Can preoperative visual analogue scale chart patterns predict surgical outcomes in older adults with lumbar spinal stenosis? : A two-center retrospective study
Kohei Shibata, Soya Kawabata, Takehiro Michikawa, Yuki Akaike, Yukio Nakajima, Sota Nagai, Kurenai Hachiya, Takaya Imai, Hiroki Takeda, Atsushi Yoshioka, Shinjiro Kaneko, Yudo Hachiya, Nobuyuki Fujita

TL;DR
This study shows that pre-surgery pain score patterns can predict how well older adults with spinal issues will recover after surgery.
Contribution
The study identifies specific preoperative VAS score patterns that predict surgical outcomes in older adults with lumbar spinal stenosis.
Findings
Equal preoperative VAS scores across pain domains predict better surgical outcomes.
High preoperative scores for low back or numbness pain predict poor surgical improvement.
Multivariable analysis confirms strong associations between score patterns and outcomes.
Abstract
Patients with lumbar spinal stenosis (LSS) exhibit significantly different scoring patterns on the visual analogue scale (VAS) chart for low back pain (LP), buttock and lower limb pain (PL), and buttock and lower limb numbness (NL). This study investigated the usefulness of these preoperative scoring patterns on the VAS chart in predicting surgical outcomes in older adults undergoing LSS surgery. Time-course data from patients aged ≥65 years who underwent LSS surgery at two institutions were retrospectively assessed. All participants completed the Zurich Claudication Questionnaire and the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire, which included the VAS chart, before surgery and at 6 months and 1 year postoperatively. In total, 334 participants were evaluated. Patients with equal preoperative scores across all three scales showed the highest average…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
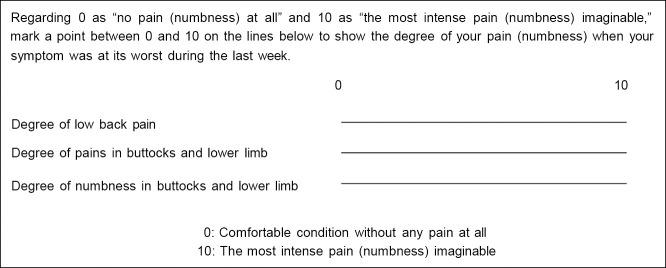 Figure 1
Figure 1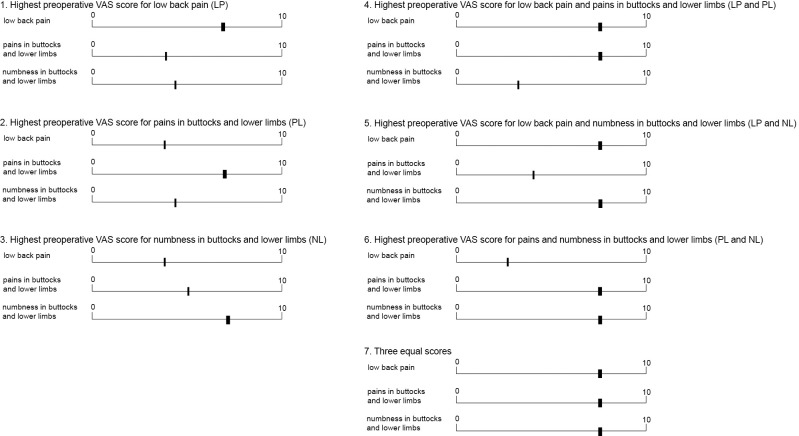 Figure 2
Figure 2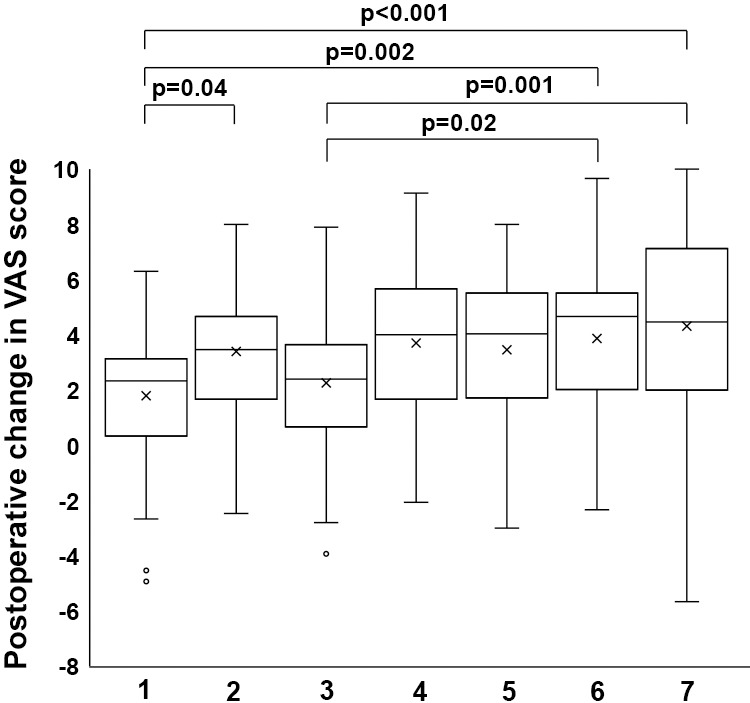 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Cardiac, Anesthesia and Surgical Outcomes · Total Knee Arthroplasty Outcomes
Introduction
Lumbar spinal stenosis (LSS) is a prevalent degenerative musculoskeletal condition in older adults, with its incidence rising globally due to population aging.^1,2^ Common symptoms of LSS include low back and buttock pain, as well as leg pain and numbness, which often lead to considerable limitations in daily activities.^3,4^ Consequently, most older adults with LSS are regarded as being in a condition that may reduce their ability to maintain a healthy life expectancy.^5^
