Increased Borrelia burgdorferi Seroprevalence in Nova Scotia—Prevalence and Distribution 10 Years Later
Carrie Phillips, Colleen Jackson, Linda Passerini, Kathryn McIsaac, Courtney Loomer, Heather Coatsworth, Jennifer Cram, Elizabeth Simms, David Haldane, Todd F. Hatchette, Glenn Patriquin

TL;DR
This study shows that the number of people in Nova Scotia infected with Borrelia burgdorferi, the bacteria causing Lyme disease, has increased over the past decade, especially in the western part of the province.
Contribution
The study provides updated data on Borrelia burgdorferi seroprevalence in Nova Scotia and identifies a significant increase and geographic shift in infection rates.
Findings
Seroprevalence of Borrelia burgdorferi increased from 0.14% to 1.60% over ten years in Nova Scotia.
The highest seroprevalence rates were observed in the western area of the province.
Seropositivity was detected across all age groups and regions of Nova Scotia.
Abstract
Lyme disease (LD), a tick‐borne infection, is endemic in Nova Scotia. One decade ago, the seropositivity rate to Borrelia burgdorferi was 2/1855 (0.14%). In the current study, using residual sera representing ages 10–64 years, we demonstrate an increase in seroprevalence, to 25/1872 (1.60%), with the highest seroprevalence in the western area of the province. Seroprevalence of Borrelia burgdorferi in Nova Scotia has increased as compared to 10 years agoSeropositivity is detected throughout the provinceHighest rates of seropositivity are in the province's Western Zone Seroprevalence of Borrelia burgdorferi in Nova Scotia has increased as compared to 10 years ago Seropositivity is detected throughout the province Highest rates of seropositivity are in the province's Western Zone
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
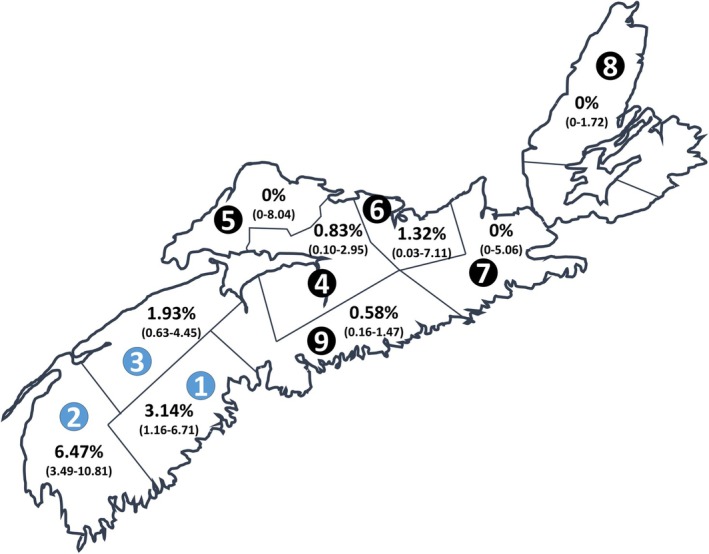 FIGURE 1
FIGURE 1| Region | Total screening tests | pepC10/VlsE EIA positive or indeterminate, no. | WCS EIA positive or indeterminate, no. | Estimated seroprevalence based on MTTT (95% CI) | IgG immunoblot positive or borderline, no. | Estimated seroprevalence based on IgG immunoblot (95% CI) |
|---|---|---|---|---|---|---|
| Western Zone | 653 | 46 | 24 | 3.68 (2.37–5.42) | 21 | 3.22 (2.0–4.87) |
| fDHA 1 | 191 | 16 | 6 | 3.14 (1.16–6.71) | 5 | 2.62 (0.86–6.0) |
| fDHA 2 | 201 | 18 | 13 | 6.47 (3.49–10.81) | 11 | 5.47 (2.76–9.58) |
| fDHA 3 | 259 | 12 | 5 | 1.93 (0.63–4.45) | 5 | 1.93 (0.63–4.45) |
| Northern Zone | 242 | 12 | 2 | 0.83 (0.10–2.95) | 1 | 0.41 (0.01–2.28) |
| fDHA 4 | 122 | 7 | 1 | 0.82 (0.02–5.93) | 0 | 0 (0–2.98) |
| fDHA 5 | 44 | 4 | 0 | 0 (0–8.04) | 0 | 0 (0–8.04) |
| fDHA 6 | 76 | 1 | 1 | 1.32 (0.03–7.11) | 1 | 1.32 (0.03–7.11) |
| Eastern Zone | 284 | 14 | 0 | 0 (0–1.29) | 1 | 0.35 (0–1.95) |
| fDHA 7 | 71 | 7 | 0 | 0 (0–5.06) | 1 | 1.41 (0.04‐7.60) |
| fDHA 8 | 213 | 7 | 0 | 0 (0–1.72) | 0 | 0 (0–1.72) |
| Central Zone (fDHA 9) | 693 | 21 | 4 | 0.58 (0.16–1.47) | 2 | 0.29 (0.03–1.04) |
| Nova Scotia | 1872 | 93 | 30 | 1.60 (1.08–2.28) | 25 | 1.34 (0.87–1.97) |
- —Research Nova Scotia10.13039/501100020170
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Zoonotic diseases and public health · Bartonella species infections research
Introduction
1
