Oxiracetam and physical activity in preventing cognitive decline after stroke: A multicenter, randomized controlled trial
Jae-Sung Lim, Joung-Ho Rha, Jong-Ho Park, Kyungbok Lee, Dae-Il Chang, Sung Hyuk Heo, Yeong Bae Lee, Jee-Hyun Kwon, Eung-Gyu Kim, Jay Chol Choi, Man-Seok Park, Kyung-Hee Cho, Jae-Kwan Cha, Mi Sun Oh, Byung-Chul Lee, Hahn Young Kim, Kyungmi Oh, Hyun-Young Park, Sanghak Yi

TL;DR
A study in South Korea found that oxiracetam did not help prevent cognitive decline after stroke, even when combined with physical activity.
Contribution
This is the first multicenter trial to evaluate oxiracetam's efficacy in preventing post-stroke cognitive impairment and its interaction with physical activity.
Findings
Oxiracetam showed no significant effect on cognitive outcomes compared to placebo.
No interaction was found between oxiracetam and physical activity in preventing cognitive decline.
Exploratory data suggested possible benefits in highly active oxiracetam participants.
Abstract
This multicenter, double-blind, placebo-controlled trial, commissioned by South Korea’s Ministry of Food and Drug Safety, evaluated the effect of oxiracetam for preventing post-stroke cognitive impairment (PSCI) and explored potential interaction with physical activity using neuroimaging. Patients at high risk of PSCI, reporting subjective cognitive decline ⩾3 months after stroke, were randomized 1:1 to receive oxiracetam or placebo for 36 weeks. Physical activity was tracked via wrist-worn actigraphy. Coprimary endpoints were changes in Mini-Mental State Examination (MMSE) and Clinical Dementia Rating–Sum of Boxes (CDR-SB). Secondary outcomes included neuropsychological assessments and resting-state functional magnetic resonance imaging network metrics. Of 500 enrolled participants (mean age 68.9 years; median 32 months post-stroke), 457 completed the study. There were no…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
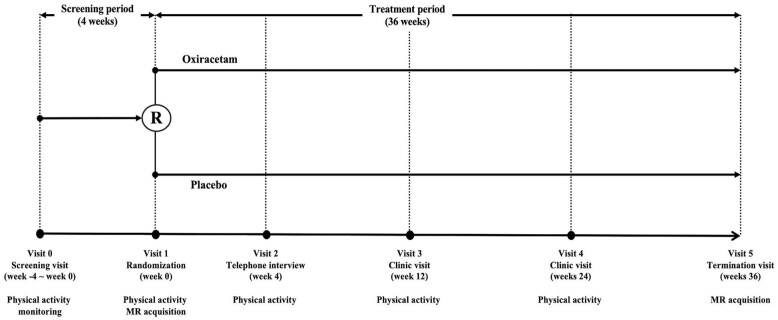 Figure 1
Figure 1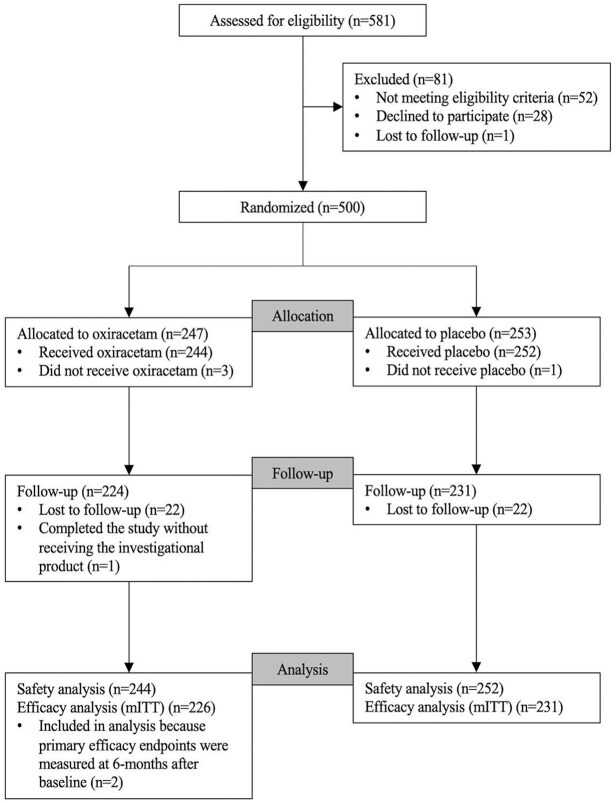 Figure 2
Figure 2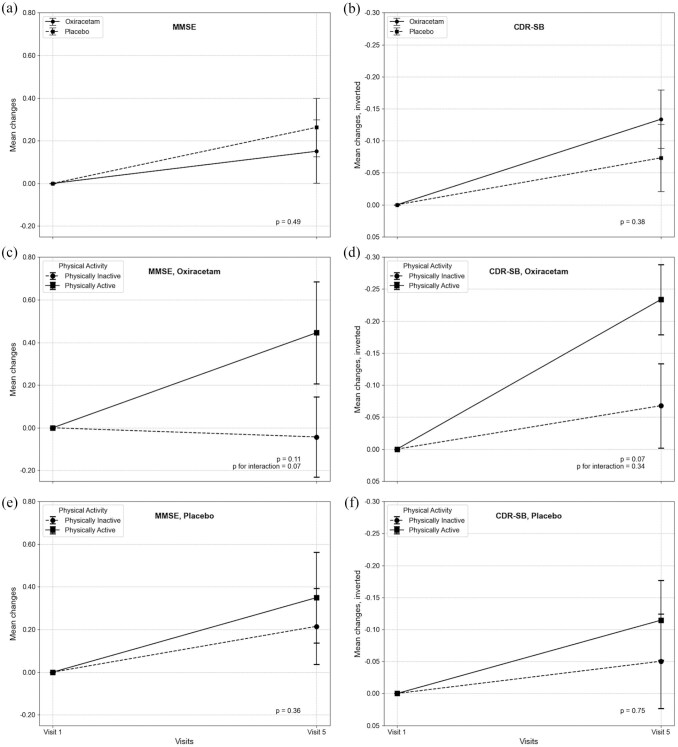 Figure 3
Figure 3| Characteristic | Oxiracetam ( | Placebo ( | Total ( |
|---|---|---|---|
| Age, years | 68.8 ± 8.6 | 69.0 ± 8.9 | 68.9 ± 8.7 |
| ⩾70 years old | 114 (50.4%) | 120 (51.9%) | 234 (51.2%) |
| Female | 56 (24.8%) | 53 (22.9%) | 109 (23.9%) |
| Education, years (median, IQR) | 10.5 (6.0, 12.0) | 12.0 (6.0, 12.0) | 11.0 (6.0, 12.0) |
| Elementary school | 67 (29.7%) | 62 (26.8%) | 129 (28.2%) |
| Middle school | 43 (19.0%) | 49 (21.1%) | 92 (20.1%) |
| High school | 74 (32.7%) | 74 (32.0%) | 148 (32.4%) |
| University or above | 42 (18.6%) | 46 (19.9%) | 88 (19.3%) |
| Interval from stroke onset to randomization, months (median, IQR) | 28.3 (12.4, 73.8) | 34.3 (12.9, 70.8) | 31.7 (12.7, 71.7) |
| Hypertension | 182 (80.5%) | 186 (80.5%) | 368 (80.5%) |
| Diabetes mellitus | 101 (44.7%) | 100 (43.3%) | 201 (44.0%) |
| Dyslipidemia | 156 (69.0%) | 154 (66.7%) | 310 (67.8%) |
| Atrial fibrillation/flutter | 45 (19.9%) | 38 (16.5%) | 83 (18.2%) |
