Giant splenic artery pseudoaneurysm fistulizing to the colon: A case report and focused literature review
Tom Simon, Nicolas Brassart

TL;DR
A rare case of a large splenic artery pseudoaneurysm that ruptured into the colon is reported, emphasizing the need for early surgery to avoid severe complications.
Contribution
This case report adds to the limited literature on splenic artery pseudoaneurysm fistulas and advocates for early surgical intervention.
Findings
A 73-year-old woman had a giant splenic artery pseudoaneurysm that fistulized into the colon, causing acute bleeding.
Initial embolization provided temporary control, but delayed surgery was needed to manage sepsis and organ complications.
The case review suggests embolization should be a temporary measure, with surgery required to prevent severe infection.
Abstract
Splenic artery pseudoaneurysm (SAP) is a rare but dangerous visceral arterial lesion, and fistulization into the gastrointestinal tract is an exceptional and life-threatening complication. We report the case of a 73-year-old woman presenting with acute lower gastrointestinal bleeding caused by a giant SAP that had eroded into the splenic flexure of the colon. Proximal embolization using coils and Onyx achieved initial hemostasis. Although the patient was clinically stabilized, she later developed delayed septic and inflammatory complications requiring splenectomy, colonic resection, partial gastrectomy, and removal of the aneurysmal sac. This case, together with our focused review of published SAP fistula cases, highlights that embolization should be considered a temporizing measure when gastrointestinal fistulization is present; early surgical management remains essential to prevent…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
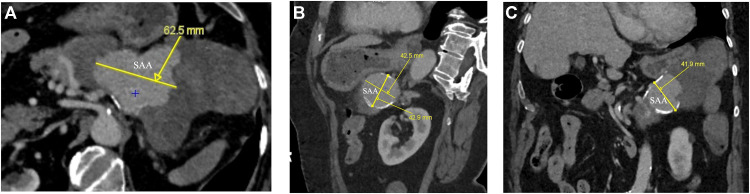 Figure 1
Figure 1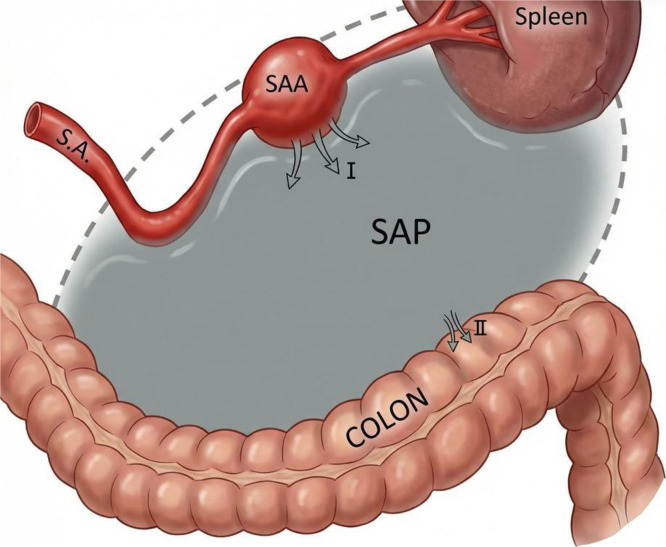 Figure 2
Figure 2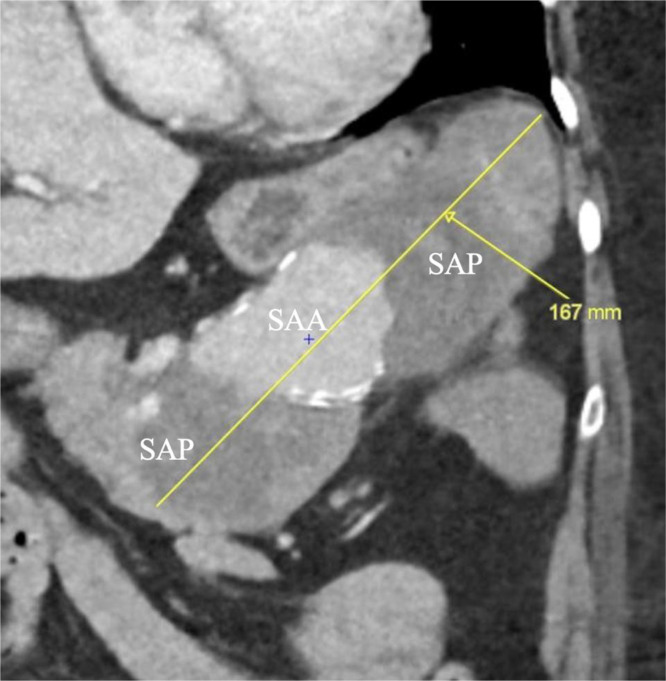 Figure 3
Figure 3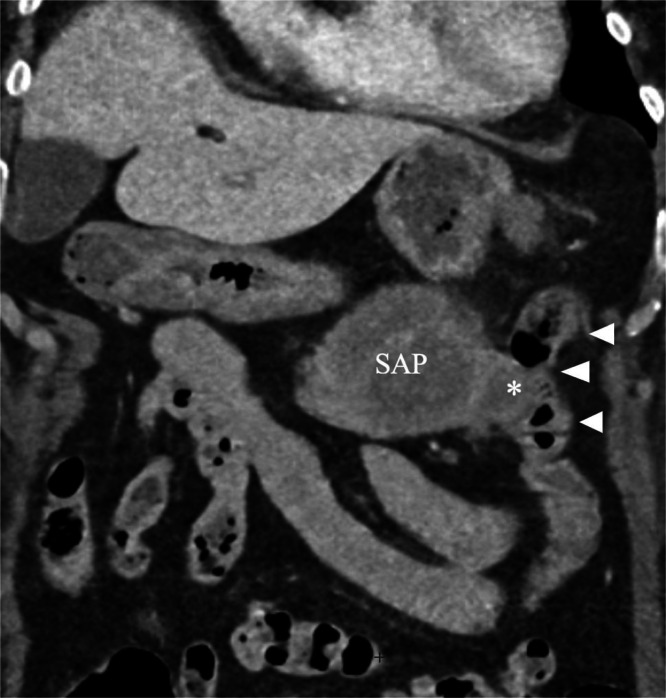 Figure 4
Figure 4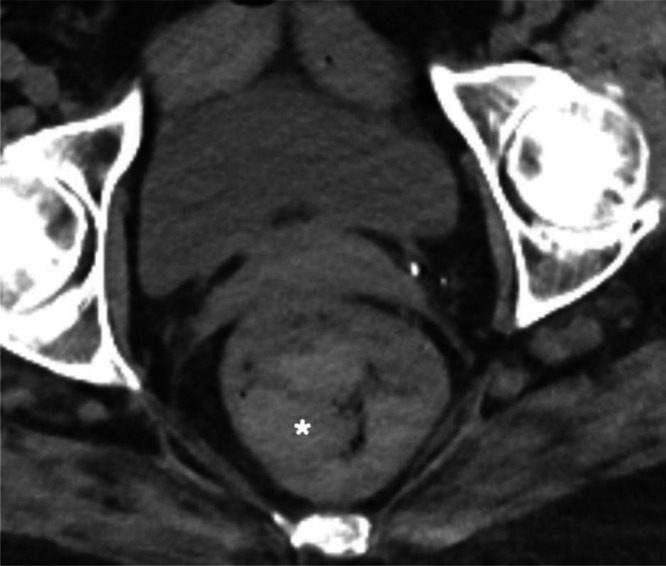 Figure 5
