Epidemiology, Management, and Outcomes of Patients Hospitalized With Community-Acquired Infection in a Resource-Limited Setting in Southeast Asia: A Prospective Observational Study
Rungnapa Phunpang, Prapassorn Poolchanuan, Taylor D Coston, Adul Dulsuk, Sopha Saeyang, Boonthanom Moonmueangsan, Narongchai Sangsa, Sermchart Chinnakarnsawas, Rachan Janon, T Eoin West, Narisara Chantratita, Shelton W Wright

TL;DR
This study examines sepsis and infection outcomes in hospitalized patients in rural Southeast Asia, highlighting high mortality and unique tropical pathogens.
Contribution
The study provides new insights into sepsis epidemiology and management in a resource-limited setting in Southeast Asia.
Findings
Sepsis was diagnosed in 66% of hospitalized patients with community-acquired infection.
Sepsis-associated acute kidney injury was independently linked to higher mortality.
Tropical infections like melioidosis and leptospirosis were notable etiologies.
Abstract
In many resource-limited settings, hospitalization for community-acquired infection is common, but data regarding illness severity, etiology, and morbidity remain sparse. We conducted a prospective observational study from May 2022 to August 2023 at 2 hospitals in northeast Thailand. Adults hospitalized with community-acquired infection were enrolled within 24 hours of admission and followed up to 28 days. We identified patients meeting sepsis criteria and assessed related epidemiology, management, and mortality risk factors. Of 1445 patients screened, 940 were enrolled. The median age was 60 years and preexisting diabetes mellitus was common (42%). Sixty-six percent of patients met sepsis criteria. Blood cultures and broad-spectrum antibiotics on admission were common (both >95%), although lactate measurement was performed in 43% of patients with sepsis. In patients with sepsis,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
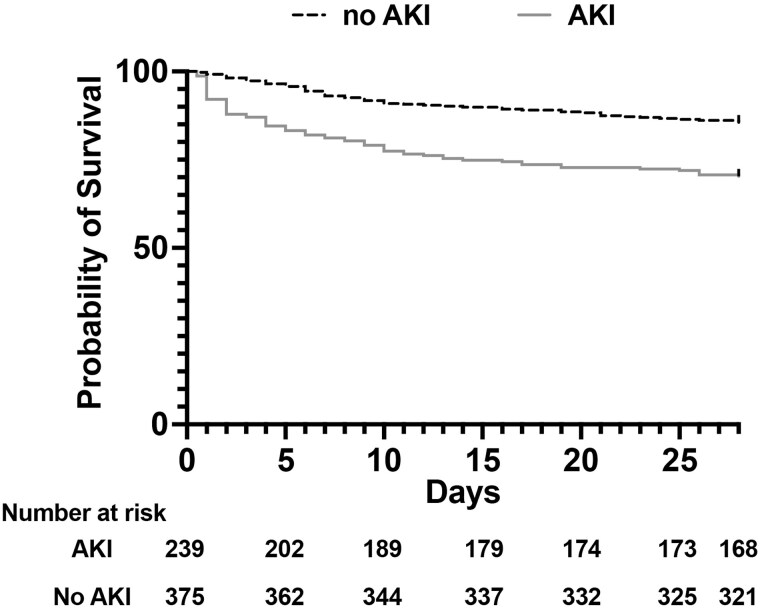 Figure 1
Figure 1| Median (IQR) or No. (%) | ||||
|---|---|---|---|---|
| Characteristics | Entire Cohort (N = 940) | Sepsis | Nonsepsis (n = 322) |
|
| Demographics | ||||
| Age, y | 60 (49–70) | 61 (50–72) | 57 (46–68) | <.001 |
| Female sex | 389 (41) | 233 (38) | 156 (49) | <.01 |
| Rainy season presentation | 614 (65) | 390 (63) | 224 (70) | .05 |
| Preexisting conditions | ||||
| Charlson Comorbidity Index | 2 (1–4) | 3 (1–4) | 2 (1–3) | <.001 |
| Diabetes mellitus | 396 (42) | 243 (39) | 153 (48) | .02 |
| Hypertension | 356 (38) | 240 (38) | 116 (36) | .40 |
| Chronic kidney disease | 139 (15) | 115 (19) | 24 (8) | <.001 |
| Dyslipidemia | 97 (10) | 60 (10) | 37 (12) | .39 |
| Stroke | 60 (6) | 45 (7) | 15 (5) | .12 |
| Chronic lung disease | 55 (6) | 34 (6) | 20 (6) | .73 |
| Chronic cardiovascular disease | 41 (4) | 36 (6) | 5 (2) | <.01 |
| Chronic steroid use | 34 (4) | 22 (4) | 12 (4) | .90 |
| Cancer | 24 (3) | 17 (3) | 7 (2) | .59 |
| Chronic liver disease | 24 (3) | 24 (4) | 0 | <.001 |
| HIV | 17 (2) | 12 (2) | 5 (2) | .68 |
| Rheumatologic disorders | 16 (2) | 12 (2) | 4 (1) | .43 |
