Surgical removal of unexpected oral squamous cell carcinoma arising from a maxillary odontogenic keratocyst in a young female patient: a case report and literature review
Tasneem A. Amer, Mai M. Saleh, Mohammed S. Alalfy

TL;DR
A rare case of squamous cell carcinoma arising from a maxillary odontogenic keratocyst in a young girl is reported, highlighting the need for careful histopathological evaluation of such lesions.
Contribution
This case report presents a rare instance of SCC in a pediatric patient arising from an odontogenic keratocyst.
Findings
SCC arising from an odontogenic keratocyst is rare and aggressive, especially in young patients.
Histopathological evaluation is crucial for diagnosing malignant transformations in seemingly benign cystic lesions.
The patient underwent subtotal maxillectomy and postoperative obturator placement for functional and aesthetic restoration.
Abstract
Although odontogenic cysts in the maxilla are often seen, malignant changes inside these cysts are rather uncommon. According to reports, the occurrence of carcinomas developing in odontogenic cysts ranges from 1 to 2 per 1,000. Squamous cell carcinoma (SCC) arising from an odontogenic keratocyst (OKC) is a rare malignant transformation that typically presents in the jaws. This form of carcinoma is locally aggressive and often associated with a poor prognosis, especially when the diagnosis is delayed. This report discusses a healthy 13-year-old girl with no medical, dental, or surgical background who visited the Oral and Maxillofacial Surgery Department due to mild, dull discomfort and gradually increasing swelling in the right maxilla, originating from the palatal side for the past six months. The surgical procedure was conducted under general anesthesia during which a biopsy was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 10
Figure 10 Figure 1
Figure 1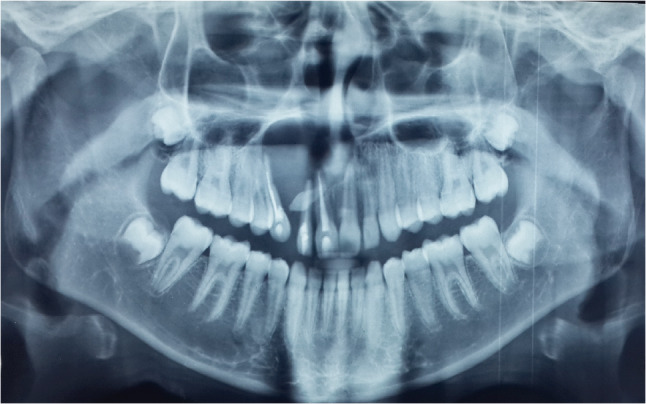 Figure 2
Figure 2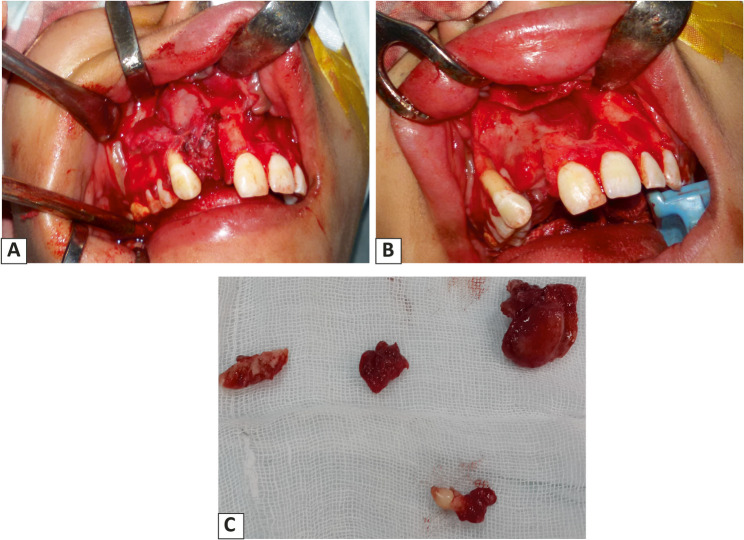 Figure 3
Figure 3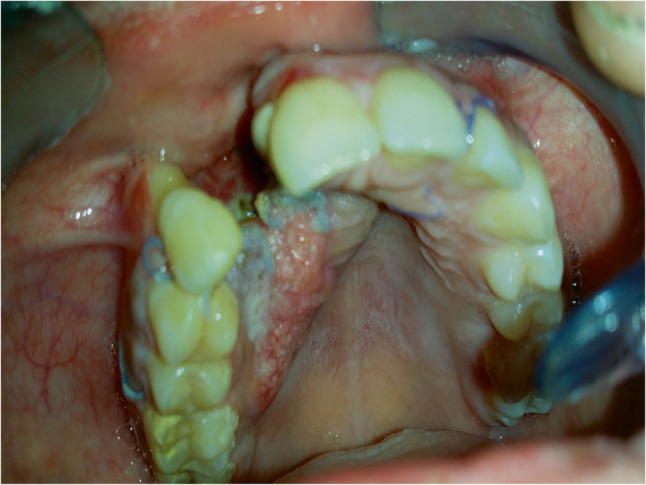 Figure 4
Figure 4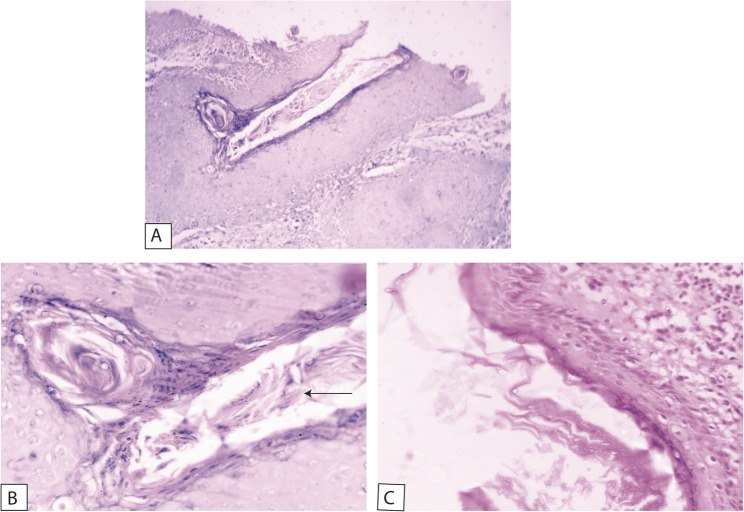 Figure 5
