A predictive algorithm for the optimal daily dosage of thiamazole to control cats with hyperthyroidism
Pak-Kan Tang, Nicola Lötter, Rebecca F Geddes, Rosanne E Jepson, Yu-Mei Chang, Harriet Syme, Jonathan Elliott

TL;DR
This study created a tool to predict the best starting dose of thiamazole for cats with hyperthyroidism based on blood test results.
Contribution
A validated predictive algorithm for thiamazole dosage in hyperthyroid cats using baseline TT4 and creatinine levels.
Findings
Higher TT4 and lower creatinine at diagnosis predict the need for >5 mg thiamazole daily.
The algorithm achieved 91.1% accuracy in predicting the correct dosage.
The model showed high specificity (96.2%) and moderate sensitivity (84.2%).
Abstract
Hyperthyroidism is the most common endocrinopathy in cats and is frequently managed using anti-thyroid medication. To develop and validate an algorithm to predict the optimal starting daily dose of thiamazole required to control hyperthyroidism in cats. One hundred eighty-eight client-owned cats with hyperthyroidism for algorithm development (2011-2021) and 45 hyperthyroid cats to validate the algorithm (2022-2024). Retrospective case-control study. Cats with hyperthyroidism controlled medically using thiamazole within a year since diagnosis were enrolled. Controlled dose of thiamazole was categorized into “≤5 mg” or “>5 mg.” Binary logistic regression was performed to explore predictors associated with thiamazole dose. The performance of the final multivariable model in prediction was assessed by receiver operating characteristic (ROC) curve analysis. A cohort of cats subsequently…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
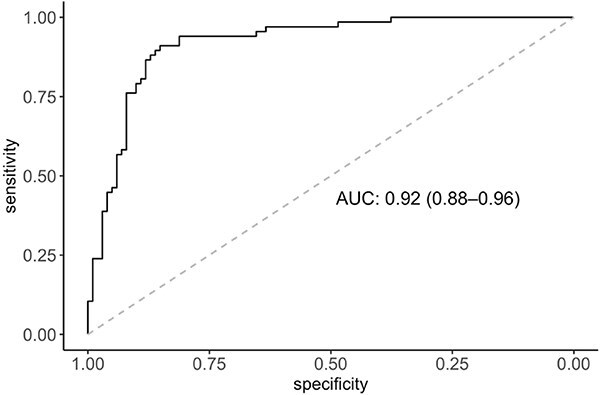 Figure 1
Figure 1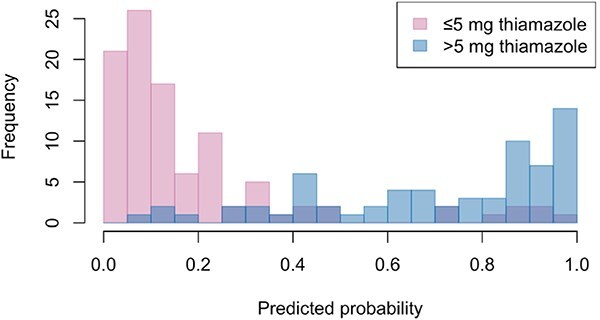 Figure 2
Figure 2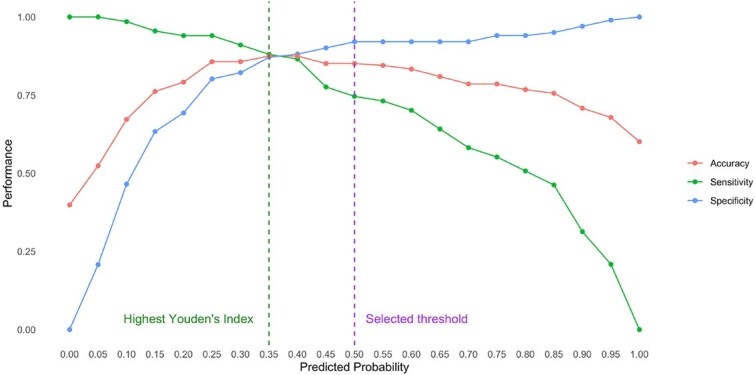 Figure 3
Figure 3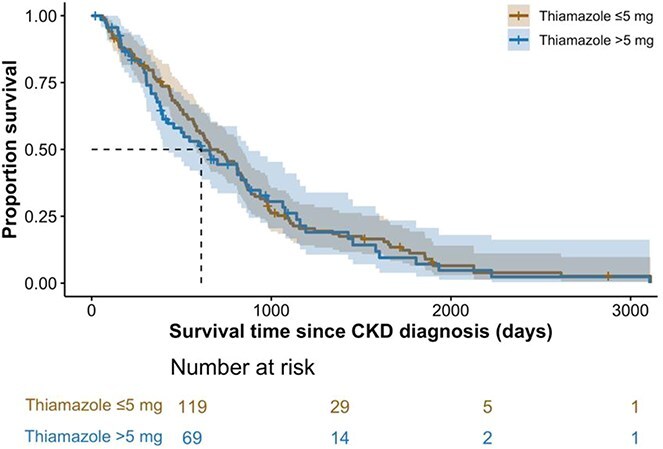 Figure 4
Figure 4|
|
|
|
|---|---|---|
|
| 1.25 | 1 (1%) |
| 2.5 | 32 (27%) | |
| 3.75 | 6 (5%) | |
| 5 | 80 (67%) | |
|
| 7.5 | 8 (12%) |
| 10 | 46 (67%) | |
| 12.5 | 7 (10%) | |
| 15 | 3 (4%) | |
| 17.5 | 1 (1%) | |
| 20 | 4 (6%) |
|
|
|
|
| ||
|---|---|---|---|---|---|
|
|
| Median |
| ||
|
| 15.5 [13.7, 17.2] | 119 | 14.1 [12.3, 15.7] | 68 |
|
|
| 43 [37], 68 [58], 6 [5] | 117 | 34 [50] 34 [50], 0 [0] | 68 | .05 |
|
| 7 [6], 40 [34], 56 [48], 13 [11] | 116 | 7 [10], 28 [41], 26 [38], 7 [10] | 68 | .46 |
|
| 3.21 [2.92, 4.03] | 113 | 3.4 [2.83, 3.81] | 70 | .48 |
|
| 71 [60] | 119 | 36 [52] | 69 | .32 |
|
| 200 [180, 223] | 119 | 220 [200, 240] | 68 |
|
|
| 3.1 [3, 3.3] | 101 | 3.1 [3, 3.2] | 67 | .14 |
|
| 58 [44, 81] | 101 | 127 [86, 187] | 67 |
|
|
| 95 [72, 152] | 101 | 260 [144, 439] | 67 |
|
|
| 0.09 [0.06, 0.13] | 79 | 0.12 [0.1, 0.18] | 67 |
|
|
| 119 [117, 122] | 79 | 119 [118, 121] | 67 | .82 |
|
| 168 [145, 198] | 79 | 161 [143, 186] | 67 | .19 |
|
| 1.29 [1.1, 1.6] | 101 | 0.94 [0.85, 1.07] | 67 |