| Hospitalization | ||||
| Referral from another facility | 416 (44) | 350 (57) | 66 (21) | <.001 |
| Days to referral | 0 (0–0) | 0 (0–0) | 0 (0–0) | .93 |
| Admission ward | ||||
| Medical | 810 (86) | 509 (82) | 301 (93) | <.001 |
| Surgical | 28 (3) | 9 (2) | 19 (6) | |
| Intensive care unit | 102 (11) | 100 (16) | 2 (1) | |
| Length of hospitalization, d | 6 (3–13) | 6 (3–13) | 5 (3–11) | <.001 |
| Procedural drainage-debridement | 87 (9) | 56 (9) | 31 (10) | .78 |
| Presenting clinical syndromes | ||||
| Pneumonia | 354 (38) | 272 (44) | 82 (26) | <.001 |
| Acute febrile illness | 204 (22) | 110 (18) | 94 (29) | <.001 |
| Gastrointestinal illness | 132 (14) | 81 (13) | 51 (16) | .25 |
| Skin or soft tissue infection | 27 (3) | 14 (2) | 13 (4) | .12 |
| Urinary tract infection | 73 (8) | 48 (8) | 25 (8) | .99 |
| Intracranial infection | 4 (0) | 3 (1) | 1 (0) | .7 |
| Abscess | 33 (4) | 14 (2) | 19 (6) | <.01 |
| No. (%) or Median (IQR) | ||||
|---|---|---|---|---|
| Characteristic | Entire Cohort (N = 940) | Sepsis (n = 618) | Nonsepsis (n = 322) |
|
| Admission management | ||||
| Blood cultures sent on admission | 902 (96) | 596 (96) | 306 (95) | .30 |
| Antibiotics received on admission | 917 (98) | 604 (98) | 313 (97) | .62 |
| Broad gram-negative coverage | 912 (97) | 603 (98) | 309 (96) | .17 |
| MRSA coverage | 185 (20) | 126 (20) | 59 (18) | .45 |
| Duration, d | 6 (3–12) | 6 (3–13) | 4 (3–11) | .002 |
| Lactate measured on admission | 302 (32) | 264 (43) | 38 (12) | <.001 |
| Admission illness characteristics | ||||
| SOFA | 3 (1–7) | 5 (3–9) | 0 (0–1) | <.001 |
| qSOFA | 1 (1–2) | 2 (1–2) | 1 (0–1) | <.001 |
| Acute kidney injury | 261 (28) | 239 (39) | 22 (7) | <.001 |
| Outcomes during hospitalization | ||||
| Mechanical ventilation | 322 (34) | 315 (51) | 7 (2) | <.001 |
| Vasoactive medication | 275 (29) | 267 (43) | 8 (3) | <.001 |
| New kidney replacement therapy | 44 (5) | 43 (7) | 1 (0) | <.001 |
| Intermittent hemodialysis | 44 (5) | 43 (7) | 1 (0) | <.001 |
| Peritoneal dialysis | 0 | 0 | 0 | |
| Mortality outcomes | ||||
| 7 d | 78 (8) | 75 (12) | 3 (1) | <.001 |
| Days to death | 2 (1–5) | 2 (1–5) | 5 (1–6) | .35 |
| 28 d | 132 (14) | 125 (20) | 7 (2) | <.001 |
| Days to death | 6 (2–13) | 6 (2–12) | 20 (6–23) | .10 |
| Lost to 28-d follow-up | 6 (1) | 4 (1) | 2 (1) | >.99 |
| Characteristic | Entire Cohort (N = 940) | Sepsis (n = 618) | Nonsepsis (n = 322) |
|
|---|---|---|---|---|
| Bloodstream infection | 164 (18) | 130 (21) | 34 (10) | <.001 |
| Gram-negative bacteremia | 133 (14) | 102 (17) | 31 (10) | .004 |
| | 58 (6) | 43 (7) | 15 (5) | .17 |
| | 39 (4) | 27 (4) | 12 (4) | .64 |
| | 21 (2) | 16 (3) | 5 (2) | .37 |
| | 3 (0) | 3 (1) | 0 | .56 |
| | 5 (1) | 5 (1) | 0 | .17 |
| | 5 (1) | 5 (1) | 0 | .17 |
| | 2 (0) | 2 (0) | 0 | .55 |
| | 1 (0) | 1 (0) | 0 | >.99 |
| | 1 (0) | 1 (0) | 0 | >.99 |
| Gram-positive bacteremia | 32 (3) | 29 (5) | 3 (1) | .002 |
| | 11 (1) | 10 (2) | 1 (0) | .11 |
| | 4 (0) | 4 (1) | 0 | .31 |
| | 6 (1) | 5 (1) | 1 (0) | .67 |
| Group G | 3 (0) | 3 (1) | 0 | .56 |
