MMP-9 as a diagnostic salivary biomarker for early detection of oral cancers: systematic review and meta-analysis
Aqsa Shaukat, Saleha Nisar, Mehmood Asghar, Muhammad Kaleem, Muhammad Sohail Zafar

TL;DR
This study reviews and analyzes the effectiveness of using salivary MMP-9 as a diagnostic biomarker for early-stage oral cancer.
Contribution
The study provides a systematic review and meta-analysis of salivary MMP-9's diagnostic accuracy for early-stage oral cancer.
Findings
Salivary MMP-9 showed high pooled sensitivity and specificity for detecting early-stage oral cancer.
The study found a high area under the curve (0.97) for salivary MMP-9 as a diagnostic biomarker.
The study highlights the need for further research due to high heterogeneity and risk of bias.
Abstract
The intention of this investigation was to evaluate the diagnostic performance of salivary MMP-9 enzyme for rapid point of care testing of early stage (I, II) oral cancer. Diagnosis at early pre-malignant stages will help in making clinical decisions for timely intervention. Original diagnostic test accuracy (DTA) studies of any design, on patients with lip and oral cavity cancers investigating salivary MMP-9 levels as an index test and histopathological confirmation via biopsy as a reference test were eligible for inclusion. Similar studies on serum or blood were excluded. Besides, the case reports/case series, reviews, letters, book chapters, conference abstracts, in vitro, and animal studies were all excluded. Non-English papers were not excluded. The databases searched from Jan 2014 to Aug 2024 were PubMed, SCOPUS, Cochrane Library, Science Direct, and Google Scholar, without…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
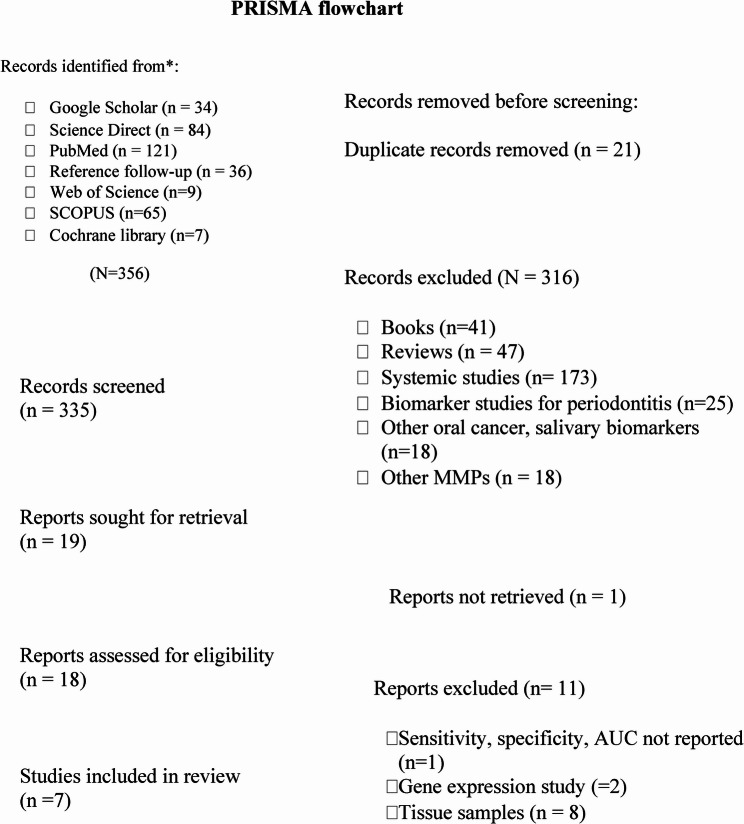 Figure 1
Figure 1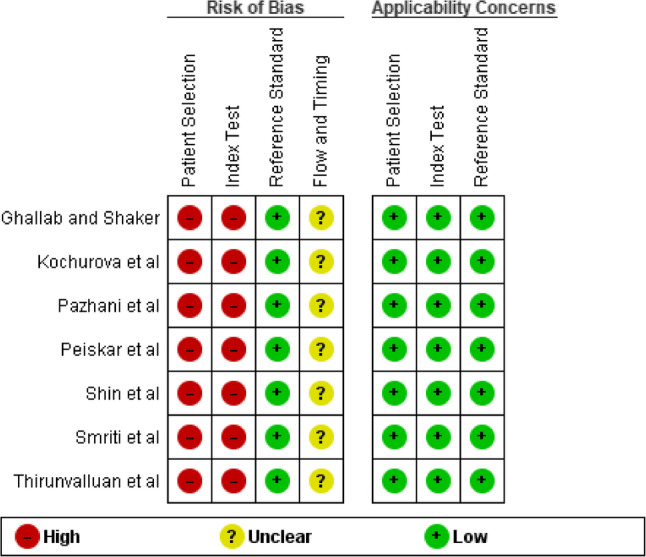 Figure 2
Figure 2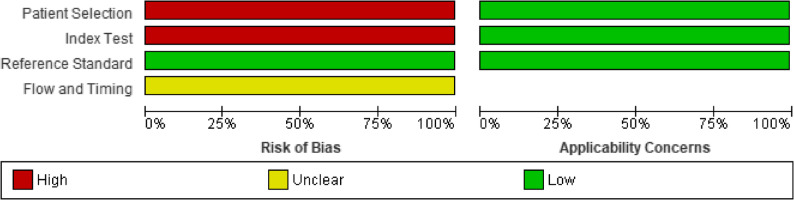 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5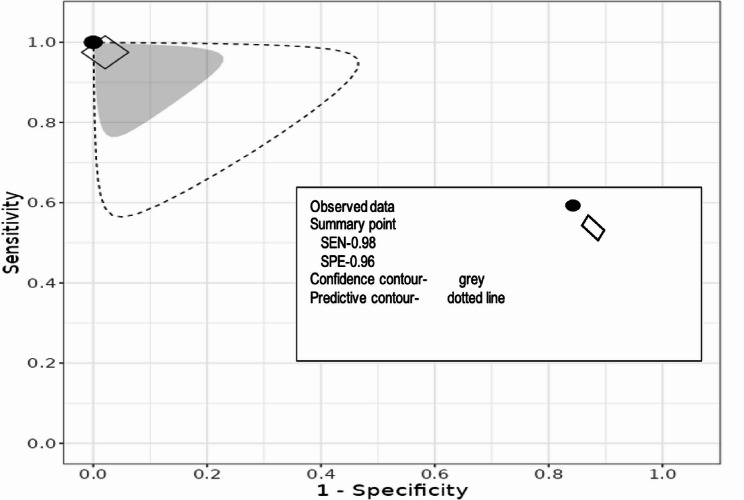 Figure 6
Figure 6- —NUMS student grant
