See One, B1, Treat One: Identifying and Managing Thiamine Deficiency in a Patient With Altered Mental Status
Michael Freddy, Tyler B Larsen, Satya Patel

TL;DR
A patient with altered mental status was found to have thiamine deficiency, which improved rapidly with thiamine supplementation.
Contribution
This case highlights the importance of considering thiamine deficiency in patients with altered mental status.
Findings
The patient's symptoms rapidly improved with intravenous thiamine.
Low serum thiamine levels confirmed the deficiency.
Early recognition and treatment can prevent Korsakoff syndrome.
Abstract
Nutritional deficiencies in the United States are relatively uncommon due to federal regulations surrounding the fortification of food. As a result, the clinical syndromes that result from nutritional deficiencies are not commonly seen, making them less likely to be encountered in the clinical setting. Thiamine deficiency in particular is an important nutritional deficiency to consider, as the presentation is highly variable and can include encephalopathy and multiple neurologic findings. We present a case of altered mental status that appears to be Wernicke’s encephalopathy due to the rapid improvement of symptoms with intravenous thiamine supplementation, corroborated by a low serum thiamine level. Assessing access to food is a critical piece of history in making this diagnosis, and early recognition can promote fully supplementing patients with thiamine to prevent ongoing thiamine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1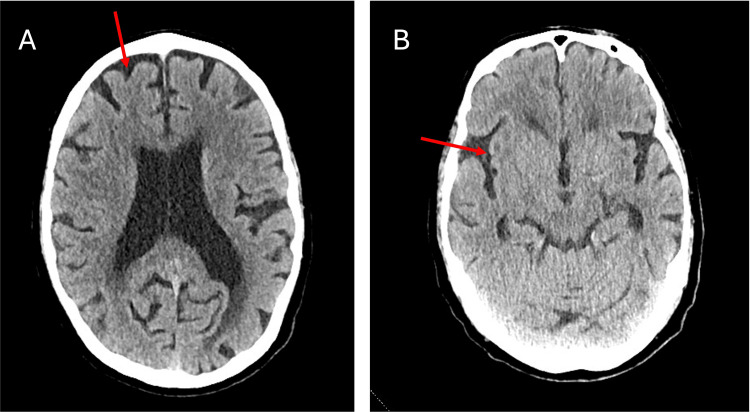 Figure 2
Figure 2| Serum Laboratory Study | Result | Reference Range |
| White blood cell | 10.85 per uL | 4.5 to 11.0 per uL |
| Blood urea nitrogen | 53 mg/dL | 5 to 25 mg/dL |
| Creatinine | 1.56 mg/dL | 0.52 to 1.28 mg/dL |
| Calculated estimated glomerular filtration rate | 46 mL/min | 88 to 110 mL/min |
| Calcium | 8.8 mg/dL | 8.4 to 10.2 mg/dL |
| Creatinine kinase | 1584 U | 40 to 280 U/L |
| Lactate | 1.12 mmol/L | 0.5 to 2.2 mmol/L |
| Thyroid-stimulating hormone | 8.365 uIU/mL | 0.55 to 4.78 uIU/mL |
| Free T4 | 1.21 ng/dL | 0.66 to 1.73 ng/dL |
| Vitamin B12 | 3145 pg/mL | 160 to 911 pg/mL |
| Folate | 15.82 ng/mL | > 5.37 ng/mL |
| Rapid plasma reagin | Non-reactive | Non-reactive |
| Human immunodeficiency virus antibody screening | Negative | Negative |
| Urine Study | Result | Reference Range |
| Specific gravity | 1.020 | 1.008 to 1.030 |
| Protein | 100 mg/dL | 0 to 20 mg/dL |
| Ketones | 20 mg/dL | Trace |
| Nitrites | Negative | Negative |
| Leukocyte esterase | 500 per uL | 0 to 25 per uL |
| White blood cell | >182 per high-powered field | 0 to 5 per high-powered field |
| Red blood cell | 123 | 0 to 5 per high-powered field |
| Squamous epithelial cells | Small | None to rare |
| Ethanol | Negative | Negative |
| Amphetamines | Negative | Negative |
| Benzodiazepines | Negative | Negative |
| Opiates | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAlcoholism and Thiamine Deficiency · Folate and B Vitamins Research · Vitamin C and Antioxidants Research
Introduction
Thiamine deficiency is relatively uncommon in the United States due to fortification of foods with thiamine, but it remains an important diagnosis to consider, especially in patients on long-term loop diuretics, who have undergone bariatric surgery, and with alcohol use disorder [1-3]. Thiamine deficiency can present as wet beriberi or as one of three presentations of dry beriberi: Wernicke’s encephalopathy, Korsakoff syndrome, or a combination of peripheral neuropathy and glossitis [1,4]. Wernicke’s encephalopathy is an acute presentation of thiamine deficiency described with a classic triad of vision issues, gait imbalance, and altered mental status [1]. If left untreated, this can progress to a more permanent and severe form called Korsakoff syndrome [1].
