ISUOG Consensus Statement on sonographic assessment of the endometrium: how to perform a gynecological ultrasound scan and report the findings
T. Van den Bosch, R. Heremans, C. Landolfo, E. Epstein, F. P. G. Leone, T. Bourne, D. Timmerman, J. Preisler, J. Preisler, O. Rotenberg, H. Marret, G. Condous, J. L. Alcázar, D. Fischerová, U. Metzger, C. Van Pachterbeke, D. Franchi, M. Nisolle, J. Huirne, C. Fotopoulou

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
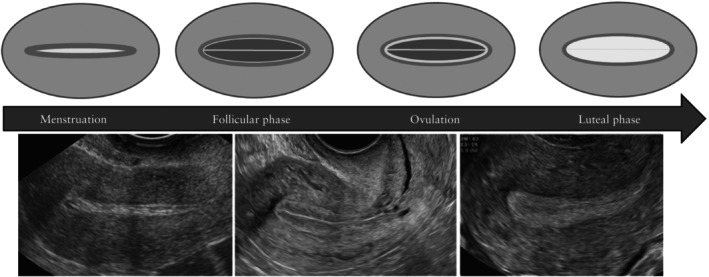 Figure 1
Figure 1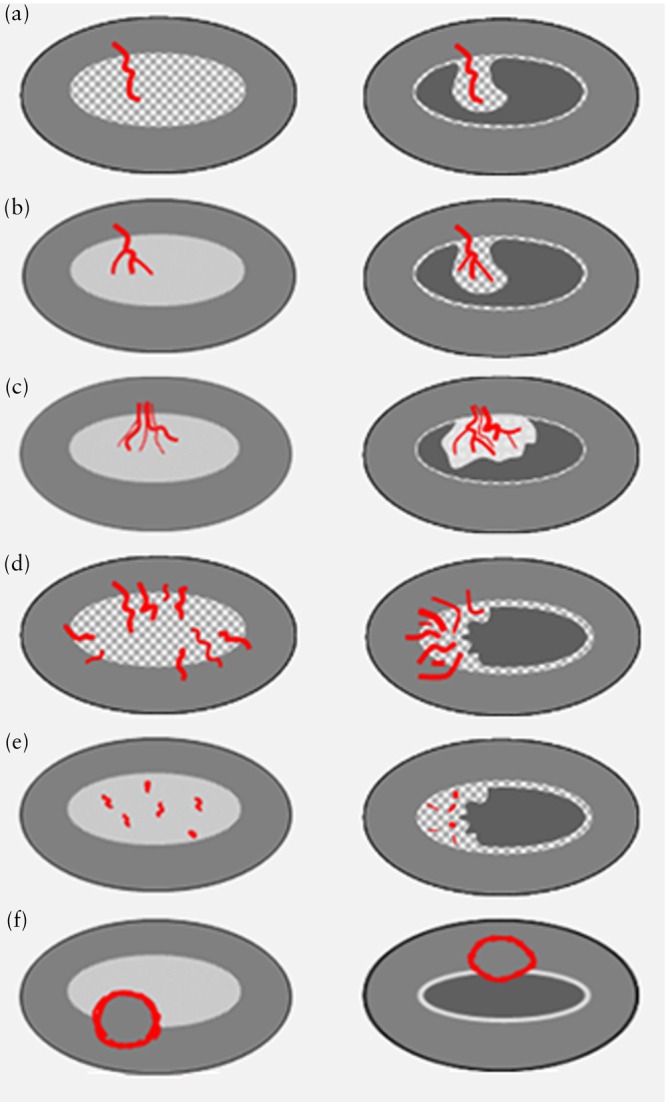 Figure 2
Figure 2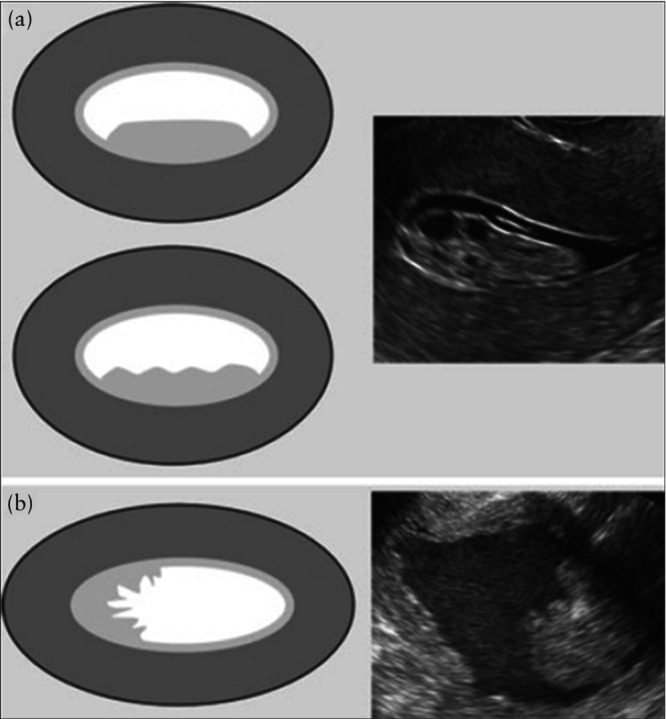 Figure 3
Figure 3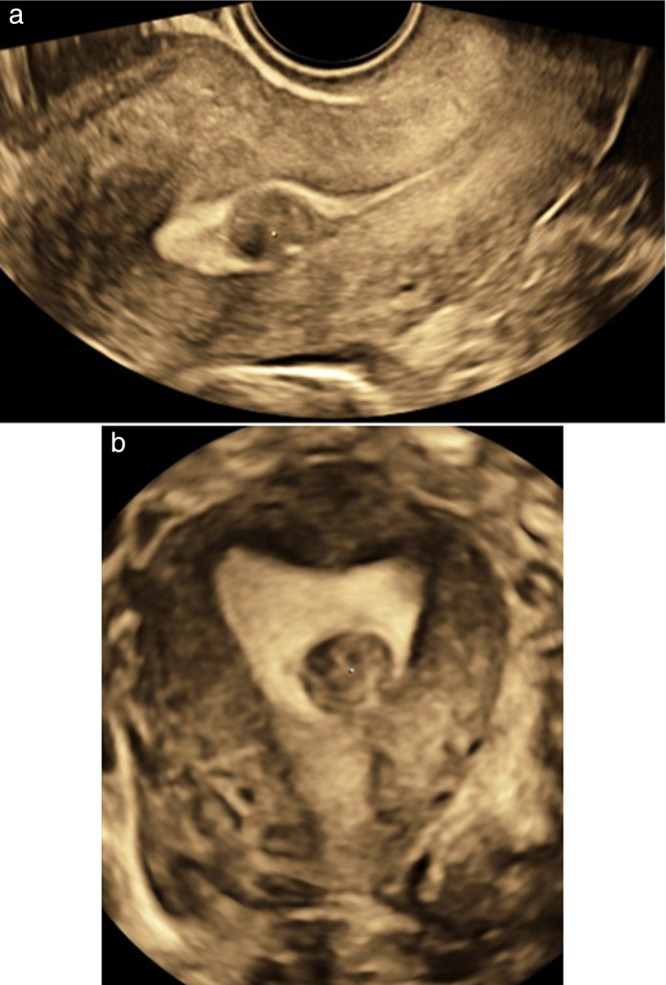 Figure 4
Figure 4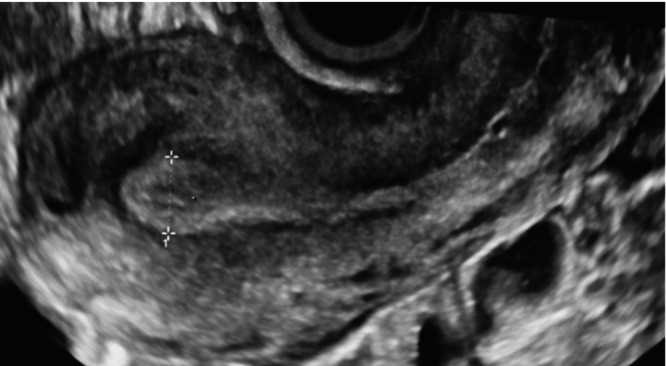 Figure 5
Figure 5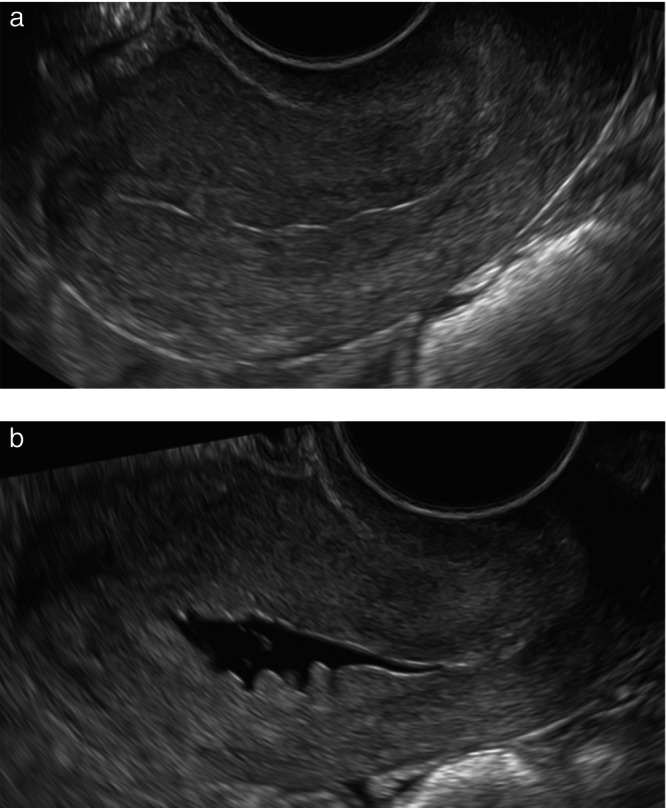 Figure 6
Figure 6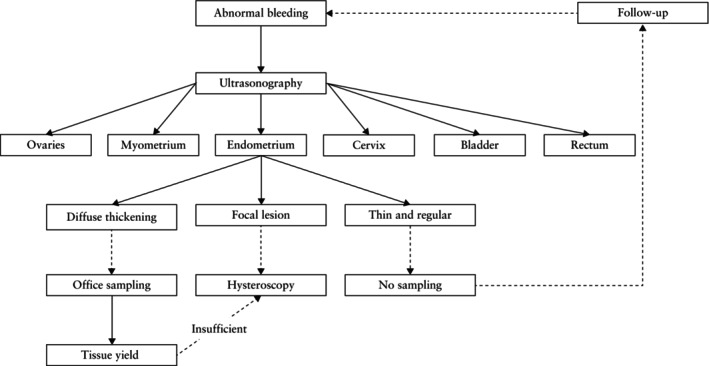 Figure 7
Figure 7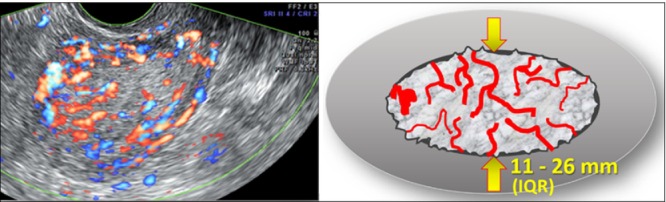 Figure 8
Figure 8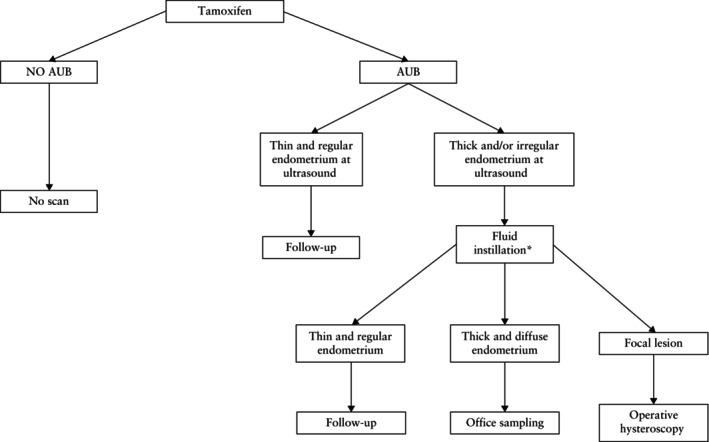 Figure 9
Figure 9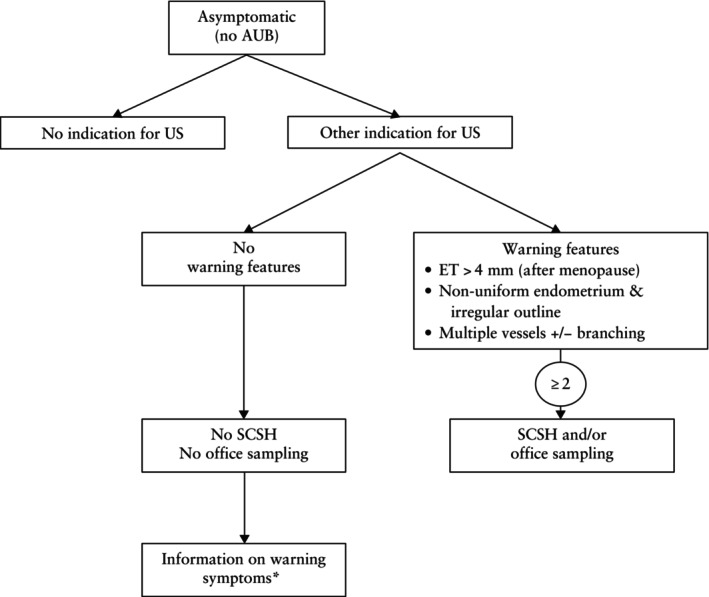 Figure 10
Figure 10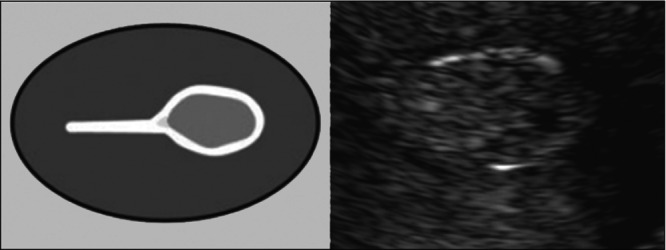 Figure 11
Figure 11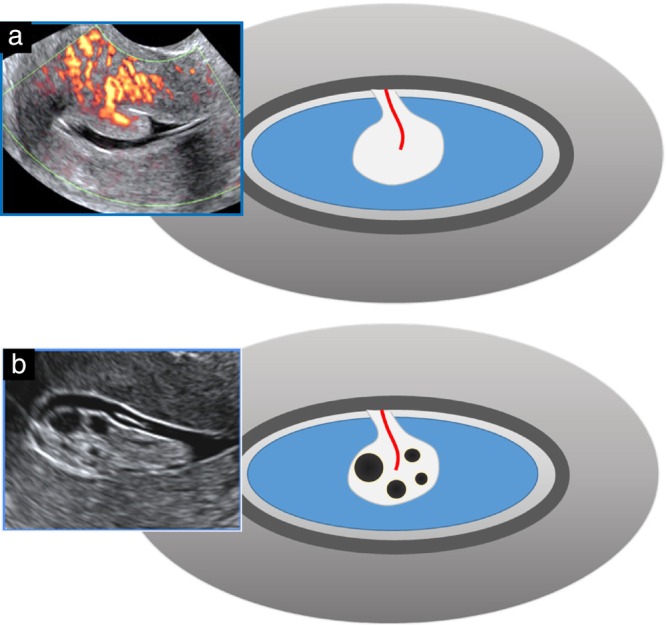 Figure 12
Figure 12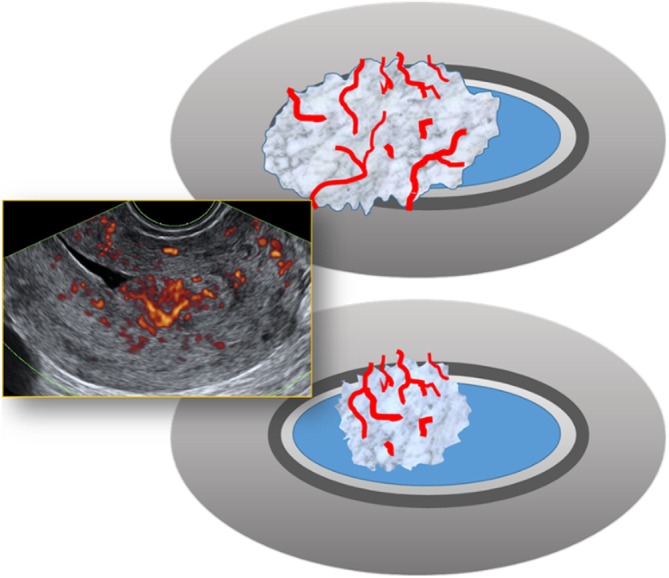 Figure 13
Figure 13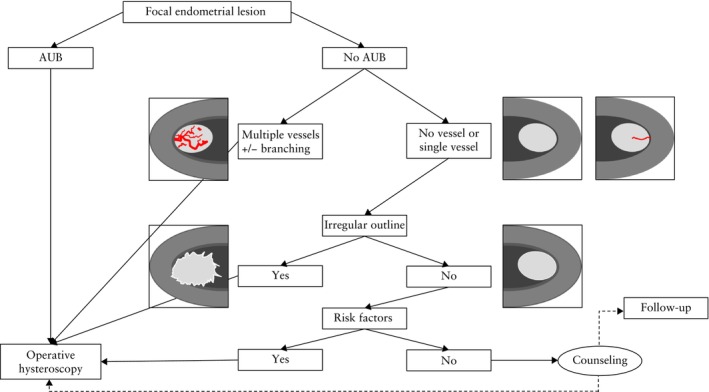 Figure 14
Figure 14| Statements | Agreement ( | |||||
|---|---|---|---|---|---|---|
| Full | Partial | Uncertain | Disagree | Grade of Rec. | Level of Evidence | |
|
| ||||||
| 1. If not contraindicated, and after informed consent has been obtained, transvaginal ultrasonography is the method of choice to evaluate the endometrium | 19/19 (100) | 0/19 (0) | 0/19 (0) | 0/19 (0) | D | 4 |
| 2. Before menopause, in women with a spontaneous cycle, the optimal timing of an ultrasound examination to detect endometrial lesions is in the proliferative phase of the cycle, after the end of menstruation | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | D | 2– |
| 3. In postmenopausal women on sequential hormone replacement therapy, the optimal timing of an ultrasound examination to detect endometrial lesions is in the estrogen‐only phase of the cycle, after the end of withdrawal bleeding | 19/19 (100) | 0/19 (0) | 0/19 (0) | 0/19 (0) | C | 2+ |
| 4. In pre‐ and perimenopausal women, repeating the ultrasound scan after the next menses or hormonally induced withdrawal bleeding may optimize the ultrasound image | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | GPP | 4 |
| 5. |
18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | GPP | 4 |
| 6. | 16/19 (84.2) | 3/19 (15.8) | 0/19 (0) | 0/19 (0) | GPP | 4 |
| 7. | 14/19 (73.7) | 5/19 (26.3) | 0/19 (0) | 0/19 (0) | GPP | 4 |
| 8. | 16/19 (84.2) | 3/19 (15.8) | 0/19 (0) | 0/19 (0) | D | 2+ |
|
| ||||||
| 9. Endometrial thickness is measured in the sagittal plane (where it appears thickest) and recorded in millimeters, conforming to the 2010 IETA Consensus Opinion | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | D | 4 |
| 10. The sonographic features of the endometrium should be described according to the 2010 IETA Consensus Opinion | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | D | 4 |
| 11. It is advisable to include color/power Doppler in the routine sonographic examination of the endometrium | 13/19 (68.4) | 6/19 (31.6) | 0/19 (0) | 0/19 (0) | B | 2++ |
