The relationship between HIV infection and depression and their determinants in the MSM population in Eastern China: an analysis based on decision tree modelling and logistic regression
Yiwei Zhou, Zejie Zhang, Wancang Li, Lite Zeng, Chunyan Shan, Tianquan Chen, Zu-Mu Zhou

TL;DR
This study examines how depression and HIV are linked in China's MSM population, finding that marital status, age, and employment are key factors.
Contribution
The novel use of decision tree modeling combined with logistic regression to assess depression and HIV correlations in the MSM population.
Findings
Depression prevalence was 28.9% among MSM participants.
HIV-positive MSM had a higher depression rate (44.4%) compared to HIV-negative individuals (26.3%).
Marital status, age, and employment status were identified as significant factors influencing depression.
Abstract
This study aims to investigate the depression status of the MSM population, explore the depression characteristics associated with different HIV statuses within this group, and determine the key factors influencing depression in this population. This was a cross-sectional web-based survey. This study was conducted through a web-based comprehensive HIV service platform for the MSM population. The questionnaire included basic socio-demographic information of the respondents, HIV-related information and the Patient Health Questionnaire (PHQ-9). A decision tree model combined with logistic regression was used to assess the factors influencing depression in the MSM population. Among the 1070 MSM in this study, the depression prevalence was 28.9%, the overall HIV prevalence among MSM was 3.4%, the depression prevalence among HIV-positive MSM was 44.4%, and that among HIV-negative MSM was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
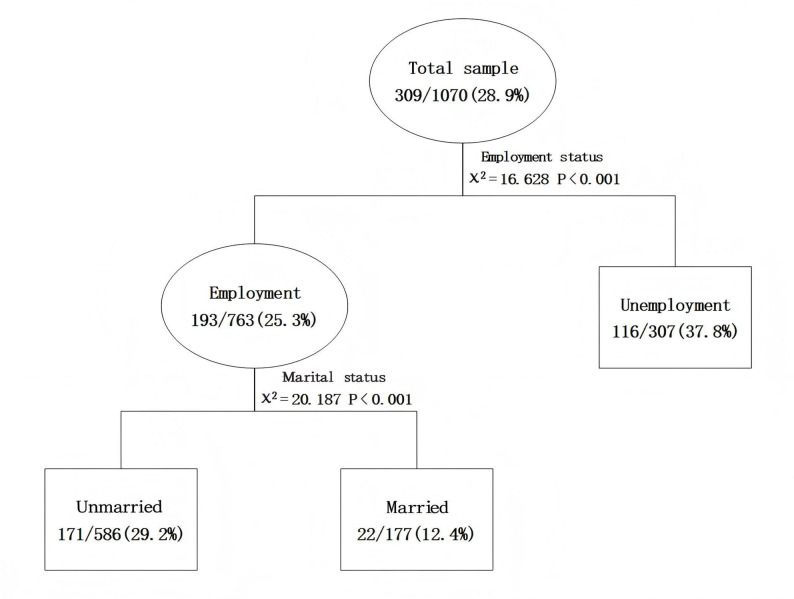 Figure 1
Figure 1- —2022 Ministry of Education of China Humanities and Social Science Youth Foundation Project
- —Shanghai Key Laboratory of Urban Design and Urban Science, NYU Shanghai Open Topic Grants
- —Shanghai University Young Teachers Cultivation and Support Project
- —National Social Science Foundation of China Post-Funding Project
- —Zhejiang Provincial Clinical Research Center for Mental Disorders Foundation Project
- —Wenzhou Science and Technology Bureau Science and Technology Program Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · HIV Research and Treatment · HIV-related health complications and treatments
Introduction
Men who have sex with men (MSM) population are at high risk of HIV infection and sexually transmitted diseases (STDs), and they tend to experience more severe mental health problems than the general population [1–5]. The low social acceptance of MSM, coupled with social discrimination and stigma, as well as the high risk of STDs, are often associated with significant psychological pressure, leading to emotional problems such as anxiety and depression [6, 7]. Chronic depressive symptoms not only cause physical harm, but also increase the incidence of self-harm and suicidal behaviour [7]. The prevalence of depression in MSM is often higher than in the general population [4, 5]. For instance, studies have shown that the prevalence of depression among MSM reaching 54% in Nepal [8, 9], 45.1% in India [10], and is three times higher in in the Netherlands compared to heterosexual men [2]. In the United States, depression rates among MSM have been reported as 33% in Massachusetts [11], 23.1% in Chicago [12] and 22.8% in Seattle [13]. Additionally, MSM have 3–5 times higher rates of depression than the general adult male population. Depression among MSM is a major public health concern, particularly due to its association with risky sexual behaviour and HIV infection [2].
