Utility of the Charlson Comorbidity Index in the Preoperative Evaluation of Patients Undergoing Cardiac Surgery
Daniel Manzur-Sandoval, Monserrat Echeverria-Ortuño, Rodrigo Gopar-Nieto, Gustavo Rojas-Velasco

TL;DR
The study shows that the Charlson Comorbidity Index helps predict postoperative complications in cardiac surgery patients, improving preoperative planning.
Contribution
The study demonstrates the CCI's effectiveness in predicting specific complications in cardiac surgery patients.
Findings
Severe comorbidity is linked to higher rates of delirium, stroke, transfusion, and renal replacement therapy.
Logistic regression identified delirium, pneumonia, acute kidney injury, and renal replacement therapy as independent predictors of severe comorbidity.
Higher CCI scores correlate with increased Sequential Organ Failure Assessment scores post-surgery.
Abstract
The Charlson Comorbidity Index (CCI) is used for assessing comorbidities and estimating risk of adverse outcomes in surgical patients. In cardiac surgery, the burden of comorbidities can significantly influence incidence of postoperative complications and mortality. This study evaluates the utility of CCI in predicting perioperative complications in patients undergoing cardiac surgery. Observational cross-sectional study with retrospective data including 483 adult patients who underwent cardiac surgery with cardiopulmonary bypass at the Instituto Nacional de Cardiología Ignacio Chávez from June 2022 to December 2023. Patients were grouped by preoperative CCI: mild (0 - 1), moderate (2), and severe (≥ 3). Statistical analyses (chi-square, Mann-Whitney U, logistic regression) assessed the association between CCI and postoperative complications, adjusting for age and sex. Patients with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
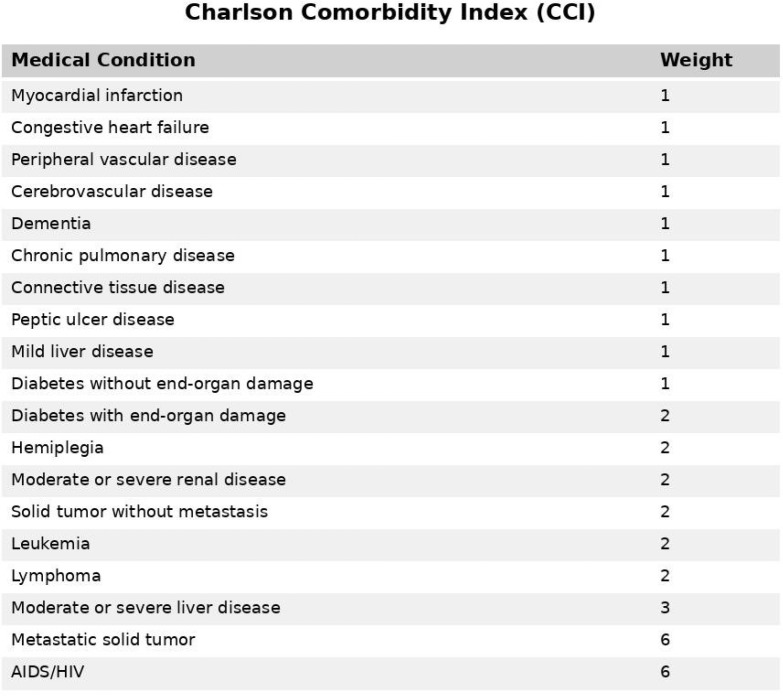 Figure 1
Figure 1| Abbreviations, Acronyms & Symbols | ||||
|---|---|---|---|---|
| AIDS | = Acquired immunodeficiency syndrome | HIV | = Human immunodeficiency virus | |
| CABG | = Coronary artery bypass grafting | ICU | = Intensive care unit | |
| CCI | = Charlson Comorbidity Index | IQR | = Interquartile range | |
| CI | = Confidence interval | NYHA | = New York Heart Association | |
| CKD | = Chronic kidney disease | OR | = Odds ratio | |
| COPD | = Chronic obstructive pulmonary disease | SOFA | = Sequential Organ Failure Assessment | |
| EuroSCORE | = European System for Cardiac Operative Risk Evaluation | STS | = Society of Thoracic Surgeons | |
| Variable | Total | Group 1 | Group 2 | Group 3 | ||
|---|---|---|---|---|---|---|
| Women, n (%) | 207 (42.9) | 173 (43.8) | 21 (38.2) | 13 (39.4) | 0.67 | |
| Men, n (%) | 276 (57.1) | 222 (56.2) | 34 (61.8) | 20 (60.6) | ||
| Hypertension, n (%) | 213 (44.1) | 160 (40.5) | 32 (58.2) | 21 (63.6) | < 0.001 | |