| Ischemic heart disease | 27 (11.9%) | 21 (9.1%) | 48 (10.5%) |
| Heart failure | 4 (1.8%) | 6 (2.6%) | 10 (2.2%) |
| Current smoking | 40 (16.2%) | 52 (20.6%) | 92 (20.1%) |
| Body mass index (kg/m2) | 25.0±3.3 | 24.5±3.0 | 24.7±3.1 |
| Systolic blood pressure | 128.3±14.5 | 130.2±13.4 | 129.3±14.0 |
| Diastolic blood pressure | 74.5±9.9 | 74.6±9.4 | 74.5±9.6 |
| Heart rates | 77.8±11.4 | 75.8±11.9 | 76.8±11.7 |
| History of recurrent stroke | 35 (15.5%) | 36 (15.6%) | 71 (15.5%) |
| Index stroke TOAST | |||
| LAA | 82 (36.3%) | 79 (34.2%) | 161 (35.2%) |
| CE | 38 (16.8%) | 38 (16.5%) | 76 (16.6%) |
| SVO | 70 (31.0%) | 73 (31.6%) | 143 (31.3%) |
| OD | 15 (6.6%) | 14 (6.1%) | 29 (6.3%) |
| UD | 21 (9.3%) | 23 (10.0%) | 44 (9.6%) |
| Index stroke NIHSS (median, IQR) | 2.0 (1.0, 4.0) | 3.0 (1.0, 5.0) | 2.0 (1.0, 4.0) |
| Baseline NIHSS (median, IQR) | 0 (0, 1.0) | 0 (0, 1.0) | 0 (0, 1.0) |
| Baseline mRS, 0/1/2 | 105 (46.5%)/97 (42.9%)/ | 115 (49.8%)/86 (37.2%)/ | 220 (48.1%)/183 (40.0%)/54 (11.8%) |
| Index stroke imaging: acute | |||
| Cortical involvement | 96 (43.2%) | 79 (35.6%) | 175 (38.3%) |
| Left-hemispheric involvement | 125 (50.6%) | 139 (54.9%) | 264 (57.8%) |
| Multiple lesions | 108 (48.6%) | 106 (47.7%) | 214 (46.8%) |
| Index stroke imaging: chronic | |||
| Periventricular WMH, Fazekas 0/1/2/3 | 0 (0.0%)/114 (54.3%)/ | 0 (0.0%)/118 (54.1%)/56 (25.7%)/44 (20.2%) | 0 (0.0%)/232 (50.8%)/ |
| Subcortical WMH, Fazekas 0/1/2/3 | 19 (9.0%)/ 139 (66.2%)/ 43 (20.5%)/ 9 (4.3%) | 22 (10.1%)/123 (56.4%)/ 61 (28.0%)/ 12 (5.5%) | 41 (9.0%)/262 (57.3%)/104 (22.8%) / 21 (4.6%) |
| Number of cerebral microbleeds | 4.12±7.78 | 5.14±11.39 | 4.63±9.78 |
| Number of lacunes | 2.23±3.38 | 2.43±3.19 | 2.33±3.29 |
| Cerebral hemorrhage | 2 (0.9%) | 9 (3.9%) | 11 (2.4%) |
| Chronic territorial infarction | 15 (6.6%) | 15 (6.5%) | 30 (6.6%) |
| Medial temporal atrophy, Scheltens 0/1/2/3/4 | 90 (40.0%)/ 57 (25.3%)/ | 86 (37.7%) / 63 (27.6%)/ | 176 (38.5%) / 120 (26.3%)/ |
| Global cortical atrophy 2 or more | 46 (22.3%) | 35 (17.4%) | 81 (17.7%) |
| SCD-Q scores | 11.69±4.35 | 11.11±3.85 | 11.39±4.11 |
| Mini-Mental State Examination | 26.58±2.57 | 26.64±2.60 | 26.61±2.58 |
| CDR-sum of boxes | |||
| 0 | 32 (14.2%) | 34 (14.7%) | 66 (14.4%) |
| 0.5 | 185 (81.9%) | 189 (81.8%) | 374 (81.8%) |
| 1.0 | 9 (4.0%) | 8 (3.5%) | 17 (3.7%) |
| SGDS ⩾ 8 | 67 (29.6%) | 57 (24.7%) | 124 (27.1%) |
| Neuroimaging (normalized) | |||
| Global efficiency | 0.85±0.03 | 0.85±0.03 | 0.85±0.03 |
| Characteristic path length | 1.26±0.07 | 1.27±0.07 | 1.26±0.07 |
| Clustering coefficient | 1.73±0.28 | 1.74±0.27 | 1.74±0.28 |
| Modularity | 3.35±0.41 | 3.36±0.39 | 3.35±0.40 |
| Physical activity levels | |||
| Baseline MVPA duration, minutes | 23.2±23.0 | 24.1±28.7 | 23.7±26.1 |
| Baseline MVPA duration ⩾ 20 min | 148 (65.5%) | 152 (65.8%) | 300 (65.6%) |
| Endpoints | Oxiracetam ( | Placebo ( |
|
|
|
|
|---|---|---|---|---|---|---|
| Primary endpoints | ||||||
| MMSE | 0.13 ± 2.27 | 0.27 ± 2.09 | 0.49 | 0.50 | 0.43 | 0.07 |
| CDR-SB | −0.14 ± 0.70 | −0.08 ± 0.80 | 0.38 | 0.40 | 0.51 | 0.34 |