| Group D | 2 (0) | 2 (0) | 0 | .55 |
| Other | 2 (0) | 2 (0) | 0 | .55 |
| | 4 (0) | 3 (1) | 1 (0) | .67 |
| Polymicrobial | 5 (1) | 4 (1) | 1 (0) | >.99 |
| Contaminant organisms | 35 (4) | 28 (5) | 7 (2) | .07 |
| Other infectious etiologies | ||||
| Leptospirosis | 36 (4) | 33 (5) | 3 (1) | <.001 |
| Acute tuberculosis disease | 24 (3) | 10 (2) | 14 (4) | .02 |
| Nonbacteremic melioidosis | 20 (2) | 12 (2) | 8 (3) | .64 |
| Scrub typhus | 14 (2) | 12 (2) | 2 (1) | .16 |
| Dengue | 7 (1) | 4 (1) | 3 (1) | .70 |
| Malaria | 1 (0) | 1 (0) | 0 | >.99 |
| Median (IQR) or No. (%) | ||||
|---|---|---|---|---|
| Characteristic | All Sepsis (n = 618) | ICU (n = 174) | Ward (n = 444) |
|
| Severity of illness at enrollment | ||||
| SOFA | 5 (3–9) | 10 (7–13) | 4 (3–6) | <.001 |
| APACHE II | … | 22 (17–25) | … | … |
| Acute kidney injury | 239 (39) | 94 (53) | 145 (33) | <.001 |
| Critical care at enrollment | ||||
| Respiratory failure | 306 (50) | 159 (90) | 147 (33) | <.001 |
| Mechanical ventilation | 277 (45) | 156 (89) | 121 (27) | <.001 |
| Vasoactive medications | 198 (32) | 106 (60) | 92 (21) | <.001 |
| New kidney replacement therapy | 15 (3) | 13 (7) | 2 (1) | <.001 |
| Admission management | ||||
| Blood cultures sent | 596 (96) | 172 (99) | 424 (96) | .05 |
| Antibiotics received | 604 (98) | 172 (99) | 432 (97) | .37 |
| Procedural drainage/debridement | 56 (9) | 16 (9) | 40 (9) | .94 |
| Lactate concentration measured | 264 (43) | 96 (55) | 168 (38) | <.001 |
| Death | ||||
| 7 d | 75 (12) | 38 (22) | 37 (8) | <.001 |
| Days to death | 2 (1–5) | 2 (1–5) | 3 (1–5) | .48 |
| 28 d | 125 (20) | 60 (34) | 65 (15) | <.001 |
| Days to death | 6 (2–12) | 5 (1–12) | 6 (2–13) | .34 |
| Lost to 28-d follow-up | 4 (1) | 0 | 4 (1) | .58 |
| Unadjusted | Adjusted | |||
|---|---|---|---|---|
| Variable | OR (95% CI) |
| OR (95% CI) |
|
| Preexisting conditions | ||||
| HIV | 4.06 (1.28–12.8) | .02 | 5.28 (1.82–15.3) | .002 |
| Presenting clinical/laboratory data | ||||
| Heart rate | 1.03 (1.02–1.04) | <.001 | 1.03 (1.02–1.04) | <.001 |
| Blood urea nitrogen | 3.87 (1.99–7.51) | <.001 | 2.21 (.98–4.97) | .06 |
| Hemoglobin | 0.90 (.83–.97) | <.001 | 0.83 (.76–.92) | <.001 |
| Presenting characteristics | ||||
| Acute kidney injury | 2.51 (1.68–3.75) | <.001 | 2.07 (1.30–3.29) | .002 |
| Respiratory failure | 3.64 (2.35–5.64) | <.001 | 2.34 (1.42–3.86) | .001 |
- —US National Institutes of Health10.13039/100000002
- —Firland Foundation10.13039/100005815
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBurkholderia infections and melioidosis · Leptospirosis research and findings · Clostridium difficile and Clostridium perfringens research
Sepsis disproportionally affects low- and middle-income countries (LMICs), with millions of estimated deaths annually [1]. In tropical regions of Southeast Asia, sepsis-related morbidity is particularly high and caused by a diverse group of pathogens [2]. The heterogeneity and global variation in this disease therefore necessitate further study to develop contextualized and comprehensive management plans [3].