| 12. Although endometrial thickness and sonographic features may be indicative of a specific pathology, ultrasonography should not replace histology. | 17/19 (89.5) | 2/19 (10.5) | 0/19 (0) | 0/19 (0) | B | 2++ |
|
| ||||||
| 13. If the endometrium cannot be identified in its entirety, or in case of doubt about the presence of an intracavitary lesion, sonohysterography using sterile saline or gel should be considered | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | C | 2+ |
| 14. | 14/19 (73.7) | 5/19 (26.3) | 0/19 (0) | 0/19 (0) | GPP | 4 |
| 15. | 13/19 (68.4) | 5/19 (26.3) | 0/19 (0) | 1/19 (5.3) | GPP | 4 |
| 16. Sonohysterography is contraindicated in the presence of a hydrosalpinx, frozen pelvis, suspicion of cervicitis or pelvic infection and if pregnancy cannot be ruled out | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | GPP | 4 |
|
| ||||||
| 17. 3D sonography is not mandatory in the diagnosis of endometrial lesions but may help in the preoperative mapping of intracavitary lesions (e.g. fibroids, polyps) | 17/19 (89.5) | 2/19 (10.5) | 0/19 (0) | 0/19 (0) | C | 2+ |
|
| ||||||
| 18. Management depends not only on the endometrial sonographic features, but also on other clinical factors (e.g. patient age or comorbidity), and requires a well‐informed and shared decision with the patient | 19/19 (100) | 0/19 (0) | 0/19 (0) | 0/19 (0) | GPP | 4 |
| 19. Further testing is not necessary in a woman presenting with postmenopausal bleeding, provided that: (1) the endometrium is clearly visible over its entirety, (2) the endometrial thickness does not exceed 4 mm, (3) there is an absence of internal endometrial vascularity and (4) cervical pathology and other gynecological causes have been ruled out. | 16/19 (84.2) | 2/19 (10.5) | 0/19 (0) | 1/19 (5.3) | C | 2+ |
|
| ||||||
| 20. Routine screening of the endometrium using ultrasound is not indicated in asymptomatic (i.e. no abnormal uterine bleeding), low‐risk, postmenopausal women | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | C | 2+ |
| 21. Routine screening of the endometrium using ultrasound is not indicated in asymptomatic (i.e. no abnormal uterine bleeding) women on tamoxifen | 16/19 (84.2) | 3/19 (15.8) | 0/19 (0) | 0/19 (0) | C | 2+ |
| 22. | 14/19 (73.7) | 4/19 (21.1) | 0/19 (0) | 1/19 (5.3) | GPP | 4 |
|
| ||||||
| 23. In women presenting with a focal endometrial lesion and abnormal uterine bleeding, hysteroscopic removal should be proposed. | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | C | 2+ |
| 24. In the absence of abnormal bleeding, the presence of multiple vessels with an irregular branching pattern as well as the observation of an irregular endometrial echogenicity or outline of the intracavitary lesion indicates that endometrial sampling should be considered. | 17/19 (89.5) | 2/19 (10.5) | 0/19 (0) | 0/19 (0) | GPP | 4 |
|
| ||||||
| 25. | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | C | 2 + |
| 26. | 17/19 (89.5) | 2/19 (10.5) | 0/19 (0) | 0/19 (0) | D | 2+ |