The incidence of Lyme disease (LD), caused by Borrelia (Borreliella) burgdorferi sensu stricto, is increasing in Canada, and it is a reportable disease in Nova Scotia, a province with the highest incidence of LD in the country (Public Health Agency of Canada 2023). In Eastern Canada and the Northeastern United States, B. burgdorferi is transmitted by the black‐legged deer tick ( Ixodes scapularis ). In 2012, a serosurvey was performed, using residual sera in Nova Scotia (specimens from routine outpatient testing that would have otherwise been discarded). Anonymised samples representing males and females, aged 10–64 years, from each District Health Authority were tested using the standard two‐tiered testing (STTT) algorithm and revealed a seropositivity rate of 2/1855 (0.14%) (Hatchette et al. 2015). The entire province of Nova Scotia has since become an at‐risk area for LD and the number of annual clinical cases reported to public health has increased from 2 cases in 2002 (Nova Scotia Department of Health 2003) to over 2000 cases in 2023 (Nova Scotia Department of Health and Wellness 2024). Although the significant increase is partially related to the change in the case definition used by Public Health (relying solely on laboratory data rather than clinical evidence coupled with laboratory confirmation), given this continued increase in cases, we sought to determine the seroprevalence of exposure to B. burgdorferi in Nova Scotia, as an update to prior work.
Materials and Methods
2
After Institutional Research Ethics Board approval, we collected 1852 residual serum samples that would have otherwise been discarded after diagnostic testing, similar to the prior study (Hatchette et al. 2015). Nine regional laboratories from throughout the province provided deidentified residual sera originally submitted for routine testing such as prenatal bloodwork, HIV, cholesterol and endocrinology requests between October 2022 and November 2023. Specimens were stratified by patient age, sex and former District Health Authority (fDHA) to maintain consistency with the 2012 data. The fDHAs have since been amalgamated into a single provincial health authority, divided into administrative zones (Western [fDHAs 1–3], Northern [fDHAs 4–6], Eastern [fDHAs 6–8] and Central [fDHA 9]). To best replicate the previous study (Hatchette et al. 2015), we used sample sizes determined previously (based on estimated seroprevalence of 1.0% ± 0.5% precision), representing the population proportionate to its fDHA (with oversampling in the Western Zone) and ensuring representation of sexes and age groups (10‐year age groups from 10 to 59 years and a single age group from 60 to 64 years).
The modified two‐tiered testing (MTTT) algorithm was performed as described previously (Khan et al. 2022; Davis et al. 2020). Briefly, a commercially available ZEUS pepC10/VlsE enzyme immunoassay (EIA) (ZEUS ELISA Borrelia VlsE1/pepC10 IgG/IgM, ZEUS Scientific, Branchburg, NJ) was used for screening the sera. Specimens that were reactive or equivocal to the screen were then confirmed as positive with the Zeus whole cell sonicate EIA (ZEUS ELISA Borrelia burgdorferi IgG/IgM). This reactive cohort was also tested approximating the STTT method (noting that the previous STTT method used the WCS EIA as an initial screen). Briefly, the pepC10/VlsE EIA‐reactive samples were tested with a B. burgdorferi US IgG immunoblot (EUROIMMUN Medical Diagnostics Canada Inc., Mississauga, ON) at the National Microbiology Laboratory (Winnipeg, Canada), according to the manufacturer's instructions. A positive IgG immunoblot consisting of at least 5/10 significant bands (p18/21, p25 (OspC), p28, p30, p39 (BmpA), p41, p45, p58, p66 or p83/93) was considered reactive, while a borderline (BL) result was defined as 4/10 significant positive bands, in addition to at least one weakly positive significant band or, when 4/10 significant bands plus the VlsE band were positive. Five BL results were considered positive for the analysis to match previously used methods.