|
| ||||||
| SVLT-E immediate recall | 0.28 ± 0.85 | 0.28 ± 0.80 | 0.69 | 0.99 | 0.95 | 0.09 |
| SVLT-E delayed recall | 0.28 ± 0.87 | 0.18 ± 0.83 | 0.21 | 0.13 | 0.47 | 0.46 |
| SVLT-E recognition | 0.18 ± 1.17 | 0.24 ± 1.17 | 0.59 | 0.32 | 0.92 | 0.24 |
| Semantic fluency | 0.01 ± 0.78 | 0.03 ± 0.75 | 0.85 | 0.99 | 0.46 | 0.98 |
| Phonemic fluency | 0.15 ± 0.69 | 0.17 ± 0.71 | 0.78 | 0.95 | 0.63 | 0.55 |
| Digit symbol coding | 0.08 ± 0.60 | 0.06 ± 0.50 | 0.82 | 0.65 | 0.57 | 0.11 |
| TMT-E part A | 0.004 ± 1.13 | 0.16 ± 1.11 | 0.14 | 0.37 | 0.13 | 0.11 |
| TMT-E part B | 0.12 ± 1.59 | −0.03 ± 1.24 | 0.25 | 0.30 | 0.30 | 0.46 |
| Short BNT | 0.23 ± 1.10 | 0.14 ± 0.74 | 0.34 | 0.43 | 0.07 | 0.60 |
| RCFT | 0.15 ± 1.22 | 0.004 ± 1.13 | 0.19 | 0.10 | 0.09 | 0.052 |
| NPI-Q | −0.49 ± 3.31 | −0.46 ± 2.97 | 0.95 | 0.99 | 0.71 | 0.64 |
| SGDS | −0.88 ± 3.46 | −1.00 ± 2.88 | 0.69 | 0.50 | 0.51 | 0.20 |
| IADL | −0.01 ± 0.20 | −0.03 ± 0.18 | 0.27 | 0.27 | 0.43 | 0.84 |
| Memory domain z-score | 0.25 ± 0.71 | 0.23 ± 0.66 | 0.85 | 0.97 | 0.73 | 0.63 |
| Frontal domain z-score | 0.07 ± 0.58 | 0.08 ± 0.46 | 0.92 | 0.79 | 0.86 | 0.19 |
| Global cognitive function z-score | 0.18 ± 0.51 | 0.11 ± 0.39 | 0.16 | 0.14 | 0.04 | 0.22 |
| EuroQoL | −0.24 ± 1.13 | −0.22 ± 1.41 | 0.85 | 0.99 | 0.90 | 0.17 |
| PGA at Visit 5 | 3.60 ± 0.82 | 3.53 ± 0.85 | 0.37 | 0.53 | ||
| Significantly improved | 5 (2.2%) | 5 (2.2%) | 0.86 | |||
| Moderately improved | 14 (6.2%) | 22 (9.5%) | ||||
| Mildly improved | 64 (28.3%) | 64 (27.7%) | ||||
| Almost the same | 128 (56.6%) | 127 (55.0%) | ||||
| Mildly worse | 13. (5.8%) | 11 (4.8%) | ||||
| Moderately worse | 2 (0.9%) | 2 (0.9%) | ||||
| Significantly worse | 0 (0%) | 0 (0%) | ||||
| Global efficiency | −0.004±0.038 | −0.002±0.039 | 0.55 | 0.94 | 0.52 | 0.70 |
| Characteristic path length | 0.005±0.089 | 0.002±0.085 | 0.73 | 0.86 | 0.36 | 0.81 |
| Clustering coefficient | 0.036±0.330 | 0.015±0.344 | 0.52 | 0.04 | 0.20 | 0.96 |
| Modularity | 0.039±0.484 | 0.016±0.524 | 0.63 | 0.96 | 0.76 | 0.73 |
| Adverse events | Oxiracetam ( | Placebo ( |
|
|---|---|---|---|
| Any AE | 100 (41.0%) | 88 (34.9%) | 0.16 |
| Any serious AE | 21 (8.6%) | 16 (6.3%) | 0.34 |
| Any serious AE causing treatment discontinuation | 3 (1.2%) | 1 (0.4%) | 0.46 |
| Serious AE by SOC term | |||
| Cardiac | 3 (1.2%) | 2 (0.8%) | 0.43 |
| Gastrointestinal | 1 (0.4%) | 3 (1.2%) | 0.99 |
| Hepatobiliary | 1 (0.4%) | 0 (0%) | n/a |
| Infections | 1 (0.4%) | 1 (0.4%) | n/a |
| Injury, poisoning and procedural complications | 1 (0.4%) | 4 (1.6%) | 0.74 |
| Musculoskeletal and connective tissue disorders | 4 (1.6%) | 2 (0.8%) | 0.16 |
| Neoplasm | 4 (1.6%) | 3 (1.2%) | 0.15 |
| Nervous system | 4 (1.6%) | 1 (0.4%) | 0.74 |
| Renal and urinary | 0 (0%) | 1 (0.4%) | n/a |
| Reproductive and breast | 1 (0.4%) | 0 (0%) | n/a |
| Skin and subcutaneous tissue | 0 (0%) | 1 (0.4%) | n/a |
| Vascular | 1 (0.4%) | 0 (0%) | n/a |
- —Korean Drug Company, Ltd.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEEG and Brain-Computer Interfaces · Stroke Rehabilitation and Recovery · Phosphodiesterase function and regulation
