Establishment and validation of a predictive model for severe pneumonia in children
Wenhua Ye, Jinyan Wu, Mi Cao, Zaidong Yang

TL;DR
This study created a model to predict severe pneumonia in children using factors like temperature and breathing rate to help with early treatment.
Contribution
The novel contribution is the development of a predictive model for severe pneumonia in children based on clinical and laboratory indicators.
Findings
High body temperature and high respiratory rate were identified as independent risk factors for severe pneumonia.
The model uses clinical parameters to distinguish between ordinary and severe pneumonia cases.
Early identification through the model can improve treatment outcomes and reduce hospital burden.
Abstract
This study aimed to develop a model for the early identification of severe pneumonia in children by comparing common laboratory indicators between children with ordinary pneumonia and severe pneumonia. Children aged 1 month to 14 years, diagnosed with pneumonia and admitted to our hospital between January 2017 and June 2022, were included in the study. Participants were divided into two groups based on the severity of their pneumonia. Data, including demographic information, medical history, clinical symptoms, laboratory indicators, and treatment outcomes, were collected from the hospital's medical records system. The single-factor analysis revealed significant differences (P < 0.05) between the two groups in various parameters, including age, length of hospital stay, repeated hospitalization within 90 days, invasive ventilation, Intensive Care Unit (ICU) stay time, birth history,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
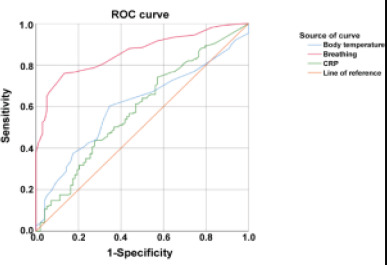 Figure 1
Figure 1| Entry items | Severe pneumonia (n/%) | Non-severe pneumonia (n/%) | X2/Z/t | P | |
|---|---|---|---|---|---|
| gender | man | 291(64.81) | 91 (61.48) | 0.534 | 0.465 |
| woman | 158(35.19) | 57(38.52) | |||
| age | 10.00(3.00.24.00) | 14.50(7.00,36.00) | -4.193 | <0.001 | |
| Length of stay | >7 | 335(25.39) | 20(13.51) | 172.375 | <0.001 |
| ≤7 | 114(74.61) | 128(86.49) | |||
| 90 days of repeated | Yes | 0(0.00) | 28(18.92) | 89.126 | <0.001 |
| hospitalization | No | 449(100.00) | 120(81.08) | ||
| Death | Yes | 5(1.11) | 0(0.00) | 0.592 | 0.442 |
| No | 444(98.89) | 148(100.00) | |||
| Invasive ventilation | Yes | 280(62.36) | 0(0.00) | 173.82 | <0.001 |
| No | 169(37.64) | 148(100.0) | |||
| Stay in ICU | Yes | 167(37.19) | 0(0.00) | 173.82 | <0.001 |
| No | 282(62.81) | 148(100.00) | |||
| History of pregnancy and dilivery | Unspecificness | 321(72.30) | 130(87.84) | 17.486 | 0.002 |
| Premature, very low/low weight baby | 76(17.12) | 9(6.08) | |||
| Intrauterine distress and asphyxia | 6(1.35) | 2(1.35) | |||
| There is a preexisting disease | 5(4.05) | 0(0.00) | |||
| Premature delivery with intrauterine distress | 23(5.18) | 7(4.73) | |||
| Body temperature | 36.90(36.60,37.80) | 36.80(36.50,37.20) | -2.635 | 0.008 | |
| Breathing | 46.00(35.00,55.00) | 28.00(25.00,32.00) | -13.685 | <0.001 | |
| mmHg | Low | 41(9.19) | 6(4.06) | 6.533 | 0.038 |
| Normal | 388(87.00) | 140(94.59) | |||
| High | 17(3.81) | 2(1.35) | |||
| PCT | 0.23(0.10,1.22) | 0.21(0.10,0.58) | -1.401 | 0.161 | |
| CRP | 9.40(2.70,25.70) | 4.30(1.75,16.23) | -3.496 | <0.001 | |
| APTT | 42.35(38.10,46.38) | 42.45(37.78,46.03) | -0.275 | 0.783 | |
| Uric Acid | 239.00(193.25,310.50) | 238.00(174.50,309.50) | -0.940 | 0.347 |
| Variable | Assignment specification |
|---|---|
| Severe pneumonia | Non-severe pneumonia =0, severe pneumonia =1 |
| Age | Original value |
| History of pregnancy and dilivery | Yes =1, no =0 |
| Body temperature | Original value |
| Breathing | Original value |
| Systolic blood pressure on admission | 1= “Low”, 2= “Normal”, 3= “High |
| CRP | Original value |
| PCT | Original value |
| Variable | B | S.E. | Wald |
| OR | 95% confidence interval |
|---|---|---|---|---|---|---|
| Age | 0.009 | 0.008 | 1.123 | 0.289 | 1.009 | 0.993-1.025 |
| History of pregnancy and dilivery | 1.243 | 0.512 | 5.890 | 0.015 | 3.467 | 1.270-9.463 |
| Body temperature | 0.677 | 0.193 | 12.254 | <0.001 | 1.968 | 1.347-2.874 |
| Breathing | 0.192 | 0.027 | 49.035 | <0.001 | 1.212 | 1.148-1.279 |