Patients with thiamine deficiency rarely present with the classic presentation, and this report emphasizes the importance of having a high index of clinical suspicion for thiamine deficiency to diagnose it.
Case presentation
A 76-year-old male with hypertension, hyperlipidemia, aortic stenosis status-post aortic valve replacement, and hypothyroidism was brought into the emergency room by the fire department after being found down.
In the emergency department, the patient was unable to recall the events leading to him being brought in, but he noted a two-year history of progressive bilateral lower extremity weakness and thigh pain that may have contributed to him losing his balance and falling to the ground without loss of consciousness or head trauma. Over the past week, he noted having some issues with memory problems, noting that for the first time, he had left his home and was unable to figure out how to return. He denied fevers, shortness of breath, or dysuria, but noted some urinary incontinence.
The patient was experiencing homelessness and was currently living in a hotel. He was unable to explain how he accesses meals, but noted drinking a few beers per week.
His vital signs were notable for a BP of 106/65 mmHg. Physical examination revealed a 2/6 systolic crescendo-decrescendo murmur loudest at the right second intercostal area, pain with palpation of the suprapubic area, bilateral lower extremity edema with deep purple hyperpigmentation, mild tenderness to the bilateral thighs, 5/5 strength throughout his bilateral upper and lower extremities, and a wide-based shuffling gate. The patient's cranial nerve exam was normal, and no nystagmus or ophthalmoplegia was noted. Extensive laboratory testing was performed upon admission (Table 1).
A portable chest X-ray revealed no acute cardiothoracic abnormality (Figure 1). A computed tomography (CT) scan of the head without contrast was performed, which showed mild-moderate global cerebral atrophy with a moderate degree of chronic microvascular ischemia (Figure 2).
Portable chest X-ray showing no acute abnormalities
Computed tomography of the head without contrast on admission. A) The arrow indicates a deep sulcus. B) The arrow indicates an area of hyperintensity.
A urinalysis and urine drug screen were ordered upon admission. A serum thiamine level was also ordered upon admission. The patient was given intravenous fluid and resuscitation for possible mild rhabdomyolysis and also empirically started on intravenous thiamine 500mg. Given the lack of urinary tract symptoms experienced by the patient, empiric antibiotics were not initiated (Table 2).
The following morning, repeat examination revealed that he was alert and oriented to self, place, time, and location, and was able to better recall his issues with ambulation. His repeat gait exam normalized. The urine culture resulted as Staphylococcus aureus 15,000 cfu/mL and Aerococcus urinae >100,000 cfu/mL. The thiamine level resulted as <6 mmol/L (normal 8 - 30 mmol/L). The results of the urine culture were thought to be asymptomatic bacteriuria, and as the patient did not develop additional urinary tract symptoms while off antibiotics, the decision to not give antibiotics was maintained. Given the severely reduced thiamine level, the decision was made to complete an additional two days of intravenous thiamine repletion. For the duration of his hospitalization, the patient’s mental status remained intact, and he did not report any urinary symptoms. Given that he was living independently, he was given extensive counseling and references to ensure that he maintained access to food. He was also given resources for further support in the event that he had difficulty completing activities of daily living and independent activities of daily living, especially in the context of his imaging findings.