Introduction
Post-stroke cognitive impairment (PSCI) is a common consequence of stroke, impairing functional recovery and long-term quality of life.^1^ Despite its clinical relevance, effective pharmacologic treatments remain limited. In South Korea, nootropics such as oxiracetam are widely prescribed and reimbursed, with annual expenditures reaching 22.8 billion KRW (€17 million) in 2021.^2,3^ However, supporting evidence on its efficacy is largely outdated and inconclusive. In response to the country’s transition to a super-aged society and increasing per capita pharmaceutical spending, the South Korean government has adopted a selective listing policy to prioritize cost-effectiveness and evidence-based therapies. This trial was commissioned by the Ministry of Food and Drug Safety (K-MFDS) as part of a national initiative to re-evaluate the clinical utility of legacy drugs such as oxiracetam in high-risk populations, including patients with PSCI.^3^
Oxiracetam, a pyrrolidone derivative, is thought to enhance cognition by stimulating phospholipid biosynthesis, stabilizing neuronal membranes, and promoting cholinergic transmission^4^ – mechanisms potentially relevant in PSCI, where cholinergic deficits and ischemic damage are prevalent.^5^ The dose tested (800 mg twice daily) corresponds to the standard approved regimen in South Korea. Although potential benefits have been reported in Alzheimer’s disease and multi-infarct dementia,^6–8^ clinical evidence in PSCI remains sparse and methodologically inconsistent.
We hypothesized that concurrent physical activity could augment oxiracetam’s effects via shared mechanisms such as hippocampal plasticity and improved cerebral perfusion.^9,10^ The FINGER trial and other multidomain interventions suggest that combining pharmacologic and lifestyle strategies may offer additive benefits.^11^ Accordingly, this trial included a structured physical activity component and monitored participants using wrist-worn actigraphy. To further elucidate related mechanisms, network-level cognitive function was assessed using resting-state functional MRI (rs-fMRI), focusing on measures of functional segregation and integration.^12^
To increase the likelihood of detecting cognitive change, we targeted high-risk individuals for PSCI– advanced age, recurrent stroke, diabetes, atrial fibrillation, and moderate-to-severe white matter hyperintensities (WMH). Prior trials such as PRoFESS and SPS3, which investigated antiplatelet regimens for secondary stroke prevention, also examined cognitive outcomes but failed to show significant treatment effects.^13,14^ Critical reviews of these studies have noted that the lack of observable cognitive decline in both arms may be attributed to the inclusion of predominantly low-risk participants. Based on these insights, we enrolled individuals with established PSCI risk factors to increase the probability of cognitive deterioration during follow-up and thereby better assess potential treatment effects.