| Diabetes, n (%) | 120 (24.8) | 74 (18.7) | 23 (41.8) | 23 (69.7) | < 0.001 | |
| Diabetes with target organ damage, n (%) | 31 (6.4) | 0 | 9 (16.4) | 22 (66.7) | 0.00 | |
| Moderate to severe chronic kidney disease, n (%) | 36 (7.4) | 5 (1.3) | 11 (20) | 20 (60.6) | 0.00 | |
| Chronic obstructive pulmonary disease, n (%) | 18 (3.7) | 5 (1.3) | 7 (12.7) | 6 (18.2) | < 0.001 | |
| Hypothyroidism, n (%) | 71 (14.7) | 58 (14.7) | 7 (12.7) | 6 (18.2) | 0.78 | |
| Previous myocardial infarction, n (%) | 54 (11.2) | 30 (7.6) | 12 (21.8) | 12 (36.4) | < 0.001 | |
| Heart failure, n (%) | 128 (26.5) | 88 (22.3) | 27 (49.1) | 13 (39.4) | < 0.001 | |
| Atrial fibrillation, n (%) | 101 (20.9) | 80 (20.2) | 11 (20) | 10 (30.3) | 0.38 | |
| Stroke, n (%) | 47 (9.7) | 21 (5.3) | 13 (23.6) | 13 (39.4) | < 0.001 | |
| Hemiplegia, n (%) | 20 (4.1) | 0 | 8 (14.5) | 12 (36.4) | < 0.001 | |
| Previous cardiac surgery, n (%) | 52 (10.8) | 41 (10.4) | 8 (14.5) | 3 (9.1) | 0.61 | |
| Peripheral vascular disease, n (%) | 38 (7.9) | 20 (5.1) | 11 (20) | 7 (21.2) | < 0.001 | |
| Connective tissue disease, n (%) | 28 (5.8) | 16 (4) | 7 (12.7) | 5 (15.1) | < 0.001 | |
| Peptic ulcer disease, n (%) | 29 (6) | 15 (3.8) | 7 (12.7) | 7 (21.2) | < 0.001 | |
| Moderate to severe liver disease, n (%) | 5 (1) | 0 | 2 (3.6) | 3 (9.1) | < 0.001 | |
| Mild liver disease, n (%) | 6 (1.2) | 1 (0.2) | 1 (1.8) | 4 (12.1) | < 0.001 | |
| Solid tumor, n (%) | 13 (2.7) | 5 (1.3) | 5 (9.1) | 3 (9.1) | < 0.001 | |
| NYHA functional class, n (%) | I | 65 (13.5) | 54 (13.7) | 5 (9.1) | 6 (18.2) | 0.04 |
| II | 296 (61.3) | 248 (62.8) | 27 (49.1) | 21 (63.6) | ||
| III | 109 (22.6) | 85 (21.5) | 20 (36.4) | 4 (12.1) | ||
| IV | 13 (2.7) | 8 (2) | 3 (5.4) | 2 (6.1) | ||
| Age (years), median (IQR) | 57 (45 - 65) | 56 (44 - 65) | 60 (51-67) | 62 (54 - 66) | < 0.001 | |
| Weight (kg), median (IQR) | 68.5 (60 - 78) | 68.8 (60 - 78) | 66 (59-77) | 73 (60 - 80) | 0.49 | |
| Height (m), median (IQR) | 1.62 (1.55 - 1.7) | 1.62 (1.55 - 1.7) | 1.62 (1.55-1.7) | 1.63 (1.57 - 1.68) | 0.95 | |
| Body mass index (kg/m2), median (IQR) | 26.1 (23.4 - 28.9) | 26 (23.3 - 28.8) | 26.4 (23.6-29.3) | 26.4 (23.6 - 29) | 0.72 | |
| Variable | Total | Group 1 | Group 2 | Group 3 | |
|---|---|---|---|---|---|
| Aortic valve replacement, n (%) | 142 (29.4) | 124 (31.4) | 11 (20) | 7 (21.2) | 0.12 |
| Coronary artery bypass grafting, n (%) | 75 (15.5) | 51 (12.9) | 13 (23.6) | 11 (33.3) | < 0.001 |
| Mitral valve replacement, n (%) | 46 (9.5) | 38 (9.6) | 6 (10.9) | 2 (6.1) | 0.74 |
| Mitral valve replacement + tricuspid valve replacement, n (%) | 26 (5.4) | 19 (4.8) | 4 (7.3) | 3 (9.1) | 0.46 |
| Aortic valve replacement + mitral valve replacement, n (%) | 31 (6.4) | 27 (6.8) | 3 (5.4) | 1 (3) | 0.87 |
