Effectiveness of a behaviour change intervention on health literacy for behavioural risk factors of non-communicable diseases among health care assistants of government hospitals in Colombo District: a cluster-randomized controlled trial
Irshad Mashood, Dulani Samaranayake, Vindya Kumarapeli

TL;DR
A behavior change program improved health literacy and reduced risk factors for non-communicable diseases among healthcare assistants in Sri Lanka.
Contribution
A cluster-randomized trial demonstrated the effectiveness of a behavior change intervention in improving health literacy among healthcare assistants.
Findings
The intervention significantly improved health literacy scores and levels among healthcare assistants.
Positive behavior changes were observed in diet, physical activity, and tobacco avoidance.
Age under 35 was a positive predictor of health literacy improvement.
Abstract
Non-communicable diseases (NCDs) are a major public health challenge in Sri Lanka, driven by behavioural risk factors. Healthcare Assistants (HCAs) play a key role in NCD prevention, but limited health literacy (HL) reduces their effectiveness. Strengthening HL among HCAs can reduce their own NCD risk, enhance their role as health promoters, and improve patient education and hospital-based health initiatives. This study aimed to assess the effectiveness of a behaviour change intervention package (BCIP) to improve HL on behavioural risk factors of NCDs among HCAs in Colombo district. A cluster Randomized Controlled Trial (cRCT) was conducted with 240 HCAs from 20 hospitals in the Colombo district, 10 hospitals each for the control and intervention arms. The 16 sessions of the BCIP were conducted over eight weeks. The HL-NCD tool and STEPS questionnaire were administered two weeks…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
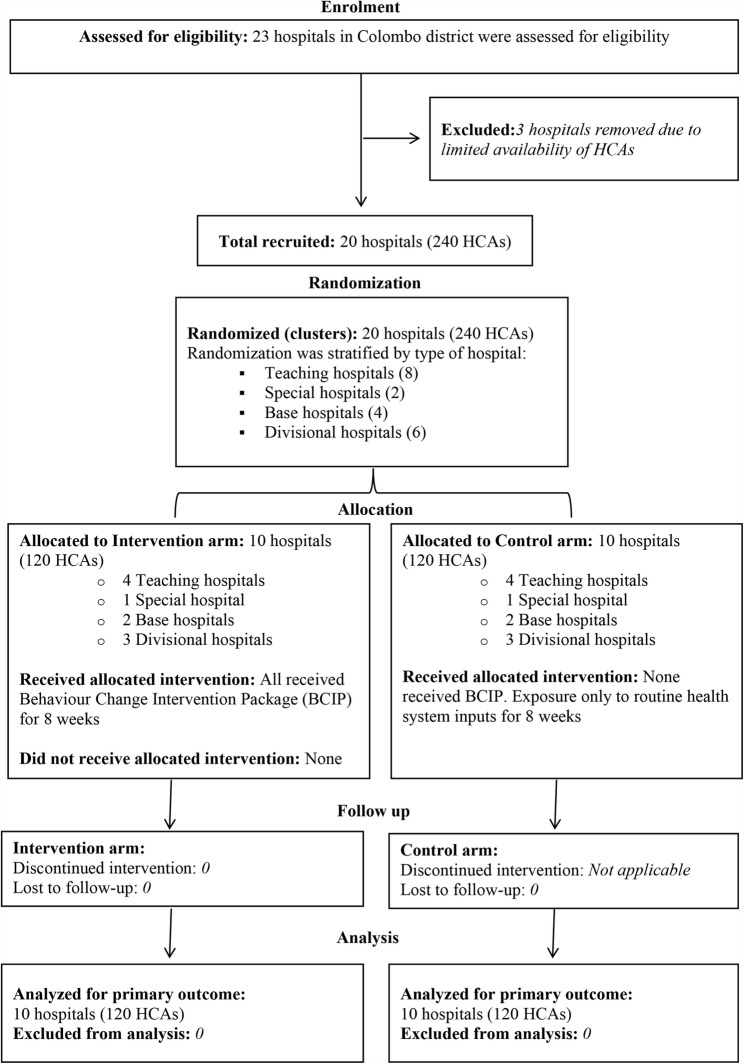 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth Literacy and Information Accessibility · Mobile Health and mHealth Applications · Behavioral Health and Interventions
Introduction
Non-communicable diseases (NCDs) are the leading cause of premature death worldwide, primarily driven by behavioural risk factors such as unhealthy diet, physical inactivity, tobacco use, and alcohol intake [1]. Limited health literacy (HL) exacerbates NCD risk and worsens outcomes, making HL-based interventions crucial for prevention [2]. In Sri Lanka, 91.4% of adults exhibit at least one behavioural risk factor, including poor diet, high salt intake, low physical activity, tobacco use, alcohol consumption, and exposure to secondhand smoke. Despite slightly better dietary habits, overall adherence to healthy behaviours remains poor, highlighting the need for targeted behaviour-focused interventions [3].