| 27. During endometrial sampling, the tissue yield should be assessed and compared to the sonographic features (in case of minimal tissue yield in a woman with a thickened endometrium at ultrasound scan, a lesion has most probably been missed, and the results of the histology will most probably not be representative) | 18/19 (94.7) | 1/19 (5.3) | 0/19 (0) | 0/19 (0) | C | 2+ |
| Threshold | Sensitivity (%) | Specificity (%) | PPV | NPV | LR+ | LR− |
|---|---|---|---|---|---|---|
| 3 mm | 96.2–100 | 23.0–42.1 | 7.3–9 | 99.7–100 | 1.29 | 0 |
| 4 mm | 94.8–96.0 | 32.0–53.0 | 10.0–12.7 | 99.0–99.4 | 1.41 | 0.13 |
| 5 mm | 88.0–96.2 | 40.0–54.0 | 11.0–21.1 | 98.0–99.3 | 1.47 | 0.31 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGynecological conditions and treatments · Endometrial and Cervical Cancer Treatments · Ultrasound Imaging and Elastography
Clinical Standards Committee
The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) is a scientific organization that encourages sound clinical practice and high‐quality teaching and research related to diagnostic imaging in women's healthcare. The ISUOG Clinical Standards Committee (CSC) has the remit to develop Practice Guidelines and Consensus Statements as educational recommendations that provide healthcare practitioners with a consensus‐based approach, from experts, for diagnostic imaging. They are intended to reflect what is considered by ISUOG to be the best practice at the time at which they are issued. Although ISUOG has made every effort to ensure that Guidelines and Consensus Statements are accurate when issued, neither the Society nor any of its employees or members accepts any liability for the consequences of any inaccurate or misleading data, opinions or statements issued by the CSC. The ISUOG CSC documents are not intended to establish a legal standard of care because interpretation of the evidence that underpins them may be influenced by individual circumstances, local protocol and available resources. Approved Guidelines and Consensus Statements can be distributed freely with the permission of ISUOG ([email protected]).
INTRODUCTION
The aim of ultrasonography of the endometrial cavity is to evaluate the physiological and pathological changes of the endometrium and detect intracavitary lesions. In 2010, the International Endometrial Tumor Analysis (IETA) consortium1 proposed a structured lexicon to standardize the description of the sonographic features of the endometrium and intrauterine lesions. In recent years, several IETA studies2, 3, 4, 5 have applied this lexicon to report the typical sonographic features of normal and abnormal endometrial changes and intracavitary lesions.
The initiative for this Consensus Statement came from the ISUOG CSC. Applying the IETA lexicon, we explain how to perform a gynecological ultrasound scan, focusing on endometrial evaluation, and discuss the reporting of sonographic endometrial findings, focusing on clinical relevance for diagnosis and management. This Consensus Statement will be of interest not only to gynecologists with a special interest in ultrasonography, but also to general gynecologists, those performing hysteroscopy, gynecological oncologists and fertility specialists. Pregnancy‐related findings, Cesarean scar defects, congenital uterine anomalies and cancer staging are beyond the scope of this Consensus Statement.