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Disorders and Functions · Oral Health Pathology and Treatment · Head and Neck Cancer Studies
Introduction
According to GLOBOCAN 2022, Lip and oral cavity cancer (LOC) is the 16th most diagnosed neoplasm (C00-C06) overall. Almost 389,485 new cases of oral cancer were diagnosed, and over 188,230 deaths were reported worldwide [1]. Cancers of the lip and oral cavity encompass malignancies affecting the lip, tongue, and oral cavity, primarily developing from epithelial cells, with approximately 90% classified as oral squamous cell carcinoma (OSCC) [2]. The cumulative risk for males and females worldwide is 21.79% and 18.5% [1].
The occurrence of OSCC is correlated with various risk factors, including tobacco use (chewing or smoking), alcohol consumption, intake of foods high in nitrosamines, infection with human papillomavirus, environmental exposures such as ultraviolet radiation, and dietary deficiencies resulting from insufficient consumption of fruits and non-starchy vegetables [3]. The incidence of oral cancers can be reduced by minimizing exposure to risk factors or by timely screening for potentially malignant oral disorders (OPMDs), including leukoplakia, erythroleukoplakia, oral lichen planus, and oral submucous fibrosis [4]. Therefore, early diagnosis is crucial for improving the prognosis and patient outcomes. Unfortunately, in most cases, by the time it is diagnosed, malignancy has already reached its advanced stages. Traditional method of diagnosing OSCC is to perform a surgical resection of the suspected tissue and doing a histopathological study on that tissue. It is a gold standard diagnostic procedure for identifying oral cancer [5]. This modality has its limitations as well, such as patient discomfort, invasiveness, and potential sampling errors related to subjective interpretation. Besides, often times the histopathological picture is inconsistent with clinical findings [5, 6]. For these reasons, there is a need to explore alternate diagnostic methods [7, 8].