In clinical practice, the visual analogue scale (VAS) is a common tool for assessing chronic pain. It evaluates specific patient sensations on a scale from 0 to 10 and can readily detect subtle differences because of its continuous scale. In 1974, Huskisson^6^ reported that the VAS could serve as a standard tool for pain assessment. Since then, it has been widely used to evaluate pain across various patient populations.^7^ Currently, patient-reported outcomes assessed using tools such as the Oswestry Disability Index, Roland-Morris Disability Questionnaire, and Zurich Claudication Questionnaire (ZCQ) are employed to examine LSS symptoms.^3,4^ Additionally, the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ)—a tool for evaluating patient-reported outcomes—includes a VAS chart comprising three scales to assess low back pain (LP), buttock and lower limb pain (PL), and buttock and lower limb numbness (NL).^8^ When older patients with LSS are asked to score their symptoms on this VAS chart, the resulting scoring patterns vary widely. For instance, some patients report the highest scores for NL, while others show the highest for LP; some may even score all three symptoms equally. A similar variation in symptom patterns is observed among older patients with LSS who undergo surgery. LP is known to be difficult to treat, and NL often persists after LSS surgery. Although several studies have evaluated longitudinal changes in the three VAS scales in LSS,^9–13^ it remains unclear whether preoperative scoring patterns on the VAS chart can predict surgical outcomes in older patients with LSS. This study aimed to longitudinally validate the detailed characteristics of the three VAS scales in older patients with LSS who underwent surgery, with particular focus on investigating the usefulness of preoperative scoring patterns on the VAS chart in predicting surgical outcomes.
Materials and Methods
Participants
Time-course data from patients aged ≥65 years who underwent LSS surgery at two institutions between April 2020 and July 2023 were retrospectively reviewed. Surgical indications and treatment procedures were determined by board-certified spine surgeons, based on patients’ symptoms and imaging results—including magnetic resonance imaging, computed tomography scans, and myelography—in accordance with the guidelines.^3,4^ Patients with an upper instrumented thoracic spine level or a lower instrumented pelvis level were excluded from the analysis.
Ethics approval
The ethics committees of each participating institution approved this study. All eligible patients were included, except those who chose to opt out. The study was conducted in accordance with the guidelines of the Declaration of Helsinki.