Similar to the prior serosurvey, descriptive statistics were used as previously (Hatchette et al. 2015), with proportions calculated with 95% CI by the Clopper–Pearson Exact method, using EPITOOLS (https://epitools.ausvet.com.au) and GraphPad QuickCalcs (https://www.graphpad.com/quickcalcs), with oversampling in the Western Zone to best approximate the previous work.
Results
3
Employing the MTTT assay, we screened 1872 serum specimens. A total of 93 specimens were positive or indeterminate by the pepC10/VlsE EIA and underwent confirmation testing by the WCS EIA (Table 1). Of the 93 screen‐positive samples, 30 were confirmed with the WCS EIA (MTTT assay), for a total seroprevalence of B. burgdorferi in Nova Scotia ranging from 0% to 6.47%, depending on the fDHA (Figure 1). Province‐wide, seroprevalence was found to be 1.60% (95% CI 1.08–2.28) overall. The highest seroprevalence was found in the Western Zone (fDHAs 1–3), at 3.68% (95% CI 2.37–5.42), especially fDHA 2, at 6.47% (95% CI 3.49–10.81). Among the 30 positive patients, two‐thirds were male, and there was no significant trend by age.
TABLE 1: Seroprevalence of B. burgdorferi in Nova Scotia, by assay and region.
Map of Lyme seropositivity in Nova Scotia, Canada. Former District Health Authorities (fDHAs) are numbered in circles. Seroprevalence for each fDHA is expressed as a percentage, with corresponding 95% confidence interval in parentheses. fDHAs with blue numbered circles represent the province's Western Zone.
Using the STTT, 25 of the 30 pepC10/VlsE EIA‐reactive samples were confirmed by the IgG immunoblot. The regional distribution was similar to that of the MTTT analysis, with the highest seroprevalence in the Western Zone, but the seroprevalence was not as high as that determined by the MTTT (Table 1). Overall provincial seropositivity based on STTT was 25 of 1872 tested (1.34%, 95% CI 0.87–1.97). Two immunoblots could not be read due to non‐specific background signal (one each of WCS EIA‐positive and ‐negative), so they were considered undetermined.
Discussion
4
Results from this study period demonstrate a higher seropositivity rate to B. burgdorferi when compared to results from a prior study performed 10 years ago (from 0.14% to 1.60%) in the Canadian province of Nova Scotia (Hatchette et al. 2015). This increased seropositivity is consistent with an increase in reported cases in Nova Scotia. The Western Zone had high seropositivity, correlating with the highest number of reported cases at 1192 (57.9% of cases in the province) in 2023, for a rate of 582.1 cases per 100,000 population (Nova Scotia Department of Health and Wellness 2024). In fact, when the Western Zone is excluded from the provincial calculation, the seroprevalence is only 0.49% (96% CI 0.18–1.07), as compared to the seropositivity rate of 3.68% in the Western Zone alone. The higher seropositivity of males in this study is consistent with clinical cases reported to public health, where the rate per 100,000 in males was 224.8 compared to 164.7 in females (Nova Scotia Department of Health and Wellness 2024). Although age distribution was important for ensuring sample representativeness, no conclusions could be drawn associating age with seropositivity from our small number of positive tests.
This study has several limitations. The seroprevalence is based on the region where testing was performed and may not reflect where the tick/pathogen exposure occurred. Unfortunately, due to the discontinuation of routine tick surveillance in the province, there is difficulty in ascertaining region‐based prevalence of I. scapularis and therefore association of disease with regional vector exposure. In addition, though residual serum has been used in the past to approximate population‐level seroprevalence (Kelly et al. 2002), the potential for bias cannot be eliminated. Residual serum from routine tests could over‐ or under‐estimate exposure to Ixodes spp. ticks (and thus the pathogen, via the tick vector) in unanticipated ways. When comparing seroprevalence differences between the current study and that of 2012, it is important to note the change in testing algorithms, from STTT to MTTT and that this may impact the results. Notably, when using the STTT algorithm with the current samples, the increased seroprevalence is approximately ninefold, at 1.34%. These discrepant results likely reflect increased sensitivity of the MTTT assay when compared to STTT, specifically in early LD, where MTTT assays were 25%–28% more sensitive than STTT assays in a Nova Scotian population. Importantly, the MTTT, maintains a high specificity of 99.6% which is essential when interpreting seroprevalence studies (Khan et al. 2022; Davis et al. 2020). Although we sampled residual sera from presumed healthy community‐dwellers, we cannot rule out the possibility that the residual sera were collected from someone with early infection. The specimens were de‐identified at the point of aliquoting, making clinical correlation not possible. Additionally, considering the increased accessibility to prophylactic doxycycline in the community through local pharmacies (Bell et al. 2025), it is possible that we have under‐detected antibodies to B. burgdorferi as prophylaxis or early therapy may abrogate an immune response (Hu 2016).