A biological marker is an indicator of a state, condition, or process in a biological system. Unlike any medical symptom, which are subjective experiences patients report, biomarkers are measurable or objective medical signs [9], hence considered chemical fingerprints. They can be proteins, nucleic acids, metabolites, or other molecules found in body fluids. Using biomarkers as a diagnostic tool can provide objective results while enhancing patient comfort and compliance. The neoplastic changes and their effects are seen quite early biochemically compared to clinical diagnosis or histopathology [7]. Hence, by using biomarkers we can identify oral cancer at earlier stages (I, II) before progression to advanced stages.
The biomarkers that can be used for OSCC diagnosis are released in biofluids like blood, urine, sweat, and saliva [7, 10]. Saliva is described as a mirror of the body, providing a comprehensive snapshot of overall health [11]. Its use as a diagnostic medium for the biomarker offers a promising alternative to tissue biopsies. Its collection is easy, non-invasive, fast, and cost-effective [12]. Based on the disease state, salivary biomarkers can be divided into prediction, detection, diagnostic, and prognostic biomarkers [13]. Researchers have explored salivary factors as biomarkers for OSCC and potentially malignant disorders (OPMD). Analysis of salivary proteomics, genomics together with the variation in their levels, may provide us insights into progression of oral cancer, its prognosis and post-treatment follow-ups [12, 14].
A gelatinase enzyme matrix metalloproteinase-9 (MMP-9) breaks down denatured collagen or gelatin under physiological process involving tissue remodeling like wound repair, formation and development of blood vessels and embryo. It particularly degrades type-IV collagen, which is an important basement membrane component [15, 16]. The MMP-9 regulation is disturbed in other pathological conditions, such as diabetes mellitus, neurodegenerative diseases, renal pathologies, and cardiac conditions [17], however in cancers MMP-9 enzyme regulation is lost at multiple levels such as during its transcription, activation, interaction with extracellular matrix (ECM), inhibition by tissue inhibitors for matrix metalloproteinase (TIMPs) or during its elimination from the ECM. Invading tumor cells secrete dysregulated proteases like MMPs, which degrade ECM and basement membrane. This increase in proteases facilitates cell motility, changes cell-cell adhesion properties, rearranges ECM, suppresses programmed cell death, and reorganizes their cytoskeleton. MMPs like MMP-2 and 13 are also raised in OSCC and increase with disease progression [17]. MMP-9 has been identified as a helpful early diagnostic biomarker that detects tumor metastasis and prognosis in OSCC patients [18]. Furthermore, a study linked MMP-9 expression with tumor invasion and lymph node involvement in OSCC. Interestingly, there are also reports that the level of MMP-9 doesn’t seem to be linked to the stage of the tumor or the lymph nodes., but rather as a prognostic factor for poor survival in head and neck carcinoma [14]. This lack of consensus highlights the uncertainty surrounding MMP-9’s role as a prognostic or diagnostic biomarker.
Existing literature has not exclusively concentrated on its role as a biomarker for the diagnosis of oral cancer in its early stages (I, II). Utilizing systematic review protocols and methodologies, we have collected original research articles about MMP-9 in the context of oral cancer, thereby offering a thorough synthesis of the existing knowledge on this topic. Our objective was to present an overview of the potential significance of salivary MMP-9. Therefore, the primary aim of this review was to investigate the relationship between salivary MMP-9 biomarkers and oral cancer and its diagnostic accuracy for the oral cancers in its early stages.
Materials and methods
The review was conducted thoroughly following the PRISMA Checklist [19] to ensure a systematic approach. The protocol was registered at PROSPERO as CRD 42,024,573,382.
Search protocols
The search protocols were defined, and a PICO format review question was formulated. The focused question was, “Can salivary MMP-9 levels be used for diagnosis of early-stage (I, II) oral cancer in adult patients?”. The study will evaluate salivary MMP-9 diagnostic performance (outcome) in adult patients with oral cancer (population) as compared to healthy patients (control) using ELISA (intervention).
Eligibility criteria
The diagnostic test accuracy (DTA) studies of any design, measuring salivary MMP-9 levels in adult patients, were included in this review. However, studies testing MMP levels other than MMP-9 or those testing in body fluids other than saliva were excluded. The case reports/case series, reviews, letters, book chapters, conference abstracts, in vitro, and animal studies were also excluded. Non-English papers were not excluded.