Figure 5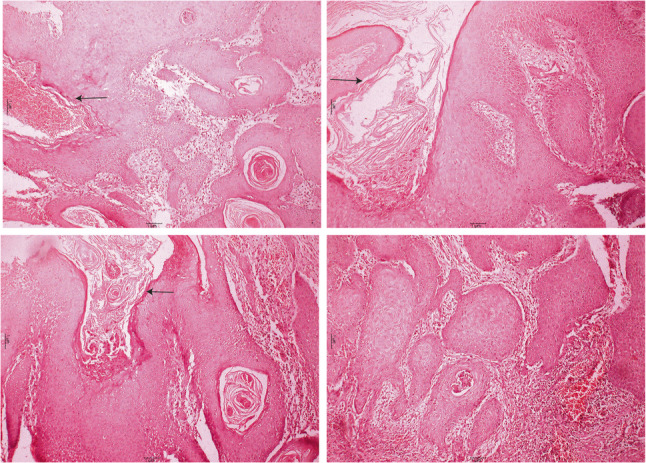 Figure 6
Figure 6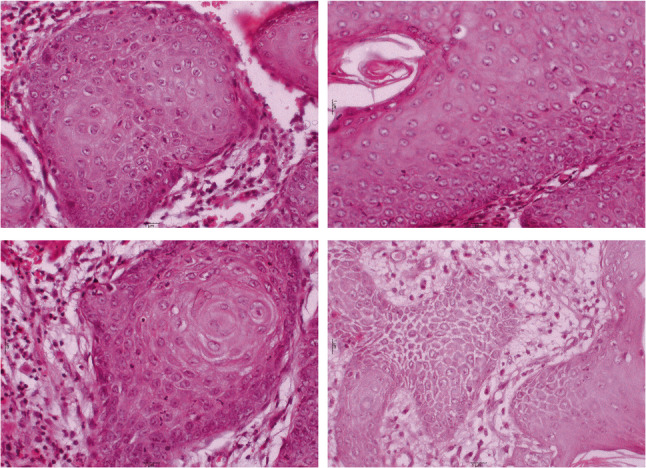 Figure 7
Figure 7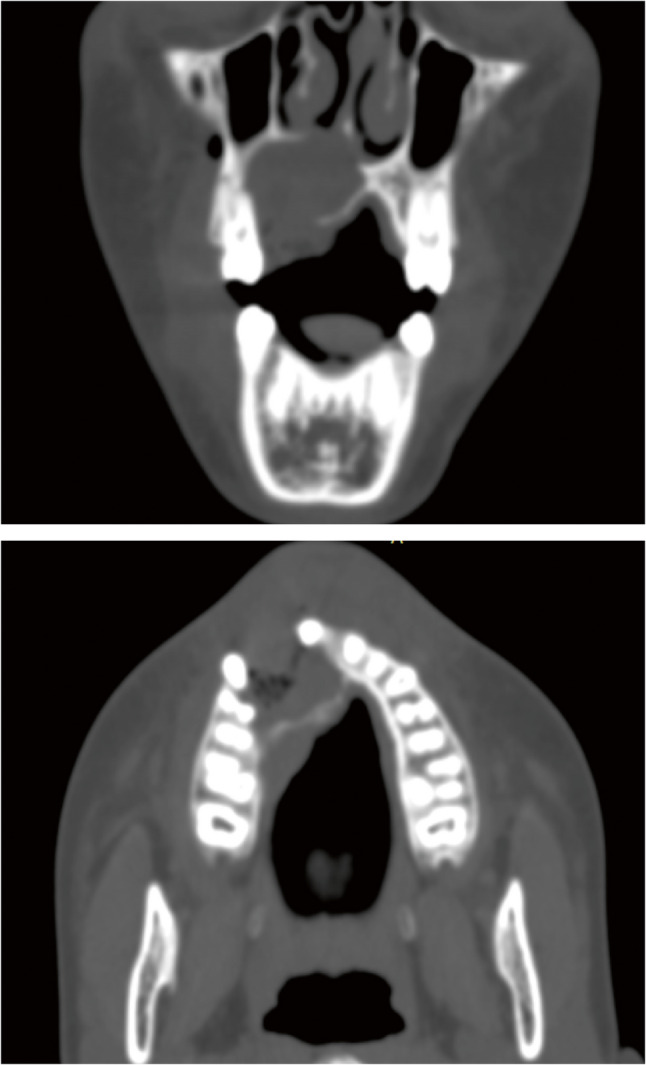 Figure 8
Figure 8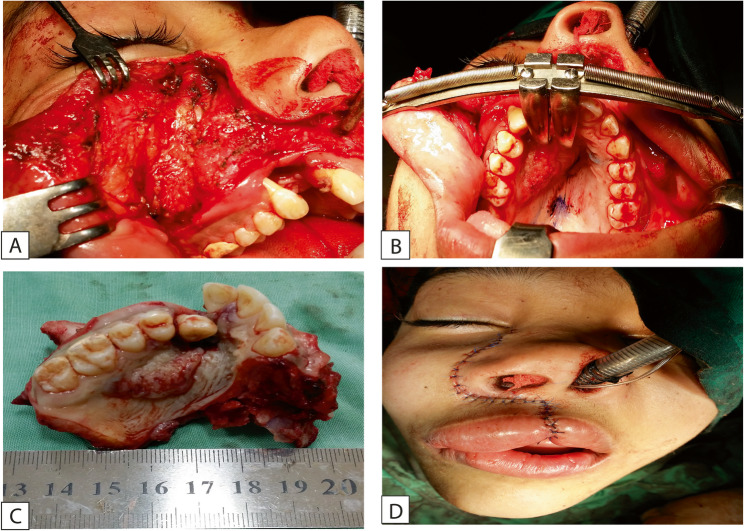 Figure 9
Figure 9- —Alexandria University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral and Maxillofacial Pathology · Sinusitis and nasal conditions · Head and Neck Surgical Oncology
Background
It is quite uncommon for cancer to develop in the bone. “A squamous cell carcinoma (SCC) that occurs in the jaws without any first communication to the oral mucous membrane.” is the definition of a primary intraosseous squamous cell carcinoma (PIOSCC) [1].
The World Health Organisation (WHO) proposed the name primary intraosseous carcinoma (PIOC) in 1972 and categorised this lesion as an odontogenic carcinoma since the epithelium involved in odontogenesis is the source of this lesion [2]. It is possible for PIOC to develop de novo from suspected odontogenic cell remains (such as reduced enamel epithelium) or from the lining of an odontogenic cyst [3].
