Uncommon Presentation of Primary Bladder Signet Ring Cell Carcinoma With Peritoneal Carcinomatosis: A Rare Case Report
Jean Paule Joumaa, Kelly Katherine Karam, Joya Ghaleb, Hilda E. Ghadieh, Alaa Korhani

TL;DR
A rare bladder cancer case with peritoneal spread is reported, emphasizing diagnostic challenges and treatment response.
Contribution
This case report adds to the limited literature on primary bladder signet ring cell carcinoma with peritoneal carcinomatosis.
Findings
The patient showed tumor shrinkage after cisplatin/gemcitabine and immunotherapy.
SRCC was confirmed via immunohistochemistry as PD-L1 positive and CDX-2/ER negative.
Nonspecific symptoms and histological overlap with gastrointestinal tumors complicate SRCC diagnosis.
Abstract
Primary signet ring cell carcinoma (SRCC) of the bladder is an exceptionally rare and aggressive malignancy, accounting for only 0.12%–0.6% of all bladder cancers. This case report describes a 54‐year‐old female who presented with urinary incontinence and abdominal pain, initially misdiagnosed as a urinary tract infection. Imaging revealed suspicious bladder findings, and subsequent cystoscopy with transurethral resection identified SRCC, later confirmed by immunohistochemistry (PD‐L1 positive, CDX‐2/ER negative). Despite peritoneal carcinomatosis, the patient responded to cisplatin/gemcitabine chemotherapy and immunotherapy, demonstrating tumor shrinkage on follow‐up imaging. This case highlights the diagnostic challenges of SRCC due to its nonspecific symptoms and potential histological overlap with other metastatic gastrointestinal tumors. Early recognition and a multidisciplinary…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
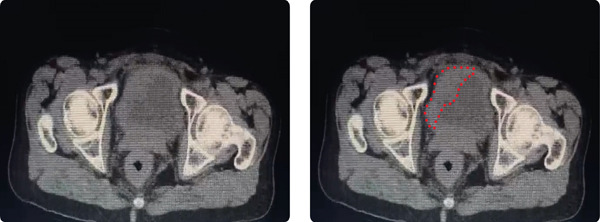 Figure 1
Figure 1|
|
|
|
|
|
|
|---|---|---|---|---|---|
| Zeng and Swee, 2022 | 64, M | Bone metastases; severe hypocalcemia | Metastatic SRCC with bone mets | Chemotherapy + immunotherapy; denosumab; palliative care | Died 16 months postdiagnosis |
| Yamamoto et al., 2001 | 56, M | Oliguria; postrenal failure due to bladder tumor | pT3b, pN2, pMx | Total cystectomy; declined adjuvant chemotherapy | Died 8 months postoperatively |
| Celik et al., 2014 | 66, M | Urinary difficulty; prostate mass; extensive bone mets | Metastatic SRCC of the prostate | Hormonal therapy → docetaxel chemotherapy; palliative radiotherapy | Died of urosepsis 22 months postdiagnosis |
| Bouhajja et al., 2019 | 70, F | Right back pain, dysuria, gross hematuria | Not specified | Biopsy diagnosis; treatment not specified | Alive 3 years postdiagnosis |
| Bouhajja et al., 2019 | 53, M | Gross hematuria; bladder wall thickening | Muscle‐invasive; perivesical fat invasion | TURBT only; no cystectomy | Alive 2 years postdiagnosis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary and Genital Oncology Studies · Bladder and Urothelial Cancer Treatments · Cancer and Skin Lesions
1. Introduction
Primary signet ring cell carcinoma (SRCC) of the bladder is a rare and aggressive malignancy, often diagnosed at advanced stages due to its nonspecific urinary symptoms and histological resemblance to other metastatic gastrointestinal tumors (1). SRCC accounts for < 1% of bladder cancers and typically affects patients over 40 years old, with a male predominance (2). Patients commonly present with hematuria, dysuria, or urinary retention, mimicking benign conditions like urinary tract infections (3).
