospective and retrospective cohort studies, observational registries, and meta-analyses evaluating corneal CXL protocols in progressive keratoconus. Quantitative meta-analysis was not undertaken due to heterogeneity in study design, protocol parameters, outcome definitions, and follow-up durations.
The review protocol was not prospectively registered. This decision reflected the exploratory and comparative nature of evolving corneal cross-linking protocols and the absence of standardized long-term outcome frameworks across study designs.
Search Strategy
A comprehensive literature search was conducted between December 21 and December 26, 2025, using PubMed/MEDLINE (Medical Literature Analysis and Retrieval System Online), Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Scopus, and ClinicalTrials.gov. Searches covered studies published from January 1, 2013, through December 26, 2025. No initial language restrictions were applied; non-English articles were translated when relevant. Grey literature and reference lists of recent systematic reviews and meta-analyses (e.g., Deshmukh et al., 2023 [9]; Kobashi et al., 2020 [12]) were manually screened to identify additional eligible studies.
Detailed database-specific search strategies and yields are presented in Table 1.
Study Selection
Study selection was conducted in two stages: title and abstract screening followed by full-text eligibility assessment. Predefined inclusion and exclusion criteria, including population characteristics, study design, intervention protocols, comparators, outcome measures, and minimum follow-up duration, are detailed in Appendix A.
AI-assisted tools were used as an adjunct during the title and abstract screening phase to support organization and prioritization of records potentially meeting eligibility criteria. AI outputs were used solely to enhance screening efficiency and did not independently determine study eligibility. All records identified as potentially relevant underwent direct manual review.
Full-text articles were assessed by the author for eligibility using the predefined criteria, and all final inclusion and exclusion decisions were made following manual evaluation of the full texts.
Data Extraction
Data extraction was performed using standardized extraction templates capturing study design, population characteristics, cross-linking protocols, outcome measures, and follow-up duration. Extracted outcomes included keratometric parameters, visual acuity measures, endothelial cell density (ECD), corneal thickness changes, biomechanical or surrogate markers, and reported complications.
AI-assisted tools were used to support structured data extraction based on predefined data fields and extraction instructions, as detailed in Appendix B. All extracted data were manually verified against the original publications prior to synthesis. To enhance reliability, approximately 20% of included studies underwent secondary verification, with extracted values cross-checked against source texts and discrepancies resolved by direct reference to the original articles. No AI-assisted output was incorporated into the analysis without author verification.
Risk of Bias Assessment
Risk of bias was assessed manually using the Cochrane Risk of Bias 2 (RoB 2) tool for RCTs and the Risk Of Bias In Non-randomized Studies - of Interventions (ROBINS-I) tool for non-randomized studies [13]. Assessments were based on reported study methodology, outcome measurement, and completeness of follow-up. AI tools were not used to assign or automate risk-of-bias judgments.
Data Synthesis
Extracted data were synthesized qualitatively and grouped by outcome domain, including keratometric stabilization, visual acuity outcomes, endothelial safety, corneal thickness changes, biomechanical or surrogate measures, and complications. Results were stratified by cross-linking protocol to facilitate comparative interpretation. Representative ranges and medians were reported descriptively where appropriate. Formal meta-analysis was not performed due to methodological heterogeneity across included studies.
Statistical Reporting Conventions
Where reported, p-values and 95% confidence intervals (CIs) reflect statistical testing performed in the original source studies and are presented as reported by individual randomized controlled trials, observational cohorts, registries, or meta-analyses. No additional pooled statistical analyses were performed for this review. Continuous outcomes are reported as mean ± standard deviation (SD) when available, or as median (interquartile range, IQR) where distributions were nonparametric or reported as such in the source studies. Units are reported uniformly across tables and text.
Results
Following database searching, 542 records were identified (166 from manual searches and 376 from automated database queries). After the removal of 49 duplicate records, 493 unique records proceeded to title and abstract screening. As a result of title and abstract screening, 318 records were excluded, and 175 reports were retrieved for full-text assessment. Of these, 91 full-text articles were excluded. Ultimately, 84 studies met the inclusion criteria and were included in the qualitative synthesis. The study selection process is summarized in the PRISMA flow diagram (Figure 1).