| CABG + aortic valve replacement, n (%) | 20 (4.1) | 17 (4.3) | 2 (3.6) | 1 (3) | 1 |
| Bentall-De Bono procedure, n (%) | 25 (5.2) | 23 (5.8) | 2 (3.6) | 0 | 0.39 |
| Other surgeries, n (%) | 121 (25) | 97 (24.6) | 15 (27.3) | 9 (27.3) | 0.82 |
| Cardiopulmonary bypass time (minutes), median (IQR) | 144 (112 - 186) | 143 (113 - 187) | 149 (105 - 208) | 140 (97 - 175) | 0.50 |
| Aortic cross-clamping time (minutes), median (IQR) | 100 (76 - 125) | 101 (77 - 124) | 98 (75 - 134) | 87 (65 - 113) | 0.26 |
| EuroSCORE (%), median (IQR) | 1.8 (1 - 3.4) | 1.6 (0.9 - 3.2) | 2.2 (1.5 - 4.9) | 2.5 (1.5 - 6.9) | < 0.001 |
| STS score (%), median (IQR) | 0.9 (0.5 - 1.7) | 0.8 (0 - 1) | 1.1 (0.9 - 1.4) | 1.3 (1 - 1.6) | < 0.001 |
| Variable | Total | Group 1 | Group 2 | Group 3 | |
|---|---|---|---|---|---|
| n = 483 | n = 395 | n = 55 | n = 33 | ||
| Mediastinal hemorrhage, n (%) | 56 (11.6) | 46 (11.6) | 5 (9.1) | 5 (15.1) | 0.68 |
| Low cardiac output syndrome, n (%) | 59 (12.2) | 47 (11.9) | 7 (12.7) | 5 (15.1) | 0.85 |
| Vasoplegic syndrome, n (%) | 33 (6.8) | 27 (6.8) | 2 (3.6) | 4 (12.1) | 0.35 |
| Hypovolemia, n (%) | 184 (38.1) | 151 (38.2) | 18 (32.7) | 15 (45.4) | 0.48 |
| Delirium, n (%) | 57 (11.8) | 37 (9.4) | 11 (20) | 9 (27.3) | < 0.001 |
| Stroke, n (%) | 18 (3.7) | 11 (2.8) | 5 (9.1) | 2 (6.1) | 0.03 |
| In-hospital pneumonia, n (%) | 50 (10.4) | 35 (8.9) | 7 (12.7) | 8 (2.42) | 0.01 |
| Mediastinitis, n (%) | 21 (4.4) | 15 (3.8) | 4 (7.3) | 2 (6.1) | 0.32 |
| Transfusion, n (%) | 235 (48.8) | 186 (47.2) | 26 (47.3) | 23 (69.7) | 0.04 |
| Acute kidney injury, n (%) | 147 (30.5) | 116 (29.4) | 15 (27.3) | 16 (48.5) | 0.06 |
| Renal replacement therapy, n (%) | 29 (6) | 21 (5.3) | 2 (3.6) | 6 (18.2) | 0.02 |
| Hepatic dysfunction, n (%) | 61 (12.7) | 56 (14.2) | 4 (7.3) | 1 (3) | 0.08 |
| Postoperative atrial fibrillation, n (%) | 76 (15.8) | 60 (15.2) | 10 (18.2) | 6 (18.2) | 0.79 |
| In-hospital mortality, n (%) | 28 (5.8) | 22 (5.6) | 3 (5.4) | 3 (9.1) | 0.63 |
| Postoperative ICU stay (days), median (IQR) | 3 (2 - 4) | 3 (2 - 4) | 2 (2 - 4) | 3 (2 - 5) | 0.19 |
| Days on mechanical ventilation, median (IQR) | 1 (1 - 1) | 1 (1 - 1) | 1 (1 - 1) | 1 (1 - 2) | 0.55 |
| Hospital length of stay (days), median (IQR) | 10 (7 - 17) | 9 (7 - 16) | 12 (7 - 21) | 11 (7 - 21) | 0.09 |
| SOFA score 24 hours, median (IQR) | 5 (3 - 7) | 5 (3 - 7) | 4 (3 - 7) | 7 (4 - 8) | < 0.001 |
| SOFA score 72 hours, median (IQR) | 3 (2 - 5) | 3 (2 - 5) | 4 (2 - 6) | 4 (2 - 7) | 0.05 |
| Variable | OR | 95% CI | |
|---|---|---|---|
| Delirium | 3.13 | 1.37 - 7.13 | < 0.001 |
| In-hospital pneumonia | 3.10 | 1.31 - 7.30 | 0.01 |
| Acute kidney injury | 2.28 | 1.12 - 4.65 | 0.02 |