The contributors to this Consensus Statement are all experts in their fields and have expressed their opinions based on the available literature and evidence. Any clinician applying this Consensus Statement is expected to use their independent medical judgment in the context of the individual clinical circumstances to determine patient care.
METHODS
Twenty experts in the field of gynecological ultrasonography, hysteroscopy and oncology were invited to participate based on their expertise and geographic spread. An online poll was created to assess agreement among all coauthors on the relevant statements for the topics under discussion (Table 1). Statements that were fully or partially agreed upon by ≥ 90% of the voters remained unaltered. Nine statements did not meet this threshold and were reformulated and circulated for a second poll. Both polls were completed by 19 of the 20 participants.
HOW TO PERFORM A GYNECOLOGICAL ULTRASOUND SCAN, WITH FOCUS ON ENDOMETRIAL EVALUATION
History
For the optimal interpretation of an ultrasound examination, the referring clinician should state clearly the reason(s) for referral and share the relevant clinical information (e.g. patient's age, height, weight, body mass index, medication, comorbidity, previous sonographic findings, latex allergy) and relevant gynecological history, including last menstrual period, age at menopause, hormonal/non‐hormonal contraceptive use, hormonal replacement therapy (HRT), gravidity, parity, previous Cesarean section, previous miscarriage or previous surgery.
Setting
Gynecological ultrasonography should be performed in a reassuring environment. The absence of latex allergy needs to be confirmed when working with latex probe covers. It is advised to have latex‐free alternatives (e.g. nitrile gloves). Fully informing the patient and obtaining their consent before proceeding with the examination are essential. The presence of a chaperone might be particularly advisable in adolescents, patients who have had previous negative experience with gynecological (sonographic) examinations, anxious patients or elderly women6. The presence of a chaperone is, whenever possible, offered in the UK and in many other countries in all cases requiring intimate examination. This is mandatory in the UK for children, adolescents and women who are unable to give informed consent6, 7.
Inspection
Prior to vaginal ultrasonography, it is advised to exclude any vulvar or perineal lesions by external examination. Scanning may cause discomfort, thus it is important to communicate with the patient, to reassure them and ask them to tell the examiner whether they experience any anxiety, pain or discomfort8, 9.
Timing of the scan
Before menopause, an ultrasound examination to detect endometrial lesions should preferably be performed in the early proliferative phase of the menstrual cycle (i.e. after cessation of menstrual bleeding) or after withdrawal bleeding in women taking combined hormonal contraception; in postmenopausal women on cyclic HRT, it should be performed in the estrogen‐only phase of the cycle, after the end of withdrawal bleeding, or 5–10 days after the last progestin tablet, depending on the HRT scheme. In the first phase of the menstrual cycle, the endometrium typically has a uniform, hypoechogenic appearance at ultrasound, with a regular, linear midline (i.e. a three‐layer pattern). A focal intracavitary lesion, such as an endometrial polyp, will distort the endometrial midline and will be easily visible against the hypoechogenic background. During menstruation, the presence of intracavitary blood (clots) may obscure the view and impede proper endometrial evaluation. In the secretory phase of the cycle, the endometrium becomes more echogenic and, at the end of the cycle, may even develop a more polypoid growth pattern (Figure 1). This may mask or mimic an intracavitary lesion. If imaging is suboptimal, especially in those presenting late in their menstrual cycle, it may be advisable to ask the patient to come back for a second ultrasound evaluation after the next bleed.
Diagrams and ultrasound images illustrating the physiological endometrial appearance and changes throughout the menstrual cycle.
Scanning technique
Ultrasonography of the endometrium may be performed using a transvaginal, transabdominal or, less commonly, transperineal or transrectal approach. According to some local protocols, it is customary to perform both transabdominal and transvaginal ultrasonography in every patient.
Transvaginal ultrasonography
In most adult women, the endometrium and uterine cavity may be scanned transvaginally7. Transvaginal scanning is the preferred approach, but is contraindicated in women who are unable to give informed consent, when there is vaginal stenosis (e.g. secondary to atrophy, radiotherapy), if the patient is virgo intacta or in the presence of other contraindications for introducing a vaginal probe (e.g. risk of heavy bleeding from an exophytic cervical cancer or after recent vaginal surgery). The management of adolescents should be individualized.
In most cases, the patient should be asked to empty her bladder before the examination. The patient is examined in the lithotomy position. Endocavitary ultrasound transducers are considered semicritical medical devices owing to the high risk of potential contamination10. They therefore require an appropriate probe cover and should undergo high‐level disinfection after use. A probe cover, filled with gel, is placed on the probe and sufficient gel is applied to the cover before the probe is introduced gently into the vagina. In some countries the use of individual gel sachets is mandatory in view of the risk of infection.
In some cases (e.g. cases of postmenopausal bleeding or when there is suspicion of endometriosis), it is advised to evaluate the bladder wall to exclude a bladder lesion (e.g. polyps, primary transitional cell carcinoma or metastatic disease11) or deep endometriosis12. In these circumstances, a minimal level of bladder filling is needed. Therefore, if the bladder is empty, the ultrasound examination may be repeated after 30 min to allow some bladder filling.
For optimal interobserver agreement, it is advisable to keep image orientation (cranial, caudal, left, right) consistent within the same unit/department, and to specify the orientation if deviating from the unit's protocol.
Ultrasound scanning is a dynamic examination13. For example, gentle pressure on the uterus may allow differentiation between a blood clot and a sessile endometrial polyp.
Selective site‐specific tenderness when applying pressure on (part of) the uterus may suggest endometritis or adenomyosis12, 14.
Transabdominal ultrasonography
A transabdominal scan may be preferred when the uterus has an axial position (i.e. when the long axis of the endometrium is continuous with and parallel to the long axis of the endocervical canal), in the presence of large fibroids or a globally enlarged uterus (in which case, having an empty bladder may be advisable) or when a transvaginal scan is considered inappropriate8.
In most cases, before carrying out a transabdominal scan, the patient should be instructed to have a full bladder15. A (partially) full bladder pushes the bowel loops upwards, which creates an acoustic window, enhancing the ultrasound signal. However, an overfilled bladder causes patient discomfort and increases the focal distance between the ultrasound probe and the target organ, decreasing image quality.
Applying gentle pressure with the probe optimizes skin contact, decreases the focal distance and may move overlying structures (e.g. bowel loops) aside. Slight flexion of the patient's legs relaxes the abdominal wall muscles, maximizing contact between the probe and the abdomen.
In patients with morbid obesity or extensive lower abdominal scarring, transabdominal ultrasonography may result in poor image quality. This should be mentioned in the scan report. In such cases, a vaginal probe may be used, placing it into the umbilicus, where the abdominal wall is usually at its thinnest. In patients with morbid obesity, the umbilicus is often located more caudally, which may also result in improved imaging. Placing the transabdominal transducer cranially to the symphysis pubis, immediately below the abdominal panniculus, may also be helpful.
Transperineal ultrasonography
A transperineal approach can be considered to assess perineal tissues, the vagina and the uterine cervix16, 17. In normal circumstances, satisfactory views of the endometrium are rarely obtained owing to suboptimal focal depth and angulation of the uterus. However, in the presence of significant hematometra or uterine prolapse, the endometrium of the lower uterine segment or even midcavity can be assessed adequately.
Transrectal ultrasonography
Transrectal scanning yields an image quality similar to that of the transvaginal route18. Indications for transrectal scanning are vaginal stenosis or other contraindications for introducing a vaginal probe.
A transrectal ultrasound scan may be considered to be intrusive. Comprehensive explanation and informed consent are mandatory8. The management of adolescents should be tailored to the individual. If an adolescent has not had previous sexual intercourse, transrectal ultrasonography may be performed, provided the patient is well informed and accompanied and the examination is carried out in a welcoming and relaxed environment. Transrectal assessment should be avoided in women who are unable to understand or consent to the procedure, for example women with impaired mental health, and in the presence of anal pathology (e.g. anal fissure). In these patients, alternative imaging modalities (e.g. transabdominal ultrasound or magnetic resonance imaging) can be offered.
A vaginal probe can be used for transrectal ultrasound. Before inserting the probe, a lubricant is applied to the anal canal. A digital anal examination is performed first, to indicate the direction of the anal canal and to relax the anal sphincter. The finger is then withdrawn and the probe is pushed gently through the anal canal immediately afterwards. During insertion, the patient is asked to ‘push as if passing stools’ to relax the anal sphincter. Once the tip of the probe has passed through the anal sphincter, the examination is usually well tolerated.