PRISMA flowchart showing study selection processCXL: corneal collagen cross-linking; LLM: large language model; PRISMA: Preferred Reporting Items for Systematic Review and Meta-Analysis
Characteristics of Included Studies
The 84 included studies comprised a heterogeneous mix of randomized controlled trials, non-randomized comparative studies, observational cohorts, registry-based analyses, systematic reviews, and non-clinical investigations. Conventional epi-off (Dresden) protocols were the most extensively studied and included multiple prospective randomized controlled trials, large observational cohorts, and long-term registry studies with follow-up extending up to ten years. Transepithelial (epi-on) protocols were evaluated primarily in prospective randomized and non-randomized comparative studies, supplemented by several observational cohorts and one experimental laboratory (ex vivo) investigation assessing riboflavin stromal penetration. Accelerated cross-linking protocols were examined across a broad spectrum of designs, including randomized controlled trials, non-randomized comparative studies, retrospective cohorts, and registries, with follow-up ranging from short-term (six to 12 months) to intermediate and long-term intervals of up to five years. In addition, two systematic reviews and meta-analyses and one economic modeling study were included to contextualize comparative efficacy and cost-effectiveness but were not treated as primary clinical evidence. Key study characteristics, including design, protocol type, sample size, and follow-up duration, are summarized in Table 2.
Risk of Bias
Among the 84 included studies, risk of bias varied by design, with randomized controlled trials (RCTs) generally demonstrating lower risk than observational studies. Of the 26 RCTs evaluated using RoB 2, 10 (38%) were judged to be at low overall risk [7,16,23,32,36,40,72-74,88], characterized by robust randomization procedures (e.g., computer-generated sequences with allocation concealment) and minimal deviations from intended interventions or missing data. The remaining 16 RCTs (62%) were assessed as having some concerns [22,31,35,37-39,42,44,45,48-50,57,58,63,80], most commonly due to unclear blinding of outcome assessors or moderate attrition (approximately 10-20% loss to follow-up without imputation). No RCTs were rated at high risk, although selective reporting concerns were identified in four trials with unregistered protocols [23,32,74,88].
Of the 54 non-randomized clinical studies assessed using ROBINS-I V2, eight (15%) were judged to be at low risk of bias [15,20,24,27,34,46,59,79], primarily comprising well-matched registries or cohorts with robust outcome ascertainment; 25 (46%) were at moderate risk [14,17-19,22,25,28-30,33,41,43,47,52-55,60,61,65-67,70,75,81], largely due to residual confounding (e.g., baseline differences in keratoconus severity) that was partially mitigated by study design or adjustment; 18 (33%) were at serious risk [56,62,64,68,69,71-73,76-78,82-86,90,91], most often related to selection bias or unaddressed missing data; and three (6%) were at critical risk [63,89,92], reflecting substantial intervention misclassification or outcome measurement limitations.
The two meta-analyses [12,21] were not formally appraised for risk of bias, instead inheriting the bias profile of their included randomized controlled trials, which were predominantly at low risk to some concerns. One experimental laboratory (ex vivo) study [51], which evaluated intrastromal riboflavin penetration across different imbibition techniques in donor corneas, was likewise not assessed using RoB 2 or ROBINS-I and is reported separately as mechanistic evidence. One economic modeling study [26], synthesizing clinical efficacy and cost assumptions from multiple clinical sources, was also excluded from formal bias assessment. Overall, while RCTs provided higher-quality evidence for short-term outcomes, non-randomized studies contributed important long-term data despite elevated risks of confounding and selection, influencing the strength of conclusions for accelerated and transepithelial cross-linking protocols.
Keratometric Outcomes
Overall, epi-off (conventional and accelerated) CXL protocols produced greater and more durable keratometric flattening than transepithelial approaches, with the most robust long-term stabilization observed after conventional Dresden CXL [2,15,16,32,34,36,58]. Accelerated protocols achieved comparable short-term Kmax reductions, while transepithelial outcomes were more variable unless enhanced with modified riboflavin delivery or supplemental oxygen [12,37,40,41,45,57].
Keratometric outcomes were primarily assessed through changes in maximum keratometry (Kmax), which were reported in 70 of the 84 included studies [2,7,12,14-42,44,45,47-50,52,57-61,63-67,69-75,77-81,83-85,87,88,91-94]. Across protocols, studies consistently demonstrated corneal flattening and stabilization, although the magnitude, onset, and durability of effect varied according to protocol type, baseline disease severity, and follow-up duration [7,12,21,24,27,36]. Long-term data beyond three years were available predominantly for conventional Dresden epi-off variants [2,20,24,27,36].
