Nontuberculous Mycobacterial Parotid Abscess: Clinical Evaluation and Management of a Rare Case in an Adult Female With Sjögren’s Syndrome
Adeeba F Ghias, Michael Black, Jae Lim

TL;DR
A rare case of a nontuberculous mycobacterial abscess in the parotid gland of an adult woman with Sjögren’s syndrome was successfully treated with surgery after failed antibiotic therapy.
Contribution
Highlights a rare NTM infection in an adult with Sjögren’s syndrome and provides management insights for similar cases.
Findings
NTM parotid abscess in an adult with Sjögren’s syndrome is uncommon and often requires surgical intervention.
Prolonged antibiotic therapy was complicated by adverse effects and failed to resolve the abscess.
Superficial parotidectomy led to no recurrence during follow-up.
Abstract
This report presents a case of a young female with Sjögren’s disease who developed a non-tuberculous mycobacterial (NTM) abscess in the right parotid gland. Following an unsuccessful four-month course of antibiotic therapy, she underwent a superficial parotidectomy. This was an unusual case in this demographic, considering that most cervical NTM infections are diagnosed in pediatric patients who have a characteristic violaceous neck mass. Her case was reviewed using the medical record, and photo-documentation was conducted throughout follow-up visits in the outpatient clinic. Infectious disease specialists were heavily involved in determining her antibiotic treatment plan, which spanned over four months. The initial therapy was complicated by multiple antibiotic changes and pauses in treatment due to adverse effects, including chest tightness and elevation of liver function tests…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1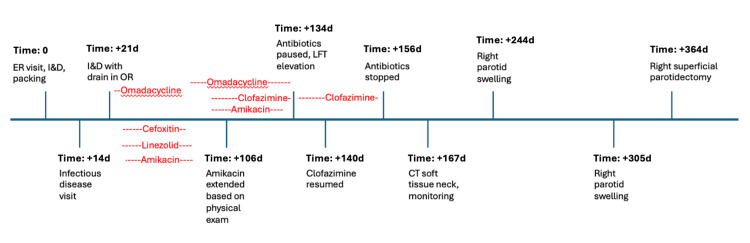 Figure 2
Figure 2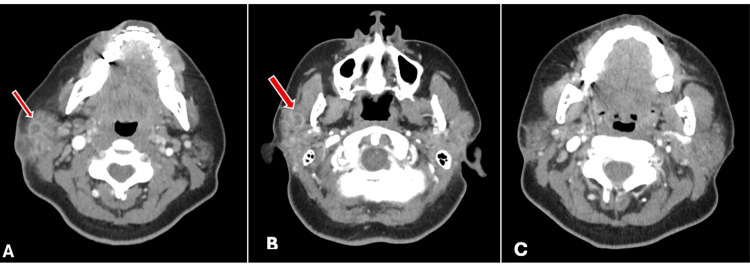 Figure 3
Figure 3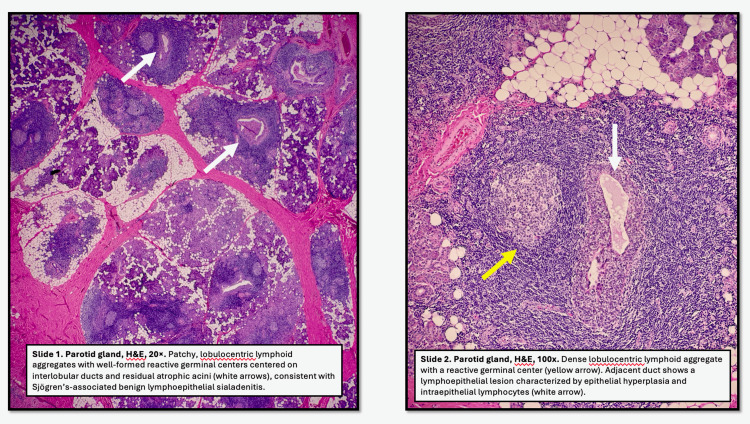 Figure 4
Figure 4| Antibiotic | Dose (mg) | Duration | Adverse effects |
| Omadacycline | 450 BID → 300 daily | Cycle 1: 23 days; Cycle 2: 85 days | - |
| Clofazimine (study drug) | 100 daily | Cycle 1: 70 days; Cycle 2: 17 days | LFT elevation to 3× upper limit of normal |
| Amikacin | 700 mg IV daily via PICC | Cycle 1: 25 days; Cycle 2: 62 days | - |
| Linezolid | 600 daily | 25 days | - |
| Cefoxitin | 3000 BID via PICC | 14 days | Chest tightness |
| Imipenem | 1000 BID via PICC | 7 days | - |
| Vancomycin | N/A (given perioperatively / as a bridge to above) | ||
| Ampicillin-sulbactam | |||
| Sulfamethoxazole-trimethoprim | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Salivary Gland Tumors Diagnosis and Treatment · Otolaryngology and Infectious Diseases
Introduction
Parotitis, as a broad term, encompasses multiple possible etiologies of parotid disease, whether infectious or non-infectious. The mumps virus, Staphylococcal species, Streptococcus viridans, and other anaerobic oral flora are commonly implicated [1]. However, few existing reports have mentioned the incidence of infection with non-tuberculous mycobacterial (NTM) species in an immunocompetent host. The most common presentation of NTM in the head and neck region is a violaceous neck mass in the pediatric population, caused by the Mycobacterium avium-intracellulare complex (MAC) [2-4]. The transmission pattern is thought to be through soil exposure [5]. Multi-drug therapy is often required and is described in the pediatric infectious disease literature, involving combinations of azithromycin or clarithromycin, clofazimine, ethambutol, isoniazid, rifampin, and/or amikacin [2,3]. The treatment course duration is highly dependent on the response to initial antimicrobial therapy [2].