| Systolic blood pressure on admission | 0.17 | 0.027 | 0.086 | 0.769 | 1.189 | 0.374-3.772 |
| CRP | 0.011 | 0.007 | 2.536 | 0.111 | 1.011 | 0.997-1.025 |
| Constant (quantity) | -31.893 | 7.529 | 17.945 | <0.001 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumonia and Respiratory Infections
Introduction
Pneumonia is a common respiratory tract infection among children, especially infants and young children. It can be classified into mild and severe categories based on disease severity1,2. Mild pneumonia is characterized by mild symptoms, the absence of complications, and a favorable prognosis. Conversely severe pneumonia presents with a rapid onset, significant changes, severe symptoms, and multiple complications, often posing a life-threatening risk to children3. In fact, it is a leading cause of death in children under the age of 5. Therefore, early identification and prediction of severe pneumonia in children are crucial for saving lives4.
The aim of this study is to develop a model capable of effectively identifying severe pneumonia in children at an early stage. This will be achieved by comparing common laboratory indicators between children with ordinary pneumonia and those with severe pneumonia. Currently, the severity grading of pediatric pneumonia primarily relies on modified consensus guidelines for managing community-acquired pneumonia in adults established by the Infectious Diseases Society of America or the American Thoracic Society. This approach is supplemented with early warning scores for children5. However, this method incorporates subjective elements and is not convenient for practical use in a clinical setting. Additionally, it is primarily based on adult standards and heavily relies on the physician's judgment, lacking objectivity. Consequently, there is a shortage of predictive models for severe pneumonia in children.
Therefore, the main objective of this study is to establish a model that can promptly identify severe pneumonia in children using commonly assessed laboratory indicators. By comparing the differences between children with ordinary pneumonia and those with severe pneumonia, this model aims to facilitate rapid clinical decision-making for healthcare professionals. This approach will enhance the objectivity and efficiency of diagnosing severe pneumonia in children, ultimately contributing to better patient outcomes.
Methods
Study Population
The study included children between the ages of 1 month and 14 years who were admitted to Foshan Maternal and Child Health Hospital for pneumonia between January 2017 and June 2022. To ensure standardized classification, community-acquired pneumonia in children was divided into two groups: severe pneumonia and ordinary pneumonia. The classification criteria were based on relevant literature's diagnostic criteria for severe pneumonia. Children with blood system diseases, malignant tumors, severe liver and kidney diseases, autoimmune diseases, and other conditions that could potentially affect the severity of pneumonia (such as congenital heart disease or severe trauma) were excluded from the study to maintain sample homogeneity. The research plan received approval from the Ethics Committee of Foshan Maternal and Child Health Hospital, adhering to the ethical standards outlined in the Helsinki Declaration of medical ethics.
Data Collection
The study subjects were divided into a severe pneumonia group and an ordinary pneumonia group based on the diagnosis of severe pneumonia. Patient information such as name, gender, age in months, length of hospital stay, occurrence of repeated hospitalizations within 90 days, mortality, use of invasive ventilation, ICU stay, birth history, temperature, respiration rate, and admission blood pressure were collected from the hospital's medical record information system. Laboratory indicators on the day of admission for both groups were recorded by referring to the clinical laboratory records. The laboratory indicators included procalcitonin (PCT), C-reactive protein (CRP), activated partial thromboplastin time (APTT), and uric acid. Blood routine indicators were measured using the TEK8520 automatic 5-category blood cell analyzer (Jinan, China), and serum indicators were measured using the Olympus AU400 automatic biochemical analyzer (Tokyo, Japan).