Data collection
All participants completed the ZCQ and JOABPEQ, which included the VAS chart, before surgery and at 6 months and 1 year postoperatively. The ZCQ consists of three subscales: symptom severity, physical function, and patient satisfaction.^14^ Data collected included age, sex, body mass index (BMI), medical history (e.g., diabetes mellitus, hypertension, dyslipidemia, cardiovascular disease, stroke, and cancer), presence of spondylolisthesis, degenerative lumbar scoliosis, failed back surgery syndrome (FBSS), American Society of Anesthesiologists (ASA) physical status, radiographic parameters, and perioperative variables such as type of surgical procedure, number of operated levels, surgical duration, and intraoperative blood loss volume. Radiographic parameters included sagittal vertical axis, thoracic kyphosis, pelvic tilt, pelvic incidence, and lumbar lordosis, as measured on standing full-length plain radiographs.
VAS
The VAS scores for LP, PL, and NL were individually assessed using the VAS chart included in the JOABPEQ (Figure 1). If numerical values were indicated on the VAS chart, those values were used as the VAS score. If no numerical values were provided, the mark on the line was measured from the leftmost 0-mark using a ruler, and the measured length was converted to a VAS score by scaling it to a range of 0 to 10. In such cases, the scores were recorded to the first decimal place. Accordingly, all VAS scores in this study were presented to one decimal point, and any difference of ≥0.1 was treated as a distinct VAS value. Based on previous literature,^15^ poor surgical improvement was defined as an average reduction of <2.0 across the three VAS scores at 1 year postoperatively. Figure 2 shows the scoring patterns of the three preoperative VAS scores. According to the VAS scores for LP, PL, and NL, patients were classified into the following groups: group 1 included patients with the highest preoperative VAS score for LP; group 2, those with the highest score for PL; group 3, those with the highest score for NL; group 4, those whose scores for LP and PL were identical and higher than that for NL; group 5, those whose scores for LP and NL were identical and higher than that for PL; group 6, those whose scores for PL and NL were identical and higher than that for LP; and group 7, those with identical scores across all three scales.
Statistical analyses
Data among the groups were compared using the Wilcoxon signed-rank test or the Kruskal–Wallis test with Bonferroni correction, as appropriate. To assess the correlation between two parameters, Pearson’s correlation coefficient (r) was calculated. Analyses were conducted using the Statistical Package for the Social Sciences software version 21.0 (IBM Corp., Armonk, NY, USA). We explored factors associated with poor surgical improvement, including age, sex, BMI, scoring patterns of the three preoperative VAS scores, diabetes mellitus, ASA physical status, spondylolisthesis, degenerative lumbar scoliosis, FBSS, type of surgical procedure, number of operated levels, surgical duration, intraoperative blood loss volume, and radiographic parameters such as sagittal vertical axis, thoracic kyphosis, and pelvic incidence–lumbar lordosis. A Poisson regression model was then constructed, adjusted for age, sex, and factors that were statistically significant in the univariable model, to estimate relative risks (RRs) and 95% confidence intervals (CIs) for poor surgical improvement. Poisson regression analysis was performed using STATA16 software (StataCorp, College Station, TX, USA). All p values of <0.05 were considered statistically significant.
Results
In total, 334 participants were assessed. Table 1 shows the baseline characteristics of the participants. Postoperative ZCQ and JOABPEQ scores (at 6 months and 1 year) were significantly improved compared with the preoperative data (Table 2). Next, changes in VAS scores for LP, PL, and NL before and after surgery were examined (Table 3). All three VAS scores significantly decreased at both 6 months and 1 year postoperatively. A cross-sectional analysis revealed that the preoperative VAS score for LP was significantly lower than that for PL. At 1 year postoperatively, the VAS score for NL was marginally higher than those for LP and PL. However, there were no significant differences among the postoperative VAS scores for LP, PL, and NL. The decrease in VAS scores for LP and NL at 1 year postoperatively was significantly smaller than that for PL. Next, the correlation between the reduction in each VAS score at 1 year postoperatively and the ZCQ satisfaction scores was examined (Table 4). The VAS score for PL showed the strongest correlation with satisfaction (r=–0.28). However, the correlations between each of the three VAS scores and satisfaction were weak. The correlation between the average reduction in the three VAS scores and the ZCQ satisfaction score was –0.29 (Table 4).