The lining epithelium of odontogenic cysts may experience cystic expansion, keratinization, or undergo dysplasia. The more frequently occurring tumors that develop from the lining of odontogenic cysts include benign odontogenic tumors such as odontoma, Pindborg tumor, and adenomatoid odontogenic tumor [4]. However, it is well-established that the lining epithelium of an odontogenic cyst has the potential to change into a SCC or a mucoepidermoid carcinoma [3].
The clinical and radiographic characteristics of these two entities are often comparable to those of benign, expansive, central odontogenic tumors or jaw cysts. Paraesthesia rarely occurs. Radiographically, they resemble the cystic lesions from which they originated [5].
Carcinomatous transformation exists in less than 1% of the odontogenic cysts. Approximately 80% of SCCs are identified after the age of forty, with a 2:1 male to female proportion. Most of the lesions are moderate to well-differentiated carcinomas, and metastasis from those lesions has not occurred very often [6].
In 1913, Loos first described PIOSCC as a central epidermoid carcinoma of the jaw [7]. It was changed to an interalveolar epidermoid carcinoma by Wills in 1948 [8]. In 1969, Shear called it primary intra-alveolar epidermoid carcinoma [9]. The lesion was classified as an odontogenic carcinoma by the WHO and Pindborg in 1972, when they accepted the name PIOSCC [10]. Elzay, after that, changed the WHO classification for the jaw’s PIOC [11]. In 1948, Slootweg and Müller made minor modifications to Elazy’s classification by taking into account several potential etiological factors [12]. Intraosseous mucoepidermoid carcinoma was added as a fourth entity of PIOCs by Waldron and Mustoe to complete the classification [13]. Ultimately, PIOSCCs were reclassified as: first, a solid tumor that leads to bone resorption, second, SCC developing from an OKC lining or carcinoma developing in other odontogenic cysts, and third, SCC associated with benign epithelial odontogenic tumors in the (2022 )WHO classification, which replaced the previous terms [14].
Primary intraosseous carcinomas arising from the wall of an OKC are a rare tumor occurring within the jaw bones. A study by Bodner et al. in 2011 conducted a retrospective study of 116 cases of PIOC between 1938 and 2010. The result of this work showed that there have been only sixteen cases of PIOC developing from keratocyst, accounting for 14% of all the odontogenic cysts [15].
An impacted tooth is more than just a dormant thing. It is a major pathological risk factor that can lead to jaw changes that are both transformational and frequently destructive. These alterations include severe, bone-destroying cysts, the loss of nearby normal teeth, and common infections like pericoronitis and even oral and maxillofacial cysts or tumors. It has been found that cystic or neoplastic lesions arise in proximity to the impacted tooth in 16% of cases, most commonly during the second and third decades of life [16]. To avoid these issues, early detection and treatment of impacted teeth depend on routine dental monitoring along with radiographic examination [17].
The occurrence of carcinomatous transformation in odontogenic cysts has been documented to range from 0.13% to 3% [18]. There is an ongoing debate regarding which type of odontogenic cyst carries the highest risk of malignant transformation. Follicular (non-inflammatory) cysts have been reported as the most common etiology by Yasuoko [19] and Borras-Ferreres [18] whereas, Jain [20] and Bodner [15] have identified radicular (inflammatory) cysts as the most frequently undergoing transformation.
The mechanisms underlying the malignant transformation of odontogenic cysts remain largely unclear. Nevertheless, it is believed that carcinogenesis induced by chronic inflammation from persistent lesions may represent one possible pathway. Chronic inflammation has the potential to damage DNA, proteins, and gene expression, which can consequently result in genetic mutations that increase the risk of malignant transformation. Thus, it has been proposed that the likelihood of malignant conversion of the epithelial lining in an odontogenic cyst is significantly reduced in the absence of inflammation. Moreover, odontogenic cysts that exhibit keratinization are at a higher risk for malignant alterations compared to their nonkeratinizing counterparts. Reports indicate that the malignant transformation of the lining of odontogenic keratocysts constitutes 14% of all malignant transformations associated with odontogenic cysts [15].