This work demonstrates an increase in seroprevalence to B. burgdorferi in Nova Scotia, consistent with the ongoing increase in LD cases seen in the province likely reflecting increases in infected tick populations. Since the first report from a decade ago, three other human pathogens transmitted by I. scapularis ( Anaplasma phagocytophilum , Babesia microti, and Powassan Virus) have been added to the Nova Scotia Notifiable Diseases list, given their increase in clinical cases (Chase and Bonnar 2018; Allehebi et al. 2022) and/or detection in the tick population (Guillot et al. 2022).
Clinicians should continue to consider LD in patients presenting with compatible syndromes and residents and travellers to Nova Scotia should continue to take precautions to protect themselves from Ixodes spp. tick exposure, given the increased risk of LD.
Funding
This work was supported by Research Nova Scotia (2023‐2915).
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Allehebi, Z. O. , F. M. Khan , M. Robbins , et al. 2022. “Lyme Disease, Anaplasmosis, and Babesiosis, Atlantic Canada.” Emerging Infectious Diseases 28, no. 6: 1292–1294. 10.3201/eid 2806.220443.35608954 PMC 9155882 · doi ↗ · pubmed ↗
- 2Bell, M. , T. Ramsey , S. Trenaman , et al. 2025. “Lyme Disease Chemoprophylaxis Prescribing Before and After Pharmacist Prescriptive Authority in Nova Scotia.” Canadian Pharmacists Journal 158, no. 1: 47–54. 10.1177/17151635241290519.39563711 PMC 11571129 · doi ↗ · pubmed ↗
- 3Chase, B. , and P. Bonnar . 2018. “A Walk Through the Tall Grass: A Case of Transaminitis, Thrombocytopenia, and Leukopenia Resulting From an Emerging Zoonotic Infection in Nova Scotia.” Journal of the Association of Medical Microbiology and Infectious Disease Canada 3, no. 4: 247–250.
- 4Davis, I. R. C. , S. A. Mc Neil , W. Allen , et al. 2020. “Performance of a Modified Two‐Tiered Testing Enzyme Immunoassay Algorithm for Serologic Diagnosis of Lyme Disease in Nova Scotia.” Journal of Clinical Microbiology 58, no. 7: e 01841‐19. 10.1128/JCM.01841-19.32321781 PMC 7315017 · doi ↗ · pubmed ↗
- 5Guillot, C. , J. Badcock , K. Clow , et al. 2022. “Sentinel Surveillance of Lyme Disease Risk in Canada, 2019: Results From the First Year of the Canadian Lyme Sentinel Network (Ca L Se N).” Canada Communicable Disease Report 46, no. 10: 354–361. 10.14745/ccdr.v 46i 10a 08.PMC 772331633315999 · doi ↗ · pubmed ↗
- 6Hatchette, T. F. , B. L. Johnston , E. Schleihauf , et al. 2015. “Epidemiology of Lyme Disease, Nova Scotia, Canada, 2002–2013.” Emerging Infectious Diseases 21, no. 10: 1751–1758. 10.3201/eid 2110.141640.26401788 PMC 4593424 · doi ↗ · pubmed ↗
- 7Hu, L. T. 2016. “Lyme Disease.” Annals of Internal Medicine 164: ITC 65–ITC 80. 10.7326/AITC 201605030.27136224 · doi ↗ · pubmed ↗
- 8Kelly, H. , M. A. Riddell , H. F. Gidding , T. Nolan , and G. L. Gilbert . 2002. “A Random Cluster Survey and a Convenience Sample Give Comparable Estimates of Immunity to Vaccine Preventable Diseases in Children of School Age in Victoria, Australia.” Vaccine 20: 3130–3136. 10.1016/S 0264-410X(02)00255-4.12163264 · doi ↗ · pubmed ↗