The Third International Consensus Definition for Sepsis defined sepsis as infection-related host response dysregulation leading to organ dysfunction [4]. Implicit in this definition were measures of organ dysfunction typically requiring critical care interventions. As such, many studies of sepsis have focused on patients in the intensive care unit (ICU), even though patients with sepsis may be identified outside of such settings [5]. Furthermore, in resource-limited settings, patients frequently do not have access to critical care, or they receive critical care outside an ICU, requiring modifications of traditional management approaches [6, 7].
Studies of patients hospitalized with community-acquired infection are limited in Southeast Asia, despite its high estimated burden and unique tropical etiologies. Several regional studies of patients with suspected or confirmed sepsis in large academic or referral centers may miss broader populations of patients who are infected [2, 8]. Therefore, in this study, we sought to identify the frequency of sepsis among a large, prospectively enrolled cohort of patients admitted for community-acquired infection at 2 rural hospitals in northeast Thailand. We then assessed the causative infectious etiologies, management, risk factors, and infection-related outcomes in this unique and understudied population.
METHODS
Study Design, Participants, and Outcomes
We conducted a prospective observational study at 2 hospitals in northeastern Thailand from May 2022 through August 2023. Patients hospitalized at Mukdahan Hospital, Mukdahan province, Thailand, and Roi Et Hospital, Roi Et province, Thailand, were screened within 24 hours of hospital admission to determine if they met enrollment criteria of age ≥18 years and a primary admission diagnosis of suspected or confirmed infection. Exclusion criteria, regional and site information, and additional study design are available in the supplemental methods. Enrolled patients were then subsequently followed during their hospitalization. All patients, including postdischarge, were followed to or contacted at 28 days following enrollment to determine death after discharge. Discharged patients not contacted were not included in analyses related to 28-day mortality.
Definitions
Sepsis was defined in accordance with the Third International Consensus Definition for Sepsis [4]. A Sequential Organ Failure Assessment (SOFA) score was calculated by parameters within the first 24 hours of admission, and sepsis was defined as patients with suspected infection and a SOFA score ≥2. Modifications to the respiratory component of the SOFA score were necessary as arterial blood gas measurement is uncommon. For patients without an available partial pressure of arterial oxygen (PaO_2_), a ratio of the pulse-oximetric oxygen saturation to the fraction of inspired oxygen (SpO_2_/FiO_2_) was calculated for patients with an SpO_2_ <98% [9, 10]. As previously reported, including adoption in resource-constrained settings, SpO_2_/FiO_2_ equivalents for the SOFA PaO_2_/FiO_2_ cutoffs were calculated by the following equation: SpO_2_/FiO_2_ = 64 + [0.84 × (PaO_2_/FiO_2_)] [11, 12]. Otherwise, patients who were intubated or mechanically ventilated with SpO_2_ >98% and no available PaO_2_ were given a default respiratory SOFA score of 2 out of 4 (Supplementary Table 1) [8]. A Glasgow Coma Scale score was recorded at enrollment by the study team. To maintain consistency with prior sepsis investigations, when score components were not available (Supplementary Table 2), they were assumed to be normal [1, 13]. The dates of receipt of antibiotics, blood cultures, and lactate were available but not the minute/hour. Therefore, timing of sepsis bundles was limited to the calendar day of admission.
Acute kidney injury (AKI) was determined by criteria from the 2012 Kidney Disease: Improving Global Outcomes guidelines [14]. AKI was defined as a creatinine value within 24 hours of admission ≥150% of a baseline creatinine. If a baseline creatinine value was not available, an estimated value was calculated in patients without known chronic kidney disease per the “modification of diet in renal disease” equation, with an estimated glomerular filtration rate of 75 mL/min/1.73 m^2^. In all patients not requiring baseline peritoneal dialysis or hemodialysis, an increase in creatinine by 0.3 mg/dL during the first 48 hours of admission was also classified as AKI. Urine output was not available and so not included in the AKI definition. Additional definitions related to critical illness, presenting clinical syndromes, and infectious disease diagnoses can be found in the supplemental methods.