Optimizing image quality
Every assessment of the uterus should start with identification of the bladder and the cervix1. The position of the uterus is noted and measurements taken. The uterus is scanned in the sagittal plane from cornu to cornu and in the transverse (oblique) plane from the cervix to the fundus. Having established an overview of the whole uterus, the image is magnified to contain only the uterine corpus. The magnification should be as large as possible, focusing on the area of interest. In general, the endometrium is easily visualized. The probe frequency should be adapted to the focal depth: for structures near to the probe, a higher frequency is chosen, while a lower frequency will optimize the visualization of deeper tissues.
Suboptimal imaging may arise from variations in uterine position (particularly when axial) or with uterine rotation (e.g. owing to endometriosis or previous surgery‐related adhesions). Further problems may be encountered when the cavity is distorted by coexisting benign pathology, such as adenomyosis or fibroids. Endometrial cancer may also distort the endometrial–myometrial interface3, 19, 20, 21. Malignancy should therefore be considered as a possible explanation when the endometrium is poorly defined.
When the endometrium is difficult to visualize, it may be helpful to trace it from the endocervical canal. If possible, the angle of insonation between the endometrium and the ultrasound beam should be 90° to optimize image quality1.
If the endometrium cannot be seen, saline or gel instillation often provides substantial additional information on the endometrium and the uterine cavity1, 22, 23, 24. For an axial uterus, a transabdominal scan may provide improved images if the endometrium cannot be visualized transvaginally.
Color and power Doppler
In many centers, color or power Doppler is integrated into the routine ultrasound examination1. The use of color or power Doppler is of added value for the detection of intracavitary lesions, such as endometrial polyps, intracavitary fibroids, endometrial malignancy or retained pregnancy tissue19, 25, 26, 27.
Color and power Doppler reflect the amount of blood flow present. The color signal in the endometrium may be scored using a subjective semiquantitative assessment: a color score of 1 is assigned when no color‐flow signals can be identified, a score of 2 when only minimal color can be detected, a score of 3 when moderate color is present and a score of 4 when abundant color is detected1. The optimal pulse‐repetition frequency for the detection of vessels within the uterus is between 0.3 and 0.6 kHz, which corresponds to a velocity scale between 3.0 and 6.0 cm/s. Endometrial blood flow is best appreciated when the direction of flow is parallel to the ultrasound beam.
When evaluating vascular patterns of the endometrium, the region of interest should include the myometrium adjacent to the endometrium, to allow accurate assessment of flow across the endometrial–myometrial junction.
The vascular pattern within the endometrium is reported with reference to the presence of a ‘dominant vessel’, the number of vessels, the presence of branching, the regularity of branching and whether blood vessels flowing into the endometrium have a focal or multifocal origin1 (Figure 2).
Diagrams showing different endometrial vascular patterns observed with power/color Doppler: unenhanced ultrasonographic (left) and sonohysterographic (right) imaging. (a) Single dominant vessel without branching. (b) Single dominant vessel with branching. (c) Multiple vessels with focal origin (two or more vessels appear to share a common stem). (d) Multiple vessels with multifocal origin at the endometrial–myometrial junction. (e) Scattered vessels (dispersed color signals within the endometrium but without visible origin at the endometrial– myometrial junction). (f) Circular flow. Adapted from Leone et al. 1 .
Dominant vessels are defined as one or more distinct (arterial and/or venous) vessels passing the endometrial–myometrial junction1. The dominant vessel may show branching within the endometrium, which is described as either regular/orderly or irregular/disorderly/chaotic. Dominant vessels may present as a single vessel (pedicle artery sign), with or without branching26. Multiple dominant vessels may have a focal origin at the endometrial–myometrial junction or a multifocal origin. Other vascular patterns within the endometrium include scattered vessels (dispersed color signals within the endometrium but without visible origin at the endometrial–myometrial junction) and circular flow1.
Pitfalls
Errors in image interpretation, such as an apparent absence of flow, may be caused by a transient myometrial contraction28, 29, 30, 31. Furthermore, flow may not be apparent at times because the vessels are oriented perpendicular to the ultrasound beam. Excessive pressure with the probe or excessive distance from the endometrium may also impair the detection of blood flow.
Sonohysterography
Sonohysterography involves the instillation of sterile fluid into the uterine cavity to enhance visualization on ultrasound1, 22. The anechoic fluid acts as a negative contrast agent. Either saline (saline contrast sonohysterography) or gel (gel instillation sonography) may be used.
Sonohysterography is indicated if the endometrium cannot be visualized in its entirety or if an intracavitary lesion is suspected1. Sonohysterography and hysteroscopy have similar reported diagnostic accuracy for the visualization of intracavitary lesions32, 33, 34.
The endometrial outline is defined as smooth if the endometrial surface facing the uterine cavity appears regular, and as having endometrial folds, or as ‘polypoid’, if there are deep indentations1 (Figure 3a). The endometrium is described as ‘irregular’ if the surface facing the uterine cavity is cauliflower‐like or sharply toothed (‘spiky’) (Figure 3b). In the presence of a spiky intracavitary lesion, the differential diagnosis must be made between a (potentially malignant) endometrial lesion and a blood clot. Using power Doppler, a blood clot will appear avascular. Unlike an endometrial lesion, a clot often moves within the cavity when gentle pressure is applied with the ultrasound probe35, 36.
Diagrams and ultrasound images showing endometrial or lesional outline at sonohysterography or when there is pre‐existing fluid in the uterine cavity: (a) smooth (upper diagram) or polypoid (lower diagram) outline; and (b) ‘spiky’/irregular outline. Reproduced with permission from Leone et al. 1 .
How to perform sonohysterography
Air bubbles are strongly echogenic and impact significantly on image quality37. It is essential to avoid the presence of air bubbles within the instilled fluid and to carefully flush all the air present within the syringe and the catheter before inserting the catheter into the endocervical canal38.
Different catheters can be used (e.g. neonatal suction catheters, pediatric nasogastric tubes, insemination catheters or dedicated sonohysterography catheters). If the cervical os is stenotic, it can be gently dilated mechanically or distended carefully by applying hydrodilatation.
Once the catheter has been inserted into the cavity, the fluid is injected slowly under direct ultrasound guidance. In most cases, minimal uterine cavity distension using 1–3 mL of fluid is sufficient to allow optimal evaluation of the endometrium and the uterine cavity39.
Sonohysterography is usually well tolerated and does not require any pain medication40. However, some women may experience lower abdominal cramps during and/or after fluid instillation. This is most likely in women with a history of severe dysmenorrhea or deep dyspareunia. In these patients, in the absence of contraindications, the use of a non‐steroidal anti‐inflammatory drug 30 min before fluid instillation may be considered38, 41, 42.
There is no consensus on the use of prophylactic antibiotics before sonohysterography in asymptomatic women. Most centers do not routinely prescribe prophylactic antibiotics, while some use them in women presenting for fertility investigations. In high‐risk populations (e.g. patients at high risk of pelvic infection or with a pre‐existing cardiac condition) prophylactic antibiotics may be considered.
Contraindications
Sonohysterography is contraindicated in the presence of a hydrosalpinx, frozen pelvis or active or previous pelvic infection, on suspicion of cervicitis and if pregnancy cannot be ruled out43.
In fertile women, sonohysterography should not be performed in the second half of the menstrual cycle, in order to avoid false‐positive findings due to normal secretory endometrial folds, which may give a polypoid appearance, and to avoid the possibility of an early pregnancy (unless the latter is deemed impossible)1.
Similar to hysteroscopy44, 45, sonohysterography may cause transtubal seeding of (potentially malignant) endometrial cells into the abdominal cavity46, 47, 48. Although its negative impact on prognosis has not been demonstrated, some experts recommend that, in cases considered highly suspicious for cancer, saline infusion should be avoided or, if performed, the pressure and the volume of saline instillation should be kept to a minimum. Owing to its higher viscosity, gel is less likely to flow through the Fallopian tubes39. Some authors therefore advocate the use of gel instead of saline to minimize the risk of seeding39.
If there is active bleeding in the early postpartum period, saline is preferred to gel infusion. Gel tends to mix with blood and clots, blurring the image, and gel emboli may cause transient hypoxia if there are dilated vessels opening into the uterine cavity and large volumes of gel are instilled42, 49.
Three‐dimensional ultrasound imaging
Three‐dimensional (3D) ultrasound imaging is not mandatory for endometrial lesions but is recommended for the evaluation of congenital uterine anomalies50, 51, 52, 53, 54, and is of added value for the correct preoperative mapping of intracavitary fibroids and polyps (Figure 4), the location of retained pregnancy tissue with enhanced myometrial vascularity, intrauterine contraceptive device/system (IUCD/IUS) localization and the evaluation of Cesarean section scars1, 14, 54, 55, 56.