The management of OKC varies significantly. It encompasses conservative surgical procedures such as marsupialization, decompression, and irrigation, which are often paired with distant definitive treatment. The definitive management of primary OKC involves enucleation and curettage and may also incorporate cryotherapy or chemoablation. Reports indicate that conservative treatments, commonly utilized for larger lesions, may carry an increased risk of malignant transformation of the cyst lining during the interval from diagnosis to definitive excision [21].
There are a few documented cases of malignant transformation arising from OKCs. Peng ye et al. investigated the clinicopathologic features of PIOSCC arising from an OKC (PIOSCC ex OKC) at Peking University School and Hospital of Stomatology. They also conducted a systematic review of studies on PIOSCC ex OKC by using online databases from their inception until February 2020. They found that all lesions were located in the mandible, which is consistent with the predilection site of OKCs [22]. In contrast, some studies showed the occurrence of SCC in maxillary odontogenic keratocysts [23, 24].
Phase I of treatment for most of these cases was either enucleation or incisional biopsy. Following an unanticipated discovery of carcinoma, additional treatment consisted of radical resection in the majority of cases, neck dissection and radiation, or chemotherapy in 1/3 of cases [25].
Case presentation
In this case report, we present a case of an OKC that was found to have undergone malignant transformation into SCC. A 13-year-old female patient without relevant medical history complains of a mild, dull pain and slowly growing swelling in the right maxilla from the palatal aspect for six months.
A few months prior to examination, the patient noticed a gradually increasing swelling on the palatal aspect of the right maxilla, despite otherwise appearing clinically normal. Intraoral examination revealed a localized swelling extending from the upper right central incisor to the upper right second premolar. The buccal mucosa appeared normal, except in the region of the right lateral incisor, where mucosal erosion was noted (Fig. 1). The palatal mucosa showed secondary inflammation, with evidence of palatal bone perforation upon palpation. Only the upper lateral incisor was mobile, while the other teeth were not sensitive to percussion or mobile. There were no reports or observations of paraesthesia, anaesthesia, nasal obstruction, or visual disturbance. Cervical lymphadenopathy was absent.
Fig. 1. Patient presented with a localized swelling in the right maxilla
Panoramic radiograph revealed a well-defined unilocular radiolucency related to a supernumerary tooth, extending from the upper left central incisor to the upper right canine, with displacement of the canine root and no evidence of additional pathology (Fig. 2).
Fig. 2. Panoramic x-ray showing a well-defined radiolucency with related supernumerary tooth, extended from the upper left central incisor to the upper right canine
Based on the patient’s history, clinical findings, and radiographic features—particularly the association with an impacted tooth—the lesion was initially strongly suspected to be a dentigerous cyst.
The surgical procedure was performed under general anaesthesia. A full-thickness muco-periosteal flap was performed using blade no. 15, extending one tooth anterior and one tooth posterior to the cystic cavity, then the muco-periosteal flap was reflected using a periosteal elevator to expose the bone. The overlying thin shell of bone was removed to expose the cystic lesion, which was enucleated with the involved tooth; the lateral incisor was also extracted, and apicectomy was performed on the central incisor (Fig. 3). The surgical wound was closed using suture 3 − 0. Then the excised lesion was sent for histopathological examination.
Fig. 3A: reflection of periosteal flap showing the cystic lesion, B: total excision of the lesion showing the boney cavity after removal of the cystic lesion, C: excisional biopsy of the cystic lesion with extraction of supernumerary tooth and related upper right lateral incisor
Approximately two weeks after the initial surgery and before the pathology report, there was no evidence of soft tissue healing at the surgical site, including the area of the extracted right lateral incisor. Instead, soft tissue thickening was observed, along with irregular tissue proliferation extending across the palatine mucosa (Fig. 4). These findings raised concern for residual pathology or possible malignant transformation,
Fig. 4. Photograph of the surgical site 2 weeks postoperative without soft tissue healing. Instead, soft tissue thickening was observed, along with irregular tissue proliferation extending across the palatal mucosa
The biopsy sample was fixed in 10% neutral buffered formalin, then processed and embedded in paraffin wax using the conventional procedures. Serial Sects. 3–4 μm thick were placed on glass slides and stained using hematoxylin and eosin (H&E). Then, the slides were studied under light microscopy.