|
|
| 38 [34, 41] | 119 | 38 [35, 41] | 68 | .41 |
|
| 3.88 [3.51, 4.5] | 101 | 4.33 [3.99, 5.21] | 67 |
|
|
| 3.8 [3.54, 4.27] | 81 | 3.9 [3.7, 4.2] | 67 | .41 |
|
| 142 [128, 154] | 118 | 147 [132, 160] | 69 | .16 |
|
| 155 [153, 157] | 79 | 154 [153, 157] | 67 | .86 |
|
| 9.7 [9.4, 10.1] | 101 | 9.5 [9.2, 9.8] | 67 |
|
|
| 7.4 [7, 7.8] | 101 | 7.1 [6.8, 7.5] | 66 |
|
|
| 66.5 [58.1, 85.7] | 119 | 184 [124, 225] | 69 |
|
|
| 31.7 [24.5, 41.3] | 79 | 26.9 [23, 32.1] | 67 |
|
|
| 1.023 [1.017, 1.038] | 73 | 1.033 [1.026, 1.042] | 35 |
|
|
|
|
| ||||
|---|---|---|---|---|---|---|
| OR (95% CI) |
|
| OR (95% CI) |
|
| |
|
| 0.87 (0.77-0.96) | 187 |
| |||
|
| 1.17 (1.07-1.29) | 187 |
| |||
|
| 1.17 (1.1-1.25) | 168 |
| |||
|
| 1.03 (1.02-1.05) | 168 |
| |||
|
| 1.09 (1.04-1.16) | 146 |
| |||
|
| 0.68 (0.58-0.77) | 168 |
| 0.83 (0.7-0.96) | 168 |
|
|
| 2.28 (1.52-3.54) | 168 |
| |||
|
| 0.41 (0.21-0.76) | 168 |
| |||
|
| 0.93 (0.88-0.99) | 167 |
| |||
|
| 1.36 (1.26-1.49) | 188 |
| 1.29 (1.19-1.42) | 168 |
|
|
| 0.97 (0.94-1) | 146 | .06 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Veterinary Medicine and Surgery · Cardiovascular Conditions and Treatments
Introduction
Hyperthyroidism is the most common endocrinopathy in cats in United States, Canada, United Kingdom, Europe, Australia, New Zealand, and Japan, with a prevalence of 6%-21% in senior cats.^1–5^ Anti-thyroid medication, such as thiamazole (also known as methimazole) and carbimazole, is commonly used either as long-term therapy or prior to more definitive treatments (surgery or radioactive iodine).^6^ Thiamazole, a thionamide anti-thyroid agent, inhibits the action of thyroid peroxidase (TPO),^7^ which is an essential enzyme for thyroid hormone synthesis by catalyzing the iodination of tyrosine residues in thyroglobulin and the oxidative coupling of iodinated tyrosines.^8^ The recommended starting dose for thiamazole (Thyronorm® [Norbrook Laboratories Limited, Newry, UK],^9^ Felimazole® [Dechra Limited, Skipton, UK],^10,11^ Thiafeline® [Le Vet Beheer B.V., Oudewater, The Netherlands]) is 5 mg per day, usually given as 2.5 mg tablet or oral solution twice daily.^12,13^ Dose adjustment is often required according to the clinical response (ie, appetite, body weight) and serum total thyroxine (TT4) concentration after the initiation of treatment. Like many other medical conditions, the severity of disease varies across a spectrum. In general, the severity of hyperthyroidism correlates with the degree of elevation in serum TT4 concentration and thyroid gland enlargement.^14^ To date, no definitive guidance on adjusting the starting dose according to the severity of hyperthyroidism at diagnosis is provided by drug manufacturers of methimazole-containing products, although expert panel opinion has suggested that a higher starting dose (ie, a total daily dose of 10 mg) might be considered for cats with severe hyperthyroidism.^13^ Nonetheless, the dose-dependent effect of thiamazole on lowering serum TT4 concentrations in hyperthyroid cats remains largely unexplored.