Example of an intracavitary fibroid visualized on three‐dimensional ultrasound, in sagittal (a) and frontal (b) section.
A 3D scan may also be of help if the uterus is rotated laterally, preventing two‐dimensional acquisition of a midsagittal section. After 3D volume acquisition, offline rotation within the sectional planes often allows reconstruction of an appropriate midsagittal plane57.
In clinical practice, immediate evaluation of the 3D volume during the examination is advisable to assess the image quality and the need for additional volume acquisitions58. Providing that the examiner has been properly trained, this may be performed swiftly, avoiding more time‐consuming secondary testing.
Tips and tricks
Endometrium not visible or not measurable
If the endometrium is not clearly visible, the following steps may be attempted to obtain a better angle of insonation and improve image quality:
Patient position on the table
The patient may be asked to slide downwards on the examination table, tilting the pelvis and flexing the hips.
Bimanual palpation and gentle pressure
Using the transvaginal probe, gentle pressure may be applied to the uterus from the anterior, posterior or lateral vaginal fornix13. Using the non‐scanning hand, the examiner may apply some pressure on the abdomen to move the uterus or the overlying organs. In some cases, waiting for some bladder filling or for transient myometrial contractions to set in or subside may improve the angle of insonation.
Gently pushing the transvaginal probe against the uterine corpus, causing the two endometrial surfaces to slide against each other, may aid in detecting the endometrial midline and/or small intracavitary lesions.
Transabdominal (or transperineal or transrectal) scan
In case of an anteverted or axial uterus, transabdominal scanning (with the patient's bladder partially filled or empty, according to circumstances) may give better ultrasound images. A full bladder may be ideal in some cases, as it helps to position the endometrium more perpendicular to the ultrasound beam, which is optimal for its evaluation.
Fluid instillation
Often, fluid instillation will allow better imaging of the endometrium and the uterine cavity.
Repeating the scan
Often, in the (late) secretory phase and during menses, the endometrium is difficult to evaluate accurately. Repeating the examination in the proliferative phase of the cycle, when the endometrium is uniformly hypoechogenic or trilayer, without intracavitary blood or clots, will generally allow proper evaluation.
Dealing with blood clots
Blood clots may be difficult to differentiate from endometrial tissue38. During fluid instillation, clots may have an irregular outline, mimicking a malignant lesion. The following maneuvers may help to differentiate between a clot and (malignant) endometrial tissue:
Color/power Doppler
On color/power Doppler examination a clot is entirely avascular. However, although the presence of vessels is indicative of an endometrial lesion, their absence does not rule one out.
Pressure
Applying gentle pressure with the probe may cause a clot to slide over the endometrial wall.
Fluid instillation
During fluid instillation a clot often moves and its shape tends to change. The irrigation can also serve to flush debris from the cavity.
Pipelle aspiration
If there is still doubt, a Pipelle aspiration can be performed to confirm the presence of a clot, and follow‐up ultrasound can confirm its disappearance post‐aspiration38.
Subendometrial cysts and adenomyosis
Subendometrial cysts, due to tamoxifen therapy or to adenomyosis, should be distinguished from endometrial cysts (e.g. within an endometrial polyp). If in doubt, fluid instillation may help to make the distinction38.
In adenomyosis, involvement of the junctional zone may blur the endometrial–myometrial junction. In some cases, this may preclude measurement of endometrial thickness. This should be reported accordingly14.
Junctional‐zone involvement in (severe) adenomyosis may not always be distinguishable from malignant myometrial invasion1. Focal increased vascularity increases the probability of malignancy. The possibility of the ‘worst‐case scenario’ should be reported first, followed by the differential diagnosis.
Shadowing
Shadowing due to the presence of (calcified) fibroids or intrauterine devices may hamper imaging. In such a case, moving the probe to optimize the angle of insonation may help1. The presence of shadowing and its cause should be mentioned in the scan report14.
HOW TO REPORT SONOGRAPHIC ENDOMETRIAL FINDINGS, WITH FOCUS ON CLINICAL RELEVANCE FOR DIAGNOSIS AND MANAGEMENT
Reporting the ultrasound scan
If the endometrium cannot be seen clearly in its entirety, it should be reported as ‘non‐measurable’ and no attempt should be made to measure it. The proportion of cases in which the endometrium cannot be measured may exceed 10%59, especially in older patients60.
Endometrial thickness
Endometrial thickness should be measured at its maximum point in the sagittal plane and include both endometrial layers (double‐layer endometrial thickness)1 (Figure 5). The calipers should be placed on the two opposite endometrial–myometrial interfaces in an appropriately magnified image, and the endometrium should be measured at the point at which it appears to be thickest, measuring perpendicular to the endometrial midline. The measurement should be reported in millimeters, rounded up to one decimal point.
Example of double‐layer measurement of endometrial thickness on ultrasound (sagittal section). Calipers should be placed on the two opposite endometrial–myometrial interfaces in an appropriately magnified image (with the full length of the endometrial cavity visible and the uterus filling more than half of the screen), and the endometrium measured at the point at which it appears to be thickest, measuring perpendicular to the endometrial midline.
When intracavitary fluid is present, the thickness of both single layers should be measured, and their sum recorded. In the presence of an intracavitary lesion (e.g. polyp), the total endometrial thickness should include the diameter of the lesion in the sagittal plane as well as both underlying anterior and posterior layers of the background endometrium. However, if an intracavitary myoma is clearly identified, the myoma should not be included in the measurement of endometrial thickness. Intracavitary lesions should be measured in three perpendicular diameters in millimeters, rounded up to one decimal point. If an intracavitary lesion is present, the total endometrial thickness is less relevant than the measurement and description of the lesion itself.
The echogenicity of the intracavitary fluid should be specified (e.g. anechoic, low level, hemorrhagic).
Morphology
An evaluation of endometrial morphology should include assessment of endometrial echogenicity, the endometrial midline and the endometrial–myometrial junction1.
Echogenicity
The echogenicity of the endometrium is described as hyperechogenic, isoechogenic or hypoechogenic compared with the echogenicity of the myometrium1. Endometrial echogenicity should be defined as ‘uniform’ if the endometrium is homogeneous, with symmetrical anterior and posterior sides. A uniform endometrium generally has either a three‐layer pattern (as seen in the proliferative phase of the cycle) or a homogeneous hyperechogenic pattern (as seen in the late secretory phase of the cycle). Endometrial echogenicity is defined as ‘non‐uniform’ if the endometrium appears heterogeneous, asymmetrical or cystic.
Midline
The endometrial midline is defined as ‘linear’ if a straight interface within the endometrium is visualized, as ‘non‐linear’ if a waved interface is seen (Figure 6, Videoclips S1 and S2), as ‘irregular’ or as ‘not defined’ in the absence of a distinct interface1.
Ultrasonographic examples of a non‐linear endometrial midline, in sagittal section. (a) Without fluid instillation, it can be seen that the endometrial midline is not linear. (b) After fluid instillation, note the irregular and polypoid delineation of the cavity.
Endometrial–myometrial junction
The endometrial–myometrial junction is the interface between the basal endometrium and the inner myometrium. It is described as ‘regular’, ‘irregular’, ‘interrupted’ or ‘not defined’1. The inner myometrium underlying the endometrium is also called the ‘junctional zone’.
Clinical relevance: management of abnormal uterine bleeding
The aim of gynecological ultrasonography in women with abnormal bleeding is to exclude or detect intracavitary lesions such as endometrial polyps, intracavitary fibroids, endometrial hyperplasia, endometrial cancer or retained pregnancy tissue61, 62, 63.
Although the focus of this Consensus Statement is on the endometrium, when investigating abnormal uterine bleeding an ultrasound examination allows a broader evaluation of adjacent structures, including the myometrium (e.g. adenomyosis, fibroids, myometrial vascularity), ovaries (e.g. corpus luteum, endometrioma, granulosa cell tumor, tubo‐ovarian abscess), Fallopian tubes (e.g. hydrosalpinx, pyosalpinx, hematosalpinx, tubal pregnancy, tubal cancer), bladder (e.g. transitional‐cell carcinoma, endometriosis, lithiasis, cystitis), cervix (e.g. endocervical polyp, cervical carcinoma, cervical involvement of endometrial carcinoma) and rectum (e.g. endometriosis, malignancy) (Figure 7).
Diagnostic algorithm for women with abnormal uterine bleeding: stepwise diagnostic approach. An ultrasound examination is performed, first, to search for lesions in the bladder, rectum, ovaries, cervix or myometrium, and second, to evaluate the endometrium, triaging women in whom office sampling is most likely to yield an accurate histological diagnosis, those in whom hysteroscopy is indicated and those who do not need further testing.