Next, the average reduction in the three VAS scores at 1 year postoperatively was compared across the seven groups based on the patterns shown on the VAS chart (Figure 3). The preoperative and 1-year postoperative VAS scores, along with their changes in each group, are summarized in Table 5. The highest average reduction in the three VAS scores was observed in group 7, where all three preoperative scores were initially the same. By contrast, the lowest average reductions were seen in group 1, which had the highest preoperative score for LP, and group 3, which had the highest score for NL (Figure 3). Statistically, the value for group 1 was significantly lower than that for group 2 (p=0.04), group 6 (p=0.002), and group 7 (p<0.001) (Figure 3). The value for group 3 was significantly lower than that for group 6 (p=0.02) and group 7 (p=0.001) (Figure 3).
The factors associated with poor surgical improvement were examined using a Poisson regression model (Table 6). In this analysis, the incidence of poor surgical improvement was similar among groups 4, 5, and 6, and the sample size for each was small, so these three groups were combined. Based on the multivariable analysis, a BMI of ≥25 kg/m^2^ (RR: 1.4 compared with a BMI of <25 kg/m^2^, 95% CI: 1.1–1.9), group 1 (RR: 2.1 compared with group 7, 95% CI: 1.1–3.8), and group 3 (RR: 2.1 compared with group 7, 95% CI: 1.2–3.7) were significantly associated with poor surgical improvement.
Finally, a separate analysis limited to patients who underwent decompression alone was conducted, as shown in Supplementary Table 1. Although no statistically significant associated factors were identified, the proportion of patients classified into group 1 and group 3 tended to be higher in the poor surgical improvement group.
Discussion
This study simultaneously evaluated LP, PL, and NL in older patients with LSS using a VAS chart to validate the detailed characteristics of their longitudinal changes and to identify preoperative scoring patterns on the VAS that were associated with poor postoperative outcomes. Regarding the longitudinal changes in the three VAS scores, the surgical reduction in PL was significantly greater than that in LP and NL, which is consistent with previous research findings.^9,16,17^ Additionally, among the three VAS scales, patient satisfaction with surgery was most strongly correlated with the reduction in the VAS score for PL. Nevertheless, this correlation was not particularly strong. Moreover, patient satisfaction was only weakly correlated with the average reduction in the three VAS scores. This suggests that patient satisfaction does not solely depend on changes in VAS scores. Previous studies have reported that satisfaction is also influenced by improvements in walking ability and preoperative psychological conditions.^18–20^ Therefore, patient satisfaction is likely determined by a complex set of factors.
In this study, there were seven distinct scoring patterns on the VAS chart. The most frequent pattern was the highest preoperative VAS score for NL, followed by the highest preoperative score for PL and then LP. Among these three patterns, patients with the highest preoperative VAS score for PL showed the most favorable improvement in average postoperative VAS scores. By contrast, those with the highest preoperative score for LP or NL exhibited the least improvement. These results are partially consistent with the notion that LP and NL are less likely to improve and more likely to persist after LSS surgery.^9,16,17^ Conversely, the reason why patients with three equal preoperative scores experienced the greatest improvement remains unclear. Based on the multivariable analysis, using patients with three equal scores as the reference, having the highest preoperative VAS score for NL or LP was significantly associated with poor postoperative outcomes. These findings suggest that the VAS chart may be a useful tool for clinicians to communicate outcome tendencies to older patients with LSS during the preoperative informed consent process, offering clinical value. Additionally, our analysis showed that a higher BMI was associated with poor postoperative outcomes, consistent with previous reports.^21,22^ Although previously reported predictors of poor surgical outcomes—such as ASA physical status,^23^ diabetes mellitus,^24^ age,^25^ FBSS,^23^ degenerative lumbar scoliosis,^10^ and sagittal imbalance^26^—were included as explanatory variables in the multivariate analysis, no significant associations were found. Discrepancies between our findings and earlier studies may reflect differences in how poor surgical outcomes are defined or variations in patient populations. Further studies with larger sample sizes and multi-faceted analyses are needed to validate these results. Taken together, the preoperative scoring pattern on the VAS chart can serve as a partial predictor of postoperative outcomes in older patients with LSS. As the use of electronic media for entering patient-reported outcomes increases, incorporating larger datasets along with additional factors such as age, sex, and BMI—and applying machine learning techniques to predict postoperative VAS scores—may hold clinical value.