For conventional Dresden epi-off CXL, randomized trials, comparative cohorts, and large registry studies consistently demonstrated progressive Kmax flattening with durable stabilization across follow-up intervals, with reported p-values and confidence intervals derived from individual study-level analyses rather than pooled estimates [2,15,16,32,34,36,58]. Collectively, these findings support the superior long-term durability of conventional epi-off CXL for keratometric stabilization, while indicating that accelerated protocols offer comparable short-term efficacy with greater variability in long-term stability and that transepithelial approaches generally require protocol enhancements to achieve similar effects [12,24,37,40,45,57]. Quantitative Kmax changes are summarized in Tables 3-5 and are reported as mean ± SD or median [IQR], as specified by the source studies, with p-values reflecting within-study or between-group comparisons conducted by the original authors.
Visual Acuity Outcomes
Overall, visual acuity was stabilized or modestly improved following corneal CXL across all protocols, with corrected distance visual acuity (CDVA) or best corrected visual acuity (BCVA) demonstrating more consistent and durable gains than uncorrected measures. Conventional epi-off CXL showed the most reliable long-term visual acuity stabilization, while accelerated and enhanced transepithelial approaches produced comparable short- to intermediate-term outcomes with faster postoperative recovery.
Visual acuity outcomes, including uncorrected distance visual acuity (UDVA) and CDVA/BCVA, were reported in 68 of the 84 included studies [2,7,12,14-18,20,22,24,25,27-30,32-42,44-50,52-54,57-61,63-75,77-81,83-85,87,91-94]. Across protocols, improvements were more consistently observed in CDVA than UDVA and most commonly emerged within the first six to 12 months following treatment, paralleling reductions in corneal irregularity and keratometric flattening [2,12,16,34,36,40,59].
Conventional epi-off CXL demonstrated the most durable visual acuity benefits, with sustained CDVA stabilization or improvement reported through two to five years and a low proportion of eyes experiencing visual decline in long-term registry and cohort data [24,34,36]. In contrast, transepithelial CXL exhibited more heterogeneous visual outcomes. Standard epi-on protocols were frequently associated with smaller or less durable CDVA gains beyond 12 months, whereas enhanced transepithelial approaches incorporating iontophoresis, modified riboflavin formulations, or supplemental oxygen achieved CDVA stabilization approaching epi-off outcomes in selected prospective studies [41,45,50,57,59].
Accelerated CXL protocols demonstrated visual acuity outcomes comparable to conventional epi-off CXL at short- and intermediate-term follow-up, with visual stability generally maintained through three to five years, although improvements often plateaued earlier in some cohorts [12,24,65,72-74].
Collectively, visual acuity outcomes across protocols mirrored keratometric trends, with conventional epi-off CXL providing the most durable long-term stabilization, while accelerated and enhanced transepithelial approaches demonstrated comparable short-term efficacy with advantages in recovery time. Quantitative visual acuity changes are reported in logMAR units as mean ± SD or median (IQR), as specified by the source studies. Reported p-values and 95% confidence intervals are derived from individual randomized trials, observational cohorts, or registry analyses where available, and outcomes stratified by follow-up interval are summarized in Table 6.
Endothelial Cell Density Outcomes
All corneal CXL protocols demonstrated a strong endothelial safety profile, with no clinically meaningful endothelial cell loss observed when established safety parameters were followed. Across studies, mean ECD changes remained within physiologic measurement variability over short- and long-term follow-up.
ECD was reported in 52 of the 84 included studies and consistently demonstrated preservation across conventional, accelerated, and transepithelial CXL protocols, with no cases of endothelial decompensation reported during follow-up [2,7,12,14-18,20,22,24,25,27,28,30,32-42,44,45,47,49,50,52,57-61,63,65,66,69,72-75,78,80,83-85,91,93]. Across RCTs, comparative cohorts, and large registries, mean ECD changes were minimal and not clinically significant, with values remaining within expected test-retest variability [2,14-16,34,36,40].