HL extends beyond the ability to read and write health information. It encompasses the capacity to access, understand, appraise, and apply health information to make informed decisions that influence lifestyle and health outcomes [4, 5]. Theoretical models such as Nutbeam’s framework conceptualize HL as a continuum of functional, communicative, and critical competencies [6], while the Calgary Charter on Health Literacy defines HL as a dynamic process linking knowledge to behavioural action [7]. According to the Charter, behaviour change occurs through sequential processes of finding, understanding, evaluating, communicating, and using health information to improve health decisions and practices.
Improvements in HL are therefore expected to influence specific behavioural outcomes through enhanced knowledge, motivation, self-efficacy, and the ability to navigate and act on health information [8]. HL-based interventions, unlike traditional information campaigns, emphasize empowerment and skill-building, thereby producing more sustained changes in diet, physical activity, tobacco use, and alcohol consumption [9]. Evidence from global HL initiatives such as the Canyon Ranch Institute Life Enhancement Program (CRI-LEP) and the WHO National Health Literacy Demonstration Projects (NHLDPs) demonstrates the effectiveness of this approach in reducing behavioural risk factors and promoting self-care [10, 11].
Within Sri Lanka, HL research has predominantly focused on groups such as pregnant mothers, schoolteachers, and environmental officers, mainly assessing knowledge and attitudes rather than behaviour change capacity [12–14]. However, Healthcare Assistants (HCAs) represent a critical but overlooked occupational group. They not only experience a high prevalence of NCD-related behavioural risks but also interact daily with patients, giving them the potential to serve as role models and change agents within hospital settings [15]. Strengthening HL among HCAs could therefore reduce their personal risk, enhance patient education, and support institutional health promotion initiatives [16].
To address this gap, a Behaviour Change Intervention Package (BCIP**)** was developed, guided by constructs from the Calgary Charter each intervention session designed to enhance participants’ ability to find standard health information on NCD risk factors, understand their practice, compare their practice with the standard, and apply standard health information to their practice. The present study evaluates the effectiveness of this BCIP in improving HL and promoting positive behavioural changes among HCAs in the Colombo District, thereby contributing to both local and global evidence on HL-based interventions for NCD prevention.
Methodology
Study design
Cluster randomized controlled trial.
Study setting
This study was conducted in 20 hospitals in Colombo district.
Study population
HCAs working in government hospitals in Colombo district.
Inclusion criteria: Permanent staff who have been working as HCA more than six months and age of HCA in between 18 years to 55 years were included.
Exclusion criteria: Staff who plan to retire or transfer within a year, HCAs who were on long leave e.g.: maternity leave or medical leave, HCAs who were detected as having NCD or facing complications like CKD and HCAs in PMCUs of Colombo district were excluded.
Study period
Study period was from June 2023 to June 2024.
Sample size
A cluster was defined as 12 HCAs selected from each hospital. The required number of clusters for this cluster-randomized controlled trial was calculated using the standard formula for comparing means, incorporating the design effect to account for intra-cluster correlation.
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\begin{array}{c}C=1+\left(Z_{\alpha/2}\right)^2\left(\sigma_{0^2}+\sigma_{1^2}\right)\times\\\;\left[1+\left(m-1\right)\rho\right]/\mathrm m\left(\mu_0-\mu_1\right)^2\end{array}$$\end{document}Sample size was based on effect sizes from a previous Iranian study where an intervention markedly increased S-TOFHLA scores in diabetic patients. A cluster size of 12 and ICC of 0.04 were used based on a CRT on health communication for diabetic patients.
C = Number of clusters.
Z_α/2_ = The standard normal deviate for α, 0.05 = 1.96.
Z_β_ = The standard normal deviate for β, 0.2 = 0.84.
m = Size of the cluster = 12.