Discussion
As is the case with all vitamins, thiamine deficiency is caused by lack of access to thiamine, lack of absorption, and/or increased excretion. Lack of access to thiamine is relatively uncommon in the United States, as many foods are fortified with thiamine to prevent this [1]. Lack of absorption can occur in patients with alcohol use disorder, where active alcohol consumption downregulates expression of thiamine transporter-1 (THTR-1), which usually promotes thiamine reabsorption in the jejunal brush border [5]. Bariatric surgery can also alter gastric anatomy, thereby impairing enteral thiamine reabsorption [2]. As thiamine is a water-soluble vitamin, long-term loop diuretics can also cause thiamine deficiency [6].
Typically, a combination of the aforementioned pathologies can contribute to clinically significant thiamine deficiency in patients. To detect thiamine deficiency, clinicians must be aware of the classic and atypical presentations of thiamine deficiency, which is exceptionally challenging given how infrequently this diagnosis occurs in the United States due to the fortification of foods. Developing an illness script for thiamine deficiency and exploring lack of access to food during history taking can be ways to recognize this diagnosis.
Inherent to this illness script is understanding that in the typical work-up of altered mental status, the base rate of thiamine in the United States does not require it to be on the initial differential diagnosis and that more common causes of encephalopathy should instead be prioritized. In the case of this patient, especially in the context of being found down, a wide metabolic and infectious work-up was rightly prioritized, with metabolic causes outside of nutritional deficiencies being placed at the top of the differential diagnosis.
Hypothyroidism was on the initial differential diagnosis given the elevated thyroid-stimulating hormone (TSH); a TSH level less than 10 uIu/mL in conjunction with a normal free T4 level made subclinical hypothyroidism more likely. The patient’s initial urinary results were possibly suggestive of a urinary tract infection despite the absence of urinary tract symptoms. The patient’s brain imaging was consistent with early dementia in the right context. Rhabdomyolysis was also considered, given the elevation in creatine kinase; however, a much larger rise would be expected to lead to acute kidney injury from rhabdomyolysis and subsequent uremia to explain the altered mental status. Diagnostic clarity was obtained since the patient improved despite not receiving treatment for any of these diagnoses.
As with many patients, there are often multiple diagnoses contributing to a clinical syndrome, and this patient’s case is no different. Initial intracranial imaging shows findings that would be consistent with the mild cognitive impairment-dementia spectrum. Patients with dementia are not only more likely to suffer from nutritional deficiencies, but are also more likely to demonstrate clinical symptoms of nutritional deficiency, likely from dementia-related alterations in the metabolism and utilization of nutrients [7]. The additional layer of clinical complexity of this case was the initial decision to avoid giving antibiotics in the face of a possible urinary tract infection, instead electing to classify it as asymptomatic bacteriuria. There has been an emerging movement to avoid unnecessary antibiotics for bacteriuria in the absence of symptoms, which is challenging as older patients who present with altered mental status and are often unable to provide history or demonstrate exam findings consistent with symptomatic bacteriuria (namely dysuria and suprapubic tenderness). The decision not to give antibiotics in these cases must always remain individualized, as urinary tract infections can commonly cause encephalopathy and sepsis in older patients.
Thiamine deficiency can present as a cardiomyopathy with the clinical syndrome of wet beriberi [1]. Thiamine is a necessary cofactor to facilitate oxidative phosphorylation to produce energy for myocardial cells, and its absence can precipitate high-output heart failure [1]. As with most patients with heart failure, they are likely to receive loop diuretics. Loop diuretics will cause the loss of water-soluble vitamins, of which one is thiamine; this may exacerbate the thiamine deficiency that initially led to the heart failure. Wernicke’s syndrome is noted by the classic findings of encephalopathy, ataxic gait, and ophthalmoplegia; only 20% of patients present with the triad [8]. Korsakoff syndrome is thought to be a further progressed version of Wernicke’s, where patients develop anterograde amnesia, confabulation, and memory impairment. A subset of patients with thiamine deficiency will have neither wet beriberi nor Wernicke-Korsakoff syndrome and instead might have peripheral neuropathy and even painful glossitis [9].