Depression is a major health problem among HIV-positive MSM and is characterized by a persistent low mood or loss of pleasure or interest in activities [14]. Patients with depression experience psychological distress, loss of pleasure, feelings of guilt, disturbances in sleep and eating, and physical fatigue. These symptoms can be long-lasting or recurrent, severely affecting an individual’s studies, work, and daily life, among other things [14]. MSM often face discrimination and stigma from society, family and the workplace. Low family acceptance of their sexual orientation [10], bullying and rejection in social settings, lack of support from friends, family and community in accessing mental health services further increase their risk of depression. This leads to higher rates of depression among this population and potentially serious consequences.
There is a strong association between human immunodeficiency virus (HIV), depression and MSM [14, 15]. Engaging in high-risk sexual behaviors, having multiple sexual partners, inconsistent use of protection, low HIV testing rates, inadequate education and awareness, and the presence of other sexually transmitted infections (STIs) can all contribute to an increased risk of HIV transmission and higher levels of depression among the MSM population [2, 16, 17].
While some research has been conducted on HIV infection in the MSM population and on the psychological status of HIV-positive MSM [2, 18, 19], the psychological status of the MSM population may differ by HIV infection status. There is limited research on depression and its influencing factors among different HIV infection statuses in the MSM population. This study aims to investigate the prevalence of depression in the MSM population, the depression status of MSM by HIV infection status, and the factors influencing depression. The findings will provide valuable insights for the local government and relevant departments to develop appropriate strategies to reduce the prevalence of depression in the MSM population, promote their mental health, and reduce the incidence and spread of HIV/AIDS and sexually transmitted diseases.
Methods
Study participants
This study was a cross-sectional survey conducted from March to June 2024 in Eastern China. Given the privacy-sensitive nature of the MSM community, the survey was conducted anonymously via the Internet. The questionnaire was disseminated through an Internet-based comprehensive service platform for HIV prevention and control tailored for the MSM population. To ensure broad coverage and targeted reach, the survey was widely distributed via social platforms such as WeChat groups and QQ groups within the MSM community. Data collection was facilitated through the Golden Data website (www.jinshuju.com). To enhance participation, an incentive policy was implemented to encourage WeChat user to complete the questionnaire. Upon questionnaire completion, each participant received an online gift worth approximately 10 CNY. Each IP address was permitted to submit the questionnaire only once to prevent duplicate entries, and all responses were collected anonymously. Six trained professionals were assigned to oversee data collection and implement quality control measures. Any submitted data that were incomplete or contained logical errors were excluded from the analysis.
Inclusion and exclusion criteria
The inclusion criteria for this study were as follows: (1) men who have sex with men; (2) age ≥ 18 years; (3) ability to read and complete the questionnaire; (4) proficiency in operating mobile phones; and (5) provision of informed consent and voluntary participation. Exclusion criteria: Participants with incomplete responses or logical errors in their answers were excluded.
Study instruments
The questionnaire was designed by the researchers themselves and comprised three parts: basic socio-demographic information of the respondents, HIV-related information and the Patient Health Questionnaire (PHQ-9). Basic personal information includes age, occupation, marital status, education, personal income, religious beliefs, employment status, and place of residence. HIV-related information covered HIV test status, syphilis test status, hepatitis C test status, anti-HIV medication status, sexual behavior with men and women, and HIV disclosure status. For more details, see the supplementary file. The PHQ-9 is a widely utilized assessment tool consisting of nine items, each scored on a four-point scale ranging from 0 to 3, with the total score ranging from 0 to 27. Scores of 0–4 were classified as no depressive symptoms, 5–9 as mild, 10–14 as moderate, 15–19 as moderate-severe, and 20–27 as severe. For the purpose of this study, a score of ≥ 10 was used as the cut-off for possible depressive symptoms. The scale has good reliability and validity [20].