This multicenter trial aimed to evaluate whether oxiracetam prevents cognitive decline in high-risk post-stroke patients and whether sustained physical activity influences treatment response. Exploratory neuroimaging analyses were also conducted to investigate underlying mechanisms.
Patients and methods
Study design, participants, and interventions
This multicenter, double-blind, placebo-controlled trial was conducted at 30 university or general hospitals across South Korea. Eligible participants were aged ⩾50 years, at least 3 months post-stroke, and reported subjective cognitive decline, with one or more additional high-risk profiles for PSCI (Supplemental Table S1).^15^ These high-risk profiles– such as subjective cognitive decline, older age, recurrent stroke, and small vessel disease– were chosen to enrich for individuals likely to decline over 36 weeks.^13^ Subjective cognitive decline was assessed using a stepwise protocol. Participants were asked: “Do you think you have had problems with your memory or other thinking abilities since your stroke?” Patients responding “yes” were further screened using the Subjective Cognitive Decline Questionnaire (SCD-Q),^16^ and the Clinical Dementia Rating (CDR). Those scoring ⩾7 on the SCD-Q or ⩾0.5 on the CDR memory domain were considered eligible. These criteria are detailed in Supplemental Table S1.
Key exclusion criteria included prior oxiracetam or cognitive enhancer use within 1 month, baseline dementia, major neurological or psychiatric illness, severe stroke disability (modified Rankin Scale (mRS) ⩾3 at screening), or unstable medical conditions (Supplemental Table S1). The mRS ranges from 0 (no symptoms) to 5 (severe disability); 6 indicates death.^17^
Participants were randomized 1:1 to receive oxiracetam 800 mg or placebo twice daily for 36 weeks using a stratified block randomization (Figure 1). Stratification was based on site and education (<12 vs ⩾12 years) due to potential confounding.^18,19^ Allocation was concealed via a web-based system. Recruitment spanned from February 2018 to September 2020.
Overview of scheduled visits, assessments, and follow-up timeline.
The design adhered to principles of causal inference framework, with randomization employed to minimize confounding. Physical activity was not randomized but uniformly promoted and monitored using wrist actigraphy. Full design details are provided elsewhere.^20^
Sample size calculations targeted 80% power at a 5% significance level. For MMSE, 120 participants per group were needed to detect a 1.1-point difference (SD = 3.02), and for CDR-SB, 227 per group to detect a 0.19-point difference (SD = 0.71). Accounting for 10% attrition, 506 participants were planned.^20^ Analyses were performed on the modified intention-to-treat (ITT) population – defined as those who received ⩾1 dose of study drug and had both baseline and 36-week MMSE and CDR-SB scores. Safety was evaluated in all participants who received at least one dose of the study drug.
The study was approved by institutional review boards and conducted in accordance with the Declaration of Helsinki. All participants gave written informed consent.
Physical activity
At screening (Visit 0), participants were equipped with wrist-worn actigraphy devices (FITMETER, 32 Hz triaxial accelerometer) and individualized exercise plans based on American College of Sports Medicine and American Heart Association guidelines.^21^
Exercise programs included aerobic, strength, flexibility, and balance components, tailored by baseline mRS. Those with mRS 0–1 performed unassisted standing exercises; those with mRS 2 performed supported modifications. This stratification promoted both safety and comparability (see Supplemental Materials).
Participants received instructional materials and were assessed at weeks 0, 4, 12, 24, and 36. The target was to maintain moderate-to-vigorous physical activity (MVPA) ⩾ 20 min/day (⩾3 METs).^21^ Participants were categorized as active or inactive based on this threshold,^21^ and adherence was supported by regular feedback from study coordinators.
Endpoints assessments
The co-primary endpoints were changes in Mini-Mental State Examination (MMSE) and Clinical Dementia Rating–Sum of Boxes (CDR-SB) from baseline to week 36. Secondary endpoints included changes in: Korean-Vascular Cognitive Impairment Harmonization Standards–Neuropsychology Protocol (K-VCIHS-NP), Korean Instrumental Activities of Daily Living (K-IADL), Neuropsychiatric Inventory (NPI), Short Geriatric Depression Scale (SGDS), EuroQoL, and Patient Global Assessment (PGA).
K-VCIHS-NP scores were standardized using Korean norms.^22^ A composite cognitive z-score was calculated across four domains: executive, language, visuospatial, and memory (Supplemental Methods). Higher MMSE and z-scores indicate better cognition; lower CDR-SB, NPI, SGDS, K-IADL, EuroQoL, and PGA scores reflect improvement.
To estimate minimum clinically important differences (MCIDs), anchor-based analyses were performed using week 36 PGA responses.^20,23^ In PGA, participants responded to the question: “How does your condition compare to before you started treatment with the study drug?” using a 7-point scale (1 = significantly improved to 7 = significantly worse). For oxiracetam, MCIDs were 0.47 (MMSE) and −0.25 (CDR-SB) for PGA ratings of 2–3 (moderate/mild improvement) as anchors, and 0.53 and −0.45, respectively, for ratings of 1–2 (significant/moderate improvement) as anchors.