Chronic kidney disease (CKD) is another common medical condition that affects older cats, with a prevalence of 31%-81% reported in cats over 15 years of age.^15,16^ A wealth of evidence supports the profound influence of thyroid status on renal function. Hyperthyroidism leads to an increased glomerular filtration rate (GFR) because of enhanced cardiac output by positive chronotropic and inotropic effects,^17,18^ reduced peripheral vascular resistance,^19^ increased renal blood flow^20^ and stimulation of the renin-angiotensin-aldosterone system.^21,22^ In human patients with hyperthyroidism, GFR decreases by an average of 29% once euthyroidism was restored.^20^ GFR reduction of 44% and 47% is documented in hyperthyroid cats treated with bilateral thyroidectomy^23^ and thiamazole.^24^ Iatrogenic hypothyroidism further exacerbates renal dysfunction in cats with CKD.^25,26^ Therefore, it is crucial to identify and preferably prevent the development of iatrogenic hypothyroidism, especially in cats with pre-existing CKD or those at increased risk of developing CKD.
Considering the pharmacological mechanism of thiamazole in the inhibition of thyroid hormone synthesis, it is reasonable to assume that hyperthyroid cats with higher plasma TT4 concentration at diagnosis would require a higher dose of thiamazole to restore euthyroidism. Therefore, the aims of this study were first, to develop an algorithm to predict the optimal starting daily dose of thiamazole required to achieve euthyroidism; second, to compare the proportion of cats that developed azotemic CKD between different thiamazole doses; and third, to evaluate whether there was any association between thiamazole dose and survival.
Materials and methods
Case selection
Clinical records of the Royal Veterinary College (RVC) Ageing Cat Clinic, which was held in 2 first-opinion practices in London, over a 11-year period (between January 1, 2011 and December 31, 2021) were reviewed and senior cats (≥9 years old) with hyperthyroidism were retrospectively identified for the algorithm training cohort. Clinical records over a subsequent 3-year period (between January 1, 2022 and December 31, 2024) were reviewed to identify a separate testing cohort of cats with hyperthyroidism. All cats examined in these clinics were enrolled as part of an ongoing longitudinal observational study of which informed consent of the owner was obtained and approval of the RVC Ethics and Welfare Committee (URN 2023 2225-3) was granted. A diagnosis of hyperthyroidism was defined as plasma TT4 concentration >55 nmol/L, or TT4 40-55 nmol/L with thyroid stimulating hormone (TSH) < 0.03 ng/mL, together with compatible clinical signs (ie, weight loss and tachycardia in addition to increased appetite or palpation of goiter).