Information sources and search strategy
Detailed individual search strategies were developed for the Cochrane Library, MEDLINE, Science Direct, and SCOPUS databases. The search covered all articles published between January 2014 and August 2024, without language or other filters. References were manually maintained, duplicates eliminated, and further references reviewed in selected papers.
The search string
A search string was defined according to PICO criteria [19] Various outcomes including salivary MMP-9 levels, Area Under the Curve (AUC), sensitivity (SEN), and specificity (SPE) were measured. The target population was adults aged 20–65 with oral cancer, oral potentially premalignant disorders (OPMD) or suspicious lesions undergoing diagnostic methods like in situ zymography or ELISA. The histopathological confirmation with biopsy is a gold standard reference test for oral cancer against a healthy control group. The string was fine-tuned for every database (Table 1).
Table 1. Electronic databases and respective keyword combinations usedDatabaseSearch stringDateScience Direct(((((“oral cancer”) OR “oral squamous cell carcinoma” OR (“OSCC”)) AND (“saliva biomarkers”)) AND “ELISA” OR “in situ zymography” AND (“matrix metalloproteinases”)) OR (“MMP”) AND “diagnostic accuracy”12-7-24MEDLINE(((((“oral cancer”) OR “oral squamous cell carcinoma” OR (“OSCC”)) AND (“saliva biomarkers”)) AND “ELISA” OR “in situ zymography” AND (“matrix metalloproteinases”)) OR (“MMP”) AND “diagnostic accuracy”12-7-24Google Scholar(((((“oral cancer”) OR “oral squamous cell carcinoma” OR (“OSCC”)) AND (“saliva biomarkers”)) AND “ELISA” OR “in situ zymography” AND (“matrix metalloproteinases”)) OR (“MMP”) AND “diagnostic accuracy”12-7-24Cochrane library“Oral cancer” OR “oral squamous cell carcinoma” OR “OSCC” AND “saliva biomarkers” AND “ELISA” OR “in situ zymography” AND “matrix metalloproteinases” OR “MMP” AND “diagnostic accuracy”12-7-24SCOPUSOral AND cancer OR OSCC AND salivary AND biomarkers OR tumor, biomarkers AND matrix metalloproteinases OR MMP AND diagnostic accuracy13-7-24Web of ScienceOral AND cancer OR OSCC AND salivary AND biomarkers OR tumor, biomarkers AND matrix metalloproteinases OR MMP13-7-24
Screening of data
The extraction of data was carried out by three researchers. In the first step, AS selected the studies independently. The titles and abstracts of the references were assessed. The selected papers met the inclusion criteria based on their titles and abstracts. Studies that did not match the inclusion criteria were excluded. SN and MA evaluated the screening results.
In the second stage, entire papers were reviewed to determine which ones reported sensitivity and specificity or offered data that permitted these diagnostic evaluations to be made. AS also carefully examined the reference lists of all included papers. Any differences during either phase were resolved through discussion and consensus among the three reviewers (AS, SN and MA).
Extraction of data
Data processing
The extraction process involved three researchers. AS gathered the necessary information from the chosen articles. SN verified the collected data and ensured its accuracy. AS obtained the essential information from the chosen articles. SN verified the collected data to guarantee its accuracy. Any discrepancies during any stage was resolved through discussion among AS, SN, and MA.
Data items
The information from included studies like authors name, country, year of publication, sample size, reference/index test and outcomes reported were documented. Outcome measures include mean MMP-9 levels (ng/ml), sensitivity (SEN), specificity (SPE), and area under the curve (AUC). If any required data were missing, no efforts were made to contact the authors for the missing information.
Qualitative and quantitative assessment
Analysis of bias
The Quality Assessment Tool for Diagnostic Accuracy Studies (QUADAS) was used to assess the bias. Reviewers (AS) and (SN) answered each question in the tool as either “yes,” “no,” or “unclear” and evaluated the quality of each study included.
Meta-analysis
A meta-analysis was conducted to evaluate the ability of the MMP-9 to distinguish OSCC patients from controls. The web application Meta DiSc 2.0 [20], was utilized to create a summary receiver operating characteristic (SROC) graph. At the same time, REVMAN version 5.4 was employed for generating forest plots as part of the meta-analysis.