µ_0_ = True mean of outcome variable in the intervention group = 132.14.
µ_1_ = True mean of outcome variable in the control group = 94.33.
σ_0_ = Standard deviation of outcome variable in the intervention group = 13.81.
σ_1_ = Standard deviation of outcome variable in the control group = 12.64.
ρ = Intraclass correlation coefficient (ICC) = 0.04.
\documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\begin{aligned} \mathrm C&=1+\left(1.96+0.84\right)^2\left(13.812+12.642\right)\;\times\;\\&\left[1+\left(12.1\right)0.04\right]\;/\;12\left(132.14-94.33\right)^2\end{aligned}$$\end{document}
C = 9.7 Number of clusters per arm was taken as 10.
Substituting these values yielded approximately 9.7 clusters per arm; therefore, 10 clusters (hospitals) were included in each arm, giving a total of 20 clusters and 240 participants. No attrition occurred during the study, as all recruited participants completed both baseline and post-intervention assessments.
Sampling technique
Stratified cluster sampling method was applied according to the type of hospitals in Colombo district.
Stratification - Types of hospitals in Colombo district are Teaching hospitals, Special hospitals, Base hospitals and Divisional hospitals and these served as strata for the sampling. Number of clusters to be selected from each stratum was calculated proportionate to the number of HCAs in each of them. Each hospital was taken as cluster and there were twenty clusters (6 teaching hospitals, 4 special hospitals, 4 base hospitals, 6 divisional hospitals).
Recruitment of HCAs - Required number of HCAs was selected randomly from the pay roll of all HCAs attached to the hospital. It was selected in three steps within the hospital.
- Step I: All HCAs were listed out based on pay roll.
- Step II: Eligible HCAs were selected based on inclusion and exclusion criteria.
- Step III: Required number of HCAs were selected using simple random sampling (random table).
Study instruments
- I)HL-NCD Questionnaire - The primary outcome was the improvement in HL on behavioural risk factors of NCDs. The Health Literacy on Behavioural Risk Factors of NCDs (HL-NCD) tool (Supplementary File 01), developed and validated for HCAs in Sri Lanka, was used for assessment. It comprised 56 items under four factors: Finding Standard Information, Understanding Self-Practice, Comparing, and Applying explaining 92.49% of the variance. The tool showed excellent construct validity (CFI = 0.99, RMSEA = 0.0072, SRMR = 0.03) and strong reliability (Cronbach’s α = 0.901; ICC = 0.836), with significant correlations to key behavioural practices (ρ = 0.43–0.58).
- Section A – Included a set of questions to assess basic characteristics such as socio-demographic characteristics, work-related characteristics, language proficiency, source of obtaining information and level of health knowledge of the participants.
- Section B – Proper HL-NCD tool to assess HL of the participants related to behavioural risk factors of NCDs.
- II)STEPS Questionnaire: Secondary outcomes were behaviour change related to pattern of Diet, frequency of physical activity, status/frequency of tobacco use and alcohol intake. These were assessed using the WHO STEPS questionnaire. The Sri Lankan version, previously validated and used in national surveys (2003–2021) to assess behavioural NCD risk factors, was employed. Relevant behavioural components CORE T (Tobacco use), CORE A (Alcohol intake), CORE D (Diet), and CORE P (Physical activity) were included.
Data collection
Data collection was conducted by principal investigator (PI) and research assistants (RAs) who were trained on administering the questionnaire. The selected HCAs were met by the RAs in person as appointment and they were explained the purpose of the study and informed written consent was obtained. Then the questionnaires were administered to the participants at two time points: baseline assessment and post-assessment. Data collectors were blinded to the group allocation of participants only at baseline assessment.
Study implementation
- I)Baseline Assessment - Baseline assessment was conducted two weeks before the implementation of the BCIP. Participants and data collectors were not informed regarding the allocation of intervention and control arm at baseline. Data collection was conducted using tools: HL-NCD and selected components of STEPS questionnaire.