Inclusion criteria for this retrospective study included cats with hyperthyroidism treated with thiamazole (Thyronorm® or Felimazole®). In accordance with our standardized clinic protocol, a starting daily dose of thiamazole of 5 mg and 10 mg was recommended in hyperthyroid cats with a baseline TT4 < 100 nmol/L or ≥ 100 nmol/L, respectively. A follow-up visit was recommended 3-4 weeks after the initiation of thiamazole for dose adjustment. If plasma TT4 concentration was < 10 nmol/L at the follow-up visit but the cat remained clinically well, non-azotemic (plasma creatinine < 2 mg/dL), or had stable CKD (≤25% increase in creatinine compared to the pre-thiamazole value), the same thiamazole dose was maintained and plasma TT4 was re-evaluated after 16 weeks. If the second TT4 is persistently low (<10 nmol/L) then the daily total dose of thiamazole was decreased by approximately 20%-25%. If plasma creatinine increased by >25% from the pre-thiamazole value and plasma TT4 concentration was <10 nmol/L after the initiation of thiamazole, the thiamazole dose was reduced by approximately 20%-25%. Plasma TT4 was re-evaluated 3-4 weeks after dose adjustment. The thiamazole dose at which the cat achieved euthyroidism (plasma TT4 10-40 nmol/L) was recorded and included in the study analysis.
Cats with hyperthyroidism treated with surgical thyroidectomy, radioactive iodine (I131), or transdermal methimazole were excluded. Hyperthyroid cats with no baseline TT4, no follow-up visits, or no information on thiamazole dose when hyperthyroidism was controlled, or cats that took over a year to restore euthyroidism (TT4 10-40 nmol/L) after starting anti-thyroid medication were also excluded.
Cats that developed azotemic CKD within a year after euthyroidism was restored and those that remained non-azotemic for at least a year were identified. Azotemic CKD diagnosis was defined as a plasma creatinine concentration ≥2 mg/dL with a USG < 1.035, or plasma creatinine concentration ≥2 mg/dL on 2 consecutive occasions with no evidence of pre-renal causes including iatrogenic hypothyroidism. Cats that developed azotemic CKD after achieving euthyroidism were classified as International Renal Interest Society (IRIS) stage 2 or 3 according to their plasma creatinine concentration at the time of CKD diagnosis.^27^
Data collection
Blood samples were collected by jugular venipuncture into heparinized tubes, while urine was obtained by cystocentesis. Samples were stored at 4 °C for <6 h before centrifugation and separation. Biochemical analysis was performed on heparinized plasma at an external laboratory (IDEXX laboratories, Wetherby, UK), TT4 and TSH were measured using chemiluminescence immunoassay, while creatinine was measured using enzymatic colorimetric assay. In-house urinalyses, including urine specific gravity (USG) measurement by refractometry, dipstick chemistry analysis, and microscopic urine sediment examination, were performed on the day of collection. Doppler method was used to measure systolic blood pressure (SBP).^28^
Clinical records were reviewed to extract: age, sex, breed, body weight, body condition score (BCS, 9-point scale), muscle condition score (MCS, 4-point scale), heart rate, plasma concentrations of creatinine, urea, total calcium, phosphate, potassium, sodium, chloride, total protein, albumin, bilirubin, cholesterol, and TT4 and the activities of alanine aminotransferase (ALT) and alkaline phosphatase (ALP), packed cell volume (PCV), SBP, and USG. Dose of thiamazole and when hyperthyroidism was controlled with plasma TT4 of 10-40 nmol/L for the first time within a year since diagnosis, and the number of dose adjustment required to achieve euthyroidism were recorded and included in the study analysis.
Statistical analysis
Statistical analyses were performed using R software (Version 4.3.1 GUI 1.79 Big Sur ARM build, R Foundation for Statistical Computing, Vienna, Austria). Type I error rate was set at 0.05. The normality of continuous variables was assessed using the Shapiro–Wilk test and by visual inspection of Q-Q plots. Most data were not normally distributed in the study and therefore numerical data are presented as median [25th, 75th percentile]. Categorical data are presented as percentages. Controlled dose of thiamazole was categorized into 2 groups: “≤5 mg” or “>5 mg.” Number of dose adjustment to achieve euthyroidism was also categorized into 2 groups: “0” or “≥1.”