Figure 5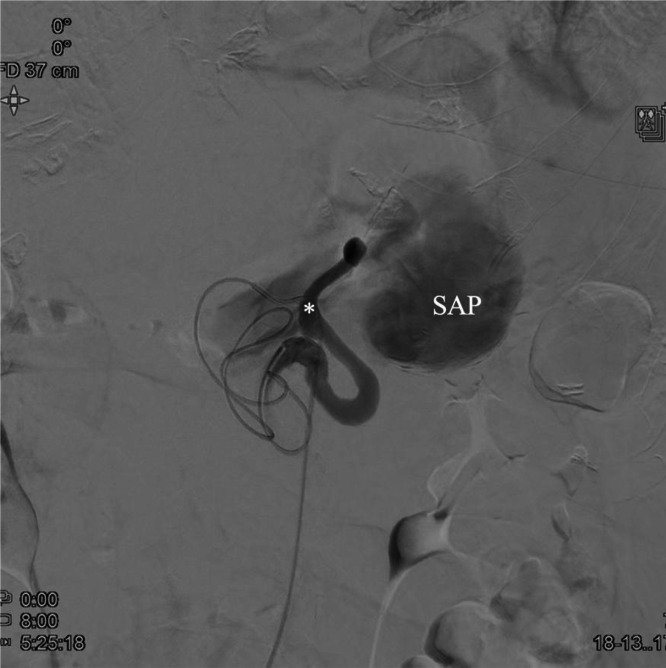 Figure 6
Figure 6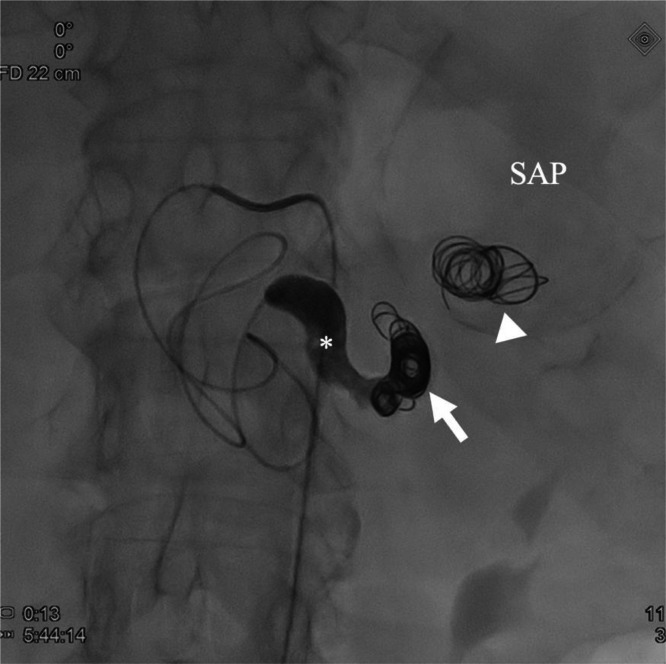 Figure 7
Figure 7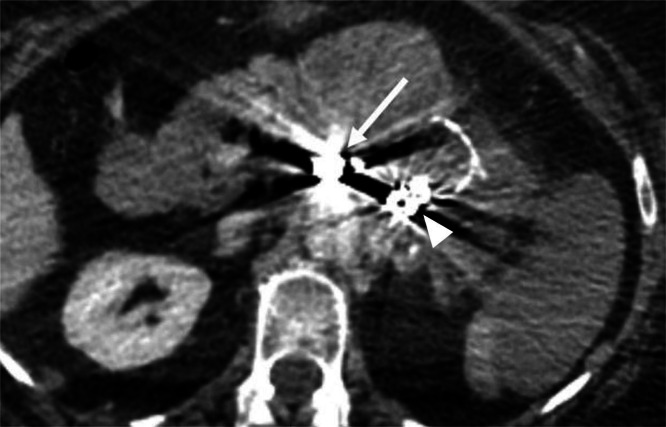 Figure 8
Figure 8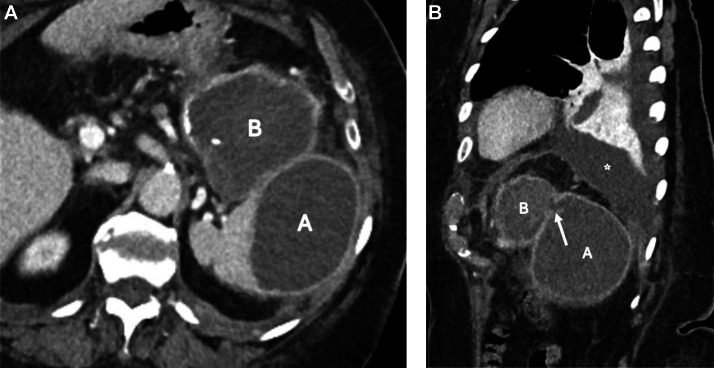 Figure 9
Figure 9 Figure 10
Figure 10Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Gastrointestinal Bleeding Diagnosis and Treatment · Abdominal Trauma and Injuries
Introduction
Splenic artery aneurysms (SAAs) are the third most common intra-abdominal aneurysms, but splenic artery pseudoaneurysms (SAPs) differ fundamentally because they lack a complete arterial wall and are far more prone to rupture [1]. SAPs most frequently arise from pancreatitis or inflammatory processes and may erode into adjacent organs. Gastrointestinal fistulization is extremely rare but may result in catastrophic bleeding [2]. Endovascular embolization is widely used as first-line management; however, in cases involving fistulization, its role as definitive therapy remains uncertain [1,3].