Statistical Analysis
Data was entered into Excel 2010 using double-entry, and Statistical Product and Service Solutions (SPSS) 25.0 software was used for statistical analysis. One-way ANOVA and multiple factor analysis were performed using SPSS 25.0 software. Normally distributed metric data was presented as mean ± standard deviation (mean ± SD), and independent sample t-tests were used for group comparisons. Non-normally distributed metric data was described using median and quartile range, and the non-parametric Mann-Whitney U test was used for group comparisons. Pearson's chisquare test was used for comparison of count data. Receiver operating characteristic (ROC) curves were used to evaluate the operational characteristics of the subjects. Statistical significance was set at P < 0.05 to indicate significant differences.
Results
Univariate analysis of severe pneumonia
The univariate analysis revealed statistically significant differences (P < 0.05) between the two groups in various factors. These factors included age, length of stay, rehospitalization within 90 days, invasive ventilation, Intensive Care Unit (ICU) stay, birth history, body temperature, respiration, blood pressure, procalcitonin (PCT), and C-reactive protein (CRP). However, there were no significant differences in gender, mortality, activated partial thromboplastin time (APTT), and uric acid levels between the two groups (P > 0.05) (Table 1).
Binary logistic regression analysis of severe pneumonia in children
Based on the significant factors identified in the univariate analysis (P < 0.05), a collinearity analysis was conducted to avoid multicollinearity issues. Hospital stay, readmission within 90 days, and ICU admission showed variance inflation factors exceeding 5 and were consequently excluded from further analysis. The remaining predictive factors were included in the binary logistic regression analysis, with the occurrence of severe pneumonia as the dependent variable (Table 2). The results of the logistic regression analysis showed that high body temperature (OR = 1.100, 95% CI: 1.033-1.170) and high respiratory rate (OR = 4.071, 95% CI: 1.355-12.231) were identified as independent risk factors for severe pneumonia in children (P < 0.05). However, age, systolic blood pressure at admission, C-re-active protein (CRP), and procalcitonin (PCT) did not show significant differences (P > 0.05), as shown in Table 3.
ROC curve analysis of body temperature, respiration, and CRP for identifying severe pneumonia in children
Receiver operating characteristic (ROC) curve analysis was performed to evaluate the predictive ability of the binary logistic regression model for severe pneumonia in children, using body temperature, respiration rate, and C-reactive protein (CRP) as independent variables. The results showed that the area under the curve (AUC) for body temperature was 60.39%, indicating moderate predictive performance. The AUC for respiration rate was 85.94%, indicating high predictive performance. Lastly, the AUC for CRP was 58.85%, indicating fair predictive performance (see Figure 1).
ROC curve of severe pneumonia in children
Discussion
Childhood pneumonia is a common and frequently occurring disease in children. It progresses rapidly and is the leading cause of death among children6. Severe pneumonia accounts for 7% to 13% of all pneumonia cases in children. In China, as a densely populated developing country, severe pneumonia in childhood imposes a significant economic and social burden on families and society. Research has shown that severe pneumonia in children under 5 years old contributes to 0.86% of all child deaths annually in China, making the prevention and treatment of this disease a critical challenge7.
Currently, the most commonly used tools for predicting severe pneumonia in children in clinical practice include altered mental status, blood urea nitrogen, respiratory rate, blood pressure, and the pneumonia severity index. However, these evaluation criteria are mainly applied to adults, and the subjective judgment combined with laboratory tests used may not be suitable for diagnosing severe pneumonia in pediatrics. Therefore, early identification and assessment of the risk of childhood pneumonia progressing to severe disease, along with timely monitoring and effective treatment, can improve the prognosis of affected children and reduce the pressure on social security and family burden8.
The single-factor analysis revealed statistically significant differences (P < 0.05) between the two groups in various factors, including age, length of hospital stay, rehospitalization within 90 days, invasive mechanical ventilation, ICU admission, birth history, body temperature, respiratory rate, blood pressure, procalcitonin (PCT), and C-reactive protein (CRP).