Conventional epi-off (Dresden) CXL showed stable endothelial outcomes across short-, intermediate-, and long-term follow-up, with no consistent or statistically significant deviations from baseline reported in randomized trials, observational cohorts, or registry-based analyses [2,14-16,24,34,36,40,58]. Transepithelial (epi-on) CXL protocols demonstrated similarly favorable endothelial safety, with prospective and comparative studies reporting equivalent endothelial preservation and no clinically meaningful differences compared with epi-off approaches [7,14,37,40,42,45,50,58,61]. Enhanced transepithelial techniques, including oxygen supplementation and iontophoresis-assisted riboflavin delivery, maintained endothelial stability through intermediate follow-up [41,45,50,60].
Accelerated CXL protocols exhibited endothelial safety comparable to conventional Dresden CXL. Comparative trials and meta-analyses reported no significant differences in ECD change between accelerated and standard protocols at short-term follow-up, with longer-term cohort and registry data confirming sustained endothelial preservation through three to five years, including with pulsed and high-fluence variants [12,24,72-74,78,81,84]. Rare reports of notable ECD reduction were confined to thin corneas or hypo-osmolar riboflavin use and did not result in endothelial dysfunction [83].
Across all protocols, no consistent associations were identified between baseline age, keratoconus severity, or treatment intensity and clinically meaningful endothelial cell loss [2,59,61]. Collectively, these findings support a robust endothelial safety profile for conventional, accelerated, and transepithelial CXL when performed within established safety thresholds. Quantitative ECD outcomes are summarized in Table 7 as mean ± SD (cells/mm²), with reported p-values and confidence intervals reflecting within-study comparisons and registry-based analyses rather than pooled estimates.
Safety and Complications
Across all protocols, corneal CXL demonstrated a favorable safety profile, with adverse events predominantly transient and serious vision-threatening complications remaining rare. Differences in safety outcomes were largely driven by epithelial management and postoperative stromal remodeling rather than treatment fluence alone.
Transient and self-limited adverse events: Transient postoperative adverse events were common and protocol-dependent. Conventional epi-off CXL was associated with the highest incidence of early corneal haze, particularly within the first one to three months, with reported rates ranging widely across studies but declining substantially over time. Large registry data demonstrated haze rates of approximately 15% at one year and <2-3% by five years, with persistent visually significant haze remaining uncommon [2,24]. Postoperative pain, delayed epithelial healing, and sterile infiltrates were more frequent following epi-off protocols but were typically self-limited and responsive to standard management [7,16,19,32].
Transepithelial and accelerated CXL protocols demonstrated more favorable short-term tolerability, with lower rates of corneal haze, fewer epithelial healing complications, reduced postoperative discomfort, and faster early visual recovery compared with conventional epi-off CXL [7,14,37,44,47]. Comparative cohorts and meta-analyses reported similar or reduced transient adverse event rates with accelerated protocols relative to Dresden CXL, without an increase in long-term complications [12,72-74,81].
Serious and vision-threatening complications: Serious vision-threatening complications following CXL were rare across all protocols. Infectious keratitis occurred infrequently, predominantly after epi-off treatment, with large retrospective series reporting incidence rates on the order of 0.001-0.5% [56]. Central toxic keratopathy was reported primarily following accelerated protocols in isolated series and remained uncommon overall [70]. Other serious events, including persistent epithelial defects, stromal scarring, or retreatment for progression, were rare and occurred more frequently in high-risk corneas or modified protocols [21,24,78].
Overall, when performed within established safety parameters, all CXL protocols demonstrated acceptable safety profiles. Epi-off CXL was associated with higher rates of transient haze and discomfort but low long-term morbidity, while transepithelial and accelerated approaches offered improved early tolerability with similarly low rates of serious complications (Tables 8, 9).
Corneal Thickness Changes (Pachymetry)
All corneal CXL protocols exhibited a predictable biphasic pachymetric response, characterized by early postoperative thinning followed by partial or complete recovery within the first year. No protocol was associated with progressive long-term corneal thinning when established safety thresholds were respected.
Corneal thickness changes, assessed primarily by central corneal thickness (CCT) or thinnest corneal thickness (TCT), were reported in 48 of the 84 included studies [2,7,12,14,15,17,18,20-22,24,25,27,28,30,32,33,36,37,39-44,46-51,55,58,60,61,63,65,69,71-74,76,80,81,91,92,94]. Across protocols, studies consistently demonstrated transient early thinning attributable to stromal dehydration and compaction, followed by recovery toward baseline within 3-12 months, without association with endothelial compromise or ectatic progression [2,12,14,15,36,61].