Differentiating between malignant and benign lesions
In women with abnormal uterine bleeding, endometrial malignancy is unlikely if the total endometrial thickness is considered ‘thin’64, 65, if the endometrium has a uniform three‐layer pattern or if the endometrial midline is regular and linear4, 66, 67. In women presenting with postmenopausal bleeding, the endometrium is considered ‘thin’ if its thickness is ≤ 4 mm, but the clinician may decide to use a lower threshold (e.g. 3 mm) to increase the sensitivity and negative predictive value (Table 2).
Alongside endometrial thickness, endometrial morphology, adequate visualization of the endometrial–myometrial junction and vascularization are also important in differentiating malignant from benign lesions. Endometrial cancer is typically associated with a thickened endometrium (i.e. > 4 mm in postmenopausal women), a heterogeneous endometrium, the presence of irregular cysts, a non‐visible endometrial midline, an irregular, interrupted or ill‐defined endometrial–myometrial junction, multiple vessels of focal or multifocal origin and/or a high color score of 3–44, 68 (Figure 8).
Color Doppler ultrasound image and diagram showing features suggestive of endometrial cancer 4 : thickened endometrium (arrows; interquartile range (IQR) = 11–26 mm in women with cancer), heterogeneous endometrium, presence of irregular cysts, non‐visible endometrial midline, irregular, interrupted or ill‐defined endometrial–myometrial junction, multiple vessels of focal or multifocal origin and/or high color score of 3–4. For postmenopausal women, an endometrial thickness > 4 mm is generally used to define thickened endometrium.
Importance of menopausal status on endometrial thickness and other ultrasound features: the premenopausal endometrium
Endometrial thickness changes continuously in response to hormonal stimulation. Unlike after menopause, a cut‐off value for endometrial thickness is not useful prior to menopause, and endometrial features other than thickness are more relevant4. To investigate abnormal uterine bleeding, ultrasound examination is recommended in the first half of the menstrual cycle, after bleeding has stopped1, 4. In the secretory phase, the endometrium may appear thickened and more echogenic, and physiological endometrial changes may be difficult to distinguish from pathology. In such cases, a repeat ultrasound examination after the cessation of menstrual bleeding may be indicated.
Spontaneous cycle
In women with a spontaneous menstrual cycle, information about the day of the cycle and the presence or absence of a dominant follicle or corpus luteum will allow better interpretation of the endometrial features observed at ultrasound. Concordance or discordance between the endometrial appearance, the day of the cycle and the ovarian characteristics should be reported.
Hormonal therapy
Endometrial thickness is affected by the use and type of hormonal contraception (e.g. progestogen‐only pill, monophasic or sequential combined oral contraception). The endometrium of women on continuous hormonal therapy tends to be thin and more hyperechogenic.
Dealing with an IUCD or IUS in situ
In the presence of an IUCD/IUS, owing to shadowing, part of the underlying endometrium is hidden. The endometrium should be recorded as ‘not measurable’. The endometrium alongside the IUCD/IUS is generally visible and relevant sonographic features may be reported. In patients using a copper IUCD, the endometrium displays the usual cyclical hormonal changes, while it stays thin and hyperechogenic in women who have a levonorgestrel IUCD/IUS.
Importance of menopausal status on endometrial thickness and other ultrasound features: the postmenopausal endometrium
Without HRT
Without HRT, endometrial thickness is expected to be thin (i.e. ≤ 4 mm) after the menopause4.
With HRT (e.g. cyclical scheme, continuous scheme)
The endometrial thickness in women using HRT is affected by the HRT regimen, composition and dosage and varies according to the time during the pseudocycle at which the measurement is taken69. According to the British Menopause Society joint guidelines70, the cut‐off for a thickened endometrium is defined as 4 mm for women on continuous combined HRT (ccHRT) and 7 mm for women on sequential HRT (sHRT). However, there is insufficient evidence that endometrial thickness in women using ccHRT differs substantially from that in women using sHRT if the measurement is taken soon after the end of the planned withdrawal bleed. There has been even less research on the effect of current day ‘body‐identical’ HRT regimens on endometrial thickness. In the absence of robust data, clinicians should adopt the same conservative endometrial thickness cut‐off as that used for non‐HRT patients (i.e. 4 mm).
With selective estrogen receptor modulator (SERM) therapy
Ultrasonography should be the first‐line examination for women with abnormal uterine bleeding on SERM therapy (e.g. tamoxifen)71. Cysts are frequently observed in women treated with tamoxifen. Cysts of various different sizes will typically be present in the subendometrial layer, within the (apparently) thickened endometrium or within glandulocystic polyps72. In the absence of abnormal uterine bleeding, there is no indication to perform a routine ultrasound evaluation of the endometrium in women on SERM therapy71, 73 (Figure 9).
*Diagnostic algorithm in patients taking tamoxifen. In those without abnormal uterine bleeding (AUB), ultrasonography is not indicated. In those presenting with AUB, ultrasonography will guide the clinician in triaging patients who do not need further testing (and may be followed up clinically), those in whom office sampling is most likely to yield an accurate histological diagnosis and those in whom hysteroscopy is indicated. Saline‐contrast sonohysterography or gel‐instillation sonography.
Incidental findings
Although there is no place for endometrial cancer screening in the general population74, 75, 76, gynecological ultrasonography is often performed in women without abnormal uterine bleeding for other indications, such as when there is suspicion of an ovarian cyst or pelvic pain5, 77.
Although concern regarding endometrial pathology may not have been the indication for the ultrasound scan, it remains a challenge to manage incidental endometrial ultrasound findings in the absence of abnormal uterine bleeding77. Many studies have focused on the risk of endometrial cancer in relation to endometrial thickness in the postmenopausal population78. However, endometrial thickness should not be the only sonographic feature that is taken into consideration when deciding on further invasive endometrial testing79.
Warning signs
In a woman without abnormal uterine bleeding, further testing should be considered in the presence of two or more warning signs observed during ultrasound examination for another indication. Warning signs include: a thickened endometrium (> 4 mm in postmenopausal women); non‐uniform endometrium with an irregular outline; and multiple vessels with or without branching (Figure 10). However, this algorithm has yet to be validated in a randomized controlled trial. In the absence of robust evidence, the incidental finding of a thickened endometrium (> 4 mm in postmenopausal women) may prompt a more detailed examination during the scan, first to scrutinize both intrauterine and extrauterine features and second to actively exclude the other two warning signs. If both these steps are reassuring, it can be stated that no immediate further action is required. However, patients should be advised to remain vigilant for any postmenopausal bleeding that may occur subsequently, mandating further evaluation.
*Diagnostic algorithm in women without abnormal uterine bleeding (AUB). In women without AUB, sonographic screening for endometrial pathology is not indicated. If an ultrasound scan (US) is performed for another indication, sonographic ‘alarm features’ within the endometrium (ET) are evaluated. These include: (1) a thickened ET > 4 mm in postmenopausal women, (2) non‐uniform endometrium with irregular outline and (3) multiple vessels with or without branching. In a woman without AUB, the incidental finding of two or more of these alarm features indicates that further testing should be considered. The patient should be asked to return if she experiences further AUB. SCSH, saline contrast sonohysterography.
Intracavitary fluid
The presence of pre‐existing intracavitary fluid should be reported1, and the examiner should assess whether a possible explanation for the fluid can be found. Although anechoic intracavitary fluid after menopause due to endometrial atrophy is a common feature and does not deserve further investigation, fluid may also be secondary to bleeding due to intracavitary or tubal pathology (e.g. polyp, fibroid, hematometra with a thin endometrium in women taking contraception associated with intermenstrual spotting or cancer)80, 81. The echogenicity of intracavitary blood often has a ground‐glass appearance or may show a sedimentation level1.
Focal intracavitary endometrial lesions
Endometrial polyps are well‐circumscribed protrusions into the uterine cavity73, 74, 75. The presence of endometrial polyps can be suspected on grayscale ultrasound by the presence of a ‘bright edge’, seen as a sharp and smooth echogenic line that is generated by the interface between the polyp and the juxtaposed endometrium1, 82 (Figure 11).
Diagram and ultrasound image showing the ‘bright‐edge’ sign (formed by the interface between the intracavitary lesion and the endometrium), suggestive of focal intracavitary endometrial pathology. Adapted from Leone et al. 1 .
Endometrial cysts are commonly associated with endometrial polyps after menopause, but can also be seen in atrophic or hyperplastic endometria4, 5. The detection of polyps can be improved by dynamic assessment13. As with blood clots, targeted gentle pressure from the probe against the uterine corpus, or autonomic uterine peristalsis28, 29, 30, 31, can unmask the presence of intracavitary lesions by elongation or sliding (i.e. the ‘sliding (polyp) sign’)1. The use of color/power Doppler will typically demonstrate the presence of a dominant vessel originating from the myometrium and reaching into the central part of the endometrium (i.e. the ‘pedicle‐artery’ sign)1, 4, 5, 26. The risk of malignancy depends on various clinicodemographic factors83. Endometrial cancer within a polyp may be suspected on ultrasonography3, 4, 5, 84, 85 if the lesion has an irregular outline, if there are multiple internal vessels with an irregular branching pattern or if the lesion is large (> 18 mm)3, 4, 5, 85. The presence of intracavitary fluid (pre‐existing or after fluid instillation) improves visualization of the lesion's outline (Figure 12).