| Renal replacement therapy | 4.10 | 1.54 - 10.93 | < 0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac, Anesthesia and Surgical Outcomes · Sepsis Diagnosis and Treatment · Frailty in Older Adults
INTRODUCTION
**: **
The Charlson Comorbidity Index (CCI), developed in 1987 by Mary Charlson et al., has become a fundamental tool for assessing comorbidities in internal medicine. It classifies 17 medical conditions, each assigned a weighted score based on its severity and association with mortality (Figure 1). These conditions range from cardiovascular diseases to malignancies, and the cumulative score is used to predict clinical outcomes and inform therapeutic decision-making^[1]^. The significance of the CCI lies in its ability to provide a comprehensive assessment of a patient’s overall health status, which is particularly relevant in surgical settings, where comorbidities can substantially impact outcomes.
Fig. 1. List of medical conditions included in the Charlson Comorbidity Index (CCI), along with their respective weights. AIDS=acquired immunodeficiency syndrome; HIV=human immunodeficiency virus.
Importance
The CCI has been validated as a predictor of mortality in diverse patient populations and has become an indispensable tool for risk stratification. Multiple studies show that higher CCI scores are strongly associated with increased postoperative morbidity and long term mortality^[2,3]^. This finding is especially relevant in cardiac surgery, where patients frequently present with several coexisting conditions that complicate perioperative care. Incorporating CCI into routine practice enables clinicians to identify high risk patients who may benefit from intensified monitoring and individualized therapeutic strategies. By accounting for the burden of comorbidities, clinicians can tailor interventions to maximize effectiveness while minimizing adverse effects. Moreover, using CCI at the bedside helps anticipate complications and implement timely preventive measures, thereby improving outcomes^[4,5]^.
Non cardiovascular comorbidities - including diabetes mellitus, peripheral vascular disease, chronic obstructive pulmonary disease (COPD), and chronic kidney disease (CKD) - have a pronounced impact on both short and long term results after cardiac surgery, particularly coronary artery bypass grafting (CABG). In a large contemporary cohort, diabetes was present in nearly 30% of CABG recipients, peripheral vascular disease in 16%, COPD in 18.6%, and renal dysfunction in 27.5%^[6]^. These conditions correlate with advanced age, higher rates of postoperative complications, and reduced access to post discharge interventions such as cardiac rehabilitation, all of which contributing to poorer prognoses. Quantifying this comorbidity burden with the CCI provides a more comprehensive risk profile than traditional cardiovascular risk scores alone.