Conventional epi-off (Dresden) CXL was associated with greater early pachymetric reduction compared with transepithelial approaches, with recovery observed over subsequent months and long-term stability thereafter [2,14,15,20,21,36]. Large registry and long-term cohort data confirmed minimal net pachymetric change at 3-5 years, supporting the absence of persistent stromal thinning following standard CXL [2,24]. Use of hypo-osmolar riboflavin in thin corneas preserved safety while mitigating excessive early thinning [72,76].
Transepithelial (epi-on) CXL demonstrated smaller and shorter-lived pachymetric changes, with rapid recovery reflecting limited stromal dehydration and preserved epithelial integrity [7,37,39,41,43,44,51,61]. Comparative studies reported significantly less early thinning with epi-on techniques than with epi-off CXL, without meaningful long-term differences in corneal thickness [7,43,44,61]. Enhanced transepithelial protocols maintained pachymetric stability through intermediate follow-up [46-50,60].
Accelerated CXL protocols exhibited pachymetric responses comparable to conventional epi-off CXL, characterized by early thinning followed by recovery within several months [55,63,65,91]. Comparative trials and meta-analyses demonstrated no significant long-term differences in CCT or TCT between accelerated and standard protocols, including pulsed and customized variants [12,17,25,69,71-74,80,81,94].
Across all protocols, early pachymetric reduction correlated with stromal remodeling and transient haze formation but did not predict long-term corneal instability or visual decline [2,59,61]. Overall, corneal thickness changes following CXL were transient and protocol dependent, with recovery toward baseline observed in the majority of eyes and no evidence of progressive thinning when established safety parameters were followed. Quantitative corneal thickness outcomes are summarized in Table 10 as mean ± SD, with reported p-values reflecting individual study-level analyses rather than pooled estimates.
Biomechanical and Surrogate Outcomes
Surrogate biomechanical measures supported effective stromal cross-linking across protocols, with greater treatment penetration generally observed following epi-off techniques. However, these metrics demonstrated variable correlation with long-term clinical outcomes and should be interpreted as complementary rather than definitive efficacy endpoints.
Biomechanical and surrogate outcomes, including stromal demarcation line depth, corneal hysteresis (CH), corneal resistance factor (CRF), and deformation-based parameters derived from devices such as the Ocular Response Analyzer® (Reichert, Inc., Depew, New York, United States) and Corvis® ST (OCULUS Optikgeräte GmbH, Wetzlar, Germany), were reported in 32 of the 84 included studies [7,12,14,16-18,21-25,39-42,50,53-55,58,61,64,67,69,74,75,80,83,88,90,94]. These measures were primarily used as indirect indicators of stromal cross-linking effect and biomechanical stiffening rather than direct clinical endpoints.
Conventional epi-off (Dresden) CXL consistently demonstrated deeper stromal demarcation lines and more pronounced biomechanical changes compared with transepithelial approaches, reflecting greater riboflavin penetration and treatment depth [21,25,39]. While modest increases in CH and CRF were reported in several studies, findings were variable and not uniformly significant, whereas deformation-based parameters more consistently indicated increased biomechanical stability following treatment [21,74].
Transepithelial (epi-on) CXL generally produced shallower demarcation lines and less consistent biomechanical changes, consistent with reduced riboflavin diffusion through the intact epithelium [39,61]. Enhanced transepithelial techniques incorporating oxygen supplementation, iontophoresis, or modified riboflavin formulations achieved greater stromal penetration in selected studies, with biomechanical profiles approaching those of epi-off protocols [41,52]. Nonetheless, biomechanical changes following standard epi-on CXL remained heterogeneous, paralleling the variability observed in long-term clinical outcomes [7,40].
Accelerated CXL protocols exhibited biomechanical surrogate outcomes broadly comparable to conventional epi-off CXL when equivalent total fluence was delivered [12,17,69,80]. Comparative trials and meta-analyses reported no consistent differences in demarcation depth or biomechanical parameters between accelerated and standard protocols, although higher irradiance regimens were occasionally associated with slightly reduced penetration [12]. Pulsed and adapted-fluence accelerated variants demonstrated similar biomechanical profiles, potentially reflecting improved oxygen availability during treatment [80,94].