Baseline clinicopathological variables between groups
Comparison of variables at diagnosis between groups (“≤5 mg” or “>5 mg”) was performed by either independent samples *t-*test or Mann–Whitney U test for continuous variables with normal or skewed distributions, respectively. Proportion of categorical outcomes was compared using chi-squared test. Spearman’s correlation was used to evaluate the relationship of total daily dose of thiamazole to achieve euthyroidism with baseline plasma TT4 concentration at diagnosis and the change in plasma TT4 concentration once euthyroidism was restored.
Risk factors and predictive algorithm for dose of thiamazole
Binary logistic regression was performed to explore predictors associated with thiamazole dose. For univariable analysis, age, body weight, heart rate, SBP, creatinine, urea, phosphate, total calcium, potassium, sodium, chloride, total protein, albumin, ALT, ALP, and PCV were entered as continuous variables, while sex, BCS and MCS were entered as categorical variables. USG was not entered in this analysis because of the substantial (>40%) missing data. The final model was derived by manual backward elimination, with P ≤ .05 denoting significance. Hosmer–Lemeshow test was used to assess the goodness-of-fit of the final model, and variance inflation factor was used to check for presence of co-linearity among the significant risk factors (P ≤ .05). The performance of the final multivariable model in prediction was assessed by receiver operating characteristic (ROC) curve analysis. Results are reported as odds ratio (OR; 95% CI).
Predicted probability for each thiamazole dose (“≤5 mg” vs “>5 mg”) for controlling hyperthyroidism for each cat was generated from a fitted multivariable logistic regression model. A predicted probability cutoff of 0.5 was applied for classification. The predictive performance was assessed by the accuracy, sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) based on the comparison between the predicted thiamazole dose group classification and the actual thiamazole dose required to achieve euthyroidism.
Validation of predictive model
Clinical records between January 1, 2022 and December 31, 2024 (3-year period) were reviewed to identify a separate testing cohort of cats with hyperthyroidism using identical inclusion and exclusion criteria as mentioned above. The algorithm derived on predicting the optimal thiamazole dose to achieve euthyroidism was applied to the testing cohort. The predictive performance was accessed by the accuracy, sensitivity, specificity, NPV, and PPV.
Comparison of proportion of cats developing azotemic CKD between thiamazole dose
Chi-square test was performed to compare proportion of cats developing azotemic CKD within a year and those remained non-azotemic for at least a year since hyperthyroidism was controlled between the different thiamazole dose (“≤5 mg” vs “>5 mg”).
Association of thiamazole dose with survival
Date of hyperthyroidism diagnosis was defined as baseline, whereas death of all-cause was the event of interest. Survival times were illustrated with a Kaplan–Meier curve and were compared between groups based on thiamazole dose (“≤5 mg” vs “>5 mg”) using log-rank test. Cox proportional hazard analysis was used to assess the association of survival with thiamazole dose to achieve euthyroidism.
Results
Over the 11-year period (2011-2021), a total of 419 cats with hyperthyroidism were identified, of which 29 cats were excluded because baseline TT4 (n = 4) or thiamazole dose (n = 25) was not recorded on our electronic database, or they had no follow-up visit after thiamazole was initiated (n = 32). Of the remaining 358 cats, 170 cats were further excluded because hyperthyroidism was treated with thyroidectomy (n = 37), transdermal methimazole (n = 3) or I131 (n = 1), or hyperthyroidism remained uncontrolled for greater than a year after diagnosis (n = 129).
In total, 188 hyperthyroid cats met the criteria and were enrolled in the training cohort, with 119 cats (63%) controlled with ≤5 mg (range, 1.25-5 mg) and 69 cats (37%) controlled with >5 mg (range, 7.5-20 mg) total daily dose of thiamazole. Table 1 presents the number of cats controlled on various thiamazole doses. Strong positive correlations were found between thiamazole dose to achieve euthyroidism and baseline plasma TT4 concentration at diagnosis and the change in TT4 once restored to a euthyroid state (both r_s_ = 0.76; P < .001). Majority of hyperthyroid cats (67%) were controlled on either 5 mg (n = 80) or 10 mg (n = 46) of thiamazole daily. Domestic shorthair was the most common breed (n = 163), followed by domestic longhair (n = 21) and one each of the following breeds: British shorthair, Norwegian Forest, Russian blue, and Siamese mix. The median time taken to achieve euthyroidism since diagnosis was 56 [35, 119] days and 70 [42, 175] days for cats with ≤5 and >5 mg thiamazole, respectively, with no significant difference observed between groups (P = .2). The number of dose adjustments required to achieve euthyroidism was significantly different between groups, with higher proportion of cats stabilized on >5 mg requiring at least 1 dose adjustment compared to those controlled on ≤5 mg (39% vs 17%; P < .001).
