Temporal Patterns of Adverse Events Associated With Selective Serotonin Reuptake Inhibitors: A Global Pharmacovigilance Analysis of Early-Onset Versus Late-Onset Toxicity
Adrian Chin Yan Chan

TL;DR
This study analyzes when common side effects of antidepressants called SSRIs occur, finding that some appear quickly while others develop over time.
Contribution
The study identifies distinct early- and late-onset adverse event patterns for SSRIs using global pharmacovigilance data.
Findings
Early-onset adverse events include nausea, insomnia, and dizziness within the first few days of SSRI use.
Late-onset adverse events like weight gain and diabetes develop over weeks to months of SSRI treatment.
Early AEs are mostly gastrointestinal or neurological, while late AEs are metabolic or endocrine-related.
Abstract
Background Selective serotonin reuptake inhibitors (SSRIs) are commonly used as first-line antidepressant medications, but adverse events (AEs) remain a common reason for treatment discontinuation. Understanding when these AEs occur can help improve patient care and treatment adherence. Objective This study aims to explore the timing of AEs associated with six commonly used SSRIs: sertraline, fluoxetine, fluvoxamine, paroxetine, citalopram, and escitalopram using global pharmacovigilance data, with a focus on early- versus late-onset profiles. Methods This study analyzed Individual Case Safety Reports (ICSRs) from VigiBase, the World Health Organization's global safety database. Reports were included if an SSRI was the suspected drug and time-to-onset (TTO) data were available. AEs with at least 10 reported TTOs were grouped as early-onset (TTO ≤28 days) or late-onset (TTO >28…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
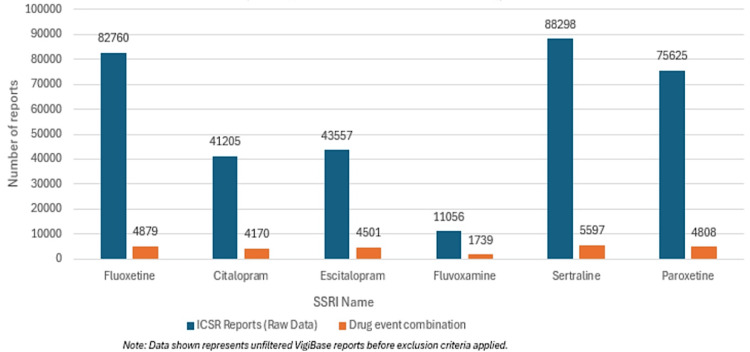 Figure 1
Figure 1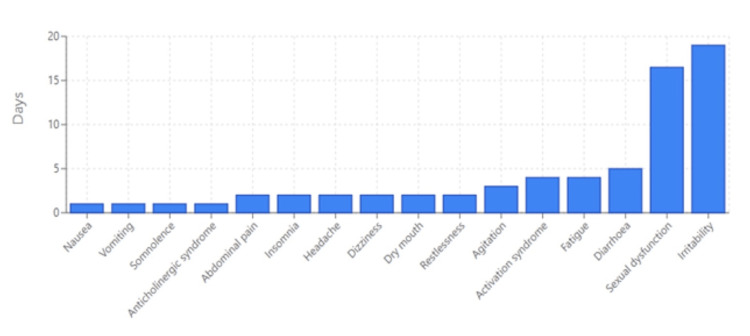 Figure 2
Figure 2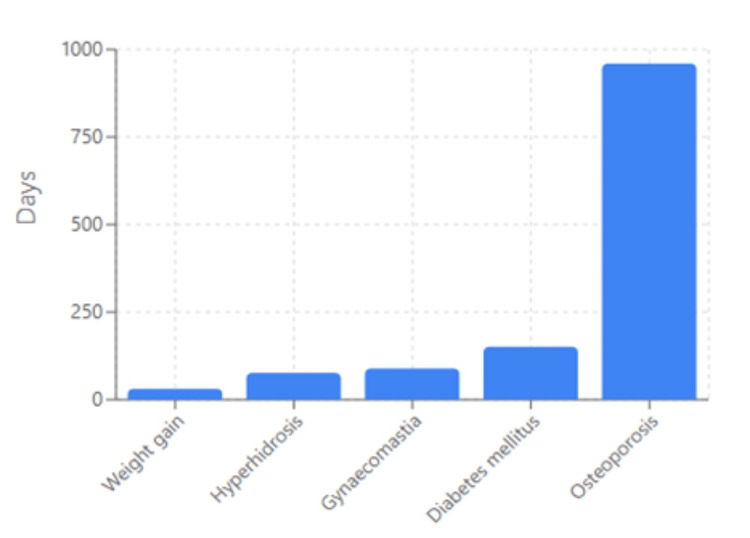 Figure 3
Figure 3| Variable | Description | n (%) |
| Gender | Female | 208,789 (67.41) |
| Male | 96,182 (31.0) | |
| Not known | 4,804 (1.6) | |
| Age group | ≤17 years | 17,345 (5.6) |
| 18–44 years | 125,501 (40.5) | |
| 45–64 years | 80,167 (25.9) | |
| ≥65 years | 52,314 (16.9) | |
| Unknown | 34,448 (11.1) | |
| Region | European Region | 171,805 (55.5) |
| Region of the Americas | 94,076 (30.4) | |
| Western Pacific Region | 31,452 (10.2) | |
| African Region | 830 (0.3) | |
| Eastern Mediterranean | 1,361 (0.4) | |
| South-East Asian | 10,251 (3.3) |
| SSRI Name | ICSR Reports (Raw Data) | Drug-Event Combination |
| Fluoxetine | 82760 | 4879 |
| Citalopram | 41205 | 4170 |
| Escitalopram | 43557 | 4501 |
| Fluvoxamine | 11056 | 1739 |
| Sertraline | 88298 | 5597 |
| Paroxetine | 75625 | 4808 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmacovigilance and Adverse Drug Reactions · Treatment of Major Depression · Electroconvulsive Therapy Studies
Introduction