Statistical methods
SPSS 26.0 software was used for statistical analysis. Count data were expressed as the number of cases (percentage), and the chi-squared test was used for intergroup comparisons. Binary logistic regression was used to analyse the factors associated with depression in the MSM population, and variables that were significant in the univariate analyses were included in the logistic regression analyses and decision tree modelling. Statistical inference was performed using the two-tailed test, with P < 0.05 as a statistically significant difference.
Decision tree model
To identify determinants of depression in the MSM population, we applied the Chi-square Automatic Interaction Detector (CHAID) decision tree model, entering depression as the dependent variable and all statistically significant factors from the univariate analysis as the independent variables. CHAID decision tree model was preferred because it efficiently handles categorical variables, exposes interaction effects, and generates an intuitive tree diagram that dovetails with logistic regression, offering a clear, complementary view of how risk factors combine to shape depressive symptoms. The parameters of the CHAID decision tree model were set as follows: the significance level of the split nodes and merged categories of the decision tree was set at 0.05. The growth depth of the decision tree was 3 levels, and the minimum number of cases for the parent and child nodes were 50 and 30, respectively; if the sample size of a node did not meet the minimum requirement, the node became the terminal node and was not further split.
Ethical review
This study was reviewed and approved by the Ethics Committee of the Affiliated Kangning Hospital of Wenzhou Medical University (Grant No. 2023014). The research was conducted in line with the Declaration of Helsinki and Good Clinical Practice. Before conducting the investigation, each respondent was informed that the information collected during this survey would be kept confidential and would not be disclosed; The data was kept by a special person. Informed consent to participate was obtained from all of the participants in the study. If informed consent was not obtained from the respondents, they could not participate in the survey.
Results
Participant characteristics
A total of 1 113 MSM were recruited for this survey, 43 questionnaires with incomplete or logical errors were excluded, 1070 individuals met the inclusion criteria, giving a valid response rate of 96.1%. The age of the respondents ranged from 18 to 65 years, with a mean of (28.5 ± 8.5) years, of which 9.0% were 19 years old or younger (96/1 070); 79.3% were unmarried (848/1 070); 12.8% had an educational level of junior high school or lower (137/1 070); 15.2% had a monthly income of ≤ 1 999 yuan (163/1 070); and 64.6% had no religious beliefs. In terms of employment, 28.7% (307/1 070) were unemployed and 66.3% (709/1 070) lived in urban areas. Regarding sexual behavior in the last six months, 62.1% (664/1 070) had sex with men, and 12.1% (129/1 070) had sex with women. In terms of testing results, 0.4% (4/1 070) tested positive for hepatitis C; 2.4% (26/1070) tested positive for syphilis; and 3.4% (36/1 070) tested positive for HIV. For more details, please refer to Table 1.