Baseline clinicopathological variables at diagnosis of hyperthyroidism are summarized in Table 2. Hyperthyroid cats controlled on a >5 mg total daily dose of thiamazole had significantly higher plasma TT4, phosphate, and bilirubin concentrations, higher ALT and ALP activities, higher heart rate and USG, and lower plasma concentrations of creatinine, urea, total protein and total calcium, and were younger than cats that were controlled on a ≤5 mg total daily dose of thiamazole. No other significant differences in baseline clinicopathological variables were identified between groups.
Risk factors and predictive algorithm for dose of thiamazole
Results from univariable logistic regression analysis identified that higher plasma concentrations of TT4, phosphate and bilirubin, ALT and ALP activities, and heart rate, and lower plasma concentrations of creatinine, total protein and total calcium, and being younger at diagnosis were associated with increased thiamazole dose (>5 mg) to achieve euthyroidism (P < .1; Table 3). In the final multivariable logistic regression model (n = 168), baseline plasma concentrations of TT4 (OR = 1.29 [95%CI, 1.19-1.42] per 10 nmol/L increase; P < .001) and decreased creatinine (OR = 0.83 [95%CI, 0.7-0.96] per 0.1 mg/dL increase; P = .02) remained significant variables for predicting the thiamazole dose to achieve euthyroidism. The area under the ROC curve was 0.92 (95% CI, 0.88-0.96; Figure 1), suggesting an excellent predictive accuracy of the final multivariable model. Predicted probability for each cat was generated based on the fitted final multivariable logistic regression model (Figure 2). The change in model performance across different predicted probability is illustrated in Figure 3, with the predicted dose (“≤5 mg” or “>5 mg”) for each cat assigned based on probability cutoff of 0.5. The overall accuracy of this predictive model in predicting the optimal dose of thiamazole to achieve euthyroidism was 85.1%, with a sensitivity of 74.6%, specificity of 92.1%, NPV of 84.6%, and PPV of 86.2%.
Receiver operating characteristic (ROC) curve illustrating the predictive ability of baseline plasma concentrations of total thyroxine and creatinine at diagnosis of hyperthyroidism for the increased total daily dose (>5 mg) of thiamazole to achieve euthyroidism within a year. Predictive accuracy of this model was excellent with an area under the curve of 0.92 (95% CI, 0.88-0.96).
Overlapping histograms illustrating the distribution of predicted probability for cats requiring total daily dose of ≤ 5 mg (pink) and >5 mg (blue) thiamazole to achieve euthyroidism in cats. Predicted probability was generated from the fitted logistic regression model using plasma total thyroxine (TT4) and creatinine concentrations at diagnosis of hyperthyroidism. Areas where the histograms overlap appear as purple.
Impacts of predicted probability threshold adjustments on model performance.
Validation of predictive model
A total of 45 hyperthyroid cats met the inclusion and exclusion criteria and were used as a separate testing cohort for validation. Hyperthyroidism was controlled with ≤5 mg thiamazole in 26 cats (58%) and >5 mg thiamazole in 19 cats (42%). Predicted probability for each cat was generated based on the fitted final multivariable logistic regression model obtained from the training cohort of 168 cats. Using the predicted probability of 0.5 as cutoff, the overall accuracy of this predictive model when applied to a separate testing cohort was 91.1%, with a sensitivity of 84.2%, specificity of 96.2%, NPV of 89.3%, and PPV of 94.1%.
Development of azotemic CKD after restoration of euthyroidism
Of the 188 hyperthyroid cats enrolled in this study, 23 cats had a diagnosis of azotemic CKD confirmed prior to a diagnosis of hyperthyroidism or before euthyroidism was achieved, 11 cats met the criteria for a diagnosis of azotemic CKD but had suspected iatrogenic hypothyroidism at the same time, 10 cats developed azotemic CKD greater than 1 year after euthyroidism was restored, and 60 cats had insufficient (<1 year) follow-up period once euthyroid to confirm the absence of CKD development. These cats were therefore excluded from further analyses. Of the remaining 84 cats, 22 developed azotemic CKD (IRIS stage 2, n = 19; IRIS stage 3, n = 3) within a year of euthyroidism being achieved and had no evidence of iatrogenic hypothyroidism, with 14 (63.6%) and 8 (36.4%) cats requiring ≤5 mg and >5 mg total daily dose of thiamazole to restore euthyroidism, respectively (Tables S1 and S2). No difference in plasma creatinine concentration (P = .31) or IRIS stage (P = 1) at diagnosis of CKD was observed between thiamazole dose groups. Sixty-two cats remained non-azotemic (≤5 mg, n = 36 [58.1%]; > 5 mg, n = 26 [41.9%]) for a minimum of 1 year after restoration of euthyroidism. There was no difference in the proportion of cats that developed azotemic CKD within a year once euthyroidism was restored between cats controlled on a total daily thiamazole dose of ≤5 and >5 mg (P = .65).