Selective serotonin reuptake inhibitors (SSRIs) are commonly used as first-line antidepressant medications worldwide and are widely utilized to treat depressive and anxiety disorders. While their efficacy is well established, adverse events (AEs) are frequently reported, contributing to treatment discontinuation in both randomized trials and real-world practice [1]. These AEs often vary in their temporal presentation, with some emerging early in treatment (e.g., gastrointestinal symptoms, activation, insomnia) and others manifesting later (e.g., weight gain, sexual dysfunction) [2,3]. Understanding the timing and characteristics of these AEs is therefore critical for optimizing clinical management and improving patient outcomes.
Existing AE data from patients receiving SSRIs are obtained primarily from controlled settings of randomized trials, where sample sizes and follow-up durations are limited, and patients are identified based on stringent inclusion and exclusion criteria that are not representative of real-world clinical populations. Additionally, although some studies and/or surveys have been conducted in a real-world setting that attempt to further understand the nature and temporal characteristics of AEs associated with SSRI therapy [3,4], these studies are also often limited by their small sample sizes and limited follow-up duration. Hence, there exist substantial gaps in our knowledge regarding the temporal characteristics and real-world safety profile of SSRI agents.
To address this gap, this study leverages cumulative AE data from VigiBase for six commonly prescribed SSRIs (sertraline, fluoxetine, fluvoxamine, paroxetine, citalopram, and escitalopram) to systematically examine the time-to-onset (TTO) of these AEs. VigiBase is the World Health Organization (WHO) global database of individual case safety reports (ICSRs), which is based on a large cohort of patients globally and provides a comprehensive and globally representative perspective on the real-world safety profiles of SSRIs.
This study aims to characterize the median TTO and clinical profile of SSRI-associated AEs, identify temporal patterns in AE emergence, and provide evidence-based guidance for clinicians to personalize monitoring and improve patient counseling. These findings may support more informed decision-making and enhance adherence by anticipating and managing adverse effects throughout the course of treatment.
Materials and methods
Data source
This observational study utilized ICSRs from VigiBase, the WHO's global pharmacovigilance database maintained by the Uppsala Monitoring Centre (UMC). VigiBase is the largest international repository of spontaneous adverse drug reaction (ADR) reports, aggregating submissions from healthcare professionals, patients, and regulatory authorities across more than 130 countries [5]. Its extensive geographic coverage and long-standing operation provide a unique opportunity to examine real-world safety profiles of widely used pharmacological agents, including SSRIs.