This study had several limitations. First, a floor effect was present in the reduction of VAS scores. Therefore, if preoperative VAS scores were already low, the potential for postoperative reduction may have been limited. Second, the follow-up period was only 1 year. However, extending the observation period in older patients increases the likelihood that other conditions unrelated to LSS may influence outcomes, making it difficult to exclusively assess the effects of LSS surgery. Third, the study did not exclude cases of spondylolisthesis or degenerative lumbar scoliosis, nor did it focus solely on patients undergoing decompression surgery alone, resulting in a heterogeneous study population. Fourth, medication use, physical therapy, and other non-surgical interventions were not considered as potential confounding factors influencing postoperative outcomes. Despite these limitations, the study clearly demonstrated the potential clinical utility of the VAS chart in predicting surgical improvement for older patients with LSS.
In conclusion, our study examined the detailed longitudinal characteristics of VAS scores for LP, PL, and NL in older patients with LSS who underwent surgery. Patients with three equal scores for the symptoms on the preoperative VAS chart were more likely to show favorable improvement in VAS scores after surgery. By contrast, those with the highest scores for LP or NL were at greater risk for poor surgical outcomes. These findings may assist in managing the complex symptoms of older patients with lumbar spinal stenosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Musculoskeletal conditions; 2022. <https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions> (Accessed Jul 14, 2022)
- 2Yabuki S, Fukumori N, Takegami M, Onishi Y, Otani K, Sekiguchi M, Wakita T, Kikuchi S, Fukuhara S, Konno S. Prevalence of lumbar spinal stenosis, using the diagnostic support tool, and correlated factors in Japan: a population-based study. J Orthop Sci 2013; 18: 893–900.23963588 10.1007/s 00776-013-0455-5PMC 3838585 · doi ↗ · pubmed ↗
- 3Kreiner DS, Shaffer WO, Baisden JL, Gilbert TJ, Summers JT, Toton JF, Hwang SW, Mendel RC, Reitman CA. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spinal stenosis (update). Spine J 2013; 13: 734–743.23830297 10.1016/j.spinee.2012.11.059 · doi ↗ · pubmed ↗
- 4Kawakami M, Takeshita K, Inoue G, Sekiguchi M, Fujiwara Y, Hoshino M, Kaito T, Kawaguchi Y, Minetama M, Orita S, Takahata M, Tsuchiya K, Tsuji T, Yamada H, Watanabe K. Japanese Orthopaedic Association (JOA) clinical practice guidelines on the management of lumbar spinal stenosis, 2021—Secondary publication. J Orthop Sci 2023; 28: 46–91.35597732 10.1016/j.jos.2022.03.013 · doi ↗ · pubmed ↗
- 5Fujita N, Sakurai A, Miyamoto A, Michikawa T, Tsuji O, Nagoshi N, Okada E, Yagi M, Otaka Y, Tsuji T, Kono H, Ishii K, Nakamura M, Matsumoto M, Watanabe K. Lumbar spinal canal stenosis leads to locomotive syndrome in elderly patients. J Orthop Sci 2019; 24: 19–23.30243520 10.1016/j.jos.2018.08.004 · doi ↗ · pubmed ↗
- 6Huskisson EC. Measurement of pain. Lancet 1974; 2: 1127–1131.4139420 10.1016/s 0140-6736(74)90884-8 · doi ↗ · pubmed ↗
- 7Litcher-Kelly L, Martino SA, Broderick JE, Stone AA. A systematic review of measures used to assess chronic musculoskeletal pain in clinical and randomized controlled clinical trials. J Pain 2007; 8: 906–913.17690014 10.1016/j.jpain.2007.06.009PMC 2691574 · doi ↗ · pubmed ↗
- 8Fukui M, Chiba K, Kawakami M, et al. Japanese orthopaedic association back pain evaluation questionnaire. Part 3. Validity study and establishment of the measurement scale. J Orthop Sci 2008; 13: 173–179.18528648 10.1007/s 00776-008-1213-y PMC 2778667 · doi ↗ · pubmed ↗