Results
A total of 356 papers were identified from the databases. After removing the duplicates (n = 21), the electronic search yielded 335 studies. Out of these, 316 were excluded after title and abstract screening. A total of 18 reports were sought for retrieval and then assessed for eligibility. Only 7 studies [21–27] met the specified inclusion criteria in this review, encompassing 795 patients (398 controls, 209 OSCC, 166 OPMD, and 22 smokers). A flow chart detailing the process of identifying, including, and excluding studies is shown in Fig. 1.
Fig. 1PRISMA Flowchart
Study characteristics
The characteristics of the studies included in this review are shown in Table 2. The included papers were from Afghanistan, Egypt, Germany, India, Korea, and Russia between 2017 and 2023. All these studies were two-gate exploratory DTA studies [28, 29]. Patients were grouped into case and control groups. The case group included OSCC and OPMD patients. The OSCC patients were from all stages (I -IV). Only one study reported MMP-9 according to OSCC grading [26]. The OPMD reported were oral submucous fibrosis (OSF) leucoplakia, erythroplakia and papilloma. The tongue and buccal mucosa were more frequently reported sites [21, 26]). The details on TNM stages or anatomical subsites are mentioned in supplementary table S1. All studies used the ELISA immune assay method to measure salivary MMP-9 levels, while no study used in situ zymography. The cut-off/threshold values were not pre-specified for any of the studies, and few studies reported any cut-off values [25–27]. All studies reported AUC, SEN, SPE, and mean MMP-9 values except for two with missing data, either mean values [23] or SEN/SPE [25]. The gold standard or reference test for all studies was histopathological confirmation through biopsy; however, one study also used CT-PET. Salivary MMP-9 levels were considered an index test and reported in ng/ml, except for one study where no scale was mentioned [23].
Table 2. Study characteristicsAuthor names/countriesType and method of saliva collectionSample sizeCases/controlIndex test (MMP-9ng/ml)Cut off value (ng/ml)SENSPEAUCGhallab and Shaker2017 [21](Egypt)USWS byPassive drooling method4515 OSCC1642.5 ± 1498.9260100%100%115OPMD275.81 ± 30.88214100%0.9915control108.44 ± 31.43318.7Kochurova et al.2017 [27](Russia)Not specified12257PL403 ± 69.8NR83.30%53.30%0.565control388 ± 125.80Pazhani et al.2023 [26](India)USWS byPassive drooling method10234 OSCC50.9 ± 5.7NR100%26.70%NR34 PL31.6 ± 6.034 controls16.2 ± 4.8Peisker et al.2017 [23](Germany)Stimulated saliva samples6030OSCCNR0.014100%26.70%0.69830 controlsShin et al.2021 [24](Seoul/Korea)USWS byPassive drooling method318106 OSCC511.86 ± 0.12120.9212 controls29.27 ± 0.0889.60%100%0.96Smriti et al.2020 [22](India/Afghanistan)8824 OSCC387.87 ± 126.51214100%59%0.91720 OPMD339.86 ± 115.7205.8100%54%0.852USWS22 smokers22 controls213.91 ± 67.11Thiruvalluvan et al.2021 [25](India)Unstimulated salivary samples6020 OSMF9.42 ± 0.859NRNRNR0.920 OL10.59 ± 0.85920 controls2.96 ± 0.859
All studies used ELISA and “histopathology following biopsy” as a reference test.
Risk of bias
The QUADAS-2 tool [30] was used for qualitative assessment. Figures 2 and 3 mention the risk of bias and applicability concerns for individuals and across studies.
Fig. 2. Quality assessment using the QUADAS-2 tool for individual diagnostic accuracy studies
Fig. 3 Graph for risk of bias and applicability concern, QUADAS-2 tool across diagnostic accuracy studies
The study designs, as reported, were prospective [23, 27], cross-sectional [22], observational [26], case-control [24], and clinical trial [21, 25]. All studies used two gates for patient selection, i.e., case and control groups were selected on different criteria, instead of using a single pool of patients with the same selection criteria. It was also based on prior knowledge of reported OSCC, which was later confirmed through histopathology, and inappropriate exclusions weren’t mentioned either. No study mentioned whether both index and reference test results were interpreted with/without knowledge of the results of the other one. The reference standard used was likely to classify the target condition, so overall bias in this section was reported to be low. The threshold/cut-off values were reported by [21–24] but were not pre-specified. These studies did not report the fourth domain, which discusses the flow and timing of both tests. The concerns for applicability were low, as the study population used in individual studies was the same as the review question. Overall, there was a high risk of bias, which should be interpreted by keeping exploratory designs in sight. Cohen’s kappa score was calculated using an online tool [31]. It was 0.35, which showed fair agreement.