The histological examination demonstrated a cystic cavity lined by corrugated parakeratinized stratified squamous epithelium with intraluminal keratin. Some areas showed partially uniform thickness with palisaded basal cells. The supra-basal cells are polyhedral and show intercellular edema and intercellular bridges. The epithelium-connective tissue interface is flat with an absence of rete pegs. Certain areas of the epithelial odontogenic surface undergo unusual squamous metaplasia with evident malignant changes in the underlying fibrous connective tissue capsule of the detected keratocyst. Epithelial pearls with central keratin formation and malignant cell nests are detected. Malignant criteria are detected, such as pleomorphism, hyperchromatism, as well as normal & abnormal mitotic figures. So, the lesion was diagnosed as an invasive, moderately differentiated, keratinizing SCC developing in an OKC (Figs. 5, 6 and 7).
Fig. 5A Photomicrograph of odontogenic keratocysts showing hyperplastic corrugated parakeratinized epithelial lining (H&E stain, x100). B High power of previous image showing the lumen of the cyst with large amount of keratin (arrow) and surrounded by epithelial lining which is parakeratinized (H&E stain, x400). C Photomicrograph showing epithelial lining with palisading basal cells and corrugated epithelial lining (H&E stain, x400)
Fig. 6. Photomicrograph showing a cystic cavity lined by parakeratinized stratified squamous epithelium (black arrows). Certain areas of the epithelial odontogenic surface undergo unusual squamous metaplasia with evident malignant changes in the underlying fibrous capsule of the detected keratocyst. Epithelial pearls with central keratin formation and malignant cell nests are detected (H&Ex100)
Fig. 7. Photomicrograph revealed epithelial pearls and cell nests of SCC with malignant criteria such as pleomorphism, hyperchromatism and normal & abnormal mitotic figures (H&Ex400)
The patient subsequently underwent a comprehensive workup, including a head and neck computed tomography (CT) scan (Fig. 8) and abdominal and pelvic ultrasound to exclude regional and distant metastases. Based on the clinical and radiographic findings, and after consultation with an oncologist, the patient was referred for a subtotal maxillectomy for total excision of the pathological tissue with enough safety margins. A subtotal maxillectomy was performed via a Weber-Ferguson incision, providing adequate access for complete surgical excision of the lesion (Fig. 9-A, B, C). The incision was closed meticulously to ensure optimal healing and achieve a more aesthetically acceptable outcome, particularly considering the young female patient’s age and appearance (Fig. 9-D). Histopathological analysis of the resected specimen confirmed clear surgical margins. A maxillary obturator was fabricated and delivered postoperatively to support function and aesthetics (Fig. 10). The patient was kept under regular follow-up for six months after the second surgery, during which no clinical signs of recurrence were detected. Unfortunately, the patient was lost to follow-up beyond this period.
Fig. 8CT scan coronal and axial cuts showing bony defect after removal of cystic lesion and palatal thickening
Fig. 9A, B: Weber-Ferguson incision, providing adequate access for subtotal maxillectomy. C: Excised maxilla including SCC with safety margins. D: incision was closed meticulously to ensure optimal healing
Fig. 10photograph showing patient follow up after subtotal maxillectomy with obturator perfectly replacing the defect and restoring esthetics and function
Discussion and conclusions
Odontogenic keratocyst (OKC) is a benign developmental cyst of odontogenic origin, recognized for its locally aggressive behavior and tendency for recurrence. Reported recurrence rates vary widely, from 0% to 62%, making it a clinically significant and challenging entity in maxillofacial pathology [26].
Malignant changes of the OKC lining are uncommon, despite its high recurrence rates and locally destructive behavior. Rare cases of malignant transformation into SCC have been reported [27]. The clinical and histological characteristics of a destructive maxillary cyst exhibiting moderately differentiated SCC were reported in this case report.
It’s interesting to note that the full histopathological analysis of the biopsies showed foci with nests of SCC emerging from the OKC lining that showed different levels of dysplasia. Prior to a diagnosis of a carcinoma arising in an odontogenic cyst, it is important to eliminate secondary involvement of a cyst by an unrelated adjacent carcinoma or cystic degeneration in a primary intraosseous carcinoma or in a metastatic deposit [28].
Gardner listed specific features for diagnosing SCC that arises in an odontogenic cyst: the lack of carcinomatous alterations in the lining epithelium, the lack of a source of carcinoma in the surrounding tissues, and the microscopic transition zone from benign cystic lining epithelium to invasive squamous cell carcinoma [29].