Objective
The primary objective of this study is to analyze the utility of CCI in the preoperative setting of cardiac surgery. The study aims to evaluate how the CCI score correlates with postoperative complication rates, mortality, and length of hospital stay. Through an analytical approach, it seeks to determine the predictive capacity of CCI for adverse outcomes in patients undergoing cardiac surgical procedures. Additionally, the study aims to establish recommendations regarding the use of CCI in clinical practice to improve decision-making and perioperative management of at-risk patients. This research will contribute not only to the existing literature on comorbidity assessment in cardiac surgery but also to providing healthcare professionals with practical tools to optimize patient care, ensuring a more comprehensive and safer surgical approach. Given the increasing complexity of patient health profiles, CCI remains a cornerstone in the evaluation and management of comorbidities in the surgical setting.
METHODS
The study was an analytical observational investigation with retrospective data collection and a cross-sectional design. An open-label approach was employed, with evaluators not blinded to patient information. The sample included adult patients (≥ 18 years) of any sex who underwent cardiac surgery with cardiopulmonary bypass at the Instituto Nacional de Cardiología Ignacio Chávez. A non-probabilistic sampling method was applied, enrolling a total of 483 patients operated on between June 1^st^, 2022, and December 31^st^, 2023. Inclusion criteria were all adult patients undergoing cardiac surgery with cardiopulmonary bypass, without gender restriction. These criteria and sample size were selected to comprehensively represent the target population undergoing this specific surgical intervention during the study period. Patients who died intraoperatively or within the first 12 hours of intensive care unit (ICU) admission were excluded, as our ICU database is designed to capture hemodynamic parameters at 0, six, 12, and 24 hours. Early mortality is often due to unpredictable surgical complications (e.g., uncontrolled bleeding) unrelated to preoperative risk, and including such cases could bias the assessment of preoperative predictors. This exclusion ensured a more homogeneous cohort for risk analysis. Patients with incomplete medical records were also excluded from the study. Data were collected through a detailed review of electronic and physical medical records, as well as electronic imaging studies, to gather demographic, clinical, and surgical information, along with patient outcomes.
In the "other surgeries" group, which individually represented a small proportion of patients, the most frequent procedures included triple valve replacement, aortic surgery (other than Bentall-De Bono), tricuspid valve replacement, congenital heart disease surgery, heart transplantation, pulmonary thromboendarterectomy, endoventricular remodeling, and post-infarction ventricular septal defect closure.
Patients were classified according to their preoperative CCI into three groups consistent with prior studies^[7,8]^:
• Grupo 1: 0 - 1 point, indicating mild comorbidity;• Group 2: 2 points, considered moderate comorbidity;• Group 3: ≥ 3 points, indicating severe comorbidity.
For statistical analysis, the normality of continuous variables was assessed using the Shapiro-Wilk test. Parametric variables are presented as mean ± standard deviation, whereas non-parametric variables are reported as median and interquartile range (IQR). Comparisons of continuous variables were performed using the Mann-Whitney U test. Categorical variables were summarized using frequencies and percentages, and comparisons were made using the chi-square test or Fisher’s exact test, depending on expected cell counts. A logistic regression model adjusted for age, sex, and CABG surgery was developed to identify predictors of adverse events. Statistical significance was set at P < 0.05 for all analyses, which were conducted using STATA version 14.
Ethics Approval and Consent to Participate
Local institutional research and ethics committees waived the requirement for approval for this study. Informed consent was obtained from all participants prior to inclusion.
Consent for Publication
Written informed consent for the publication of patient information and images was obtained either from the patient or a legally authorized representative.
RESULTS
Baseline Characteristics
A total of 483 patients were classified by comorbidity severity into mild (n = 395), moderate (n = 55), and severe (n = 33) groups. Arterial hypertension prevalence was higher in moderate (58.2%) and severe (63.6%) groups (P = 0.00). Diabetes mellitus was more frequent in moderate (41.8%) and severe (69.7%) groups (P = 0.00), with target organ damage present in 66.7% of severe cases (P = 0.00). CKD was observed in 2.5% of mild and 57.6% of severe patients (P = 0.00), with moderate-to-severe stages in 60.6% of the severe group (P = 0.00). Previous myocardial infarction affected 36.4% of severe vs. 7.6% of mild patients (P = 0.00). Heart failure and cerebrovascular disease were also significantly more prevalent in the severe group (49.1% vs. 22.3% and 39.4% vs. 5.3%, respectively; P = 0.00). Median age was 57 years (IQR 45 - 65), with 76.6% aged 41 - 70 years (Table 1).