Power Doppler and grayscale ultrasound images and diagrams highlighting the differences between premenopausal (a) and postmenopausal (b) focal endometrial pathology on fluid‐instillation sonography. Before menopause, a polyp most often appears hyperechogenic and has a distinct dominant vessel, while after menopause, approximately half of polyps show regular internal cysts and the feeding vessel is often less distinct or even not visible. Adapted from Van den Bosch et al. 4 .
In women presenting with a focal endometrial lesion and abnormal uterine bleeding, hysteroscopic removal is recommended. For the more common clinical scenario of an incidentally identified endometrial polyp in asymptomatic premenopausal or postmenopausal patients, additional sonographic features can help to guide management. The presence of multiple vessels with or without an irregular branching pattern, as well as the observation of an irregular endometrial echogenicity or outline of the intracavitary lesion, should prompt in‐depth discussion on the need for histological diagnosis of the lesion (Figures 13 and 14). In the absence of such warning signs, the following management approaches may be considered: (1) expectant management with no immediate intervention; (2) interval reassessment to evaluate for spontaneous resolution at a later date; (3) sonohysterography to confirm that the lesion is solitary and well‐circumscribed prior to making a management decision.
Power Doppler ultrasound image and diagrams showing multiple vessels with an irregular branching pattern, within an extended (upper diagram) or localized (lower diagram) intracavitary lesion with an irregular outline. Adapted from Van den Bosch et al. 4 .
Diagnostic/management algorithm for focal endometrial lesions. The sonographic detection of a focal endometrial lesion (e.g. polyp) in a woman with abnormal uterine bleeding (AUB) warrants operative hysteroscopy with complete removal of the lesion. In the absence of AUB, a stepwise diagnostic approach is proposed. Hysteroscopy is indicated if multiple intralesional vessels, or an irregular lesion outline, are seen on ultrasound imaging. In the absence of abnormal sonographic features as well as of risk factors for endometrial malignancy, the patient may decide, after appropriate counseling, to undergo expectant management or hysteroscopy.
(Socio)demographic characteristics86, clinical and sonographic findings87 and the patient's preference should be taken into account when considering further management.
Endometrial sampling
When focal lesions are found at sonohysterography, they should be removed using hysteroscopy, while when the endometrium is globally thickened blind sampling techniques may be adequate88.
If endometrial malignancy is suspected based on the sonographic features (Figures 7, 9 and 10), office endometrial sampling is indicated89 and should be processed with priority. Pipelle sampling has good accuracy to detect endometrial (pre)malignancy89, 90 and is a cost‐effective first diagnostic step91. Ultrasound guidance should be considered to optimize sampling adequacy if access to the uterine cavity is difficult. If the sample is inadequate or inconclusive or shows only benign findings, hysteroscopy is recommended.
During endometrial sampling, the tissue yield should be assessed and compared with the sonographic features. If there is minimal tissue yield in a woman with a thickened endometrium at ultrasound scan, a lesion has most probably been missed, and the results of the histology will most probably not be representative92, 93, 94, 95. In these cases, hysteroscopy with targeted biopsy is suggested as a diagnostic alternative (Figure 7)96. Office hysteroscopy is a cost‐effective alternative to immediate operative hysteroscopy97.
Collaborators
J. Preisler, Departamento de Ginecología y Obstetricia, Facultad de Medicina, Clínica Alemana‐Universidad del Desarrollo, Santiago, Chile; Departamento de Ginecología y Obstetricia, Hospital Clínico Universidad de Chile, Santiago, Chile
O. Rotenberg, Department of Obstetrics & Gynecology and Women's Health, Albert Einstein College of Medicine/Montefiore Medical Center, Bronx, NY, USA
H. Marret, Department of Obstetrics, Gynecology and Reproductive Medicine, University Hospital of Tours, Tours, France
G. Condous, Acute Gynaecology, Early Pregnancy, and Advanced Endosurgery Unit, Nepean Hospital, Kingswood, NSW, Australia
J. L. Alcázar, Department of Obstetrics and Gynecology, Clinica Universidad de Navarra, School of Medicine, Pamplona, Spain
D. Fischerová, Department of Obstetrics and Gynecology, First Faculty of Medicine, Charles University and General University Hospital in Prague, Prague, Czech Republic
U. Metzger, Département d'Échographie en Gynécologie et Obstétrique, Centre d'Échographie de l'Odéon, Paris, France
C. Van Pachterbeke, Department of Obstetrics and Gynecology, Brugmann University Hospital, Brussels, Belgium
D. Franchi, Preventive Gynecology Unit, Division of Gynecology, European Institute of Oncology IRCCS, Milan, Italy
M. Nisolle, Department of Obstetrics and Gynecology, Hospital de La Citadelle, University of Liege, Liege, Belgium
J. Huirne, Department of Gynecology and Obstetrics, Research Institute ‘Reproduction and Development’, Amsterdam UMC, Location VUmc, Amsterdam, The Netherlands
C. Fotopoulou, Gynaecological Oncology, Department of Surgery and Cancer, Imperial College London, London, UK
S. Goldstein, Department of Obstetrics and Gynecology, New York University, New York City, NY, USA
CITATION
This Consensus Statement should be cited as: ‘Van den Bosch T, Heremans R, Landolfo C, Epstein E, Leone FPG, Bourne T, Timmerman D and Collaborators. ISUOG Consensus Statement on sonographic assessment of the endometrium: how to perform a gynecological ultrasound scan and report the findings. Ultrasound Obstet Gynecol. 2026;67(2):241–258.
Supporting information
Videoclips S1 and S2 Grayscale (Videoclip S1) and power Doppler (Videoclip S2) ultrasonographic examples of a non‐linear midline.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leone FP , Timmerman D , Bourne T , et al. Terms, definitions and measurements to describe the sonographic features of the endometrium and intrauterine lesions: a consensus opinion from the International Endometrial Tumor Analysis (IETA) group. Ultrasound Obstet Gynecol. 2010;35:103‐112.20014360 10.1002/uog.7487 · doi ↗ · pubmed ↗
- 2Sladkevicius P , Installé A , Van Den Bosch T , et al. International Endometrial Tumor Analysis (IETA) terminology in women with postmenopausal bleeding and sonographic endometrial thickness ≥ 4.5 mm: agreement and reliability study. Ultrasound Obstet Gynecol. 2018;51:259‐268.28715144 10.1002/uog.18813 · doi ↗ · pubmed ↗
- 3Epstein E , Fischerova D , Valentin L , et al. Ultrasound characteristics of endometrial cancer as defined by International Endometrial Tumor Analysis (IETA) consensus nomenclature: prospective multicenter study. Ultrasound Obstet Gynecol. 2018;51:818‐828.28944985 10.1002/uog.18909 · doi ↗ · pubmed ↗
- 4Van den Bosch T , Verbakel JY , Valentin L , et al. Typical ultrasound features of various endometrial pathologies described using International Endometrial Tumor Analysis (IETA) terminology in women with abnormal uterine bleeding. Ultrasound Obstet Gynecol. 2021;57:164‐172.32484286 10.1002/uog.22109 · doi ↗ · pubmed ↗
- 5Heremans R , Van Den Bosch T , Valentin L , et al. Ultrasound features of endometrial pathology in women without abnormal uterine bleeding: results from the International Endometrial Tumor Analysis study (IETA 3). Ultrasound Obstet Gynecol. 2022;60:243‐255.35385178 10.1002/uog.24910 · doi ↗ · pubmed ↗
- 6General Medical Council . Intimate examinations and chaperones. Accessed December 11, 2023.: https://www.gmc‐uk.org/ethical‐guidance/ethical‐guidance‐for‐doctors/intimate‐examinations‐and‐chaperones/intimate‐examinations‐and‐chaperones
- 7The British Medical Ultrasound Society . Transvaginal ultrasound examinations –guidance for practitioners. Accessed August 12, 2023. https://www.bmus.org/policies‐statements‐guidelines/professional‐guidance/guidance‐pages/tvguidance‐for‐practitioners/
- 8Torres A , Horodeńska M , Woźniakowska E , Borowik J . Anxiety connected with pelvic ultrasound in adolescents and their caregivers: comparison of transabdominal and transrectal approaches. J Pediatr Adolesc Gynecol. 2023;36:284‐290.36764510 10.1016/j.jpag.2023.01.216 · doi ↗ · pubmed ↗