- II)Randomization - Randomization by cluster was implemented in two steps to ensure no allocation bias. First, twenty Hospitals selected using the stratified cluster sampling method were randomized into two groups (ten hospitals each) using stratified randomization. Eligibility criteria were considered that may account for potential variations within the clusters that could influence the outcome. Then, the two groups were allocated as the intervention and the control ensuring that each group was comparable at baseline. Hospitals were located in different geographic areas, and only one cluster was selected from each hospital to minimize contamination between study arms. This approach minimized potential biases and ensured a fair distribution of hospitals, enhancing the reliability and internal validity of the study.The two steps in randomization were,Step I: Twenty hospitals selected through a stratified cluster sampling method were randomized into two groups based on hospital type (Teaching, Special, Base, and Divisional hospitals). Within each stratum, hospitals were randomly allocated to intervention and control arms using the lottery method.Step II: Allocation of hospitals to intervention and the control arms was selected by an independent person (Consultant Community Physician attached to MoH), who was not involved in the selection of participants or any other activity of the research study thereby ensuring allocation concealment.
- III)Implementation of the intervention - Intervention was conducted without interruption of HCAs’ work in a suitable date, time and place with an appropriate environment after discussing with support from medical and public health staff. Dates and venues were communicated via group-appointed leaders and WhatsApp. The PI assisted by trained RAs, delivered 16 two-hour sessions (Supplementary File 02) over 8 weeks using a facilitator guide, handbook, and PowerPoint, incorporating presentations, interactive discussions, and group activities. A WhatsApp group was used to share educational materials and experiences. Attendance was recorded, dropouts documented, and delivery monitored with process evaluation indicators. To minimize contamination, no personnel, activities, or training materials were shared between clusters during the intervention period. The control group received only routine health services during the study, but was given the BCIP after the post-test with the same interactive format.
- IV)Post-assessment - Post-assessment of the level of HL and secondary outcomes among intervention and control arms after two weeks of completion of BCIP. Data collection was conducted using the same tools in both arms through IAQ. Feedback form was also given to the participants in the intervention group.
Data analysis
The intervention effectiveness was evaluated using primary and secondary outcome indicators, with data entered, cleaned, and analyzed in SPSS version 23.
Participant characteristics including socio-demographics, work-related factors, information sources, language proficiency, and health knowledge were analyzed first. Health knowledge scores ≥ 7/10 were classified as satisfactory, and < 7 as limited based on expert consensus. Categorical variables were compared using Chi-squared or Fisher’s exact tests (independent groups) and McNemar’s test (paired groups).
The primary outcome, HL score and level, was measured using the validated HL-NCD tool. This tool had 56 items on a 4-point Likert scale, giving a total score between 56 and 224. Scores were converted to a percentage, and scores above 50% were considered satisfactory HL. Analysis included within-group comparisons using paired sample t-test and between-group comparisons using independent sample t-test at baseline and after the intervention for HL score. Analysis included within-group comparisons using McNemar’s test and between-group comparisons using the Pearson Chi-squared test at baseline and after the intervention for HL level.
Secondary outcomes were analyzed similarly, with Chi-squared/Fisher’s exact tests for categorical variables and paired/independent t-tests for continuous variables. Behavioural risk factors were assessed using the Sri Lanka STEPS Survey criteria, where the presence of risk behaviour was defined as tobacco or alcohol use within 30 days, less number of varieties of fruit/vegetable intake, adding salt to food, or < 150 min of physical activity per week.
Both unadjusted and cluster-level analyses were conducted to compare baseline and post-intervention outcomes between study arms. To account for intra-cluster correlation, adjusted analyses using Generalized Estimating Equations (GEE) were performed. GEE was selected over mixed-effects modeling as it provides robust population-averaged estimates aligned with the study’s aim of evaluating overall intervention effectiveness without assumptions on random-effect distributions.
Consort Flow diagram of the study is given in Fig. 1.Fig. 1CONSORT flow diagram of the study
Ethical considerations
Approval for the study was obtained from the Board of Study, Community Medicine from the Postgraduate Institute of Medicine, Colombo. Permission from DDG MS II, PDHS of Western province, and RDHS Colombo were obtained. Written permission was obtained from the Directors of each selected hospital. Ethical clearance was obtained from the Ethics Review Committee of the Faculty of Medicine, University of Colombo with the clinical trial registration. (SLCTR/2023/023, https://slctr.lk/trials/slctr-2023-023, 11th December 2023, Sri Lanka Clinical Trial Registry). Informed written consent was obtained from all HCAs, and strict measures for privacy, confidentiality, and data safety were implemented.
Results
The CONSORT flow diagram detailing participant enrollment, intervention allocation, follow-up, and inclusion in the analysis is given in Fig. 1.