Association of thiamazole dose to achieve euthyroidism with survival
No difference in survival was found between hyperthyroid cats controlled on ≤5 mg thiamazole compared to cats that required >5 mg thiamazole to achieve euthyroidism (P = .65), with medium survival time of 661 (95% CI, 584-838) days and 610 (95% CI, 425-874) days, respectively (Figure 4).
Kaplan–Meier curve illustrating survival in cats with hyperthyroidism (n = 188) grouped by the thiamazole dose to achieve euthyroidism (“≤5 mg” vs “>5 mg”). Right censoring was employed for cats that were lost to follow-up or remained alive at the end of study period. No difference in survival time was observed between groups (P = .65).
Discussion
The present study provided a reliable algorithm, using plasma concentrations of TT4 and creatinine, to predict the optimal starting daily dose of thiamazole at diagnosis of hyperthyroidism in cats. The predictive model was successfully validated using an additional cohort. The algorithm has the potential to control hyperthyroidism in cats more efficiently, reducing the time taken and the number of veterinary visits and dose adjustment required. Not only would this help to mitigate stress in these hyperthyroid cats, but also alleviate financial burdens associated with recurrent follow-up appointments and repeated plasma TT4 concentration measurements.
Results from our multivariable logistic regression analysis showed that higher plasma TT4 concentration and lower plasma creatinine concentration at hyperthyroidism diagnosis were associated with increased (>5 mg) total daily dose of thiamazole to achieve euthyroidism. It is well-established that thyroxine increases GFR, and muscle mass is often reduced in patients with thyrotoxicosis.^29^ Furthermore, thyroid hormone may also influence the rate of endogenous creatinine production.^30^ Consequently, these factors contribute to the reduced plasma creatinine concentration in hyperthyroid patients with excessive thyroxine production.^23,24,31^ Thiamazole has been suggested to act as a competitive substrate for TPO to decrease the incorporation of iodide into tyrosine molecules for the formation of thyroid hormone.^32,33^ Therefore, a dose-dependent inhibitory effect of thiamazole is expected. This is further supported by our finding that thiamazole dose required to achieve euthyroidism correlates positively with plasma TT4 concentration at diagnosis and the change in TT4 once euthyroid.
An additional explanation for the requirement of the higher dose of thiamazole in cats with higher TT4 and lower creatinine concentrations is that thiamazole is more rapidly cleared by the kidney in the more severely hyperthyroid cats. The route of elimination of thiamazole in the cat has not been studied and while the mean residence time of thiamazole was reported to be shorter in hyperthyroid cats compared to euthyroid (healthy) cats after a single dose,^34^ this difference is unlikely to be clinically significant as it was dependent on 2 of the healthy cats having slow clearance, which increased in these 2 cats on multiple dosing.^35^
Cats controlled on >5 mg thiamazole required higher number of dose adjustments before euthyroidism was achieved, with 39% requiring at least 1 dose adjustment compared to 17% in those controlled on ≤5 mg. Interestingly, if all cats controlled on >5 mg thiamazole had initially been started on the recommended daily dose of 5 mg, at least 1 dose adjustment would certainly be needed regardless. However, 61% of our hyperthyroid cats controlled on >5 mg thiamazole did not require any dose adjustment because our cats with plasma TT4 concentration >100 nmol/L were immediately started on 10 mg total daily dose of thiamazole at diagnosis according to our clinic’s protocol. Therefore, the number of dose adjustments for cats controlled on >5 mg thiamazole reported in our study is likely to be lower than if they had initially started on a total daily dose of 5 mg, due to the additional adjustment required. On the contrary, no significant difference in the time taken to achieve euthyroidism between cats requiring ≤5 and >5 mg thiamazole was observed in our population. There are several explanations for this finding. First, only cats with hyperthyroidism controlled within the first year since diagnosis were included in the study. Second, not all hyperthyroid cats were started on 5 mg total daily dose of thiamazole at diagnosis; those with plasma TT4 > 100 nmol/L at diagnosis were started on 10 mg total daily dose of thiamazole according to our clinic’s protocol. Third, these results could be heavily influenced by the owners, despite all being advised to bring their cats back for the measurement of plasma TT4 concentration 3-4 weeks after each dose adjustment until hyperthyroidism was controlled. However, these factors should not affect the results of our predictive algorithm on the optimal starting dose of thiamazole.
