Clostridium associated emphysematous gastritis: A case report and review of literature
Roma Tarar, Chinedu Ezekekwu, Chibuike Enwereuzo, Anishur Rahman

TL;DR
A rare case of Clostridium-associated emphysematous gastritis in a 77-year-old woman is reported, highlighting the importance of early diagnosis and aggressive treatment for survival.
Contribution
This case report documents a rare instance of Clostridium perfringens causing emphysematous gastritis without trauma or malignancy, emphasizing successful surgical intervention.
Findings
Clostridium perfringens was identified as the causative agent in a case of emphysematous gastritis.
Aggressive surgical treatment led to survival in a high-risk patient with this rare condition.
Literature review shows few human cases of Clostridium-associated emphysematous gastritis with definitive identification.
Abstract
Emphysematous gastritis is a rare, often fatal infection of the stomach wall characterized by gas formation and tissue necrosis, most frequently associated with polymicrobial infections. Cases with demonstration of tissue invasion by Clostridium species are exceptionally uncommon. We report the case of a 77-year-old woman with multiple comorbidities, including diabetes mellitus, obesity, atherosclerosis, and chronic kidney disease, who presented with severe abdominal pain, nausea, and vomiting. Imaging revealed gastric emphysema with pneumoperitoneum. Emergent laparotomy demonstrated full-thickness necrosis of the stomach along the lesser curvature, necessitating total gastrectomy with Roux-en-Y esophagojejunostomy and splenectomy. Histopathology confirmed extensive necrosis with gas dissection and abundant gram-positive, boxcar-shaped bacilli consistent with Clostridium perfringens.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2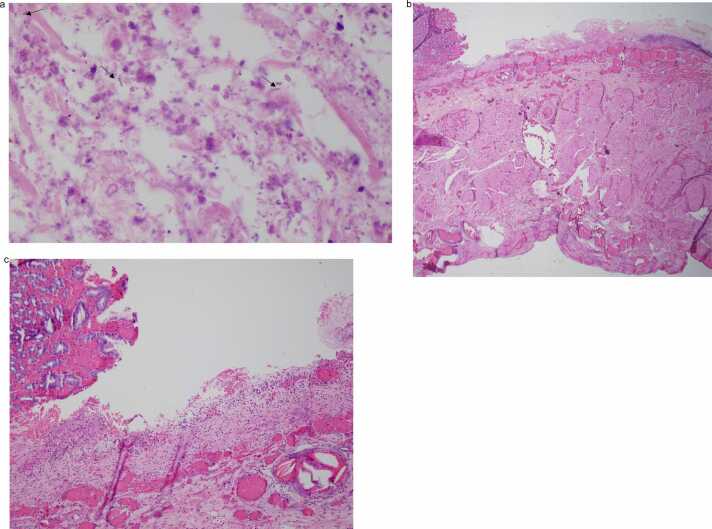 Figure 3
Figure 3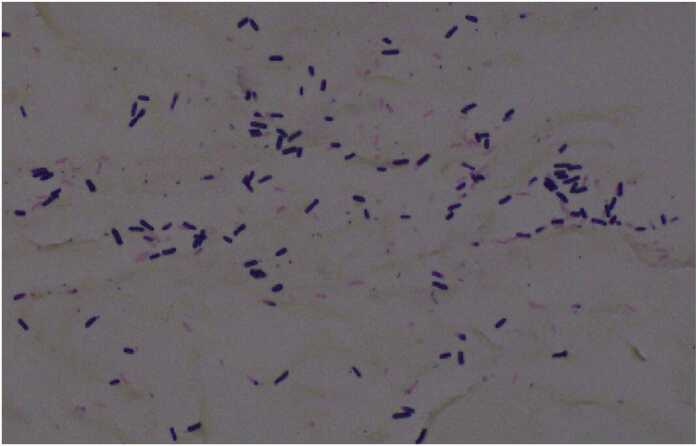 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Infectious Disease Case Reports and Treatments · Pneumothorax, Barotrauma, Emphysema
Introduction
The Clostridia are anaerobic, spore-forming bacilli that are part of the normal intestinal flora of man and animals. They usually cause disease when abnormal tissue provide a relatively anaerobic environment that gives the bacilli a selective growth advantage, favor toxin production and disease establishment [1]. Clostridia associated with human diseases are gram positive [1]. Clostridial myonecrosis or gas gangrene, most frequently caused by C. perfringens is a severe, often-fatal disease characterized by local tissue necrosis, systemic toxemia and gas production from anerobic fermentation [1], [2]. Most cases of intra-abdominal gas gangrene are usually preceded by trauma or surgery, seeding previously sterile tissue with clostridium spores or bacilli [1], [2]. Malignant colorectal neoplasms or some underlying diseases are often seen in cases not previously associated with trauma [2], [3]. Emphysematous gastritis is a rare, life threatening manifestation of Clostridium, characterized by the presence of gas within the gastric wall. [4], [5] The condition has been associated with alcoholism, diabetes mellitus, renal failure, recent abdominal surgery, gastroenteritis, long-term corticosteroid use, ingestion of corrosive agents, and certain medication. [5], [6] Streptococcus species*, Escherichia coli, Enterobacter* species*, Clostridium* species*, Pseudomonas aeruginosa, Staphylococcus aureus, Candida* species*,* and Mucor species have all been implicated in the etiology and the infection has often been reported as polymicrobial. [4], [5], [6] Spontaneous cases, confined to the stomach and not previously associated with trauma, bowel neoplasm or disease have only rarely been reported. We present a case of necrotizing, emphysematous gastritis, associated with prominent tissue invasion by Clostridium Spp.
Case summary