Across all protocols, greater demarcation line depth correlated with baseline corneal thickness and disease severity but did not reliably predict long-term keratometric or visual outcomes [12,25,61]. Cross-study comparability was limited by variability in measurement techniques, device-specific parameters, and follow-up duration. Overall, biomechanical and surrogate measures provided supportive evidence of effective stromal cross-linking but should be interpreted as adjunctive indicators alongside clinical endpoints. Quantitative biomechanical outcomes are summarized in Tables 11, 12 using the statistical format reported by the source studies, with p-values and confidence intervals reflecting individual study-level or meta-analytic analyses where applicable.
Discussion
Summary of Key Findings
This systematic review synthesizes comparative evidence from 84 studies evaluating conventional Dresden (epi-off), accelerated, and transepithelial (epi-on) corneal CXL protocols for progressive keratoconus. Across randomized trials, observational cohorts, and large registry datasets, conventional epi-off CXL consistently demonstrated the most durable keratometric stabilization and visual acuity preservation, with sustained effects reported up to 5-10 years in long-term follow-up [2,20,24,36]. Accelerated protocols achieved comparable short-term outcomes but exhibited greater variability in durability beyond two to three years, particularly in registry-based analyses [12,24]. In contrast, transepithelial approaches showed more heterogeneous efficacy, with standard epi-on protocols frequently underperforming relative to epi-off CXL unless enhanced with modified riboflavin delivery or supplemental oxygen [37,40,45,57].
Despite these differences in efficacy, safety profiles across all protocols were favorable. ECD was preserved, corneal thickness changes followed predictable and transient biphasic patterns, and serious complications remained rare [2,7,12,24]. Collectively, these findings suggest that differences in long-term outcomes are driven primarily by epithelial management, oxygen availability, and effective stromal penetration depth rather than by treatment fluence alone, underscoring the importance of protocol selection tailored to disease severity and patient-specific factors.
Reconciling Differences in Protocol Efficacy
Observed heterogeneity in CXL efficacy across protocols reflects fundamental differences in epithelial removal, oxygen-dependent photochemical reactions, and stromal penetration rather than total delivered fluence alone [3,5,12]. Conventional epi-off CXL enables unimpeded riboflavin diffusion and sustained oxygen availability, resulting in deeper and more uniform stromal cross-linking. These mechanistic advantages are consistent with its superior long-term keratometric stability and visual outcomes [17,39,69].
Accelerated CXL protocols, while grounded in the Bunsen-Roscoe reciprocity law, may be constrained by oxygen depletion at higher irradiances. This limitation likely contributes to the greater variability in long-term outcomes observed in registry and cohort data, despite short-term non-inferiority demonstrated in randomized trials and meta-analyses [3,12,24]. Pulsed and adapted-fluence accelerated strategies partially address this limitation by facilitating oxygen replenishment during treatment and have demonstrated biomechanical and clinical outcomes approaching those of conventional protocols in selected studies [69,80,94].
Historically, transepithelial CXL underperformed due to the epithelial barrier limiting riboflavin diffusion, resulting in shallower demarcation depths and reduced biomechanical stiffening [39,61]. However, recent enhancements-including oxygen supplementation, iontophoresis, and modified riboflavin formulations-have improved stromal penetration and surrogate biomechanical measures, narrowing the efficacy gap with epi-off CXL in prospective trials [41,45,52,57]. These advances highlight the evolving nature of epi-on techniques and the importance of distinguishing standard from enhanced transepithelial protocols in comparative analyses.
Safety Considerations Across CXL Techniques
Across all protocols, CXL demonstrated a favorable safety profile, with most adverse events being transient and closely related to epithelial management and postoperative stromal remodeling [2,7,12]. Conventional epi-off CXL was associated with higher rates of early corneal haze and postoperative discomfort; however, haze typically resolved over time and rarely progressed to visually significant scarring, resulting in low long-term morbidity [2,15,21,24]. Accelerated and transepithelial protocols generally offered improved early tolerability, with lower rates of epithelial complications and faster visual recovery [7,37,50,72].
Serious complications-including infectious keratitis, central toxic keratopathy, and persistent stromal scarring-were rare across all protocols and were most commonly reported in the context of epi-off or high-risk accelerated treatments accompanied by additional risk factors [24,56,70]. These findings reinforce the overall safety of CXL when established parameters are followed and emphasize the importance of careful patient selection, perioperative management, and adherence to protocol-specific safety thresholds.