SSRIs represent the most commonly prescribed class of antidepressants globally and are extensively used across diverse age groups and clinical settings in both high- and low-income countries [6,7]. However, because VigiBase relies on spontaneous reporting, the frequency of reported AEs does not reflect true incidence. Reporting is influenced by multiple factors, including prescribing volume, reporter awareness, perceived seriousness of events, regulatory activity, and media or scientific attention. It is well established that spontaneous reporting systems capture only a small fraction of actual AEs, with under-reporting estimates commonly ranging from approximately 1% to 10% of true events across pharmacovigilance systems worldwide [6,7]. Consequently, AE data in VigiBase should be interpreted as indicators of reporting patterns and temporal associations rather than absolute risk estimates. All AEs were coded using the Medical Dictionary for Regulatory Activities (MedDRA) Preferred Terms (PTs), ensuring standardized terminology and consistency across reports.
We focused on ICSRs involving six SSRIs: sertraline, fluoxetine, fluvoxamine, paroxetine, citalopram, and escitalopram, which are among the most frequently prescribed antidepressants in clinical practice. SSRIs account for the majority of antidepressant prescriptions worldwide across diverse populations, and recent real-world prescribing data indicate high utilization of this class in both primary and specialist care settings [6,7].
Data preparation
A cumulative retrieval from Vigibase of all ICSRs reporting any of the six SSRIs listed above as suspect medications was implemented, with a data lock point of 08 June 2024. The ICSRs were then aggregated across six SSRIs into a unified dataset. Individual drug names were removed, considering all SSRIs as a single class. Reports were included irrespective of the documented causality assessment in VigiBase (i.e., reports were not limited to "certain," "probable," or "possible" designations according to WHO-UMC or Naranjo criteria). This approach reflects typical pharmacovigilance practices in large spontaneous reporting analyses, where individual causality assessments are not uniformly available and are often incomplete, and where inclusion of all suspect reports enables comprehensive characterization of AE patterns. However, reports lacking essential fields (e.g., drug start date or event onset date) were excluded during TTO calculation because accurate temporal information is necessary for time-to-onset analyses. AEs with negative TTO values or missing TTO information were excluded. If an ICSR reports more than one valid TTO value for a particular AE term (i.e., the same AE was reported with valid TTO values more than once in a single patient), then only the smallest/earliest valid TTO value is included for analysis (i.e., subsequent TTO values of an AE that recurred in the same patient were discarded). For each AE term in the unified dataset, the total count of valid TTO entries was calculated by summing across all SSRIs (e.g., if SSRI-1 reported six nausea events and SSRIs 2-6 reported 10 each, the combined count equals 56). After summation, event terms with fewer than or equal to 10 valid TTO observations were removed. The final dataset comprised 1,428 distinct event terms, and median TTO values for each event term were presented in the Appendices section. This data cleaning process reduced the dataset from the raw ICSR totals to a final analytical sample of 309,775 ICSRs with 1,428 distinct MedDRA Preferred Terms.
Inclusion criteria comprised all ICSRs in VigiBase that listed at least one of the six SSRIs (sertraline, fluoxetine, fluvoxamine, paroxetine, citalopram, or escitalopram) as a suspect drug and contained valid dates for both drug initiation and AE onset.
Exclusion criteria included reports lacking essential temporal information (missing drug start date or event onset date), reports yielding negative or implausible TTO values, duplicate records, and AE terms with ≤10 valid TTO observations after aggregation.
TTO calculation and classification
TTO was defined as the interval from the documented start of SSRI therapy to the onset of the AE, consistent with recent pharmacovigilance practice. Median TTO was used for each event term, given its robustness to skew and outliers in spontaneous reporting data. TTO classification schemes in the literature vary, with many studies evaluating early onset within 30 days and late onset over longer treatment durations. While no single universal cutoff exists, pragmatically classifying AEs as early (median TTO < 28 days) versus late (median TTO > 28 days) aligns with several recent pharmacovigilance analyses that use similar early/late demarcations (e.g., within the first month versus later treatment phases) and acknowledges both clinical treatment cycles and real-world monitoring practices [8]. It approximates one standard prescription cycle, aligns with typical follow-up intervals in antidepressant initiation studies, and represents a pragmatic midpoint between Hu et al.'s [3] 14-day definition of acute AEs and Bull et al.'s [4] 90-day discontinuation window.