Table 1. Univariate analysis of factors influencing depression in the MSM populationVariablesNon-depressionDepressionΧ^2^ P Age, years 18–19603626.893˂0.0001 20–29390189 30–3920370 40–497310 ≥ 50354Occupation Administrative clerks89264.8910.299 Agriculture, forestry, fisheries and transport staff6319 Commercial services10953 Professionals12050 Others380161Marital status Unmarried57827017.648˂0.0001 Married15231 Divorced and widowed318Education background Junior high school or below100375.8440.119 High School14445 College200101 University or above317126Monthly income, CNY ≤ 1999106578.7800.032 2000–399910355 4000–599925297 ≥ 6000300100Religious belief Buddhism187696.3690.272 Christianity5132 Catholicism105 Islam42 Others118 No Religion498193Whether employment Unemployed19111616.628˂0.0001 Employed570193 HIV testing HIV(--)64022815.6820.001 HIV (+)2016 Never tested8051 Unwilling to tell test results2114Whether taking anti-HIV medication No7422899.8910.007 Yes1920Whether syphilis tested (–)5572074.7560.191 (+)197 Never tested for syphilis16284 Unwilling to tell test results2311Whether HCV tested (–)56019811.3860.010 (+)31 Never tested for HCV17592 Unwilling to tell test results2318Sexual activity with men in the last 6 months No2861200.1460.702 Yes475189Sexual activity with woman in the last 6 months No6642771.1840.276 Yes9732Disclosure of HIV test results Self-knowledge only46017210.2170.037 Family member knows3220 Friends know18970 Others8047Place of residence Rural area2511100.6730.412 Urban area510199
Univariate analysis of factors associated with depression in the MSM population
Among the 1070 MSM, 309 (28.9%) exhibited depressive symptoms. Univariate analysis revealed that the prevalence of depressive symptoms in the MSM population was statistically significantly different in relation to age, marital status, income, employment status and HIV testing, use of anti-HIV medication, hepatitis C testing and disclosure of HIV test results (p < 0. 05). In contrast, the prevalence of depression did not show statistically significantly difference with respect to occupation, education, religion, syphilis testing, sex with men in the last 6 months, sex with women in the last 6 months and place of residence (P > 0.05). See Table 1.
Logistic regression analysis of factors associated with depression in the MSM population
Eight variables were selected for logistic regression analysis based on their statistical significance in the univariate analysis: age, marital status, income, employment status, HIV test status, use of anti-HIV medication, hepatitis C test status, and disclosure of HIV test results. The results indicated that age and employment status were independent factors influencing depression in the MSM population. Specifically, the odds ratio (OR) for depression in individuals aged 40–49 years compared with ≤ 19 years was 0.347 (95% CI 0.142–0.846), indicating a lower risk of depression in the 40–49 age group. Additionally, the OR for depression in employed individuals compared to unemployed individuals was 0.572 (95% CI 0.394–0.831), suggesting that employment was associated with a lower risk of depression than unemployment. See Table 2.Table 2. Logistic regression analysis of factors influencing depression in the MSM populationVariablesβS.EWaldSignificanceExp(B)95% CI of EXP(B)LowerUpperAge, years ≤ 1910.4940.033 20–290.0680.2500.0740.7851.0710.6551.749 30–39−0.1720.2890.3530.5520.8420.4781.483 40–49−1.0600.4555.4190.0200.3470.1420.846 ≥ 50−1.1500.6243.3910.0660.3170.0931.077Marital status Unmarried1.5800.454 Married−0.3190.2541.5760.2090.7270.4421.196 Divorced and widowed−0.1400.4490.0970.7550.8690.3602.098Monthly income, CNY ≤ 19991.8070.613 2000–39990.2960.2571.3270.2491.3450.8122.226 4000–59990.3010.2531.4150.2341.3510.8232.219 ≥ 60000.2110.2610.6570.4181.2350.7412.060 Employment status: Employed−0.5580.1908.6110.0030.5720.3940.831Whether HIV tested (–)1.8680.600 (+)0.2280.4970.2110.6461.2560.4753.325 Never tested0.1300.2730.2270.6341.1390.6671.947 Unwilling to tell test results0.5180.4091.6030.2051.6790.7533.744Whether taking anti-HIV medication No4.4130.110 Yes0.8100.4653.0270.0822.2470.9035.596Whether HCV tested (–)1.8100.613 (+)0.0501.2040.0020.9671.0510.09911.132 Never tested0.1380.1940.5080.4761.1480.7851.679 Unwilling to tell test results0.4690.3721.5880.2081.5980.7713.312Disclosure of HIV test results Self-knowledge only3.4910.479 Family member knows0.2140.3320.4150.5201.2380.6462.371 Friends know−0.0460.1730.0710.7900.9550.6801.341 Others−0.2640.4610.3270.5670.7680.3111.896
Decision tree analysis of factors influencing depression in the MSM population
The CHAID decision tree model revealed that employment status and marital status significantly influenced depression occurrence in MSM. The first decision tree layer showed that unemployment was associated with a higher depression rate (37.8%) than employment (25.3%) (χ² = 16.628, P < 0.001). The second layer highlighted marital status as another key factor. Among employed MSM, those who were unmarried exhibited a higher prevalence of depression at 29.2% compared to their married counterparts at 12.4% (χ² = 20.187, P < 0.001). Furthermore, the model indicated an interaction effect between employment status and marital status, as depicted in Fig. 1.