The median survival time for hyperthyroid cats in our study was 610 days, which is longer than the 417 days reported in a previous study of medically treated senior cats (≥9 years old).^36^ However, our study population was highly selected and different to other feline studies.^22,25,36,37^ Notably, only hyperthyroid cats that were successfully restored euthyroidism with thiamazole within a year since diagnosis were included in our analysis. Therefore, the results from our survival analysis could have been overestimated because inadequately treated cats were excluded. While our study was not designed to determine the influence of control of hyperthyroidism on survival, our findings suggested hyperthyroid cats restored to a euthyroid state may have a longer survival than those with either persistent hyperthyroidism or iatrogenic hypothyroidism. Further studies with appropriate survival analysis are needed to confirm these findings. Additionally, survival times and proportion of cats developing azotemic CKD following restoration of euthyroidism were not found to be different between cats that required different dose of thiamazole, providing that euthyroidism was successfully restored.^37^
Overall, we developed an algorithm, using plasma TT4 and creatinine concentrations, to better predict the optimal starting daily dose of thiamazole to achieve euthyroidism in cats. The performance of this predictive model was excellent. The performance of the predictive algorithm was developed and validated using the methodologies for TT4 and creatinine in our clinics; therefore extrapolation to other laboratories or analytical methods, especially those with differing reference intervals, may not be applicable. External validation with a larger data set is warranted to further evaluate the predictive performance of our model. Furthermore, a novel TSH assay based on bulk acoustic wave has recently been developed to measure TSH in cats with enhanced sensitivity and lower limit of quantification.^38^ Future study could explore the potential of incorporating TSH measurement, either using the traditional canine TSH or this novel sensitive assay, to enhance the predictive accuracy of our algorithm in determining the optimal starting dose of thiamazole to achieve euthyroidism.
Supplementary Material
aalag009_Supplemental_Files
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wakeling J, Elliott J, Syme H. Evaluation of predictors for the diagnosis of hyperthyroidism in cats. J Vet Intern Med. 2011;25:1057-1065.21985139 10.1111/j.1939-1676.2011.00790.x · doi ↗ · pubmed ↗
- 2Miyamoto T, Miyata I, Kurobane K, et al. Prevalence of feline hyperthyroidism in Osaka and the Chugoku region. Journal of the Japan Veterinary Medical Association. 2002;55:289-292.
- 3Gójska-Zygner O, Lechowski R, Zygner W. Prevalence of feline hyperthyroidism in mature cats in urban population in Warsaw. Bull Vet Inst Pulawy. 2014;58:267-271.
- 4Bree L, Gallagher BA, Shiel RE, Mooney CT. Prevalence and risk factors for hyperthyroidism in Irish cats from the greater Dublin area. Ir Vet J. 2018;71:2. 10.1186/s 13620-017-0113-x · doi ↗
- 5Köhler I, Ballhausen BD, Stockhaus C, Hartmann K, Wehner A. Prevalence of and risk factors for feline hyperthyroidism among a clinic population in southern Germany. Tierarztliche Praxis Ausgabe K: Kleintiere - Heimtiere. 2016;44:149-157. 10.15654/TPK-15059026902958 · doi ↗ · pubmed ↗
- 6Candellone A, Saettone V, Badino P, et al. Management of feline hyperthyroidism and the need to prevent oxidative stress: what can we learn from human research? Antioxidants. 2021;10:1496.34573128 10.3390/antiox 10091496 PMC 8469997 · doi ↗ · pubmed ↗
- 7Manna D, Roy G, Mugesh G. Antithyroid drugs and their analogues: synthesis, structure, and mechanism of action. Acc Chem Res. 2013;46:2706-2715. 10.1021/ar 400122923883148 · doi ↗ · pubmed ↗
- 8Roy G, Mugesh G. Bioinorganic chemistry in thyroid gland: effect of antithyroid drugs on peroxidase-catalyzed oxidation and iodination reactions. Bioinorg Chem Appl. 2006;2006:23214.17497002 10.1155/BCA/2006/23214 PMC 1794076 · doi ↗ · pubmed ↗