Statistical Analyses
Data were summarized by proportions for discrete variables and median (IQR) for continuous variables. Differences in proportions and medians between groups were assessed by χ^2^ and the Mann-Whitney test, respectively. To identify risk factors of 28-day mortality, 44 clinical characteristics available at enrollment were a priori identified. In univariate analyses, the association of each variable with 28-day mortality was calculated by logistic regression. To identify a set of variables for inclusion in multivariable models, all 44 clinical variables were subjected to logistic regression analysis by least absolute shrinkage and selection operator (LASSO) methodology, in which lambda was selected by the bayesian information criterion. The selected risk factors were confirmed with the lambda that minimizes the minimal mean squared prediction error [15]. The LASSO-identified risk factors were then assessed for their association with 28-day mortality in multivariable models, which included enrollment site. Curves for 28-day survival were compared via the log-rank test. P values <.05 were considered significant. Analyses were performed in Stata/SE version 14.2.
Patient Consent Statement
Written informed consent was obtained from all study participants or their surrogate decision makers. The study was approved by the ethics committees of Mukdahan Hospital (MEC 09/64), Roi Et Hospital (RE035/2564), the Mahidol University Faculty of Tropical Medicine (MUTM 2021-043-01), and the University of Washington (STUDY00012758).
RESULTS
Cohort Characteristics
Of 1445 patients screened, 940 were enrolled and included in analyses (Supplementary Figure 1). Enrolled patients were predominantly male (551/940, 59%) with a median age of 60 years (IQR, 49–70; Table 1, Supplementary Table 3). Notably, diabetes mellitus was common (396/940, 42%), and 44% (416/940) of patients were referred from another facility, typically on the same day as initial presentation. A total of 618 (66%) patients met sepsis criteria within 24 hours of admission. Patients with sepsis at enrollment tended to have more comorbidities vs those without sepsis by Charlson Comorbidity Index (P < .001), although diabetes mellitus was more common in patients without sepsis (P = .02). Patients with sepsis were more likely to have an admission diagnosis of pneumonia (272/618, 44%) than those without sepsis (82/322, 26%; P < .001). Conversely, patients with sepsis were less likely to have an admission diagnosis of an acute febrile illness (sepsis, 110/618, 18%; nonsepsis, 94/322, 29%; P < .001).
Initial Management and Outcomes by Sepsis Classification
On admission to the study hospitals, blood cultures were sent on 96% of patients (902/940; Table 2, Supplementary Table 4). Antibiotics were frequently given on admission (917/940, 98%) and overwhelmingly included broad gram-negative coverage (912/940, 97%). Ceftazidime and ceftriaxone were the most frequently received antibiotics at the study hospitals or referring sites (Supplementary Table 5). Antibiotics started on admission were continued for a median 6 days (sepsis, 6 days [IQR, 3–13]; nonsepsis, 4 days [IQR, 3–11]; P = .002). Finally, lactate was measured for 32% (302/940) of patients on admission and was more frequently measured for patients with sepsis as opposed to those without (264/618 [43%] vs 38/322 [12%]; P < .001). Given the inconsistency of lactate measurement, adherence to the recommended sepsis bundle on admission (blood cultures, antibiotics, and lactate measurement) per the 2021 Surviving Sepsis Campaign (SSC) occurred in only 41% of patients with sepsis (255/618) [16].
A total of 132 patients (14%) died within 28 days after enrollment (Table 2, Supplementary Table 4). Highlighting local cultural practices, 67 (51%) of those who died by 28 days were discharged from the hospital prior to their death, and 41 (62%) died within 1 day of discharge. Death within 28 days of enrollment was more common in patients with sepsis (125/618, 20%) than those without sepsis (7/322, 2%; P < .001). Out of 940 enrolled patients, 6 were lost to follow-up at 28 days after enrollment.