We present a case of a giant SAP fistulizing into the splenic flexure of the colon, initially stabilized by proximal embolization but complicated by delayed septic evolution requiring major surgery. A focused literature review is included to contextualize optimal management strategies.
Case presentation
A 73-year-old woman presented to the emergency room with massive rectal bleeding and abdominal pain. She also reported vomiting without hematemesis and had no prior episodes of rectal bleeding, trauma, vasculitis or history of pancreatitis.
Physical examination showed mild epigastric tenderness. At admission, the patient was hemodynamically stable with a blood pressure of 101/78 mmHg, a heart rate of 80 bpm, and an oxygen saturation of 90% on room air; amylase and lipase levels were normal.
An arterial- and venous-phase contrast-enhanced abdominal CT revealed a large saccular splenic artery aneurysm measuring approximately 42 × 43 × 62 mm (Fig. 1A-C). This lesion was surrounded by an oval-shaped mass containing dense hematic material, partially enhancing on delayed phases, consistent with a pseudoaneurysm measuring approximately 16.8 × 6.5 × 7.3 cm (Fig. 2). The lesion was in contact with the stomach, pancreatic tail, and splenic flexure of the colon, with imaging evidence of active fistulization into the splenic flexure (Figs. 3 and 4).Fig. 1(A) Contrast-enhanced computed tomography (CT), axial multiplanar reconstruction (MPR), demonstrating a large saccular splenic artery aneurysm (SAA), measuring 62 × 42 × 43 mm. (B) Contrast-enhanced CT, sagittal MPR, demonstrating a large saccular splenic artery aneurysm (SAA), measuring 62 × 42 × 43 mm. (C) Contrast-enhanced CT, coronal MPR, demonstrating a large saccular splenic artery aneurysm (SAA), measuring 62 × 42 × 43. CT, computed tomography; DSA, digital subtraction angiography; MPR, multiplanar reconstruction; SAA, splenic artery aneurysm; SAP, splenic artery pseudoaneurysm.Fig 1 dummy alt textFig. 2Contrast-enhanced CT, oblique MPR along the long axis of the lesion, demonstrating a giant pseudoaneurysm (SAP) surrounding the saccular splenic artery aneurysm (SAA), measuring ≈16.8 cm in maximal length.Fig 2 dummy alt textFig. 3Contrast-enhanced CT, coronal MPR, showing a fistulous tract (asterisk) between the pseudoaneurysm (SAP) and the splenic flexure of the colon (arrowheads).Fig 3 dummy alt textFig. 4Contrast-enhanced CT, axial pelvis, showing blood clots (asterisk) within the rectal lumen, compatible with active lower gastrointestinal bleeding.Fig 4 dummy alt text
Urgent digital subtraction angiography confirmed a giant splenic artery pseudoaneurysm with slow wash-out, partial intraluminal hematoma, and sluggish inflow into the distal splenic artery (Fig. 5). Owing to the severely distorted vascular anatomy and the impossibility of identifying a reliable outflow vessel within the aneurysm, distal catheterization and classical “Sandwich” technique embolization were not technically feasible. The initial objective was therefore to exclude the vascular supply of the pseudoaneurysm by proximal embolization. Attempts at dense coil packing within the proximal splenic artery were unsuccessful, as the coils repeatedly migrated into the pseudoaneurysmal sac (Fig. 6), where they failed to provide effective occlusion. Consequently, the embolization strategy was modified to a combined technique using detachable metallic coils (7 × 150 mm) and the liquid embolic agent Onyx. Post-embolization angiography confirmed complete exclusion of the SAP (Figs. 6 and 7).Fig. 5. Digital subtraction angiography (DSA), coronal projection, demonstrating the splenic artery (asterisk) and the pseudoaneurysm (SAP) before treatment.Fig 5 dummy alt textFig. 6Post-embolization DSA showing proximal embolization of the splenic artery with metallic coils (arrow) and liquid embolic agent Onyx (asterisk) proximal to the pseudoaneurysm (SAP). Migrated coils within the pseudoaneurysmal sac are also visualized (arrowhead).Fig 6 dummy alt textFig. 7Follow-up contrast-enhanced CT confirming complete exclusion of the pseudoaneurysm (arrow indicates the deployed coils). Coils migrated into the pseudoaneurysmal sac are also visualized (arrowhead).Fig 7 dummy alt text
Due to initial hemodynamic stability and successful embolization, emergency laparotomy was deferred.