Case presentation
We present a case of a 38-year-old Asian female with a history of Sjögren’s disease, asthma, alpha-thalassemia trait, and non-alcoholic steatohepatitis who had previous intermittent episodes of right parotid swelling and then presented to the emergency room with a fluctuant, multiloculated right parotid abscess extending nearly through the epidermis (Figure 1). On history, she had never been on immunosuppressive medications, nor was she ever in an immunocompromised state. She reported no sick contacts and no recent travel. Her facial nerve function remained intact despite the presenting complaint. The abscess was drained, cultured, and the resultant wound packed with iodoform; the patient was discharged on clindamycin and a steroid taper until her short-interval outpatient follow-up for removal and replacement of packing. Despite a good interval result at a follow-up visit, she started to develop increasing pain on the last day of her week-long antibiotic course. Sulfamethoxazole-trimethoprim was then added. Wound cultures that were initially negative then grew 2+ highly resistant strains of Mycobacterium abscessus. Appropriate infectious disease follow-up was arranged. She continued to have drainage from the site despite additional antibiotic treatment, and there was concern for recollection of abscess as well as fistulization. She underwent surgical incision and drainage with drain placement in the operating room 20 days after initial presentation.
Physical examination during active infection.
Per our infectious disease colleagues, this was a highly resistant bacterium requiring likely four to six weeks of combination IV and PO multiagent antibiotic therapy. Bacterial growth occurred from culture at eight weeks, in a delayed fashion, as is typical of NTM infections. Initial data indicated susceptibility to amikacin and intermediate susceptibility to cefoxitin, imipenem, and linezolid. Resistance was noted to ciprofloxacin, clarithromycin, doxycycline, moxifloxacin, and sulfamethoxazole-trimethoprim. These data were used to guide the treatment plan. Her complicated antibiotic course and medical timeline are detailed in Table 1 and Figure 2. Clofazimine was initiated as a study drug, so there was a delay in obtaining it at our institution. Audiology performed appropriate ototoxic monitoring while on an aminoglycoside (amikacin), with high-frequency audiologic testing and otoacoustic emissions testing (OAEs). A follow-up CT soft tissue scan of the neck was conducted five months after her initial presentation to help guide antibiotic duration. This scan demonstrated near-resolution of her abscess, and therefore, all antibiotics were discontinued after the patient completed eighteen weeks of treatment. Note that her treatment course was not truly continuous due to the adverse effects as listed in Table 1. Figure 3 demonstrates her juxtaposed initial presentation and post-treatment resolution. She had recurrence of parotid swelling without abscess three months and then five months later. These presentations were treated with a steroid taper, once with amoxicillin-clavulanate and once with linezolid, respectively. The swelling resolved, although a five-month post-treatment scan demonstrated recurrence of two intraparenchymal fluid collections measuring one centimeter and half a centimeter.