Baseline characteristics of the intervention and control groups are summarized in Table 1. The intervention and control groups were comparable across most socio-demographic and work-related characteristics, with no significant baseline differences except for participation in special health-related training (p < 0.001), use of radio (p = 0.049) and mass media (p = 0.043) for health information, and English proficiency (p = 0.005). All participants were proficient in Sinhala, and no difference was found in Tamil proficiency. The GEE models adjusted for baseline covariates and accounted for clustering to estimate intervention effects.
Table 1. Comparison of sociodemographic and other basic characteristics of HCAs in the intervention and control groupsCharacteristicsIntervention Group (n = 120)Control Group(n = 120)Sig.No.(%)No.(%)Age in yearsχ2 = 3.774^^df = 1p* = 0.052 18–354537.53125.8 36–557562.58974.2Sexχ2 = 0.153df = 1p = 0.696 Male5041.35344.2 Female7058.36755.8Ethnicity ^a^ Sinhala11898.311999.2χ2 = 0.338^^df = 1p* = 1.000 Tamil21.700.0 Muslim00.010.8 Malay00.000.0Religion ^a^χ2 = 0.684^^df = 1p* = 0.684 Buddhism11696.711898.3 Hinduism10.800.0 Christianity21.700.0 Roman catholic10.810.8 Islam00.010.8Educationχ2 = 0.826^^df = 1p* = 0.363 Up to grade 0932.5108.3 Up to GCE O/L6050.06050.0 Up to GCE A/L5243.34638.3 Above GCE A/L21.743.3 Diploma/Degree32.500.0Service yearsχ2 = 0.270df = 1p = 0.603 Less than 10 years6957.56554.2 More than 10 years5142.55545.8Participated in special training related to healthχ2 = 14.423df = 1p = 0.000 Yes2621.765.0 No9478.311495.0Level of Health Knowledgeχ2 = 1.571df = 1p = 0.210 Limited7865.08772.5 Satisfactory4235.03327.5Language Proficiency Sinhala120100120100Constant English3529.21714.2χ^2^ = 7.954df = 1p = 0.005 Tamil ^a^32.521.7χ^2^ = 0.204df = 1p = 1.000*Chi-squared test was considered when rows were amalgamated^a^Fisher’s exact test was performed since more than 20% of the cells have the expected value < 5
The BCIP produced a significant improvement in HL among HCAs. The median HL score increased from 42.4 to 52.2 in the intervention group (p < 0.001, r = 0.8), while the control group showed no change (Table 2). The GEE analysis indicated that intervention participants scored 7.8 points higher than controls (95% CI: 7.38–8.22, p < 0.001). The proportion achieving satisfactory HL increased significantly (p = 0.003) (Table 3), and intervention participants were 3.8 times more likely to reach satisfactory HL than controls (OR = 3.8, 95% CI: 1.59–9.11, p = 0.003).
Table 2. Comparison of HL score of HCAs in the intervention and control groupsPoint in TimeIntervention group (n = 120)Control group (n = 120)Sig*(Betweengroup)Effect sizer=(z/√N)MeanSDMedianIQRMeanSDMedianIQRPre- test42.44.742.44.942.73.942.93.6Z=−1.577p = 0.115r = 0.1Post- test50.43.852.24.442.74.142.94.5Z=−10.48p < 0.001r = 0.6Sig*(Within group)Z=−9.319p < 0.001Z=−0.014p = 0.989Effect sizer=(z/√N)r = 0.8r = 0.0
Table 3. Between group comparison of HL level of HCAs in the intervention and control groupsLevel of HLPre-testSig.Post-testSig.Intervention groupNo. (%)Control groupNo. (%)Intervention groupNo. (%)Control groupNo. (%)Limited108 (90.0)114 (95.0)Χ^2^ = 2.162df = 1p = 0.14192 (6.7)111 (92.5)χ^2^ = 11.535df = 1p = 0.001Satisfactory12 (10.0)6 (5.0)28 (93.3)9 (7.5)
Significant improvements were also observed in behavioural outcomes. Table 4 summarizes the GEE analysis results. The intervention group showed higher odds of limiting sugar (OR = 12.35, p < 0.001) and salt (OR = 9.42, p < 0.001) intake, and increasing fruit (OR = 9.15, p = 0.026) and vegetable (OR = 5.05, p < 0.001) consumption. Adequate physical activity rose from 18.3% to 33.3% (OR = 5.83, p < 0.001), and active transport use increased (OR = 5.44, p < 0.001). Smokeless tobacco use (OR = 2.70, p = 0.022) and exposure to secondhand smoke (OR = 46.72, p < 0.001) significantly decreased, while no significant reduction was found in smoking or alcohol use.