Results of individual studies
All included studies emphasize the significance of salivary MMP-9 as a biomarker for early-stage oral cancer. Ghallab and Shaker [21] noted its use in screening and diagnosing early cancer, though it’s not a replacement for established diagnostic tools. Shin et al. [24] found that salivary MMP-9 levels may improve outcomes in OSCC patients, including mortality and morbidity. Smriti et al. [22] consider it an early detection diagnostic tool, but not for recurrence follow-up. A non-intrusive saliva-based screening kit could aid in identifying OSCC and OPMD patients. Pazhani et al. [26] observed higher salivary MMP-9 levels in poorly differentiated OSCC, suggesting it as an alternate marker for cancerous transformation. Salivary diagnostics for OSCC are promising due to the direct contact between oral cancer lesions and saliva, making it non-invasive and suitable for population screening, especially in remote areas [23, 27]. Thiruvalluvan et al. [25] found significant MMP-9 expression in oral leukoplakia and OSMF as compared to control, considering it a reliable biomarker for assessing OPMD malignant transformation. However, they reported an insignificant difference in expression between the two types.
Meta-analysis
The forest plots for MMP-9 values for OSCC are shown in Fig. 4. The overall effect size was SMD 5.96 with 95% confidence interval − 3.30 to 15.22. The heterogeneity or I^2^ was 100% while p-value was 0.21. The quantitative synthesis for sensitivity and specificity is shown in Fig. 5. The pooled sensitivity and specificity were consistently higher, 1.00 and 1.00, respectively with 95% confidence interval between 0.85 and 1. The summary ROC graph (Fig. 6) shows the summary operating point (black point), confidence contour (grey), and prediction contour (dotted line). Since, the number of included studies were less than 10 the publication bias testing was not pursued.
Fig. 4. Forest plot of salivary MMP-9 in OSCC
Fig. 5. Sensitivity and specificity plot for salivary MMP-9 in OSCC
Fig. 6. Summary Receiver Operators Curve (SROC) for salivary MMP-9 in OSCC
Discussion
The accuracy of diagnostic tests plays a pivotal role in clinical decision-making, influencing patient management and healthcare outcomes. The rapid diagnostic tests, due to their speed, convenience, and portability, are preferred over routine laboratory processing. In this systematic review, we evaluated the diagnostic performance of salivary MMP-9 enzyme for rapid testing of oral cancer in early stages (I, II). We synthesized evidence from multiple studies to provide a comprehensive assessment of its sensitivity and specificity. Our findings highlight key methodological considerations, clinical implications, and potential limitations inherent in the evaluation of diagnostic test accuracy.
Salivary MMP-9 is an enzyme protein involved in multiple cancer-related processes. It cleaves surface proteins, degrades ECM, and alters cell-to-cell and cell-to-ECM interactions [32]. Its involvement in other systemic conditions has also been reported. Its serum and, hence, salivary levels may increase in not only inflammatory conditions like diabetes, autoimmune diseases, and arthritis but also in hypertension, atherosclerosis, and myocardial infarction [33]. MMP-9 involvement in cancers has been reported extensively, such as in osteosarcoma, giant cell bone tumor, and other cancers, such as hepatocellular cancer, lung cancer, cervical cancer, ovarian cancer, and breast cancer [32], and specifically oral cancer [18, 34, 35]. Approximately 30% of the proteins in plasma are also present in saliva [36, 37], which suggests significant links between the salivary proteome and various bodily systems. For example, tumor necrotic factor-alpha is released in the serum and saliva of OPMD patients [32]. With more advanced analytical techniques, saliva can be a valuable resource for translating biomarker studies to point-of-care diagnostic devices, particularly in dental and personalized medicine [36, 37].