Waldron introduced a fourth criterion. Physical, radiological, and subsequent clinical examinations are necessary to rule out the potential that the lesion is a distant tumor metastasis [30].
Symptoms consistent with an odontogenic cyst were evident in the patient presented in this report. Large, untreated odontogenic cysts are known to cause thinning of the cortical bone and, in some cases, perforation of the palatal aspect of the maxilla. In this case, the mobility of the adjacent tooth and the presence of a supernumerary tooth within the cystic lesion supported the diagnosis of an odontogenic cyst, particularly one resembling a dentigerous cyst. Additionally, the patient’s age was within the typical range for the development of dentigerous cysts. This was in agreement with the literature regarding odontogenic manifestations [31].
In our case, after cystic lesion enucleation in the 1st surgery, the transformation was suspected clinically even before histopathology was available, based on delayed mucosal healing and abnormal proliferation on the palatal mucosa. This emphasizes the importance of close clinical follow-up during the early postoperative phase, especially in lesions initially thought to be benign.
Before initiating timely surgical intervention in such cases, a thorough understanding of the tumor’s biological behavior and cellular kinetics is essential. Since its initial description, the OKC is considered one of the most controversial pathological lesions of the maxillofacial area [32]. Although previously classified as a benign neoplasm in the 2005 WHO classification, OKC was reclassified as a cystic lesion in the 2017 and remains so in the 2022 WHO classification of Head and Neck Tumours [14]. On rare occasions, though, the OKC epithelial lining exhibits signs of dysplasia and malignant transformation to SCC [33].
Odontogenic tumors, which make up only 1% of all oral tumors, are classified as rare tumors in the most recent edition of the WHO. They are also benign entities that have a high recurrence rate and may behave aggressively [34]. In the 2017 edition, keratocystic odontogenic tumor is nowadays classified as a cyst and called an OKC [35].
Since carcinomatous transformation occurs in only about 1% of all odontogenic cysts, these carcinomas often present with clinical features that closely resemble those of benign expansile jaw lesions, not associated with pain or paresthesia. On plain radiographs, they appear similar to cystic lesions from which they arise. Therefore, depending on plain panoramic radiography in this case, which suggested a well-defined cystic lesion, was considered a limitation. While useful for preliminary evaluation, plain radiographs may underestimate the lesion’s true extent and fail to reveal cortical perforation or soft tissue involvement. CT would have provided more detailed information regarding the lesion’s boundaries, aggressiveness, and possible invasion of adjacent structures. Marcelo Cavalcanti et al. have claimed that because a CT scan provides a greater understanding of the damage to surrounding structures, it could be a more sensitive method of identifying a malignant change in the lesions [36].
According to previous reports, PIOSCC predominantly affects the mandible approximately 79% compared with the maxilla 21% [1, 15]. Cases of PIOSCC arising from an OKC have been documented across a broad age spectrum, with a mean age of 57 years and a male-to-female ratio of 2:1. Similar findings were observed in cases reported by Aboul-hosn Centenero et al.. in 2006 [37], Mosqueda Taylor et al.. in 2003 [38] and Scheer et al.. in 2004 [39]. However, this age distribution contrasts with our reported case, in which the patient was only 13 years old, representing an exceptionally early onset for such malignant transformation.
To date, only a few pediatric cases of SCC arising from odontogenic cysts have been published. Ours may be among the youngest reported cases, reinforcing the need to consider malignant potential even in the pediatric population, where OKC is more often associated with syndromic or developmental origins [40]. Other published studies showed SCC arising from maxillary OKC were reported in older age [23, 41].
The surgical approach via Weber-Ferguson incision allowed for adequate access and complete excision with safety margins. This technique is well-documented in the management of maxillary tumors and provides both functional and aesthetic advantages when carefully closed, particularly in young patients [42]. Postoperative rehabilitation with a maxillary obturator proved effective in restoring speech, mastication, and aesthetics.
Although the patient was recurrence-free for six months postoperatively, she was unfortunately lost to follow-up thereafter. Long-term follow-up is essential given the potential for delayed recurrence, particularly in malignancies arising within odontogenic cysts. Literature suggests at least five years of follow-up with periodic imaging and clinical evaluation to monitor for recurrence or metastasis [34].