The patient is a 77 year-old woman who presented with a five-day history of upper abdominal pain radiating to the back, accompanied by nausea and vomiting. There was no history of melena, hematemesis, or prior esophagogastroduodenoscopy. The patient's past medical history was notable for morbid obesity, type 2 diabetes mellitus, hypertension, coronary artery disease, stage 3 chronic kidney disease, obstructive sleep apnea, chronic obstructive pulmonary disease, and a history of nicotine abuse. On presentation, the patient was febrile and tachycardic, with laboratory findings significant for leukocytosis, elevated serum lactate, procalcitonin, and C-reactive protein levels, consistent with a systemic inflammatory response.
A non-contrast computed tomography (CT) scan of the abdomen revealed pneumoperitoneum and extensive gastric emphysema. Additionally, marked aortic atherosclerosis and a dilated descending aorta were observed. The patient underwent emergency surgery the same day, including exploratory laparotomy, total gastrectomy and Roux-en-Y esophagojejunostomy. A splenectomy was performed due to active splenic hemorrhage. Intraoperative inspection revealed full-thickness necrosis along the entire length of the lesser curvature of the stomach, extending from the gastroesophageal (GE) junction to the prepyloric region. An intraoperative upper gastrointestinal endoscopy confirmed ischemic changes extending beyond the GE junction into the stomach, while the esophagus appeared uninvolved (see Fig. 1). The stomach was resected, together with a portion of the duodenum and spleen and submitted for pathological evaluation.Fig. 1. Gastric endoscopy, showing gastric necrosis.Fig. 1
Pathology
On gross examination, the gastric serosa was greyish brown and appeared necrotic with thinned areas along the lesser curvature (see Fig. 2). The mucosa surface was erythematous, with gray-brown, flattened areas and loss of gastric folds, corresponding to the necrotic areas noted on the serosa (see Fig. 2). Microscopy revealed extensive necrosis with gas dissection into tissue planes. Prominent, plump boxcar-shaped bacilli were present throughout the necrotic tissue (see Fig. 3a-c). These bacilli were demonstrated to be gram positive on gram stain and morphologically consistent with Clostridium perfringens (see Fig. 4). No notable pathological alterations were identified in the resected portion of the duodenum. The spleen exhibited patchy areas of necrosis, subcapsular hemorrhage, as well as multifocal, calcifying vascular thrombosis.Fig. 2. Formalin fixed tissue showing loss of gastric folds along the lesser curvature (white arrow and circle) with relative sparing of the greater curvature.Fig. 2. Fig. 3a. H&E section of gastric tissue showing transmural necrosis, necro-inflammatory debris and gas expanding and dissecting through tissue planes. The black arrows show numerous plump bacilli visible in the section (x60 objective). Fig. 3b. Low power view of the stomach cross section showing extensive mucosal necrosis and hemorrhage (x2 objective). Fig. 3c. High power view of the stomach cross section showing mucosal necrosis, partially necrotic and hemorrhagic (x10 objective).Fig. 3. Fig. 4Gram stain confirms numerous, plump, “boxcar” shaped gram-positive organisms, morphologically consistent with *Clostridium Spp.*Fig. 4
Discussion
This patient presented with necrotizing emphysematous gastritis, localized along the lesser curvature, which corresponds to the distribution of the left gastric artery. The stomach typically has a rich vascular network, receiving arterial blood from multiple primary sources with collateral circulation that protects the stomach from ischemic injury, making isolated gastric necrosis an exceptionally rare event. Clostridium rarely invades healthy tissue and requires a localized reduction in oxygen tension to establish disease. The patient’s history of type II diabetes mellitus, atherosclerotic disease and morbid obesity (BMI-49) increases the risk of vascular disease. A localized thrombosis may have caused tissue hypoxia, providing a nidus for Clostridium to invade, multiple and amplify the necrosis. This possibility is supported by involvement of a vascular distribution area (the lesser curvature perfused by the left gastric artery) and partial viability around the greater curvature, as well as the patchy vascular thrombosis present in the spleen.