The present systematic review evaluated the potential role of MMP-9 in determining its diagnostic significance as a biomarker for oral cancers in early stages (I and II). The systematic literature search identified studies reporting the diagnostic accuracy of salivary MMP-9 levels. The review of included studies suggested a promising potential of salivary MMP-9 for the early detection of oral cancers, specifically at initial stages I and II.
The included studies in the present review were from Europe, Asia, and Africa. Qualitative assessment is the most critical component of any systematic review, facilitating the synthesis of high-quality evidence [38]. In line with this, studies included for assessment are expected to provide all the necessary information to establish constructive results. The DTA studies should be reported according to Standards for Reporting Diagnostic Accuracy Studies (STARD) guidelines [39] to ensure every aspect gets covered. However, all studies in this review were surprisingly not per STARD guidelines.
The QUADAS-2 tool was used for qualitative assessment. It presented a high risk of bias, however, with low concerns for applicability. This is because all the studies included in this review were exploratory design according to Cochrane Diagnostic Test Accuracy (DTA) guidelines [29]. This guideline categorizes diagnostic accuracy studies as exploratory and pragmatic studies. The exploratory studies establish a hypothesis, whereas pragmatic trials help in clinical decision-making. Another difference between these studies is that the threshold value is explored in the exploratory study, whereas it is pre-specified in the pragmatic study. The exploratory study often uses a smaller sample size and involves a single centre compared to a larger sample size and multiple centers in pragmatics [28]. The pragmatic designs have a single criterion for patient selection, which is also called a single gate study. Second, a blinded interpretation of the index and reference test is sought [40–43]. Third, the flow and timing of both tests are essential because any long interval between two or more tests can introduce bias in a study [40–43]. Ideally, both tests shall be taken simultaneously [40–43].
The sensitivity and specificity forest plots (Fig. 5) summarize the results of five studies on the oral cancer diagnosis using MMP-9 as a biomarker. All five studies 24, 26) demonstrate a sensitivity of 1.00, indicating that the test correctly identified all actual positive cases in each study. The 95% confidence intervals (CIs) for sensitivity in all studies range from 0.78 to 1.00, suggesting high sensitivity with some variability in the lower bound of the CI. The consistency of these results across multiple studies suggests that the diagnostic test using MMP-9 as a biomarker is highly effective for detecting oral cancer in its early stages (I and II). The subgroup analyses were not possible as MMP-9 values were not consistently reported by included studies. One study report values by cancer staging [24] and others [22, 26] by grading, only one study reports according to anatomical subsite [24] (Table S1).
However, the overall effect shown in Fig. 4 challenges the hypothesis that MMP-9 could serve as a diagnostic biomarker. There can be several reasons why the overall effect’s p-value is not significant, even though individual studies show substantial p-values. First, high heterogeneity represents high variability among studies, diluting the overall impact and making it less likely to reach statistical significance. Secondly, although the overall sample size was large, the effect sizes varied significantly between studies. The inconsistent effect sizes across studies can result in the overall effect not being statistically significant. Thirdly, wide confidence intervals in overall effect size indicate uncertainty in the estimate, which can lead to insignificant p-values. Other reasons may include the presence of publication bias and the use of different statistical methods across studies. Additionally, while our meta-analysis aimed to provide pooled estimates, the presence of this heterogeneity suggests that caution must be exercised in interpreting summary estimates and underscores the need for further research to verify the diagnostic performance of MMP-9 in OSCC.
Beyond numerical accuracy, the clinical applicability of an index test is evaluated in terms of false positives and false negatives. In diagnostic settings where misclassification can have serious consequences, understanding the trade-offs between sensitivity and specificity is crucial. False negatives may lead to delayed interventions and potentially worsen clinical outcomes, while false positives could result in unnecessary treatments and increased healthcare costs. Therefore, the clinical utility of the test must be evaluated beyond statistical measures, integrating real-world implications.
The study has several limitations. Although, the literature search was systematic, missing of any published or unpublished article cannot be ruled out. Secondly, the included studies were found to have low methodological quality and level of reporting. While these two-tailed designs might be helpful in early evaluation of diagnostic tests, they usually lead to inflated test results compared to what could be expected in clinical practice. Lastly, since there was high level of heterogeneity i.e. I^2^ = 100% among the studies, the summary estimates from the exploratory meta-analysis need to be interpreted very cautiously. Further studies on pragmatic design are needed to establish its importance as an aid in screening oral cancers.