Infectious Diseases by Sepsis Classification
We next characterized the infectious diseases represented in the cohort (Table 3, Supplementary Table 6). Overall, 18% (164/940) had a positive blood culture from admission. Bacteremia was more common in patients with sepsis (130/618, 21%) than those without sepsis (34/322, 10%; P < .001). Gram-negative bacteria accounted for most positive blood cultures (133/164, 81%), including patients with sepsis (102/130, 78%) and without (31/34, 91%). Burkholderia pseudomallei, the antibiotic-resistant bacteria endemic in northeast Thailand and the cause of the severe tropical infection melioidosis, was the most common bacteria identified in blood cultures. We compared other tropical infectious diseases based on final hospital diagnosis. Leptospirosis was diagnosed in 36 of 940 (4%) patients, with 92% (33/36) meeting sepsis criteria. Other infectious diseases were diagnosed in the cohort, such as acute tuberculosis (24/940, 3%), scrub typhus (14/940, 2%), dengue (7/940, 1%), and nonbacteremic melioidosis (20/940, 2%). Notably, no specific bacteremia pathogen differed by sepsis category, and the majority of the cohort did not have a specific infectious etiology identified.
Critical Illness in Sepsis
As many patients in resource-limited settings receive medical care outside of traditional ICUs, we next sought to characterize the medical management of patients with sepsis inside and outside the ICU (Table 4). In 618 patients with sepsis, 176 (28%) were initially admitted to an ICU while 444 (72%) were admitted to a ward. Notably, critical care was still common in patients with sepsis outside the ICU, as 27% (121/444) required mechanical ventilation and 21% (92/444) required vasoactive medications within 24 hours of admission. Patients with sepsis initially admitted to the ICU had higher 28-day mortality (34%) and frequency of AKI on admission (54%) as compared with those with critical illness but admitted to the medical ward (19% [P = .001] and 38% [P = .002], respectively; Supplementary Table 7).
Risk Factors of 28-Day Mortality in Sepsis
Finally, we investigated whether specific risk factors present at enrollment were associated with 28-day mortality in patients with sepsis (Supplementary Tables 8 and 9). Using 44 routinely obtained enrollment variables, such as patient characteristics, vital signs, and laboratory data (Supplementary Table 10), we performed a LASSO regression to identify a parsimonious set of variables associated with 28-day sepsis mortality. Six variables were identified, and all were associated with 28-day sepsis mortality in unadjusted models (Table 5). In a multivariable model including enrollment site, 5 risk factors were associated with an increased risk of 28-day sepsis mortality (all P < .01; Table 5): a preexisting HIV diagnosis, higher heart rate, lower hemoglobin, respiratory failure, and AKI (adjusted odds ratio, 2.07; 95% CI, 1.30–3.29; P = .002). As 39% (239/618) of patients with sepsis had AKI at enrollment, we next looked at the outcomes of sepsis cases with and without AKI. In patients with sepsis-associated AKI (SA-AKI), 15% (35/239) required kidney replacement therapy (KRT) during their hospitalization, and 30% (71/239) died within 28 days as compared with 14% (54/375) without AKI (P < .001). Finally, patients with sepsis with AKI at enrollment had significantly worse survival over 28-days when compared those without AKI (P < .001; Figure 1).
Survival curve of sepsis cases with and without AKI. Kaplan-Meier survival curves over 28 days demonstrate worse survival in patients with sepsis-associated AKI (gray) at enrollment vs those without AKI (black dashed; P < .001, log-rank test). AKI, acute kidney injury.
DISCUSSION
This observational prospective cohort study is one of the largest multicenter studies of patients hospitalized with suspected community-acquired infection in a resource-limited setting, including Southeast Asia. We report that sepsis is common in this cohort, is caused by different pathogens as compared with high-income country (HIC) settings, and is associated with significant mortality. Furthermore, we report that critical illness is not only common but also frequently managed outside a traditional ICU. Finally, we identify SA-AKI as a significant risk factor for sepsis mortality.
Limited prospective data exist regarding the frequency of sepsis among patients hospitalized for community-acquired infection in resource-limited settings. Previously reported large prospective studies in Southeast and South Asia enrolled patients with suspected or confirmed sepsis, often only in ICUs, limiting broader application in the region [2, 5, 8, 17]. In HIC settings, 25% to 44% of patients presenting to emergency departments with community-acquired infection typically meet criteria for sepsis [18, 19]. However, in our study, 66% of patients hospitalized with community-acquired infection met sepsis criteria. Notably, patients in this study frequently received mechanical ventilation and vasoactive medications outside the ICU. These findings confirm the frequency of sepsis in this region but also highlight the challenges of applying traditional definitions of sepsis to locations with resource limitations [20, 21]. Additionally, our findings suggest that prospective enrollment of patients with sepsis in an ICU may miss patients meeting sepsis criteria and those with critical illness in similar settings. Whether patients outside the ICU requiring mechanical ventilation or vasoactive medications may benefit from an early escalation of care is unknown, although only 4% of those initially admitted to the ward with sepsis were eventually transferred to the ICU, despite a 15% mortality rate. In the United States, admission to the ward rather than the ICU may be associated with improved outcomes among patients with sepsis not requiring life support [22]. However, the 2021 SSC guidelines recommend ICU admission within 6 hours for patients requiring critical care, and early ICU transfer is associated with improved mortality in sepsis [16, 23]. In resource-limited settings where ICU transfer may not be possible for all patients who are critically ill, further study is necessary to determine the optimal management strategy and outcome effect of critical care outside the ICU.