Table 4. Adjusted analysis for clustering and confounding Variables, using generalized estimating equation with individual data for the effect of the interventionOutcomeOR95% CIp valueHL Score7.8017.378–8.224< 0.001HL level3.8001.585–9.1130.003Consuming Less than the Recommended Daily amount of Sugar12.3464.270–35.701< 0.001Consuming Less than the Recommended Daily amount of Salt9.4234.538–19.569< 0.001Consuming the Recommended Number of Fruits per Day9.1541.295–64.7170.026Consuming the Recommended Number of Vegetables per Day5.0532.466–10.354< 0.001Engaging in the Recommended Level of Physical Activity5.8273.222–10.537< 0.001Using Active Mode of Transport5.4392.336–12.663< 0.001Not Using Smokeless Tobacco2.7041.152–6.3500.022Currently Non-Smoking1.6540.611–4.4780.322Non-exposure to Secondhand smoking46.7188.091–269.745< 0.001Currently Not Taking Alcohol1.8890.401–8.8980.421Model: (Threshold), Arm, Age, Sex, Education, Service years, Monthly income, Membership in Health club or Welfare Group, Special Course in Health, Awareness program related to health, Health information from Radio, Health information from mass media, Health information from the internet, Proficiency in English
Discussion
The BCIP demonstrated robust short-term effectiveness in enhancing both HL scores and HL levels among HCAs, as evidenced by unadjusted, cluster-level, and GEE analyses. The intervention group achieved a large effect size (r > 0.8), with median HL scores increasing from 42.4 to 52.2 (p = 0.005) and GEE analysis indicating a 7.8-point advantage over controls (OR = 7.801, 95% CI 7.378–8.224, p < 0.000). These findings indicate that a structured, theory-driven HL intervention can produce meaningful short-term improvements in HL within an occupational group with important public health responsibilities.
Age < 35 years and higher education were significant positive predictors of HL, consistent with the NAAL survey in the USA and German findings of greater HL and willingness to improve HL among younger adults [17–19], while education only up to O/Ls predicted poorer HL (OR = 0.465, p = 0.029),aligning with evidence that identifies low HL as a mediator between lower education and adverse health outcomes [18, 20].
The strong intervention effects are likely attributable to BCIP’s grounding in the Calgary Charter and its emphasis on practical skill-building features that consistently identified in systematic reviews as critical to intervention success [21, 22]. Although the HL-NCD tool assesses four distinct HL domains - finding standard information, understanding self practice, comparing, and applying; domain-specific analyses were not conducted in this study. This was primarily due to the study’s focus on overall HL improvement and sample size considerations that limited statistical power for robust domain-level comparisons. This limits understanding of which HL components contributed most to behaviour improvement. Future studies with larger samples should incorporate domain-specific analyses to better elucidate the pathways through which HL improvements translate into behavioural change.
With regard to behavioural outcomes, the BCIP was associated with significant improvements in diet-related practices, including increased adherence to recommended sugar and salt limits and improved fruit and vegetable intake. These findings are consistent with prior evidence demonstrating that group-based, theory-driven HL interventions can effectively influence dietary behaviours [9, 19, 22]. Physical activity levels also improved substantially following the intervention, supporting evidence from systematic reviews indicating that education- and counselling-based interventions, as well as multi-component workplace programs, can promote physical activity [23–25]. A two-week follow-up period was used to minimize recall bias, consistent with previous behaviour change interventions assessing diet and physical activity [22]. While improvements observed at follow-up indicate immediate post-intervention effects, the sustainability of dietary and physical activity behaviour changes cannot be determined due to the limited follow-up duration. Future research should incorporate extended follow-up periods of 6–12 months to adequately assess the sustainability and long-term impact of the intervention.