Chronological timeline of key events during treatment, with antibiotics superimposed to clarify the timing of administration.Please note that the initial “Time = 0” point is followed by progressively increasing time (in days) from the ER visit.LFT: Liver function test; I&D: Incision and drainage.
CT soft tissue neck scan showing (A) the initial rim-enhancing infection pre-treatment, (B) recurrence of symptoms and radiologic findings at five months, and (C) post-treatment following antibiotic therapy and superficial parotidectomy.
Given the recurrent symptoms, a superficial parotidectomy was recommended. The patient consented to the procedure and, for aesthetic contouring, concurrently underwent a sternocleidomastoid muscle rotation flap and abdominal fat grafting to the site. Final histopathologic analysis (Figure 4) and culture did not reveal any atypical mycobacterial growth. Final pathology reported “abscess, features consistent with Sjögren syndrome, and two benign intraparotid lymph nodes.” Her operative site has healed well, and there has been no further recurrence of symptoms.
Histopathological examination from the patient’s superficial parotidectomy, provided by the pathologist, Dr. Michael Black.(A) Parotid gland, H&E, 20×. Patchy, lobulocentric lymphoid aggregates with well-formed reactive germinal centers centered on interlobular ducts and residual atrophic acini, consistent with Sjögren’s-associated benign lymphoepithelial sialadenitis. (B) Parotid gland, H&E, 100×. Dense lobulocentric lymphoid aggregate with a reactive germinal center. The adjacent duct shows a lymphoepithelial lesion characterized by epithelial hyperplasia and intraepithelial lymphocytes.
Discussion
NTM cervical lymphadenitis is classically described in the pediatric population, with a slight female-to-male predominance [3]. Of the NTM infections, Mycobacterium abscessus is characterized by its slow growth in culture media [2]. Therefore, the initial diagnosis of atypical mycobacterial infections can be difficult and is subsequently complicated by multidrug resistance [6]. Although in this case the cause of the patient’s parotid swelling was deemed infectious, a neoplasm must be ruled out in the evaluation process [6]. Imaging findings are non-specific, with these abscesses appearing as cystic nodal masses that do not cause mass effect or significant fat stranding in the surrounding tissue [7]. Other important differential diagnoses to consider are toxoplasmosis, cytomegalovirus (CMV) or Epstein-Barr virus (EBV) infection, sarcoidosis, and Bartonella [3,8].
There are two reports of parotid abscesses in immunocompetent adult patients, one of a 48-year-old female [9] and the other in a 79-year-old male [5]. The female patient had a multi-year history of suppurative bacterial sialadenitis prior to diagnosis of Sjögren’s disease, later necessitating parotidectomy [9]. Underlying autoimmune parotid disease, like Sjögren’s, although known to cause recurrent sialadenitis and intermittent recurrent swelling of the major salivary glands, does not have a strong association with an increased risk of abscess formation or atypical infection [9]. The male patient required eight months total of various antibiotics for cure of his NTM parotid abscess without the need for parotidectomy, and he had no evidence of recurrence through four years of surveillance [5].