Future research should aim to refine threshold selection strategies, ensuring better test standardization and reproducibility across diverse clinical settings. Additionally, salivary MMP-9 testing can be seamlessly integrated into clinical workflow through the development of rapid, non-invasive point of care assays and chairside diagnostic kits. Apart from its use as POC diagnostic tool, salivary MMP-9 can be used as a screening tool and incorporated into high-risk population programs such as tobacco users or individuals with precancerous lesions using mobile health care units or saliva collection kits. Such integration would support timely intervention, personalized care and improved outcomes. Besides, comparison with other established biomarkers is essential for placing its performance in proper clinical context. By directly assessing multiple biomarkers under identical conditions and patient cohorts, clinicians can identify synergistic biomarker panels which when used together to enhance diagnostic accuracy beyond what any single marker can achieve.
Conclusions
Within the limitations of this review, salivary MMP-9 levels demonstrate promising potential as a critical biomarker for the detection of OSCC in early stages (I, II). Elevated MMP-9 in saliva may reflect early pathological changes preceding overt clinical symptoms. Its testing at the time of initial inquiry of OPMD will offer a valuable window for timely intervention. To fully validate and harness this potential, future research should prioritize prospective multicentre studies to ensure reproducibility across diverse populations and clinical settings.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Silva LTL, Nicolau CA, Moreira CSPD, Silva AA, de Carvalho L, Fernandes GE. RMD, Diagnosis of oral cancer using biomarkers, a non invasive proposal | International Seven Journal of Health Research. Available from: https://sevenpublicacoes.com.br/index.php/ISJHR/article/view/3748. Cited 19 Mar 2025.
- 2Sahibzada HA, Khurshid Z, Khan RS, Naseem M, Siddique KM, Mali M, et al. Salivary IL-8, IL-6 and TNF-α as potential diagnostic biomarkers for oral cancer. Diagnostics. 2017 June;7(2):21.10.3390/diagnostics 7020021 PMC 548994128397778 · doi ↗ · pubmed ↗
- 3Khurshid Z, Zafar MS, Khan RS, Najeeb S, Slowey PD, Rehman IU. Role of Salivary Biomarkers in Oral Cancer Detection. In: Advances in Clinical Chemistry. Elsevier; 2018. pp. 23–70. Available from: https://linkinghub.elsevier.com/retrieve/pii/S 0065242318300313. Cited 19 Apr 2025.10.1016/bs.acc.2018.05.00230144841 · doi ↗ · pubmed ↗
- 4Utilization of the PICO framework. to improve searching Pub Med for clinical questions | BMC Medical Informatics and Decision Making | Full Text. Available from: https://bmcmedinformdecismak.biomedcentral.com/articles/. 10.1186/1472-6947-7-16. Cited 26 Apr 2025 Apr 26.10.1186/1472-6947-7-16PMC 190419317573961 · doi ↗ · pubmed ↗
- 5Bossuyt PM. Understanding the design of test accuracy studies. In: Deeks JJ, Bossuyt PM, Leeflang MM, Takwoingi Y, editors. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy. 1st edn Wiley; 2023. pp. 35–51. Available from: https://onlinelibrary.wiley.com/doi/. 10.1002/9781119756194.ch 3. Cited 21 Feb 2025.
- 6Bobbitt Z. Cohen’s Kappa Calculator. Statology. 2021. Available from: https://www.statology.org/cohens-kappa-calculator/. Cited 22 Sept 2024.
- 7Deeks JJ, Bossuyt PM. Evaluating medical tests. In: Deeks JJ, Bossuyt PM, Leeflang MM, Takwoingi Y, editors. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy. 1st edn Wiley; 2023. pp. 19–33. Available from: https://onlinelibrary.wiley.com/doi/. 10.1002/9781119756194.ch 2. Cited 21 Feb 2025.
- 8Deeks JJ, Takwoingi Y, Macaskill P, Bossuyt PM. Understanding test accuracy measures. In: Deeks JJ, Bossuyt PM, Leeflang MM, Takwoingi Y, editors. Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy. 1st edn Wiley; 2023. pp. 53–72. Available from: https://onlinelibrary.wiley.com/doi/. 10.1002/9781119756194.ch 4. Cited 24 Jul 2024.