Data analysis
All descriptive analyses were conducted at the MedDRA Preferred Term level. For each AE term, the total number of valid TTO observations, median TTO, and interquartile range (IQR) were calculated. Event terms were ranked according to median TTO to explore temporal patterns of SSRI-associated AEs. AEs were categorized as early- or late-onset based on the predefined median TTO threshold of 28 days. Frequencies of early- and late-onset events were summarized descriptively. No stratification by individual SSRI, dose, age, sex, or geographic region was performed, as such variables were incompletely reported in VigiBase and could introduce bias. Given the spontaneous and non-comparative nature of the data, no inferential statistical testing or risk estimation was conducted. Analyses were performed using R statistical software (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria). Due to the nature of pharmacovigilance data, no inferential comparisons (e.g., adjusted hazard ratios) were conducted; however, patterns of clinical interest were flagged for future hypothesis-driven studies.
Ethical considerations
Access to VigiBase was granted via formal application to the UMC, which governs data access in accordance with WHO pharmacovigilance policies. As the dataset consists entirely of de-identified, spontaneously reported safety data, no ethical approval was required. All analyses were conducted in compliance with WHO and UMC data security protocols and international best practices for pharmacovigilance research.
Results
A total of 309,775 ICSRs were included in the final dataset after data cleaning. Among these reports, there was a higher proportion of females (208,789, 67.4%) compared to males (96,182, 31.0%), while gender information was missing for 4,804 (1.6%) participants. The age distribution showed that the majority were adults (18-64 years; 125,501, 66.4%), followed by the elderly (≥ 65 years; 52,314, 16.9%). In terms of geographic representation, most case reports were from the European Region (171,805, 55.5%) and the Region of the Americas (94,076, 30.4%) (Table 1).
Figure 1 and Table 2 present the total number of ICSRs and unique drug-event combinations for each SSRI. Sertraline and fluoxetine had the highest ICSR counts, while fluvoxamine had the lowest. This trend aligns with global prescription patterns: fluoxetine (introduced in 1987) and sertraline (early 1990s) have been widely prescribed worldwide [9], whereas fluvoxamine's use remains indication-specific (primarily for obsessive-compulsive disorder and social anxiety disorder) and less common [10].
Total number of raw individual case safety reports (ICSRs) and unique drug-event combinations for each SSRI in the VigiBase dataset prior to application of inclusion criteria and data cleaning
After applying the data cleaning procedures described in the Methods section, the final analytical dataset comprised 309,775 ICSRs with a total of 1,428 MedDRA Preferred Terms. Of these 1428 events, median TTO values ranged from immediate (0 days) to markedly delayed (959.5 days); 515 events were late-onset events (i.e., median TTO > 28 days), while the remaining 913 events were early-onset events (median TTO ≤ 28 days). See the Appendices section for a complete list of these events and their median TTO values.
Early-onset AEs (Figure 2) were predominantly gastrointestinal, neurological, anticholinergic, or related to activation. Examples of such early-onset events include nausea, with a median TTO of just one day, followed by insomnia and headache, both appearing at two days. Agitation and dizziness also emerged early, with median TTOs of three and two days, respectively. Restlessness, anticholinergic syndrome, and dry mouth were similarly observed during the first two days of treatment, whereas fatigue occurred with a median TTO of four days.
Top early-onset adverse events (median TTO ≤ 28 days)
In contrast, late-onset AEs mainly encompassed metabolic and endocrine complications (Figure 3). Among the most clinically significant late-onset events was weight gain, with a median TTO of 31 days. Hyperhidrosis (increased sweating) appeared later, with a median TTO of 76.5 days, while more severe metabolic disturbances, such as diabetes mellitus, developed after a median of 151 days. Notably, osteoporosis was the latest-onset event, with a median TTO of 959.5 days.
Top late-onset adverse events (median TTO > 28 days)
Discussion
This study demonstrates clear and reproducible temporal patterns in AEs associated with SSRIs, with approximately two-thirds of reported events occurring within the first 28 days of treatment initiation and the remainder emerging later in the treatment course. Early-onset AEs were predominantly gastrointestinal, neurological, anticholinergic, or activation-related, whereas late-onset AEs were largely metabolic or endocrine in nature. This distinct temporal clustering observed in our dataset suggests that SSRI tolerability is dynamic and evolves over time, reflecting underlying pharmacodynamic mechanisms rather than uniform reporting behavior. While similar temporal frameworks have been explored in other antidepressant classes, the consistency and breadth of early-late separation observed here underscore a characteristic pattern associated with SSRIs.