According to the 2021 SSC guidelines, early empiric broad-spectrum antibiotics and blood cultures are recommended for patients with community-acquired sepsis [16]. Sepsis bundles have been widely implemented in Thailand, although usage varies countrywide [24]. Reflecting this, nearly all patients in our cohort received empiric antibiotics and had blood cultures sent at admission. Conversely, lactate measurement was less common, occurring in less than half of patients with sepsis. Lactate levels are associated with sepsis mortality, including that in northeast Thailand, and its measurement is recommended in the SSC hour 1 sepsis bundle [16, 25]. A recent multinational study of patients with sepsis admitted to tertiary ICUs throughout Asia reported poor compliance with 1- and 3-hour sepsis bundles [17]. However, the utility of lactate levels to guide resuscitation in patients with sepsis is unknown in LMICs and remains a topic of debate in HICs [26, 27]. Therefore, further study is necessary to determine whether broader adoption of SSC bundles is cost-efficient and improves outcomes in similar settings.
The adoption of broad, early empiric antibiotics in patients with suspected infection may contribute to antibiotic resistance, a growing concern in LMICs, including Thailand [28, 29]. Indeed, in northeast Thailand, antimicrobial-resistant infections, such as Escherichia coli, Klebsiella species, and Acinetobacter species, are associated with excess mortality in hospitalized patients [30]. Given this concern, the necessity of broad empiric gram-negative antibiotics in hospitalized patients in HICs has become a matter of debate [31]. In our cohort, nearly all patients, regardless of illness severity or sepsis status, received broad gram-negative coverage at admission, most commonly with ceftazidime, a third-generation cephalosporin with antipseudomonal activity, similar to prior reports in the region [32]. This approach may reflect the high frequency of gram-negative bacteremia in our cohort, a trend noted across Southeast and South Asia but distinct from many HICs [2, 5, 8, 33]. Empiric antibiotics were not discontinued quickly, as the median antibiotic duration was 6 days in patients with sepsis and 4 days in those without sepsis. Therefore, it is possible that in some patients, particularly those without sepsis and negative cultures, empiric antibiotics could have been avoided or coverage de-escalated quickly. As sepsis management in tropical settings continues to evolve, the evolution of antimicrobial stewardship programs, including biomarker-based or other de-escalation protocols, may be a reasonable approach to help address the potential for future antimicrobial resistance [7, 34].
Reflecting the increasing prevalence of diabetes mellitus in Asia, 42% of enrolled patients in this cohort had a preexisting diagnosis of diabetes [35]. The high prevalence of diabetes among patients with sepsis has been described in similar large sepsis studies in the region [2, 5, 8, 17]. In Thailand, diabetes associated with poor glycemic control is particularly prevalent in the northeast region of the country [36]. Additionally, diabetes is a major risk factor for melioidosis, perhaps reflecting the high rates of that disease in our cohort [37]. As diabetes prevalence increases in lower-resourced tropical settings, particular attention needs to be paid to how this demographic change may affect infection etiologies and management.
An intriguing finding in our study relates to the frequency and importance of SA-AKI. AKI at enrollment was common in patients with sepsis and independently associated with 28-day mortality. The burden of AKI is particularly high in LMICs, where an estimated 85% of global cases occur [38]. However, access to KRT is often limited in these settings, and continuous KRT is frequently restricted to urban quaternary facilities [39]. Only limited intermittent hemodialysis was available at the study hospitals in our report, although 15% of patients with SA-AKI at enrollment received this intervention during their hospitalization. The incidence of KRT in SA-AKI has frequently been reported as >20%, so it is possible that KRT usage would have been higher in our cohort with greater access [39, 40]. Notably, some tropical infections, including those common in rural Southeast Asia, such as leptospirosis and melioidosis, are associated with particularly increased risks of AKI [41, 42]. While it is unclear whether SA-AKI is preventable, optimized management may reduce the risk of disease progression [43]. Additionally, recent reports have identified subphenotypes of HIC AKI cases with potentially unique responses to therapeutic interventions [44]. Critically, few studies have assessed the epidemiology of SA-AKI in resource-constrained settings globally, including Southeast Asia [45]. Given the prevalence and importance of this sepsis-associated disease, further contextualized consideration of SA-AKI in global settings is urgently needed.