Intravenous thiamine should be prioritized over oral repletion for patients with Wernicke’s encephalopathy, wet beriberi, severe alcohol use disorder, and patients who have undergone bariatric surgery (given impaired enteral absorption) [4].
This patient only had two of the findings of Wernicke’s syndrome, but rapid improvement after thiamine repletion suggests the diagnosis despite the patient having many other potential etiologies. As this is a rarer diagnosis in the United States, review of common etiologies of altered mental status, such as infection or common metabolic derangements, should be initially prioritized. If thiamine is to be empirically given, it is recommended to obtain a thiamine level prior to repletion, as the level will normalize as early as 6 hours after intravenous repletion [10].
Conclusions
In summary, thiamine deficiency can present atypically and should be considered in cases of altered mental status, especially in patients with issues with enteral absorption (either through alcohol use disorder or through altered gastric anatomy). As with all cases of altered mental status, prioritizing the common causes of infectious and structural pathologies is appropriate. In suspected cases of thiamine deficiency, empiric thiamine repletion can lead to rapid improvement in symptoms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cardiomyopathy in children: classification and diagnosis: A scientific statement from the American Heart Association Circulation Lipshultz SE Law YM Asante-Korang A 01402019 https://www.ahajournals.org/doi/full/10.1161/CIR.000000000000068210.1161/CIR.000000000000068231132865 · doi ↗ · pubmed ↗
- 2Thiamine deficiency in US veterans with obesity Obesity (Silver Spring) Costello E Kerns J 416421332025 https://pubmed.ncbi.nlm.nih.gov/39837759/3983775910.1002/oby.24210 PMC 11774014 · doi ↗ · pubmed ↗
- 3Wernicke encephalopathy—Clinical pearls Mayo clinic proceedings Sinha S Kataria A Abdelhamid YA 10651072 Elsevier 942019 https://www.sciencedirect.com/science/article/abs/pii/S 00256196193025513117111610.1016/j.mayocp.2019.02.018 · doi ↗ · pubmed ↗
- 4Wernicke's encephalopathy: New clinical settings and recent advances in diagnosis and management Lancet Neurol Sechi G Serra A 44245562007 https://pubmed.ncbi.nlm.nih.gov/17434099/1743409910.1016/S 1474-4422(07)70104-7 · doi ↗ · pubmed ↗
- 5Thiamine deficiency and neuroinflammation are important contributors to alcohol use disorder Pathophysiology Kalapatapu N Skinner SG D'Addezio EG Ponna S Cadenas E Davies DL 34322025 https://pubmed.ncbi.nlm.nih.gov/40700076/4070007610.3390/pathophysiology 32030034 PMC 12286186 · doi ↗ · pubmed ↗
- 6Loop diuretic therapy, thiamine balance, and heart failure Congest Heart Fail Sica DA 244247132007 https://pubmed.ncbi.nlm.nih.gov/17673878/1767387810.1111/j.1527-5299.2007.06260.x · doi ↗ · pubmed ↗
- 7Plasma nutrient status of patients with Alzheimer's disease: Systematic review and meta-analysis Alzheimers Dement Lopes da Silva S Vellas B Elemans S 485502102014 https://pubmed.ncbi.nlm.nih.gov/24144963/2414496310.1016/j.jalz.2013.05.1771 · doi ↗ · pubmed ↗
- 8Clinical and pathological features of alcohol-related brain damage Nat Rev Neurol Zahr NM Kaufman KL Harper CG 28429472011 https://pubmed.ncbi.nlm.nih.gov/21487421/2148742110.1038/nrneurol.2011.42PMC 8121189 · doi ↗ · pubmed ↗