Histologically, SRCC is characterized by cytoplasmic mucin accumulation displacing nuclei peripherally, forming the classic “signet ring” appearance as its name states (4). Diagnosis requires exclusion of metastatic origins, particularly gastric or colorectal primary cancers, through both endoscopic and immunohistochemical evaluation (5). Management remains challenging, with radical cystectomy (RC) as the gold standard for localized disease, though advanced cases often require chemotherapy and immunotherapy (6). This case highlights the diagnostic complexities and emphasizes the need for early suspicion in patients with persistent urinary symptoms.
2. Case Report
A 54‐year‐old Gravida 6 Para 6 (G6P6) postmenopausal female, previously healthy, presented for urinary incontinence and lower abdominal pain. History goes back to 4 months, when the patient started having symptoms of urinary dribbling, increased frequency of urination, and dysuria, alongside a persistent lower abdominal pain. Notably, the patient has a smoking history of 30 pack‐years (one pack per day for 30 years). To rule out an infectious cause, multiple urinalyses were ordered, each showing a range of 20–25 white blood cells (WBCs) in the urine sample. A urine culture revealed Streptococcus species. As such, she was given the antibiotic amoxicillin and clavulanic acid, which only partially helped relieve her symptoms. As a result, a pelvic ultrasound was done that showed a right 7‐cm ovarian cyst. For confirmation, the patient visited a different physician who performed another pelvic ultrasound that showed no signs of the previously found ovarian cyst; nonetheless, it showed nonspecific but suspicious bladder findings. This prompted a visit to the urologist, who ordered a computed tomography (CT) scan, which the patient refused to do, and a cystoscopy.
During cystoscopy, due to suspicious and irregularly shaped mucosa, a transurethral resection of bladder tumor (TURBT) was done, and pathology results following surgery revealed SRCC of the bladder. A follow‐up positron emission tomography (PET) scan showed peritoneal carcinomatosis but no evidence of distant metastasis. As a result, a laparotomy was made to debulk the tumor. A second biopsy postlaparotomy also confirmed the results of the previous biopsy.
The patient underwent standard surgical cytoreduction of peritoneal carcinomatosis starting with a midline laparotomy. A systematic exploration of the peritoneal cavity was performed, and intra‐abdominal assessment demonstrated a diffuse distribution without any major vascular structure or deep parenchymal organ invasion, allowing for a complete resection. Debulking proceeded starting with omentectomy and resection of visible peritoneal implants along the anterior abdominal wall. Peritoneal stripping was performed, followed by excision of nodular deposits over the mesenteric surfaces and pelvic peritoneum. The remainder of the procedure followed standard technique, and the patient remained in stable condition.
Tumor cells were negative for CDX‐2 and ER but positive for PDL‐1 with a total proportion score (TPS) of 100% and a combined positive score (CPS) of 100%. Based on the presence of peritoneal carcinomatosis in the absence of nodal disease or distant visceral metastasis, the tumor was staged as T4b N0 M1b, corresponding to Stage IV bladder cancer according to the American Joint Committee on Cancer (AJCC) eighth edition. The patient had firm directives against any further urological surgical procedures, including partial cystectomy (PC) or RC, and elected to proceed with drug therapy as a mainstay treatment option.
After a visit to the oncologist, six‐cycle chemotherapy with cisplatin and Gemzar (gemcitabine) was performed, complicated by symptoms including alopecia and a 12‐kg weight loss. Following chemotherapy, the patient was started on an immunotherapy agent, avelumab, also known as Bavencio, of which she has received 20 out of the expected 36 doses over a period of 18 months. Follow‐up abdominal and pelvic CT imaging demonstrated a reduction in tumor burden following immunotherapy (Figure 1). Cyclic scans are done every 3 months to assess tumor development. The last scan showed improvement and tumor shrinkage compared to previous scans.
CT scan of the pelvis showing the bladder with the signet ring cell carcinoma mass (outlined in red dots) postoperatively upon 20 doses of immunotherapeutic treatment.