Clinical Implications and Protocol Selection
From a clinical standpoint, these findings support conventional epi-off CXL as the preferred option for patients with moderate-to-advanced keratoconus or a high risk of progression, where durable long-term stabilization is paramount [2,24,36]. Accelerated protocols represent a reasonable alternative when treatment efficiency, patient tolerance, or resource constraints are prioritized, particularly given their comparable short-term efficacy [12,24,72]. Enhanced transepithelial approaches may be appropriate for select patients seeking reduced invasiveness and postoperative discomfort, provided that potential trade-offs in long-term durability are carefully considered [37,45,57].
Accordingly, shared decision-making that integrates baseline disease severity, corneal thickness, progression risk, and patient preferences remains essential, especially as protocol refinements and longer-term comparative data continue to emerge.
Limitations
This review is subject to several limitations. Substantial heterogeneity in study design, outcome definitions, follow-up duration, and protocol parameters precluded quantitative meta-analysis. Long-term comparative data beyond five years remain limited for accelerated and transepithelial protocols, and many studies relied on surrogate biomechanical measures rather than direct clinical endpoints [12,21]. These limitations should be considered when interpreting comparative efficacy, particularly for newer or evolving protocol variants.
Conclusions
This systematic review of 84 studies published through December 2025 supports conventional Dresden epi-off corneal CXL as the most consistently supported reference standard for the management of progressive keratoconus in adults, with robust evidence for long-term keratometric stabilization, visual acuity preservation, biomechanical reinforcement, and endothelial safety. Accelerated CXL protocols demonstrate comparable short-term efficacy with advantages in treatment efficiency, reduced postoperative morbidity, and faster visual recovery, supporting their use as appropriate alternatives in selected clinical settings.
Enhanced transepithelial (epi-on) approaches, including oxygen-augmented and modified riboflavin delivery systems, offer improved tolerability and safety with minimal invasiveness and may be suitable for early-stage disease, thin corneas, or patients prioritizing comfort. However, long-term durability remains more variable without protocol optimization. Collectively, these findings emphasize the importance of individualized, patient-tailored protocol selection and standardized monitoring strategies to optimize outcomes and address the growing global burden of keratoconus. Further well-designed RCTs with extended follow-up and broader population representation are needed to refine protocol selection and clarify long-term comparative durability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global incidence and prevalence of keratoconus: a systematic review and meta-analysis Cornea Sriranganathan A Chan CC Dhillon J Felfeli T 202510.1097/ICO.000000000000397340833011 · doi ↗ · pubmed ↗
- 2Five-year corneal cross-linking outcomes: a save sight keratoconus registry study Clin Exp Ophthalmol Ferdi AC Kandel H Nguyen V Tan J Arnalich-Montiel F Abbondanza M Watson SL 9185120233624004710.1111/ceo.14177 PMC 10091974 · doi ↗ · pubmed ↗
- 3Corneal cross-linking: the evolution of treatment for corneal diseases Front Pharmacol Wu D Lim DK Lim BX Wong N Hafezi F Manotosh R Lim CH 6866301220213434964810.3389/fphar.2021.686630 PMC 8326410 · doi ↗ · pubmed ↗
- 4Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus Am J Ophthalmol Wollensak G Spoerl E Seiler T 62062713520031271906810.1016/s 0002-9394(02)02220-1 · doi ↗ · pubmed ↗
- 5Eye Wiki: Corneal cross-linking 12 2025 2025 Eye Wiki 2025 https://eyewiki.org/Corneal_Cross-Linking
- 6Induction of cross-links in corneal tissue Exp Eye Res Spoerl E Huhle M Seiler T 97103661998953383510.1006/exer.1997.0410 · doi ↗ · pubmed ↗
- 7Transepithelial versus epithelium-off corneal cross-linking for the treatment of progressive keratoconus: a randomized controlled trial Am J Ophthalmol Soeters N Wisse RP Godefrooij DA Imhof SM Tahzib NG 82182815920152570347510.1016/j.ajo.2015.02.005 · doi ↗ · pubmed ↗
- 8Corneal cross-linking in keratoconus: a scoping review of clinical evidence and public health implications Research Square Ojeda-Salamanca R Villagra B Figueroa Vargas N Berríos-Arvey H 262025