MRI included T1, rs-fMRI, and DTI with harmonized protocols (Supplemental Table S2). Functional network parameters (e.g. global efficiency, clustering coefficient) were computed and analyzed as secondary outcomes.^24^ Network parameters were normalized to null distributions and assessed using paired t-tests or Wilcoxon signed-rank tests.
Statistical analysis
Baseline characteristics were summarized as means ± SD or medians (IQR) for continuous variables, and as counts (percentages) for categorical variables. Group comparisons were performed using Student’s t-test for normally distributed continuous variables, the Mann–Whitney U test for skewed data, and chi-square or Fisher’s exact tests for categorical variables. Normality was assessed using the Shapiro–Wilk test and visual inspection of histograms.
The co-primary endpoints were analyzed using Student’s t-test or the Mann–Whitney U test. Two-way ANOVA was prespecified to adjust for MVPA imbalance. Secondary endpoints were evaluated using paired and Student’s t-tests or Wilcoxon signed-rank tests.
Multivariable linear mixed models were used to adjust for baseline covariates if imbalances remained despite randomization (p < 0.10), with center as a random effect and education as a fixed effect. Significant treatment-by-covariate interactions were retained in the final models.
As sensitivity analysis, effect modification by physical activity was assessed using MVPA tertiles and two-way ANOVA. MVPA was also modeled continuously in ANCOVA. A sequential conditional mean model (SCMM) accounted for repeated MVPA measurements. Regression models tested interaction terms between treatment and physical activity (active/inactive, or MVPA tertile; see Supplemental Methods).
Participants with missing MMSE or CDR-SB scores at week 36 were excluded from the modified ITT analysis. No imputation was performed for cognitive outcomes. For missing physical activity data (~13%, mainly due to device malfunction), median imputation was performed within strata defined by treatment group and education level.
All statistical tests were two-sided, with a significance threshold of 0.05 for primary and secondary endpoints. A p-value < 0.10 was used to guide the inclusion of covariates in multivariable models and interaction terms in exploratory analyses.^25,26^ All analyses were conducted using SAS^®^ version 9.4 (SAS Institute, Cary, NC, USA).
Results
Participants
A total of 500 patients were randomized to oxiracetam (n = 247) or placebo (n = 253). The modified ITT population included 457 participants, excluding one who did not initiate treatment and 42 lacking co-primary endpoint data (Figure 2). The median time from stroke to randomization was 2.61 years, slightly shorter in the oxiracetam group (2.2 vs 2.6 years).
CONSORT diagram showing participant enrollment, randomization, and analysis populations. The follow-up population includes participants who received at least one dose of study drug and completed both baseline and 36-week cognitive assessments.
Mean age was 68.8 ± 8.6 years (oxiracetam) and 69.0 ± 8.9 years (placebo); women comprised 24.8% and 22.9%, respectively. The trial population (n = 457) showed high PSCI risk: 51% were aged ⩾70, 16% had recurrent stroke, 44% had diabetes, and 24% had moderate-to-severe WMH, with no significant differences between the treatment groups.
Medication adherence was high and similar across groups (oxiracetam: 91%, placebo: 92%, p = 0.46). Baseline imaging showed more cortical involvement in the oxiracetam group (43.2% vs 35.6%), while prior cerebral hemorrhage was more frequent in the placebo group (3.9% vs 0.9%). Depressive symptoms (SGDS ⩾ 8) were reported in 29.6% of oxiracetam and 24.7% of placebo participants (p = 0.23), with no significant group difference at baseline.
Feasibility of physical activity monitoring
Wrist actigraphy successfully recorded activity in 87% of participants. MVPA adherence was similar (oxiracetam: 65.5%, placebo: 65.8%, p = 0.94) with no significant difference in tolerability. Mean daily MVPA duration was also comparable (oxiracetam: 23.2 ± 23.0 min; placebo: 24.1 ± 28.7 min; p = 0.75; Table 1, Supplemental Table S3).
Efficacy outcomes
As baseline MVPA did not differ significantly (p = 0.94), co-primary endpoints were compared using Student’s t-tests. No significant between-group differences were observed in changes from baseline to week 36 in MMSE (+0.13 ± 2.27 vs +0.27 ± 2.09; p = 0.49) or CDR-SB (–0.14 ± 0.70 vs −0.08 ± 0.80; p = 0.38; Tables 1 and 2, Figure 3). These changes did not exceed the MCID thresholds (0.47–0.53 for MMSE; –0.25 to –0.45 for CDR-SB). MMSE improvement ⩾2 points was observed in 25% of the oxiracetam group and 21% of the placebo group (Supplemental Figure S1).