3. Discussion
Primary SRCC of the bladder comprises 0.12%–0.6% of bladder malignancies (1). SRCC of the bladder is usually diagnosed at an advanced stage due to its rarity and aggressiveness (7). It can be found in patients of any age (2). However, its incidence increases in patients more than 40 years old, with a male‐to‐female ratio of 2.70–3.20:1 (2). SRCCs are typically found in the stomach, colon, gallbladder, or breast (8). Consequently, primary adenocarcinomas of these organs must be ruled out before the diagnosis of primary SRCC of the bladder (8).
SRCC of the bladder is a rare diagnosis and often presents at an advanced stage, making identification of its risk factors challenging. However, existing literature suggests that advanced age (> 40 years), male sex, and chronic bladder irritation or inflammation, such as cases of recurrent infections or long‐term catheter use, may predispose individuals to bladder adenocarcinomas, including SRCC subtypes (7). Genetic factors are not well defined for primary bladder SRCC, but mucin‐producing adenocarcinomas have been linked to intestinal metaplasia and chronic inflammation, which may lead to malignant transformation (9). Notably, this patient had several risk factors associated with bladder carcinoma, including a significant smoking history of 30 pack‐years, chronic urinary tract infections leading to persistent bladder inflammation, and female sex with multiparity, which may predispose to recurrent urinary dysfunction.
Bladder SRCC presents with hematuria, dysuria, frequent urination, incontinence, or urinary retention (10). These urinary symptoms are similar in all bladder cancers (3). On imaging, SRCC appears as a diffuse wall thickening in the bladder (4). However, on cystoscopy, it may appear as an exophytic growth similar to two‐thirds of other bladder carcinomas (4). In this case, the 54‐year‐old female patient′s high WBC count in urine suggested a possible urinary tract infection. The patient′s persistent urinary incontinence and lower abdominal pain prompted further investigation.
Histologically, these cancers have the appearance of a signet ring due to the accumulation of abundant mucin in the cytoplasm, leading to nuclei dislocation to the periphery (11). In this case, SRCC of the bladder was confirmed via biopsy and immunohistochemical staining. However, metastatic tumors from the gastrointestinal tract (GIT) should be eliminated before confirming the diagnosis of primary SRCC of the bladder (4). The immunostainings overlap between the GIT and bladder primary SRCC (4). Both are positive for CK7, CK20, CEA, EMA, and CDX2 (4). Nonetheless, ruling out endoscopically any GIT lesion and the absence of nuclear positivity for β‐catenin favors primary SRCC of the bladder (5).
The management of primary SRCC of the bladder is challenging. Surgeries such as TURBT, PC, and RC are the first treatment approach (2, 12). RC is the method of choice; however, TURBT and PC are beneficial in localized tumors (2). Although SRCC is found to be resistant to the standard chemotherapy regimens and radiotherapy used for advanced bladder carcinoma, the patient was followed by adjuvant chemotherapy with cisplatin and gemcitabine (6).
Although systematic reviews and large comparative analyses are lacking, most case reports described primary bladder SRCC as a biologically aggressive and highly lethal tumor. For instance, Jin et al. contrasted SRCC with more common urothelial carcinomas (UCs), stating that the prognosis of SRCC is poorer than that of UC, even after adjustment for patient baseline demographic and clinicopathological characteristics, as well as cancer treatment (13). SRCC often presents in advanced stages and exhibits resistance to conventional therapy.
This case emphasizes the importance of early recognition of primary SRCC of the bladder, especially in females. Bladder primary SRCC′s delayed diagnosis, high mortality, and poor prognosis underscore the need for a multidisciplinary team, including urologists, oncologists, and pathologists, to diagnose and efficiently treat it. Table 1 summarizes selected published cases, highlighting variations in patient demographics, presenting symptoms, disease stage, treatment approaches, and outcomes.
4. Conclusion
This case illustrates the diagnostic and therapeutic challenges of primary SRCC of the bladder, a malignancy often misdiagnosed as other benign urinary conditions. The patient′s initial misdiagnosis underscores the importance of considering SRCC in refractory urinary symptoms, particularly in older adults. Immunohistochemistry, such as PD‐L1 positivity, and imaging play important roles in confirming diagnosis and guiding therapy.