Gangrenous tissue infection caused by Clostridium spp, especially C. Perfringens is a frequently fatal condition that requires prompt surgical resection of affected tissue to control the infection and offer any chance of survival. Our review of literature showed about four cases of emphysematous gastritis in humans with definitive identification of Clostridium species in clinical specimens and two cases in veterinary medicine. Of the four cases reported in humans, only one was caused by Clostridium perfringens.[7] The patient had gastric wall emphysema and the disease had a fulminant course that was rapidly fatal. Clostridium perfringens was identified in multiple organs on post mortem microbial culture. The remaining 3 cases reported in human were caused by Clostridium ventriculi.[8], [9], [10] Of the three reported cases attributed to Clostridium ventriculi, two did not receive surgical intervention and resulted in fatality. [9], [10] The last case caused by Clostridium ventriculi responded to gastrectomy with full recovery. [8], [9] Two of the cases caused by Clostridium ventriculi occurred in patients with weakened immunity from cancer chemotherapy and immunosuppressant for organ transplant, respectively. This suggests immunosuppression may play some role in disease pathogenesis for cases caused by Clostridium ventriculi. At least 2 fatal cases have been reported in veterinary medicine, due to Clostridium perfringens and Clostridium septicum involving a cat and a horse respectively. [11], [12] Table 1 shows a list of emphysematous gastritis with demonstration of clostridium in clinical specimen.Table 1A summary of of reported cases of emphysematous gastritis. The index case is number 1.Table 1. SpecieAgesexOrganismCo-morbidityTreatmentOutcome1.Human77 yFClostridium perfringensDM II, Hypertension, Obesity, AtherosclerosisGastrectomyRecovery2.Human76 yFClostridium perfringensHypertension, Obesity, AtherosclerosisMedicalFatal [7]3.Human80 yFClostridium ventriculiBreast cancer on Paclitazel chemotherapyGastrectomyRecovery [8]4.Human35 yMClostridium ventriculiDM, Kidney transplant on immunosupressantMedicalFatal [9]5.Human86 yFClostridium ventriculiDM II, HypertensionMedicalFatal [10]6.Cat10MClostridium perfringensNeuteredMedicalFatal [11]7.Horse3.5 yMClostridium septicumExploratory celiotomyEuthanized [12]
We recognize that conclusive attribution of the disease process to Clostridium perfringens cannot be established based exclusively on histomorphologic features, as other clostridial species may exhibit overlapping characteristics. Molecular confirmation, such as PCR-based detection of C. perfringens toxin genes from formalin-fixed paraffin-embedded tissue, would provide greater evidence of species level identification and toxin profiling, as described by Rood et al. [13] Unfortunately, bacteriologic culture was not performed at the time of surgery, and subsequent efforts to obtain molecular confirmation through multiple commercial reference laboratories were unsuccessful, as such testing is not currently available. Despite this limitation, the observed histopathologic features, namely large, boxcar-shaped, gram-positive bacilli in association with extensive tissue necrosis and gas formation, are most consistent with C. perfringens and do not correspond to morphology typically described for clostridial species known to cause human disease. Furthermore, the fulminant clinical course and necrotizing emphysematous gastritis observed in this case align with previously reported manifestations of C. perfringens, associated infection. Tissue blocks from this case remain available, and we would be willing to pursue PCR-based toxin gene analysis should be an appropriate reference laboratory with expertise in testing formalin-fixed specimens be identified. While conclusive strain typing is not possible under the present circumstances, the convergence of clinical, histopathologic and epidemiologic features supports C. perfringens as the most likely etiologic agent.