Changes in MMSE and CDR-SB scores from baseline (Visit 1) to week 36 (Visit 5) by treatment allocation and baseline physical activity status (N = 457) Error bars represent standard errors (SE) of the mean changes. (a and b) Mean changes in MMSE and CDR-SB scores for the oxiracetam and placebo groups, respectively. (c and d) Mean changes in MMSE and CDR-SB scores among participants allocated to oxiracetam, stratified by baseline physical activity (Physically Active vs Physically Inactive). (e and f) Corresponding mean changes in the placebo group. For clarity, the direction of the CDR-SB was inverted so that upward trends represent cognitive improvement, as with the MMSE. As physical activity at baseline was balanced across randomized groups, the mean changes in MMSE and CDR-SB scores (follow-up [V5] − baseline scores [V1]) between treatment groups were compared using Student’s t test. In addition, the significance of the interaction effect between treatment group and baseline physical activity was tested using a 5% significance level through multiple linear regression analysis with sequential conditional mean model (SCMM). Physically Active was defined as engaging in ⩾20 min/day of MVPA at baseline; Physically Inactive was defined as <20 min/day of MVPA. Abbreviations: MMSE, mini-mental state examination; CDR-SB, clinical dementia rating-sum of boxes; MVPA, moderate-to-vigorous physical activity.
Secondary endpoints were comparable between groups, though the study was not powered to detect differences in these measures (Table 2). Within-group improvements were noted in global cognitive z-scores (Supplemental Table S4): oxiracetam from −0.49 ± 0.74 to −0.32 ± 0.79, and placebo from −0.46 ± 0.79 to −0.35 ± 0.82 (both p < 0.01). A significant within-group reduction in CDR-SB was observed in the oxiracetam group but not in the placebo group.
In multivariable generalized linear mixed model analyses, adjusting for site, education, and baseline imbalances (p < 0.10), no significant treatment effects were detected for primary or secondary endpoints. However, among brain network metrics, the normalized clustering coefficient was higher in the oxiracetam group compared to placebo (adjusted mean difference in clustering coefficient [β] = 0.09, SE = 0.04, p = 0.04; Supplemental Table S5).
In exploratory sensitivity analysis, participants in the highest MVPA tertile receiving oxiracetam showed greater CDR-SB improvement (–0.28 ± 0.55 vs −0.10 ± 0.50, p < 0.05; Supplemental Figure S2). However, the treatment-by-MVPA interaction was not significant (p = 0.76).
Safety outcomes
Safety was assessed in all 496 participants who received at least one dose. Adverse events occurred in 41.0% of the oxiracetam group (100/244) and 34.9% of the placebo group (88/252; p = 0.16; Table 3). While not statistically significant, this represents a numerically higher incidence in the oxiracetam group. No clinically relevant safety signals attributable to oxiracetam were identified.
Discussion
This multicenter randomized controlled trial evaluated whether oxiracetam prevents PSCI in high-risk patients with subjective cognitive decline, and whether sustained physical activity modifies its effect. Oxiracetam did not show superior efficacy over placebo in preventing PSCI. Across 457 participants with previous stroke and elevated PSCI risk, cognitive function was generally preserved or improved over the 36-week follow-up. Although participants in the highest physical activity tertile showed greater cognitive improvements, no statistically significant interaction with oxiracetam was found.
The trial design incorporated causal inference principles, with randomization aimed to reduce confounding. Physical activity was standardized and closely monitored to support exploratory analyses. However, since it was not randomized, any related findings should be considered hypothesis-generating, not causal. Future trials using factorial designs are needed to examine its interactive effects more definitively.
Our findings did not replicate earlier reports of oxiracetam efficacy in PSCI.^6,7^ We hypothesized additive or synergistic effects with physical activity, but found none. While physical activity is generally associated with cognitive benefit, emerging data suggest its effects may vary by intensity and duration, with some studies reporting neutral or adverse outcomes.^27,28^ Including relatively active participants may have led to selection bias, favoring healthier individuals and attenuating observable treatment effects. Prior research links preserved mobility with better cognition,^29^ suggesting physical activity alone may have contributed to cognitive stability across both groups.
Compared to earlier trials, our participants demonstrated minimal cognitive decline. Rozzini et al. reported a 1.3-point MMSE gain with oxiracetam versus 0.2 with placebo over 2 months.^6^ In contrast, we observed only a 0.13-point gain in the oxiracetam group and 0.27-point gain in the placebo group over 9 months. The higher baseline MMSE in our cohort (mean 26.6 vs 22.1 in Rozzini et al.) likely limited measurable improvement.^6^ Our sample size was based on Winblad et al., who found a 0.19-point CDR-SB difference between galantamine and placebo in MCI.^30^ While PSCI differs from MCI, we deemed them comparable in risk and cognitive status. Nonetheless, both groups in our trial improved (–0.14 vs −0.08), yielding only a 0.06-point difference– far smaller than anticipated.
Notably, 21% of placebo participants improved ⩾2 MMSE points, highlighting the possible role of non-pharmacologic factors, such as sustained physical activity. Nearly 60% met target MVPA levels, and activity adherence was supported through actigraphy feedback and educational resources. Although the trial was not powered to assess physical activity effects, greater CDR-SB improvement in the most active oxiracetam subgroup (–0.28 vs −0.10, p = 0.0459) was observed. However, interaction testing was not significant (p = 0.76), and these exploratory findings warrant caution. Still, the feasibility and acceptability of long-term activity in stroke survivors were demonstrated, offering direction for future intervention trials.
Among rs-fMRI metrics, only the clustering coefficient – reflecting local segregation – differed between groups, favoring oxiracetam. This metric captures regional processing efficiency and has been linked to cognition.^24,31^ Despite standardized protocols and quality control, scan variability and participant factors may have limited detection of other network differences.