The histopathological examination in this case revealed carcinomatous alterations in the lining epithelium of the odontogenic keratocyst. The occurrence of carcinoma associated with this OKC was unforeseen, paralleling other documented instances where similar unexpected features were noted [28].
There were no indications of nerve paraesthesia or pain, likely due to the malignant changes still in the early stages of development. This may account for the well-defined radiolucency observed in the panoramic film. This contrasts with the observations suggesting that malignant transformations in odontogenic cysts had to be suspected if the radiolucent area exhibits uneven edges with indentations and poorly defined borders [36], a scenario not applicable to the current report.
Instances of the epithelial lining of OKC exhibiting dysplastic criteria and carcinomatous transformation are seldom reported, making this particular case significant due to the presence of malignant changes, especially considering that it involves a pediatric patient [43].
In conclusion, the clinical manifestations, radiographic, and histopathologic criteria of a carcinomatous change of an OKC in the maxilla of a young female patient are presented in this unique case report of moderately differentiated SCC. It also emphasizes how crucial it is to carefully examine any removed pathologic tissue histopathologically due to the potential for carcinomatous change in the cystic lesion’s epithelial lining.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Saxena C, Aggarwal P, Wadhwan V, Bansal V. Primary intraosseous squamous cell carcinoma in odontogenic keratocyst: a rare entity. J Oral Maxillofac Pathol: JOMFP. India. 2015;19:406. https://pubmed.ncbi.nlm.nih.gov/26980976/10.4103/0973-029X.174615.10.4103/0973-029X.174615 PMC 477430126980976 · doi ↗ · pubmed ↗
- 2Maria A, Sharma Y, Chhabria A. Squamous cell carcinoma in a maxillary odontogenic keratocyst: a rare entity. Natl J maxillofac Surg. India; 2011;2:214–8. 10.4103/0975-5950.94486.10.4103/0975-5950.94486 PMC 334340022639518 · doi ↗ · pubmed ↗
- 3Loos D. Central epidermoid carcinoma of the jaws. Dtsch Mscnr Zahnhelic. 1913;31:308 10. Quoted in: Morrison R, Deeley TJ. Intra alveolar carcinoma of the jaw. Treatment by supervoltage radiotherapy. Br J Radiol. 35:321–6. 10.1259/0007-1285-35-413-321.10.1259/0007-1285-35-413-32114476303 · doi ↗ · pubmed ↗
- 4Kumchai H, Champion AF, Gates JC. Carcinomatous transformation of odontogenic keratocyst and primary intraosseous carcinoma: a systematic review and report of a case. J Oral Maxillofac Surg. 2021;79(5):1081.e 1–1081.e 9. 10.1016/j.joms.2020.12.04633529609 · doi ↗ · pubmed ↗
- 5Jalali E, Ferneini EM, Rengasamy K, Tadinada A. Squamous cell carcinoma arising within a maxillary odontogenic keratocyst: a rare occurrence. imaging science in dentistry. Korea (South). 2017;47:135–40. 10.5624/isd.2017.47.2.135.10.5624/isd.2017.47.2.135PMC 548967028680851 · doi ↗ · pubmed ↗
- 6Sharif FN, Oliver R, Sweet C, Sharif MO. Interventions for the treatment of keratocystic odontogenic tumours (KCOT, odontogenic keratocysts (OKC)). Cochrane Database Syst Rev. 2010;(9):CD 008464. 10.1002/14651858.cd 008464.pub 3.10.1002/14651858.CD 008464.pub 220824879 · doi ↗ · pubmed ↗
- 7Suma NK, Babu NSV, Jha S, Dental V. In. Odontogenic keratocyst of maxillary premolar region: a case report. 2015. https://www.semanticscholar.org/paper/Odontogenic-Keratocyst-of-Maxillary-Premolar-A-Case-Suma-Babu/730b 531de 200ab 391700 cc 34f 6d 329c 3b 6fa 2837.
- 8Medawela RMSHB, Jayasuriya NSS, Ratnayake DRDL, Attygalla AM, Siriwardena BSMS. Squamous cell carcinoma arising from a keratocystic odontogenic tumor: a case report. J Med Case Rep. 2017;11(1):335. Available from: 10.1186/s 13256-017-1486-x.10.1186/s 13256-017-1486-x PMC 571012929191248 · doi ↗ · pubmed ↗