Surgical Characteristics
Aortic valve replacement was performed in 29.4% of patients, with no significant differences between groups (P = 0.12). CABG was performed in 15.5% of patients and was more frequent in the moderate (23.6%) and severe (33.3%) comorbidity groups compared to the mild group (12.9%) (P < 0.001). Mitral valve replacement was performed in 9.5% of patients, with no significant differences between groups (P = 0.74). The European System for Cardiac Operative Risk Evaluation (EuroSCORE) had a median value of 1.8 (IQR: 1-3.4), with significant increases observed in the moderate (2.2) and severe (2.5) groups (P < 0.001). The median cardiopulmonary bypass time was 144 minutes (IQR: 112 - 186), with no significant differences between groups (P = 0.50). Similarly, the median aortic cross-clamping time was 100 minutes (IQR: 76 - 125), also showing no significant differences (P = 0.26) (Table 2).
Postoperative Complications
A higher incidence of postoperative complications was observed in the severe comorbidity group. Delirium occurred in 27.3% of patients with severe comorbidities compared to 9.4% in the mild group (P = 0.00). Stroke was more frequent in the moderate (9.1%) and severe (6.1%) groups than in the mild group (2.8%) (P = 0.03). Hospital-acquired pneumonia affected 12.7% of patients in the moderate group vs. 8.9% in the mild group (P = 0.01). Transfusion rates were significantly higher in the severe group (69.7%) compared to the mild group (47.2%) (P = 0.04). Renal replacement therapy was more common in the severe group (18.2%) than in the mild group (5.3%) (P = 0.02). The median Sequential Organ Failure Assessment score at 24 hours was higher in the severe group (7 [IQR 4-8]) compared to the mild group (5 [IQR 3-7]) (P = 0.00), with a trend toward higher scores at 72 hours (P = 0.05). Although acute kidney injury was more frequent in the severe group (48.5%) than in the mild group (29.4%), this difference did not reach statistical significance (P = 0.06). No significant differences were found in mediastinal hemorrhage, low cardiac output syndrome, vasoplegic syndrome, hypovolemia, mediastinitis, hepatic dysfunction, postoperative atrial fibrillation, in-hospital mortality, ICU stay, mechanical ventilation duration, or total hospital length of stay (Table 3).
Logistic Regression Analysis
Logistic regression analyses were conducted to identify factors associated with severe comorbidity, adjusting for age, sex, and CABG surgery. Due to the statistically significant difference in CABG distribution across comorbidity groups (33.3% in the severe group vs. 12.9% in the mild group; P < 0.001), CABG was included as a covariate in the multivariable logistic regression model to control for potential confounding. Postoperative delirium (odds ratio [OR]: 3.13; 95% confidence interval [CI]: 1.37 - 7.13; P = 0.001) and nosocomial pneumonia (OR: 3.10; 95% CI: 1.31 - 7.30; P = 0.01) were significantly associated with an increased risk of severe comorbidity. Acute kidney injury also showed a significant association (OR: 2.28; 95% CI: 1.12 - 4.65; P = 0.02). Renal replacement therapy was associated with the highest odds ratio (OR: 4.10; 95% CI: 1.54 - 10.93; P < 0.001), indicating a more than fourfold increased risk (Table 4).
DISCUSSION
This study highlights the importance of CCI as a key tool in the preoperative assessment of patients undergoing cardiac surgery, particularly when compared with more commonly used risk scores such as EuroSCORE and the Society of Thoracic Surgeons (STS) score. Our results suggest that the CCI could have a significant impact on predicting postoperative complications by incorporating a broad spectrum of comorbidities, not limited to cardiac conditions alone. The high prevalence of diseases such as hypertension and diabetes in our cohort underscores the need to integrate tools that assess the risk associated with these comorbidities, which are crucial for effective preoperative management.
Regarding the performance of conventional risk scores, previous studies have shown that both EuroSCORE and STS score have limited discriminatory power in certain populations. Nilsson et al.^[9]^ reported that EuroSCORE is among the scores with the greatest discriminatory ability in cardiac surgery, closely followed by the Cleveland Clinic score and the Magovern score. Despite their widespread acceptance, these tools may not be sufficient to optimally predict postoperative outcomes in patients with multiple comorbidities. The CCI, by accounting for comorbidities beyond cardiovascular diseases, could offer a more robust prediction, particularly in patients with multiple chronic conditions. It is important to emphasize that, although EuroSCORE and STS score are more specific to cardiovascular procedures, their performance is limited in patients with significant non-cardiac comorbidities, as reflected in our study’s findings. For example, the incidence of severe complications such as delirium and acute kidney injury was higher in patients with elevated CCI scores - outcomes that are not always adequately captured by traditional scores.