To minimize practice effects, MMSE and CDR-SB were assessed only at baseline and week 36. Prior research suggests that learning effects wane after the initial 3 months.^32^ The 9-month interval likely reduced this bias.
Several limitations should be noted. First, actigraphy data were missing in 13% due to device failure. Although largely technical, missingness may not be random – patients with cognitive decline may have had lower adherence, potentially biasing results.
Second, women comprised ~20% of the cohort, reflecting persistent sex imbalance in stroke trials.^33^ Reasons may include higher comorbidity, lower participation rates, or recruitment bias. While physical activity was standardized, its demands may have disproportionately deterred women. Future studies should adopt sex-sensitive designs to improve representativeness and equity in trial participation.
Third, MMSE has limited sensitivity for post-stroke cognitive deficits, particularly executive dysfunction, attention deficits, and delayed recall.^34^ Ceiling effects in our relatively high-functioning cohort likely blunted its responsiveness. While CDR-SB and domain-specific scores showed improvement, MMSE changes remained modest. Future studies should consider more sensitive, stroke-specific instruments.
Our eligibility criteria targeted individuals with subjective cognitive decline and additional risk factors for PSCI, including advanced age, recurrent stroke, diabetes, atrial fibrillation, and moderate-to-severe WMH. While this approach enriched the sample for those at higher risk of cognitive decline, it may have introduced selection bias toward individuals with more advanced neurodegenerative burden, potentially limiting the observable treatment effect. Furthermore, requiring self-reported cognitive concerns may have excluded individuals with impaired awareness or lower concern about their symptoms. Conversely, this criterion may have favored the inclusion of individuals with relatively preserved cognition and heightened health awareness – so-called “worried well” – who tend to have a more favorable prognosis. As a result, our cohort may not fully represent the broader spectrum of post-stroke cognitive trajectories, and caution is warranted in generalizing these findings.
In conclusion, this randomized trial did not support the efficacy of oxiracetam in preventing cognitive decline among high-risk post-stroke patients. In January 2023, the K-MFDS issued a drug safety communication recommending the suspension of oxiracetam prescriptions. These findings underscore a broader challenge faced by aging societies worldwide: the imperative to ensure that pharmaceutical use is both evidence-based and economically sustainable. Our results may inform similar drug reassessment initiatives in other countries, particularly in guiding the reevaluation of legacy medications and the development of cost-conscious, value-driven health policy frameworks.
Supplementary Material
sj-docx-1-eso_23969873251350141
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rost NS, Brodtmann A, Pase MP, et al. Post-stroke cognitive impairment and dementia. Circ Res 2022; 130: 1252–1271.35420911 10.1161/CIRCRESAHA.122.319951 · doi ↗ · pubmed ↗
- 2Colucci L, Bosco M, Rosario Ziello A, et al. Effectiveness of nootropic drugs with cholinergic activity in treatment of cognitive deficit: a review. J Exp Pharmacol 2012; 4: 163–172.27186129 10.2147/JEP.S 35326 PMC 4863555 · doi ↗ · pubmed ↗
- 3Park S, Kim S, Park E, et al. Research on rationalizing the reassessment of drug reimbursement appropriateness. Sejong: Korea Institute for Health and Social Affairs, https://repository.hira.or.kr/bitstream/2019.oak/3227/2/%EC%95%BD%EC%A 0%9C%20%EA%B 8%89%EC%97%AC%EC%A 0%81%EC%A 0%95%EC%84%B 1%20%EC%9E%AC%ED%8F%89%EA%B 0%80%20%ED%95%A 9%EB%A 6%AC%ED%99%94%20%EB%B 0%A 9%EC%95%88%20%EC%97%B 0%EA%B 5%AC.pdf (2023, accessed 3 May 2025).
- 4Spignoli G, Pedata F, Giovannelli L, et al. Effect of oxiracetam and piracetam on central cholinergic mechanisms and active-avoidance acquisition. Clin Neuropharmacol 1986; 9: S 39–S 47.3594455 · pubmed ↗
- 5Lim J-S, Kim N, Jang MU, et al. Cortical hubs and subcortical cholinergic pathways as neural substrates of poststroke dementia. Stroke 2014; 45: 1069–1076.24603067 10.1161/STROKEAHA.113.004156 · doi ↗ · pubmed ↗
- 6Rozzini R, Zanetti O, Bianchetti A. Effectiveness of oxiracetam therapy in the treatment of cognitive deficiencies secondary to primary degenerative dementia. Acta Neurol 1992; 14: 117–126.1414555 · pubmed ↗
- 7Villardita C, Grioli S, Lomeo C, et al. Clinical studies with oxiracetam in patients with dementia of Alzheimer type and multi-infarct dementia of mild to moderate degree. Neuropsychobiology 1992; 25: 24–28.1603291 10.1159/000118805 · doi ↗ · pubmed ↗
- 8Nardella C, Terracina L, Brunetti M, et al. Choline incorporation into phospholipids in brain areas from spontaneously hypertensive rats: effect of oxiracetam treatment. Farmaco Soc Chimica Italiana 1991; 46: 1051–1059.1807290 · pubmed ↗