In our analysis, early-onset AEs (median TTO <28 days) were dominated by gastrointestinal, neurological, anticholinergic, and activation-related symptoms, with nausea, insomnia, headache, dizziness, agitation, and restlessness among the most rapidly emerging events. These findings are consistent with clinical observations reported by Strawn et al. [2], who found that such symptoms tend to emerge early in treatment, especially in younger populations, and may subside with continued use. Recent pharmacovigilance studies utilizing the FDA Adverse Event Reporting System have corroborated these patterns, demonstrating that gastrointestinal and neurological symptoms constitute the most frequently reported early-onset AEs in real-world settings [11].
Importantly, sexual dysfunction was also categorized as an early-onset event in our study (median TTO: 16.5 days), corroborating results from Hu et al. [3], where nearly 70% of patients experiencing SSRI-associated sexual dysfunction reported symptom onset within the first two weeks of therapy. This finding aligns with prior literature indicating that sexual side effects may occur early in therapy and, in some contexts (e.g., dapoxetine use for premature ejaculation), are known to emerge acutely. Contemporary research has further highlighted the complexity of SSRI-induced sexual dysfunction, with studies demonstrating that sexual side effects can manifest within days of treatment initiation and may persist even after discontinuation, leading to the recognition of post-SSRI sexual dysfunction (PSSD) as a distinct clinical entity [12,13]. A recent Israeli cohort study estimated that approximately 2.3% of males treated with serotonergic antidepressants may develop persistent erectile dysfunction, emphasizing the clinical significance of early recognition and management [14].
Late-onset AEs in our study (median TTO >28 days) were primarily metabolic and endocrine disturbances, including weight gain, hyperhidrosis, diabetes mellitus, osteoporosis, and gynecomastia. These findings align with those of Strawn et al. [2] and Hu et al. [3], who reported delayed onset of metabolic effects, particularly weight gain, with the majority of cases occurring beyond the initial two-week period. A comprehensive pharmacovigilance analysis focusing specifically on SSRI-associated metabolic complications demonstrated that overweight and glucose/lipid metabolism abnormalities show distinct temporal patterns. While short-term SSRI use is often associated with mild weight loss, prolonged treatment can lead to gradual weight gain in a subset of patients, typically after four to six weeks, and metabolic syndrome developing over months to years of continuous therapy [11]. Notably, osteoporosis emerged as the most delayed AE (median TTO: 959.5 days), underscoring the need for vigilance in long-term SSRI users. This finding is supported by emerging evidence suggesting that chronic SSRI use may interfere with bone metabolism through serotonin receptor-mediated mechanisms, particularly in older adults [15].
The clinical implications of these findings are clinically meaningful. Early-onset AEs, although often transient, may impact adherence if not proactively addressed. Interventions such as gradual dose titration, temporary symptom-targeted adjunctive therapies, and pre-treatment counseling can improve tolerability and persistence [16,17]. Recent clinical guidelines emphasize the importance of structured patient education programs that address expected early-onset symptoms and provide practical management strategies to enhance treatment retention [18]. On the other hand, late-onset AEs, particularly metabolic and endocrine complications, necessitate longitudinal surveillance. Clinical strategies should include periodic monitoring of body mass index (BMI), fasting glucose, lipid profiles, and, where applicable, bone mineral density assessments. A systematic approach to long-term monitoring has been proposed, incorporating risk stratification based on patient demographics, concurrent medications, and baseline metabolic status [6]. Identifying at-risk patients early may help prevent escalation into clinically significant syndromes such as diabetes or osteoporosis.
Strengths of the study
A major strength of this study is the use of a large, globally representative pharmacovigilance dataset encompassing reports from over 130 countries. This breadth captures real-world SSRI use across diverse populations that are typically under-represented in randomized controlled trials. The large sample size enabled identification of robust temporal trends across a wide range of AEs, providing insights into both early- and late-onset toxicity patterns.