A follow-up CT the next day showed near-global infarction of the splenic parenchyma, sparing only the upper pole. Several follow-up CT examinations were performed during the early post-embolization period. A control CT performed on day 5 showed findings similar to those observed on day 1, without progression of the splenic infarction or new collections. On day 16, a new CT demonstrated a splenic subcapsular collection and a small left-sided pleural effusion, while the patient was still clinically asymptomatic, and afebrile, with normal white blood cell counts and stable C-reactive protein levels. Despite the persistence of radiological abnormalities, the favorable clinical course led to hospital discharge.
One month after embolization, the patient was re-hospitalized with a marked elevation of inflammatory markers, including a C-reactive protein level of 214 mg/L and leukocytosis (11.05 × 10³/µL), despite minimal clinical symptoms. Follow-up imaging allowed better delineation of the fistulous tract between the splenic and hematic collections (Fig. 8), which was clinically suspected given the initial episode of lower gastrointestinal bleeding. Percutaneous drainage of the splenic collection yielded limited hematic and purulent material (Fig. 9), and a separate pleural drain was placed to treat the associated pleural effusion causing dyspnea.Fig. 8. One-month contrast-enhanced CT. Axial image showing splenic subcapsular (A) and perisplenic hematic collection (B) One-month contrast-enhanced CT. Sagittal MPR depicting a fistulous tract (arrow) between the splenic (A) and hematic (B) collections, with associated left pleural effusion (asterisk).Fig 8 dummy alt textFig. 9Non-contrast-enhanced CT. Axial MPR, performed after percutaneous drain (arrow) placement in the perisplenic hematic collection (B) fistulized into the splenic collection (A).Fig 9 dummy alt text
Open surgery was performed, including splenectomy, resection of the splenic flexure, partial gastrectomy, and excision of the pseudoaneurysm sac.
Postoperative complications included septic shock, pancreatic fistula, acute respiratory distress syndrome, and pulmonary embolism.
The patient ultimately recovered and remained well at 1-year follow-up.
Timeline of presentation, interventions, and outcomesTime pointEventOutcomeDay 0Emergency admission for massive rectal bleeding and abdominal pain. Contrast-enhanced CT: giant splenic artery aneurysm with surrounding pseudoaneurysm and active fistulization into the splenic flexure → urgent DSA and endovascular embolization (coils + Onyx).Complete exclusion of the splenic artery pseudoaneurysm; hemodynamic stabilization; emergency surgery deferred.Day 1Follow-up CT scan.Near-global splenic infarction sparing the upper pole.Day 5Control CT scan.Stable findings compared to day 1; no progression of splenic infarction or new collections.Day 16Follow-up CT scan.Splenic subcapsular collection and small left pleural effusion; patient asymptomatic, afebrile, with normal WBC count and stable CRP.Early post-embolization periodClinical follow-up during hospitalization.Favorable clinical course despite persistent radiological abnormalities → hospital discharge.∼1 monthRe-hospitalization for elevated inflammatory markers (CRP 214 mg/L, leukocytosis). CT: better delineation of fistulous tract between splenic and hematic collections.Percutaneous drainage of splenic collection; pleural drainage for symptomatic effusion.ThereafterOpen surgery: splenectomy, splenic flexure resection, partial gastrectomy, and excision of the pseudoaneurysm sac.Postoperative septic and inflammatory complications.Postoperative courseSeptic shock, pancreatic fistula, ARDS, pulmonary embolism.Progressive recovery.1-year follow-upClinical assessment.Patient asymptomatic and in good general condition.ARDS, acute respiratory distress syndrome; CRP, C-reactive protein; CT, computed tomography; DSA, digital subtraction angiography; SAP, splenic artery pseudoaneurysm; WBC, white blood cells.
Discussion
Fistulization of splenic artery aneurysms (SAAs) or pseudoaneurysms (SAPs) into the gastrointestinal tract is a rare but life-threatening complication, most often revealed by massive gastrointestinal bleeding [2,[4], [5], [6]]. Pseudoaneurysms are particularly fragile and rupture-prone, and both true and false aneurysms may erode into adjacent structures—especially the colon or stomach—when they reach large dimensions or develop in inflammatory environments such as pancreatitis [1,5,7].