For addictive behaviours, the BCIP resulted in significant reduction in smokeless tobacco use (OR = 2.704, p = 0.022) and secondhand smoke exposure (OR = 46.718, p < 0.000), aligning with prior evidence supporting behavioural interventions for smokeless tobacco cessation [26–28]. In contrast, no significant reductions were observed in smoking tobacco and alcohol use, likely due to the socially reinforced and habitual nature of these behaviours, which require longer-term, individualized, multi-modal approaches and sustained support [28, 29]. This differential responsiveness highlights an important implication for intervention design: while HL-focused, group-based programs may be effective for modifying diet and physical activity, more intensive or specialised strategies such as sustained counselling, brief interventions, pharmacological support, or structured cessation services are likely necessary to address addictive behaviours, even among motivated occupational groups.
Although randomization was stratified by hospital type and analyses adjusted for baseline covariates using GEE models, several baseline imbalances were observed between intervention and control groups. Participants in the intervention group had greater prior exposure to special health-related training, higher use of radio and mass media for health information, and better English proficiency. These factors may have facilitated improved access to information and greater receptivity to HL-related content, potentially contributing to the magnitude of HL improvement observed. While statistical adjustment was applied to mitigate these effects, residual confounding cannot be entirely excluded and should be considered when interpreting the findings.
The reliance on self-reported HL and behavioural data represents another limitation. Although validated Sri Lankan STEPS Survey components were used, self-reported measures are susceptible to social desirability and recall biases, which may have led to an overestimation of positive behavioural changes, particularly for diet and physical activity. Future research should incorporate objective outcome measures, such as biochemical validation for tobacco or alcohol use and device-based monitoring of physical activity, to strengthen the validity of behavioural assessments.
Despite these limitations, the BCIP among a relatively homogenous group of HCAs indicates strong potential for scalability and adaptation to other workplace and community settings. Its modular design and combination of face-to-face and m-Health components enhance feasibility in resource-limited contexts, while its group-based format supports cost-effectiveness through peer learning. Although only one cluster was selected from each hospital and the BCIP content was withheld from the control group until the end of the intervention to minimize contamination, the possibility of limited information exchange between participants cannot be entirely excluded.
Overall, these findings reinforce evidence from low- and middle-income country settings that HL interventions can produce substantial short-term improvements in diet, physical activity, tobacco use, and self-care behaviours [30]. By integrating a theory-driven framework, comprehensive HL measurement, and skill-based learning, the BCIP offers a novel, scalable, and potentially cost-effective model for addressing NCD risk factors through HL enhancement. Future studies incorporating domain-specific HL analyses, objective outcome measures, and longer follow-up periods of 6–12 months are needed to clarify mechanisms of action and assess long-term sustainability.
Conclusions
The BCIP demonstrated short-term effectiveness in enhancing both HL scores and HL levels among HCAs in Colombo district hospitals. The intervention led to significant improvements in self-reported dietary practices including reduced sugar and salt consumption and increased fruit and vegetable intake as well as notable gains in physical activity and active transport. Reductions in smokeless tobacco use and exposure to secondhand smoke were also observed; however, no significant changes were identified for smoked tobacco or alcohol intake during the study period. These heterogeneous outcomes highlight that while the BCIP effectively promoted healthier lifestyle practices, certain entrenched behaviours may require longer-term or more intensive strategies.
Grounded in the four domains of HL, the BCIP demonstrates the potential of HL-based approaches to strengthen individual capacity for informed health decisions and self-management. Integrating such HL-focused programs into routine staff training or national NCD control initiatives could enhance their reach and sustainability. Overall, the BCIP contributed to improved self-reported behavioural practices and strengthened HL among healthcare workers, offering a promising and scalable approach to support NCD prevention in similar resource-limited contexts.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Health literacy in the Nordic countries—Not only a determinant of health, but also a tool for health promotion. Nordic Welfare Centre. Published 1988. Accessed October 29, 2024. https://nordicwelfare.org/pub/Health_Literacy/health-literacy-concept-and-definition.html.
- 2Bakker MM, Putrik P, Aaby A et al. Acting together—WHO National Health Literacy Demonstration Projects (NHLD Ps) address health literacy needs in the European Region. Public Health Panorama. 2019;5(2):233–243. Accessed August 18, 2025. https://cris.maastrichtuniversity.nl/en/publications/acting-together-who-national-health-literacy-demonstration-project.
- 3Kutner M, Greenberg E, Jin Y, Paulsen C. The health literacy of America’s adults: results from the 2003 National Assessment of Adult Literacy. Washington, DC: U.S. Department of Education, National Center for Education Statistics; 2006. Accessed August 18, 2025. http://www.edpubs.org.