Fig. 1. Decision tree of factors influencing depression in the MSM population
Prevalence of depressive symptoms in the MSM population by HIV status
Among the 1070 MSM, there were 36 HIV-positive cases, yielding an HIV-positive rate of 3.4%. Of these 36 HIV-positive individuals, 16 (44.4%) exhibited depressive symptoms. In contrast, among the 868 HIV-negative participant, 228 (26.3%) had depressive symptoms. Additionally, of the 35 individuals unwilling to disclose their HIV test results, 14 (40.0%) showed depressive symptoms, and of the 131 individuals who had never been tested for HIV, 51 (38.9%) had depressive symptoms. See Table 3 for details.
Table 3. Prevalence of depressive symptoms in the MSM population by HIV statusvariablesNumber of caseNon-depressiondepressionprevalence(%)HIV (+)36201644.4HIV (-)86864022826.3Never HIV tested131805138.9Unwilling to disclose their HIV test results35211440.0Total107076130928.9
Discussions
Depression is more prevalent among MSM than in the general population in both developed and developing countries [1], yet its prevalence varies across regions [2, 11, 21]. In the U.S. and Australia, depression rates among MSM from 22.8% to 33% [2, 11], while in France, depression prevalence was 28.1% among MSM [22]. Even within the U.S., rates also vary by state, ranging from 22.8% in Seattle and 23.1% in Chicago to 33% in Massachusetts [11–13]. The Tanzanian study found a prevalence of depression among MSM of 46.3% [2] and two studies in South Africa reported prevalence rates of 44% and 56% [2, 21, 23]. Our survey found a 28.9% depression rate among MSM, lower than in Tanzania, South Africa, and Australia [2, 11] but higher than in Chicago and Seattle [2, 11], and similar to the prevalence observed in France [22]. This heterogeneity signals that locally salient stressors—rather than a universal minority stress—drive poor mental health. Tailoring interventions therefore requires unpacking context-specific risk profiles instead of importing “one-size-fits-all” programmes.
Our decision-tree analysis identified two modifiable nodes that increased depression risk locally: unemployment and being unmarried. Embedding these findings into an operational definition of ‘effectiveness’ strives to meet international standards while considering local realities. Consistent with criteria used in nutrition-behaviour trials and physical-activity interventions for socially isolated older adults [24, 25], we define an effective anti-depression intervention for MSM as one that, relative to control or baseline: (1) achieves a statistically significant and clinically meaningful improvement (≥ 6-point PHQ-9 reduction [26], 20% reduction in PHQ−9 scores [27], or Cohen’s d ≥ 0.3) [28]; and (2) is acceptable, scalable and sustainable in the setting where it will run. Translating this definition into practice, eastern-China health authorities could integrate three low-cost, high-feasibility components into the existing digital HIV-prevention ecosystem: (1) Embed a two-minute PHQ-9 screen into the HIV-testing apps already ubiquitous among local MSM, ensuring seamless uptake without additional download burden. (2) Upon simultaneous completion of HIV testing and the depression scale, instantly issue an appropriate number of small-denomination cash top-up vouchers (e.g., ¥20) or e-coupons for vocational-training courses, directly offsetting the unemployment pathway while incentivising completion. (3) Push time-limited WeChat-mini-program coupons for free or subsidised counselling that is explicitly branded “partner-friendly”, reducing the help-seeking barrier faced by unmarried men who lack spousal encouragement. All elements leverage the region’s near-universal smartphone ownership and the same platform that hosted our survey, guaranteeing rapid uptake, cultural congruence and immediate action on the risk factors our model uncovered. By anchoring effectiveness benchmarks to internationally recognised thresholds while delivering the intervention through locally embedded, app-based touch-points, we reconcile global rigour with contextual relevance—an alignment that, according to our data, is indispensable if the mental-health gap among Chinese MSM is to close.