From a pathophysiological standpoint, we hypothesize that the lesion initially corresponded to a SAA, estimated at 4.5 cm based on the presence of circumferential mural calcifications. Such calcifications are typically associated with chronic aneurysmal wall remodeling and are less commonly observed in pseudoaneurysms, which lack a native arterial wall. A subsequent contained rupture of this aneurysm likely led to the formation of a splenic artery pseudoaneurysm, which progressively enlarged over an undetermined period. Progressive expansion, local inflammation, and mass effect may have contributed to erosion of the adjacent digestive wall, ultimately resulting in gastrointestinal fistulization (Fig. 10).Fig. 10. Schematic representation of the proposed pathophysiological mechanism. A true splenic artery aneurysm (SAA) undergoes contained rupture (I), resulting in formation of a large secondary splenic artery pseudoaneurysm (SAP). Persistent inflammatory contact between the SAP and the splenic flexure of the colon leads to progressive erosion and fistulization (II). Proximal embolization may control bleeding but does not eliminate the infected pseudoaneurysmal cavity, explaining delayed septic complications.Fig 10 dummy alt text
In our case, the patient presented with a giant pseudoaneurysm (>10 cm) fistulized into the splenic flexure of the colon, leading to acute lower gastrointestinal bleeding. Emergency endovascular embolization rapidly stabilized the patient and achieved hemostasis, which initially suggested successful management. However, this improvement proved transient: over the following weeks, the patient developed delayed complications, including abscess formation, pancreatic fistula, pleural effusion, and ultimately septic shock.
This unfavorable evolution underscores a crucial lesson: while embolization is highly effective in the acute setting, apparent clinical stabilization should not delay definitive surgical management. In the presence of a digestive fistula, prolonged postponement of surgery allows ongoing inflammation, infection, and local necrosis, which dramatically increase postoperative morbidity.
To better contextualize this timeline-dependent risk, we performed a narrative review of the literature. We searched PubMed and Google Scholar using combinations of the terms “splenic artery aneurysm,” “pseudoaneurysm,” “fistula,” “colon,” “stomach,” “small bowel,” “digestive tract,” and “gastrointestinal bleeding,” identifying 19 relevant cases of splenic artery (pseudo)aneurysms fistulizing into the digestive tract. Our review (Table 1) highlights distinct patterns based on the fistula location: the stomach remains the most common site (n = 12), followed by the colon (n = 6) and the small bowel (n = 1).Table 1. Review of relevant published cases of splenic artery (pseudo)aneurysms with digestive fistulization.Table 1 dummy alt textAuthor (Year)TypeFistula locationAneurysm sizeInitial managementDefinitive managementOutcomeColonic fistulasSentenach et al. (1997) [8]SAASplenic Flexure4 cmNone (Emergency)Open surgery (Splenectomy + Colectomy)Uneventful recovery.Sakai et al. (2016) [9]SAPTransverse Colon10 cmTransfusionOpen surgery (Splenectomy + Colectomy)Recovered. Complex course (pancreatitis).Maharaj et al. (2018) [10]SAASplenic Flexure6 cmNone (Emergency)Open surgery (En-bloc resection)Uneventful recovery. Symptom-free at 2 years.Costa et al. (2021) [4]SAPTransverse ColonNREndovascular (Coils)None (Conservative follow-up)Uneventful recovery. No rebleeding.Zogheib et al. (2024) [5]SAAStomach + Colon10 × 12 cmNoneOpen surgery (Splenectomy + Repair)Uneventful recovery.Present caseSAPSplenic Flexure16.8 cmEndovascular (Coils + Onyx)Open surgery (Splenectomy + Resections)Survival after septic shock and ARDS.Gastric fistulasAbuRahma et al. (1991) [6]SAAStomachNRNoneOpen surgery (Splenectomy + Resection)Uneventful recovery.Chiu et al. (1993) [11]SAAStomachGiant (> 5 cm)NoneOpen surgery (Splenectomy + Gastrectomy)Uneventful recovery.Ghassemi et al. (2010) [12]SAAStomach4 cmNoneOpen surgery (Gastric suture)Uneventful recovery.Al-Habbal et al. (2012) [13]SAAStomach8 cmNoneOpen surgery (Splenectomy + Gastrectomy)Uneventful recovery.Ma et al. (2013) [14]SAAStomach5 cmNoneOpen surgery (Splenectomy + Repair)Uneventful recovery.Yang et al. (2013) [15]SAAStomach4.8 cmNoneOpen surgeryUneventful recovery.Akbulut et al. (2015) [1]SAAStomachGiant (> 5 cm)Emergency laparotomySplenectomy + Partial gastrectomyDeath. Intraoperative cardiac arrest.Yue et al. (2015) [16]SAPStomach0.6 cmNoneOpen surgery (Ligature)Recovered after ARDS.Karabulut et al. (2016) [17]SAAStomachGiant (> 5 cm)ResuscitationSurgery (Attempted)Death. Massive hemorrhagic shock.Fierro et al. (2017) [18]SAPStomachNRNoneOpen surgeryUneventful recovery.Panzera et al. (2020) [2]SAAStomach>5 cmEndoscopy (Glue)Open surgery (Splenectomy + Pancreatectomy)Good outcome.Ben Layne et al. (2021)SAPStomachNREndoscopy (Clip)Angioembolization + SurgeryRecovered. Prolonged hospital stay.Small bowel fistulasChen et al. (2021) [19]SAPJejunumNRNoneOpen surgery (Resection)Recovered. Diagnosis was difficult.ARDS, acute respiratory distress syndrome; NR, not reported; SAA, splenic artery aneurysm; SAP, splenic artery pseudoaneurysm.