Limitations
These findings must be interpreted with caution, given the inherent limitations of spontaneous reporting data. VigiBase data primarily reflect spontaneous reporting patterns rather than true incidence or causal relationships, and the absolute number of reports is minimal compared to the global population receiving SSRI therapy. Several limitations of this study warrant consideration. First, data were derived from spontaneous reporting via VigiBase, which is subject to reporting bias, particularly underreporting of mild, self-limiting, or socially sensitive symptoms (e.g., sexual dysfunction). Recent methodological studies have demonstrated that spontaneous reporting systems capture only an estimated 1-10% of actual AEs, with sexual dysfunction being particularly underreported due to social stigma and patient reluctance to discuss such symptoms [7]. Second, confounding by indication may influence results; the underlying psychiatric conditions themselves (e.g., depression or anxiety) are known to be associated with systemic metabolic alterations, potentially mimicking or amplifying drug-related effects [19]. Third, the dataset lacked information on SSRI dose, duration of therapy, and treatment switching, limiting the ability to assess dose-response effects or pharmacodynamic relationships. Advanced pharmacovigilance methodologies are increasingly incorporating machine learning approaches to address these limitations and improve signal detection accuracy [20]. Fourth, VigiBase reports do not include standardized demographic or baseline clinical data, such as age, sex, comorbidity, or treatment indication. Consequently, subgroup differences in TTO could not be explored. Some AEs, such as gynecomastia or menstrual disorders, are sex-specific, whereas others (e.g., nausea, fatigue) are common to both sexes; treating them equivalently may obscure biological variation in onset timing.
Future research directions
To further clarify SSRI-related AE timing and risk, future studies should incorporate longitudinal cohort designs that prospectively track symptom onset, standardized AE reporting tools to enhance data comparability, and pharmacogenomics analyses to identify individual-level predictors of susceptibility to early- or late-onset toxicity. Recent advances in precision medicine have identified genetic polymorphisms in cytochrome P450 enzymes and serotonin transporter genes that may predict individual variation in SSRI tolerability and AE susceptibility [21,22]. Additionally, the integration of electronic health records with pharmacovigilance databases offers promising opportunities for real-world evidence generation and continuous safety monitoring [23,24]. These approaches would improve the precision of AE risk stratification and support personalized SSRI prescribing strategies.
Conclusions
This study identifies distinct temporal patterns of AEs associated with SSRIs, with the majority occurring early in treatment and a substantial proportion emerging later. Early-onset AEs were predominantly gastrointestinal, neurological, and activation-related, whereas late-onset events were mainly metabolic and endocrine in nature, including weight gain, diabetes mellitus, and osteoporosis. These findings highlight that SSRI-associated adverse effects evolve over time and differ meaningfully in their onset profiles. Recognizing these temporal patterns has important implications for patient counseling, expectation setting, and long-term treatment planning in individuals receiving SSRI therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Selective serotonin reuptake inhibitors Stat Pearls [Internet] Chu A Wadhwa R Treasure Island (FL)Stat Pearls Publishing 2025 https://www.ncbi.nlm.nih.gov/books/NBK 554406/32119293 · pubmed ↗
- 2Adverse effects of antidepressant medications and their management in children and adolescents Pharmacotherapy Strawn JR Mills JA Poweleit EA Ramsey LB Croarkin PE 6756904320233665168610.1002/phar.2767 PMC 10378577 · doi ↗ · pubmed ↗
- 3Incidence and duration of side effects and those rated as bothersome with selective serotonin reuptake inhibitor treatment for depression: patient report versus physician estimate J Clin Psychiatry Hu XH Bull SA Hunkeler EM 9599656520041529168510.4088/jcp.v 65n 0712 · doi ↗ · pubmed ↗
- 4Discontinuing or switching selective serotonin-reuptake inhibitors Ann Pharmacother Bull SA Hunkeler EM Lee JY 5785843620021191850210.1345/aph.1A 254 · doi ↗ · pubmed ↗
- 5Data-driven identification of adverse event reporting patterns for Japan in Vigi Base, the WHO global database of individual case safety reports Drug Saf Wakao R Taavola H Sandberg L 148714984220193155954210.1007/s 40264-019-00861-y PMC 6858382 · doi ↗ · pubmed ↗
- 6Global burden of antidepressant-associated seizures from 1967 to 2023: a comparative analysis of the international pharmacovigilance database J Affect Disord Cho H Lee K Wang SM 21522338120254018906510.1016/j.jad.2025.04.024 · doi ↗ · pubmed ↗
- 7Safety profile of selective serotonin reuptake inhibitors in real-world settings: a pharmacovigilance study based on the FDA Adverse Event Reporting System Ann Pharmacother Zhao Y Zhang Y Yang L Zhang K Li S 110511165820243840714710.1177/10600280241231116 · doi ↗ · pubmed ↗
- 8Neurological adverse events associated with antidepressants: a comprehensive 22-year analysis of the FDA adverse event reporting system Front Pharmacol Yu Q Yao J Li E 16442411620254082246010.3389/fphar.2025.1644241 PMC 12354350 · doi ↗ · pubmed ↗