Conclusion
In conclusion, the identification of clostridium species in the clinical specimens of patients with emphysematous gastritis or spontaneous gastric necrosis could be alarming and life threatening if not quickly identified and treated. The precise trigger or cause of the condition and why the disease is often confined to the stomach is still unclear. A high index of suspicion is necessary for prompt diagnosis. From the reported cases, gastric resection is the most promising intervention that offers the best chance of survival.
Author agreement statement
We the undersigned declare that this manuscript is original, has not been published before and is not currently being considered for publication elsewhere. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We understand that the Corresponding Author is the sole contact for the Editorial process. She is responsible for communicating with the other authors about progress, submissions of revisions and final approval of proofs.
CRediT authorship contribution statement
Chibuike Enwereuzo: Writing – review & editing, Writing – original draft, Data curation, Conceptualization. Anishur Rahman: Supervision. Chinedu Ezekekwu: Writing – review & editing, Writing – original draft, Data curation, Conceptualization. Roma Tarar: Writing – review & editing, Writing – original draft, Data curation, Conceptualization.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Patient consent
None
Ethical Approval
This study did not involve human participants or animals, therefore IRB/ethical approval was not required.
Funding
This research received no external funding.
Declaration of Competing Interest
All authors declare that there is no conflict of interest regarding the publication of this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wells C.L.Wilkins T.D.Clostridia: Sporeforming Anaerobic Bacilli Baron S.Medical Microbiology. Galveston (TX): University of Texas Medical Branch at Galveston Copyright © 19961996 The University of Texas Medical Branch at Galveston.21413315 · pubmed ↗
- 2Sivasubramanian G.Rapidly progressive and fatal distant spontaneous gas gangrene due to Clostridium septicum after biopsy of malignant cecal mass ID Cases 242021 e 0112910.1016/j.idcr.2021.e 01129 PMC 811125434007786 · doi ↗ · pubmed ↗
- 3Yıldız T.GündeşS.Willke A.Solak M.Toker K.Spontaneous, nontraumatic gas gangrene due to <em>Clostridium perfringens</em>.Int J Infect Dis 101200683851631039410.1016/j.ijid.2005.02.005 · doi ↗ · pubmed ↗
- 4Elnaggar M.Abbas O.F.Haddad R.Helal M.M.Abou Shawareb H.Abouelmagd A.A.Unrevealing emphysematous gastritis: Insight from a comprehensive systematic review Clin Res Hepatol Gastroenterol 497202510263810.1016/j.clinre.2025.10263840532847 · doi ↗ · pubmed ↗
- 5Riaz S.Kudaravalli P.Saleem S.A.Sapkota B.Emphysematous gastritis: a real indication for emergent surgical intervention?Cureus 1252020 e 810610.7759/cureus.8106 PMC 722880132426198 · doi ↗ · pubmed ↗
- 6Moosvi A.R.Saravolatz L.D.Wong D.H.Simms S.M.Emphysematous gastritis: case report and review Rev Infect Dis 1251990848855223712810.1093/clinids/12.5.848 · doi ↗ · pubmed ↗
- 7Sarvari K.P.Vasas B.Kiss I.Lazar A.Horvath I.Simon M.Fatal Clostridium perfringens sepsis due to emphysematous gastritis and literature review Anaerobe 40201631342703699810.1016/j.anaerobe.2016.03.011 · doi ↗ · pubmed ↗
- 8Savvala N.Carr J.Gallo M.Debourdeau A.Navarro F.Herrero A.An emphysematous gastritis case induced by Clostridium ventriculi, in a patient treated by paclitaxel for breast cancer. Mini review of emphysematous gastritis treatment Surg Open Dig Adv 112023100095