Analysis of these cases reveals that while gastric fistulas are more frequently reported, they are associated with a high risk of massive hemorrhage and mortality if not surgically managed immediately. Conversely, colonic fistulas—such as the one presented here—are exceptional.
The literature supports our observation: embolization alone may suffice for small, contained aneurysms (<5 cm) without overt fistula, but in giant aneurysms (>5 cm) with digestive tract erosion, a 2-step approach is consistently favored. Immediate endovascular control is valuable for hemodynamic stabilization but must be rapidly followed by early surgical resection to prevent delayed complications [[3], [4], [5], [6]].
Recent expert consensus and systematic reviews have attempted to standardize the management of visceral artery aneurysms (VAAs), focusing on size thresholds and symptomatology. The 2023 ESVS clinical practice guidelines recommend intervention for SAAs >2 cm or in the presence of symptoms or pseudoaneurysmal morphology, but do not address fistulization into hollow organs [20]. Our case highlights this gap and underlines the need for management strategies that explicitly incorporate gastrointestinal fistulization as an indication for expedited surgery.
Conclusion
For splenic artery pseudoaneurysms complicated by gastrointestinal fistula, embolization is an essential first step for hemorrhage control but should be considered a temporizing measure only. Definitive surgical management should follow within days to remove the infected and necrotic focus and prevent delayed septic and inflammatory complications. Early multidisciplinary planning is crucial in these complex cases.
Data availability
All data are included in this article; additional de-identified information is available upon reasonable request.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. Identifiers were removed and images anonymized in accordance with journal policy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Akbulut S.Otan E.Management of giant splenic artery aneurysms: case report and literature review Int Surg 10052015872878
- 2Panzera F.Marchese M.Virdis F.Splenic artery pseudoaneurysm presenting with gastrointestinal hemorrhage: endoscopic and surgical management World J Gastroenterol 2622202031103116
- 3Krokidis M.Hatzidakis A.Hatzitheoklitos E.Endovascular treatment of giant visceral aneurysms: an overview Vasc Endovascular Rev 42021 e 06
- 4Costa A.Gaspar N.Nogueira A.Splenic artery pseudoaneurysm rupture into the colon: a rare cause of lower GI bleeding BMJ Case Rep 1462021 e 241472
- 5Zogheib E.Esmer M.Ouattara D.Ruptured giant splenic artery aneurysm with an exceptional concurrent gastric and transverse colonic fistula: a rare case report Medicine (Baltimore)103202024 e 3395810.1097/MD.0000000000039159 PMC 1129642539093788 · doi ↗ · pubmed ↗
- 6Abu Rahma A.F.Stone P.A.Srivastava M.Ruptured splenic artery aneurysm into the stomach Ann Vasc Surg 531991254257
- 7Rinaldi L.PraticòA.Sica G.Giant visceral artery aneurysms and pseudoaneurysms: a systematic review J Clin Med 1319202457933940785210.3390/jcm 13195793 PMC 11477110 · doi ↗ · pubmed ↗
- 8Sentenach M.Fernandez-Cebrian J.M.Vega JL.Ruptured splenic artery aneurysm into the colon: a rare cause of massive lower gastrointestinal bleeding Hepatogastroenterology 44131997234236