The loose treatment algorithm accepted in the pediatric literature recommends initial antimicrobial trials to avoid unnecessary and disfiguring surgical intervention. A combination of national and international studies report a variable response rate between patients in the United States (50%), the Netherlands (66%), and France (90%) after studying multiple case series at their respective pediatric hospitals [2,3,10]. As interpreted from the available literature, antibiotic therapy alone has demonstrated a lower rate of cure than antibiotic therapy in combination with surgery and should be reserved for cases where medical comorbidities prevent surgical intervention or where the patient adamantly refuses surgery [2-4]. Due to the adverse effect profiles and poor compliance with the long duration of the antibiotics utilized in NTM treatment, the literature has historically favored surgical excision [2,6]. Commonly cited drug effects are weight loss, gastrointestinal upset, nausea, and allergic reactions [2]. In fact, Lindeboom et al [10] published a 78% adverse effect rate in their study compared to a 28% surgical complication rate. There is consensus within the literature that if operative intervention is required, excision is preferred over incision and drainage to reduce the risk of relapse and/or fistulization to the skin [2,3,8]. Preoperative medical therapy, by decreasing edema within the salivary gland, decreases the risk of subsequent surgical morbidity, particularly facial nerve injury [11].
Involvement of infectious disease specialists is critical in drug administration, titration, and monitoring treatment response [2]. Clarithromycin is most frequently cited in the literature, combined synergistically with ethambutol or rifabutin [3,11]. However, there is no standardization of antibiotic duration or timing of surgery in cases of NTM salivary gland abscesses, with the literature reporting multiple different combinations of antibiotics as well as a range of therapy from a minimum of two weeks to up to eight months [3-5,11].
Conclusions
Although the existing literature provides limited evidence and lacks a well-established consensus on the occurrence of NTM parotid abscess in patients with Sjögren’s syndrome, this patient achieved complete resolution of her atypical mycobacterial parotid abscess after approximately one year of combined medical and surgical management. A multimodal therapeutic approach is supported by multiple clinical reports, despite significant variation in the duration of antimicrobial therapy and the choice of drug regimens. Individualized treatment planning is critical and should be guided by a thorough evaluation of the risks and benefits associated with long-term antimicrobial therapy compared to surgical intervention for each individual case. Additional case reports and systematic studies of this rare condition are necessary to establish robust, evidence-based treatment algorithms and improve long-term clinical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1[Clinical aspects of abscess development in parotitis]HNO Thiede O Stoll W Schmäl F 3323385020021206369110.1007/s 001060100544 · doi ↗ · pubmed ↗
- 2Non tuberculous mycobacterial lesion of the parotid gland and facial skin in a 4year old girl: a proposed treatment strategy Am J Otolaryngol Berkovic J Vanchiere JA Gungor A 89943720162695485810.1016/j.amjoto.2015.09.006 · doi ↗ · pubmed ↗
- 3Cervicofacial non-tuberculous mycobacteria: a report of 30 cases Eur Ann Otorhinolaryngol Head Neck Dis Rives P Joubert M Launay E Guillouzouic A Espitalier F Malard O 10711113320162695277810.1016/j.anorl.2016.02.001 · doi ↗ · pubmed ↗
- 4Atypical mycobacterial adenitis presenting as a parotid abscess Am J Otolaryngol Tunkel DE 428432161995857226210.1016/0196-0709(95)90083-7 · doi ↗ · pubmed ↗
- 5Non-tuberculous mycobacterial infection of the parotid gland in an immunocompetent elderly patient BMJ Case Rep Yamanaka T Okamoto H Hosoi H 02013201310.1136/bcr-2013-200990 PMC 382215924132446 · doi ↗ · pubmed ↗
- 6Mycobacterial disease of the parotid gland Oral Surg Oral Med Oral Pathol Oral Radiol Endod Holmes S Gleeson MJ Cawson RA 2922989020001098294910.1067/moe.2000.107973 · doi ↗ · pubmed ↗
- 7Nontuberculous mycobacterial lymphadenitis of the head and neck: radiologic observations and clinical context Pediatr Radiol Bagla S Tunkel D Kraut MA 4024063320031269269710.1007/s 00247-003-0884-y · doi ↗ · pubmed ↗
- 8Cervicofacial mycobacterial infections presenting as major salivary gland disease Laryngoscope Stanley RB Fernandez JA Peppard SB 12711275931983662122310.1002/lary.1983.93.10.1271 · doi ↗ · pubmed ↗