Employment status, marital status and age have a significant impact on depression in the MSM population in our study. Several studies indicate unemployment can increases stress, anxiety and even depression [29, 30]. The present study show that the prevalence of depression was significantly higher among the unemployed than among the employed, which is consistent with the above findings [29, 31, 32].
The effect of marital status on depression is variable [33, 34]. Some studies suggest that married individuals may be more prone to depression than unmarried one [2]. For instance, Yang et al. [33] reported that currently married MSM had the highest depression symptoms compared to single and divorced individuals. However, other studies indicated that married MSM has not a higher prevalence of depression than, single or divorced people [34]. In our study, being married was a significant determinant associated with higher depression in the MSM population. These discrepancies may stem from differences in study periods, sites, population, subgroup compositions, and measurement tools [35].
The present study shows that the risk of depression was lower in those aged 40–49 years than in those ≤ 19 years, which is consistent with the report by Thirunavukkarasu et al. [10, 33] but is not consistent with other studies [34, 36]. The reasons for the different results need to be further investigated in the future.
While numerous studies have reported the prevalence of depression in HIV-positive MSM populations [14, 37–39], comparatively fewer have focused on the prevalence of depression in HIV-negative MSM populations. Nouri et al. [35] reported a 47% prevalence of depression among 3 753 HIV-positive MSM in 11 studies, compared with a 33% prevalence among 47 788 HIV-negative MSM in 60 studies. The prevalence of depression was significantly higher among HIV-infected MSM than among HIV-uninfected MSM. Among the 1 070 MSM in our study, the overall HIV prevalence was 3.4%. Among HIV-positive individuals, 44.4% were depressed, compared with 26.3% of HIV-negative individuals. Although HIV-positive MSM had a significantly higher rate of depression than HIV-negative individuals in unadjusted analysis, this association was not significant after adjusting for covariates. This finding does not aligns studies indicating that HIV-positive MSM in sub-Saharan Africa have higher depression rates [14, 40, 41]. This discrepancy may be due to regional differences in social determinants of health, access to healthcare, or study methodologies. Thus, enhanced social support and psychological counseling for MSM, regardless of HIV status, are crucial to reducing depression. Implementing targeted interventions that address the specific needs of MSM and promoting mental health literacy can contribute to improved mental health outcomes in this population.
Decision tree algorithms and logistic regression are widely used clinically for the prediction and analysis of various disease risk factors [42–47]. Decision tree, as a machine learning method, is intuitive use of probabilistic analysis of a graphical method. It is easy to implement, sensitive to the data analysis, interpretable, and can be visualised and analyzed, fully aligning with human intuitive thinking, and thus having a wide range of applications. However, the decision tree model is rarely used for analyzing depression-related factors. Furthermore, after searching several databases such as PubMed, no studies were found that used the decision tree algorithm for predicting or analyzing depression risk factors in the MSM population. In this study, the Chi-Square Automatic Interaction Detector (CHAID) decision tree algorithm combined with a logistic regression model was used to analyse the factors associated with depression in the MSM population.
Our finding highlights the complementary strengths of using both logistic regression and decision tree models in analyzing depression among MSM. The logistic regression identifies age and employment status as key independent factors influencing depression, underscoring the importance of these variables in traditional statistical analysis. Meanwhile, the CHAID decision tree model not only corroborates the significance of employment status but also reveals marital status as an additional influential factor. This suggests that the decision tree model can capture nuances in the data that logistic regression might miss, possibly due to its ability to handle non-linear relationships and interactions between variables more flexibly. The fact that marital status emerged as a factor in the decision tree but not in the logistic regression could indicate that its effect is more complex or context-dependent, and might be better uncovered through the decision tree’s partitioning approach. Overall, this demonstrates how combining these analytical methods can provide a more comprehensive understanding of the factors associated with depression in the MSM population, potentially leading to more effective and targeted interventions.