While SRCC carries a poor prognosis due to its aggressive nature and resistance to many conventional therapies, this case demonstrates that multidisciplinary management, such as combining surgery, chemotherapy, and immunotherapy, can achieve meaningful responses. Future efforts should focus on standardized diagnostic criteria and novel targeted therapies to improve survival in this highly fatal disease.
NomenclatureSRCCprimary signet ring cell carcinomaIHCimmunohistochemistryPD‐L1programmed death‐ligand 1CDX‐2caudal type homeobox 2ERestrogen receptorTURBTtransurethral resection of bladder tumorPETpositron emission tomographyTPStotal proportion scoreCPScombined positive scoreGemzargemcitabineGITgastrointestinal tractCK7cytokeratin 7CK20cytokeratin 20CEAcarcinoembryonic antigenEMAepithelial membrane antigenPCpartial cystectomyRCradical cystectomyWBCswhite blood cells
Ethics Statement
This case report was reviewed and approved by the Institutional Review Board (IRB) of the University of Balamand, and written informed consent was obtained from the patient for the publication of this case report. All procedures followed were in accordance with the ethical standards of the responsible committee and with the Declaration of Helsinki.
Disclosure
All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Conception, organization, and writing of the first draft: J.P.J., K.K.K., and J.G. Writing of the first draft and editing: J.P.J., K.K.K., and J.G. Conception and design and review/editing of the manuscript: A.K. Review/editing: H.E.G., J.P.J., K.K.K., and J.G. contributed equally to these studies.
Funding
This work did not receive specific funding.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ivanov A. , Antonov P. , Zapryanov M. , Uchikov P. , and Belovezhdov V. , Primary Signet-Ring Cell Adenocarcinoma of the Bladder-A Case Report and Review of Literature, Urology Case Reports. (2022) 42, 102022, 10.1016/j.eucr.2022.102022.35530556 PMC 9073209 · doi ↗ · pubmed ↗
- 2Akamatsu S. , Takahashi A. , Ito M. , and Ogura K. , Primary Signet-Ring Cell Carcinoma of the Urinary Bladder, Urology. (2010) 75, no. 3, 615–618.19819534 10.1016/j.urology.2009.06.065 · doi ↗ · pubmed ↗
- 3Stephen L. , Taylor S. S. , and Narothama A. , Bladder Cancer, 2024, Available from:https://www.ncbi.nlm.nih.gov/books/NBK 536923/.
- 4Benerjee N. , Parmar K. , and Vaiphei K. , Primary Signet-Ring Cell Carcinoma of the Urinary Bladder, Autops Case Rep. (2021) 11, e 2021264, 10.4322/acr.2021.264.33968831 PMC 8087395 · doi ↗ · pubmed ↗
- 5Thomas A. A. , Stephenson A. J. , Campbell S. C. , Jones J. S. , and Hansel D. E. , Clinicopathologic Features and Utility of Immunohistochemical Markers in Signet-Ring Cell Adenocarcinoma of the Bladder, Human Pathology. (2009) 40, no. 1, 108–116.18789486 10.1016/j.humpath.2008.06.022 · doi ↗ · pubmed ↗
- 6Xie Y. , Zhang Y. , Du Z. , Liu D. , Yan W. , Liu Y. , and Ping H. , Treatment Options for Signet Ring Cell Carcinoma of the Urinary Bladder: A Population-Based Study, Cancer Control. (2024) 31, 10.1177/10732748241278485, 39159955.PMC 1133414139159955 · doi ↗ · pubmed ↗
- 7Hong X. , Wang T. , Liu Q. , Bi J. , and Li H. , Primary Signet-Ring Cell Carcinoma of the Urinary Bladder – A Rare Bladder Tumor, Clinics [Internet]. (2024) 79, 100500, 10.1016/j.clinsp.2024.100500, 39316894.39316894 PMC 11462279 · doi ↗ · pubmed ↗
- 8Sarı H. , Uysal F. Ş. , Ekenci B. Y. , Bozpınar S. , Çimen S. , and İmamoğlu M. A. , Rare Primary Signet Ring Cell Carcinoma of the Bladder Cancer, Bulletin of Urooncology. (2023) 22, no. 1, 42–45, 10.4274/uob.galenos.2022.2022.6.2. · doi ↗