This study has several strengths. To our knowledge, this is the largest multicenter prospective cohort study of patients hospitalized with community-acquired infection in a resource-limited setting. Our study included all-cause 28-day mortality, important given the local culture practice of discharging moribund patients to die at home, with minimal loss to follow-up. Study data were collected by a trained study team, yielding minimal missing data. Additionally, strict, broadly accepted definitions were used to define patients with sepsis and AKI.
Our study also has several limitations. Highlighting the resource constraints of the study hospitals, arterial blood gases were not routinely obtained, requiring modification of SOFA. Additionally, the timing of specific interventions, including antibiotics, was not available on a minute or hour level of specificity, rather the calendar day. Identification of infectious etiologies was limited to the testing performed at the study hospitals and did not include prospective specific pathogen testing. Antibiotic susceptibility data were not available either. Both study hospitals were referral hospitals within their rural provinces; therefore, care delivery may have differed among hospitals and may have been affected by the prospective study design. Additionally, patient demographics and management may differ as compared with local health care centers or larger academic quaternary care centers within Thailand and other global settings. The study was also conducted over a 16-month period and may not completely reflect the seasonal variations of some infections; moreover, it did not enroll patients infected with SAR-CoV-2.
In conclusion, sepsis and sepsis-associated critical illness are common and associated with mortality in adults with community-acquired infection in rural Southeast Asia. SA-AKI on presentation was associated with an increased risk of mortality. Given the paucity of high-quality existing data on sepsis in resource-constrained settings, this study provides critical and timely data to inform future clinical and research approaches in global settings.
Supplementary Material
ofag022_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rudd KE, Seymour CW, Aluisio AR, et al Association of the quick Sequential (Sepsis-Related) Organ Failure Assessment (q SOFA) score with excess hospital mortality in adults with suspected infection in low- and middle-income countries. JAMA 2018; 319:2202–11.29800114 10.1001/jama.2018.6229 PMC 6134436 · doi ↗ · pubmed ↗
- 2Sudarmono P, Aman AT, Arif M, et al Causes and outcomes of sepsis in Southeast Asia: a multinational multicentre cross-sectional study. Lancet Glob Health 2017; 5:e 157–67.28104185 10.1016/S 2214-109X(17)30007-4PMC 5332551 · doi ↗ · pubmed ↗
- 3Cummings MJ, Jacob ST. Equitable endotyping is essential to achieve a global standard of precise, effective, and locally-relevant sepsis care. E Bio Medicine 2022:86:104348.36470830 10.1016/j.ebiom.2022.104348 PMC 9782810 · doi ↗ · pubmed ↗
- 4Singer M, Deutschman CS, Seymour C, et al The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016; 315:801–10.26903338 10.1001/jama.2016.0287 PMC 4968574 · doi ↗ · pubmed ↗
- 5Virk HS, Biemond JJ, Earny VA, et al Unraveling sepsis epidemiology in a low- and middle-income intensive care setting reveals the alarming burden of tropical infections and antimicrobial resistance: a prospective observational study (MARS-India). Clin Infect Dis 2025; 80:101–7.39352692 10.1093/cid/ciae 486PMC 11797389 · doi ↗ · pubmed ↗
- 6Rudd KE, Tutaryebwa LK, West TE. Presentation, management, and outcomes of sepsis in adults and children admitted to a rural Ugandan hospital: a prospective observational cohort study. P Lo S One 2017; 12:1–13.
- 7Thwaites L, Nasa P, Abbenbroek B, et al Management of adult sepsis in resource-limited settings: global expert consensus statements using a Delphi method. Intensive Care Med 2025; 51:21–38.39714613 10.1007/s 00134-024-07735-7PMC 11787051 · doi ↗ · pubmed ↗
- 8Hantrakun V, Somayaji R, Teparrukkul P, et al Clinical epidemiology and outcomes of community acquired infection and sepsis among hospitalized patients in a resource limited setting in Northeast Thailand: a prospective observational study (Ubon-sepsis). P Lo S One 2018; 13:1–14.