As children grow older, their immune system gradually strengthens, reducing the probability of respiratory diseases and the development of severe pneumonia. This finding is consistent with previous research. A longer hospital stay or repeated hospitalizations indicate an unstable condition requiring further treatment and care. Invasive mechanical ventilation is used to improve oxygenation and ventilation, correcting hypoxemia and hypercapnia. Children requiring invasive mechanical ventilation usually exhibit more severe hypoxia, indicating a higher likelihood of developing severe pneumonia.
Moreover, children with a birth history have a higher probability of developing severe pneumonia compared to those without such a history. This finding aligns with multiple studies, as children born prematurely, with low birth weight, immunodeficiency, or congenital heart disease, have relatively weaker immune systems. In the case of lung infections, their ventilation function may be further compromised, promoting the development of pneumonia and ultimately leading to severe pneumonia.
Body temperature, respiratory rate, and blood pressure are vital signs that indicate the severity and criticality of a patient's condition. Therefore, when a patient develops severe pneumonia, it signifies that the condition has progressed to a more severe and critical stage, consistent with previous findings. The concentrations of PCT and CRP are positively correlated with the severity of the inflammatory response and can serve as markers for the early diagnosis of sepsis. This observation aligns with multiple studies8.
Overall, these findings highlight the significance of various factors in the development and severity of pneumonia in children, providing valuable insights for clinical practice and further research.
There are limitations to this study. First, the cases included in this study were from a single hospital in Foshan City, and data from other hospitals were not included in the analysis, making external validation impossible. Therefore, further expansion of the sample size is needed to improve the accuracy of the prediction model. Second, other factors that may affect the disease, such as body mass index, white blood cell count, acute physiology and chronic health evaluation II (APACHE II), and lactate dehydrogenase, were not included in the analysis. Third, some predictive factors (such as whether the hospital stay was longer than seven days and whether the patient had been rehospitalized within 90 days) overlap with each other. Therefore, further multicenter, large-sample, prospective studies are needed in different hospitals to enhance the accuracy and adaptability of the model.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ness-Cochinwala M Kobaitri K Totapally BR Characteristics and Outcomes of Children With Necrotizing Pneumonia Pediatr Crit Care Me 202122 e 640e 64310.1097/PCC.000000000000279334284428 · doi ↗ · pubmed ↗
- 2Goyal JP Kumar P Mukherjee A Das RR Bhat JI Ratageri V Risk Factors for the Development of Pneumonia and Severe Pneumonia in Children Indian Pediatr 2021581036103934837363 · pubmed ↗
- 3Gross CJ Porter JJ Lipsett SC Monuteaux MC Hirsch AW Neuman MI Variation in Management and Outcomes of Children With Complicated Pneumonia Hosp Pediatr 2021112072143357974910.1542/hpeds.2020-001800 · doi ↗ · pubmed ↗
- 4Yu HR Hsu JH Editorial: Emerging Pneumonia in Children Front Pediatr 202198130343495699310.3389/fped.2021.813034 PMC 8692733 · doi ↗ · pubmed ↗
- 5Lipsett SC Hirsch AW Monuteaux MC Bachur RG Neuman MI Development of the Novel Pneumonia Risk Score to Predict Radiographic Pneumonia in Children Pediatr Infect Dis J 20224124303469425410.1097/INF.0000000000003361 · doi ↗ · pubmed ↗
- 6Macpherson L Ogero M Akech S Aluvaala J Gathara D Irimu G Risk factors for death among children aged 5-14 years hospitalised with pneumonia: a retrospective cohort study in Kenya Bmj Glob Health 20194 e 171510.1136/bmjgh-2019-001715 PMC 673057431544003 · doi ↗ · pubmed ↗
- 7Zou L Yi L Yu J Song Y Liang L Guo Q Adenovirus infection in children hospitalized with pneumonia in Guangzhou, China Influenza Other Resp 202115273310.1111/irv.12782 PMC 776796132761743 · doi ↗ · pubmed ↗
- 8Yang AP Liu J Yue LH Wang HQ Yang WJ Yang GH Neutrophil CD 64 combined with PCT, CRP and WBC improves the sensitivity for the early diagnosis of neonatal sepsis Clin Chem Lab Med 2016543453512635192510.1515/cclm-2015-0277 · doi ↗ · pubmed ↗