Limitations
This study has the following limitations: First, this is a cross-sectional survey. As such, the data were collected at a single point in time, which means the results can only show associations and cannot establish causality. Second, depressive symptoms and HIV status were self-reported by the study participants. Self-reported data can be subject to biases. Participants might not remember accurately or might be hesitant to report certain information due to social stigma or other concerns. This could lead to information bias, where the data might not fully reflect the true situation. Third, due to the sensitive and privacy nature of the MSM population, some potential influencing factors were not included in this study. For instance, detailed information on specific behaviors or social contexts that could influence the outcomes was not collected. This limitation means that our findings might not capture all the important factors at play. Overall, while our study provides valuable insights, these limitations should be considered when interpreting the results. Future research could benefit from longitudinal designs, more comprehensive data collection methods, and additional validation of self-reported information to address these issues.
Conclusion
This study examined the depression status of the MSM population, explored the depression characteristics associated with different HIV statuses within this group, and applied decision tree modelling and logistic regression to assess the factors influencing depression. Among the 1070 MSM studied, the depression prevalence was 28.9%, with an overall HIV prevalence was 3.4%. The decision tree algorithms combined with logistic regression modelling showed that marital status, age and employment status were the factors influencing depression in this population. The combined use of the two methods can complement each other and improve the analytical effect. These findings provide a scientific basis for the government and relevant departments to develop targeted measure. These findings provide a scientific basis for governments and relevant departments to develop targeted measures. Such measures can help reduce depression rates in the MSM population, promote their physical and mental well - being, and lower the incidence of STDs and AIDS.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ahaneku H, Ross MW, Nyoni JE, et al. Depression and HIV risk among men who have sex with men in Tanzania. AIDS Care. 2016;28(Suppl 1):140–7. 10.1080/09540121.2016.1146207.10.1080/09540121.2016.1146207 PMC 485932027002772 · doi ↗ · pubmed ↗
- 2Reisner SL, Mimiaga MJ, Skeer M, Bright D, Cranston K, Isenberg D, et al. Clinically significant depressive symptoms as a risk factor for HIV infection among black MSM in Massachusetts. AIDS Behav. 2009(4). 10.1007/s 10461-009-9571-9.10.1007/s 10461-009-9571-9PMC 394741119462228 · doi ↗ · pubmed ↗
- 3Fendrich M, Avci O, Johnson TP, Mackesy-Amiti ME. Depression, substance use and HIV risk in a probability sample of men who have sex with men. Addict Behav. 2013(3):1715–8. 10.1016/j.addbeh.2012.09.00510.1016/j.addbeh.2012.09.005PMC 361919823254224 · doi ↗ · pubmed ↗
- 4Perdue T, Hagan H, Thiede H, Valleroy L. Depression and HIV risk behavior among Seattle-area injection drug users and young men who have sex with men. AIDS Educ Prev. 2003(1). 10.1521/aeap.15.1.81.23842.10.1521/aeap.15.1.81.2384212627745 · doi ↗ · pubmed ↗
- 5Mulqueeny DM, Nkabini SM, Pokiya MH. Mapping evidence of depression in HIV-seropositive MSM in sub-Saharan africa: a scoping review protocol. Syst Rev. 2021;10(1):50. 10.1186/s 13643-021-01604-w.10.1186/s 13643-021-01604-w PMC 786645633546768 · doi ↗ · pubmed ↗
- 6Xiao L, Qi H, Wang YY, et al. The prevalence of depression in men who have sex with men (MSM) living with HIV: A meta-analysis of comparative and epidemiological studies. Gen Hosp Psychiatry. 2020;66:112–9. 10.1016/j.genhosppsych.2020.04.001.32818791 · doi ↗ · pubmed ↗
- 7Li Y, Cai M, Qin S, Lu X. Depressive emotion detection and behavior analysis of men who have sex with men via social media. Front Psychiatry. 2020;11:830. 10.3389/fpsyt.2020.00830.10.3389/fpsyt.2020.00830 PMC 745691132922323 · doi ↗ · pubmed ↗
- 8Tucker A, Liht J, de Swardt G, et al. An exploration into the role of depression and self-efficacy on township men who have sex with men’s ability to engage in safer sexual practices. AIDS Care. 2013(10):1227–35. 10.1080/09540121.2013.76438310.1080/09540121.2013.76438323387517 · doi ↗ · pubmed ↗