The application of CCI could potentially reduce the rates of these severe complications, which substantially increase the costs associated with postoperative care. Moreover, improved prediction of complications would allow for optimized resource allocation and more efficient tailoring of interventions, potentially enhancing survival and reducing long-term healthcare costs in patients with multiple chronic conditions^[10-14]^. Our findings suggest that CCI may offer an advantage in clinical settings where patients present with multiple comorbidities. By integrating a broader evaluation of overall patient health status, CCI could enable more precise personalization of perioperative care, tailoring management strategies according to the specific risks each patient faces, including those from conditions beyond the cardiovascular system.
Limitations
This study has several inherent limitations. Firstly, its retrospective design introduces potential selection and recording biases. Additionally, the absence of follow-up data limits the ability to evaluate the temporal progression of patients. While associations between variables can be identified in this type of study, causal relationships cannot be established. Furthermore, as a single-center study, the findings may not be generalizable to other populations or settings.
CONCLUSION
The CCI has proven to be a valuable tool for predicting complications in patients undergoing cardiac surgery. Early identification of comorbidities can guide clinical decision-making and improve patient outcomes. It is essential for healthcare professionals to incorporate comorbidity assessment into the surgical care process, as this not only enhances the quality of care but also positively influences survival and quality of life in this patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stavem K Hoel H Skjaker SA Haagensen R. Charlson comorbidity index derived from chart review or administrative data: agreement and prediction of mortality in intensive care patients Clin Epidemiol 2017931132010.2147/CLEP.S 133624.28652813 PMC 5476439 · doi ↗ · pubmed ↗
- 2Manlhiot C Rao V Rubin B Lee DS. Comparison of cardiac surgery mortality reports using administrative and clinical data sources: a prospective cohort study CMAJ Open 201863 E 3162110.9778/cmajo.20180072.PMC 618211830181346 · doi ↗ · pubmed ↗
- 3Klevens RM Edwards JR Richards CL Jr, Horan TC Gaynes RP Pollock DA Estimating health care-associated infections and deaths in U.S. hospitals, 2002 Public Health Rep 2007122216016610.1177/003335490712200205.17357358 PMC 1820440 · doi ↗ · pubmed ↗
- 4Ho MH Nealon J Igwe E Traynor V Chang HR Chen KH Postoperative delirium in older patients: a systematic review of assessment and incidence of postoperative deliriumworldviews evid based nurs 202118529030110.1111/wvn.12536.34482593 · doi ↗ · pubmed ↗
- 5Boockvar KS Judon KM Eimicke JP Teresi JA Inouye SK. Hospital elder life program in long-term care (HELP-LTC): a cluster randomized controlled trial J Am Geriatr Soc 202068102329233510.1111/jgs.16695.32710658 PMC 7718417 · doi ↗ · pubmed ↗
- 6Scrutinio D Giannuzzi P. Comorbidity in patients undergoing coronary artery bypass graft surgery: impact on outcome and implications for cardiac rehabilitation Eur J Cardiovasc Prev Rehabil 200815437938510.1097/HJR.0b 013e 3282 fd 5c 6f.18677160 · doi ↗ · pubmed ↗
- 7Núñez JE Núñez E Fácila L Bertomeu V Llàcer A BodíV Papel del índice de Charlson en el pronóstico a 30 días y 1 año tras un infarto agudo de miocárdio Rev Esp Cardiol 200457984284915373990 · pubmed ↗
- 8Rius C Pérez G Martínez JM Bares M Schiaffino A Gispert R An adaptation of Charlson comorbidity index predicted subsequent mortality in a health survey J Clin Epidemiol 200457440340810.1016/j.jclinepi.2003.09.016.Erratum in: J Clin Epidemiol. 2007;60(6):643.15135843 · doi ↗ · pubmed ↗