Minimal immune response after transplantation of a cryopreserved human amniotic membrane on the ocular surface
Jean-Baptiste Baudey, Lauriana Solecki, Christophe Picard, Bastien Mathéaud, Pauline Jamain, Isabelle Jollet, Lucas Hubert, Alain Coaquette, Adeline Desanlis, Xavier Lafarge, Pascal Pedini, Florelle Gindraux

TL;DR
This study found that transplanting cryopreserved human amniotic membrane on the eye causes minimal immune response, supporting its long-term safety.
Contribution
First clinical study to assess anti-HLA and anti-HLA-G antibodies after cryopreserved human amniotic membrane transplantation.
Findings
Only one patient developed new antibodies after transplantation.
Six patients showed a temporary increase in preformed antibodies.
No anti-HLA-G antibodies were detected before or after the procedure.
Abstract
Human amniotic membrane (hAM) is considered to have low immunogenicity since Akle et al. reported no anti-HLA antibodies (Abs) in four volunteers after subcutaneous grafting of fresh hAM in 1981. But the sensitivity of the detection methods has significantly improved since then. Furthermore, hAM graft is a massive local input of allogenic HLA-G whose potential immunogenicity has never been assessed. The objective of this study was to look for the presence of anti-HLA class I, II, and anti HLA-G Abs at 1 and 3 months after hAM transplantation on the ocular surface. Twenty-three patients who required a hAM graft on the ocular surface (cornea and/or conjunctiva) for any indication were enrolled in this prospective clinical study. Sera were collected on the day of transplantation and at 1- and 3-months post-transplantation (M0, M1, M3). Anti-HLA class I, and II Abs were assessed using the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
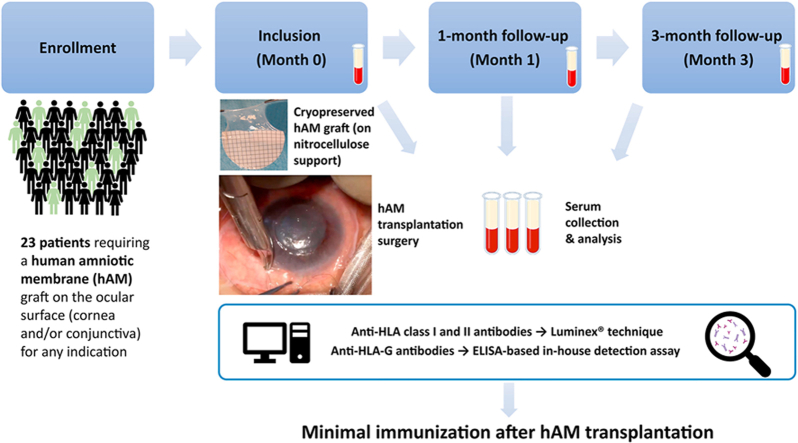 Figure 1
Figure 1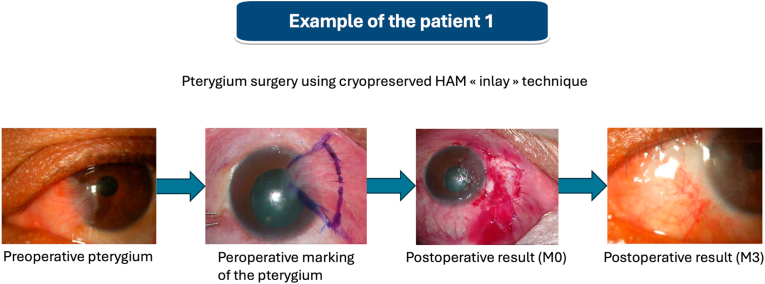 Figure 2
Figure 2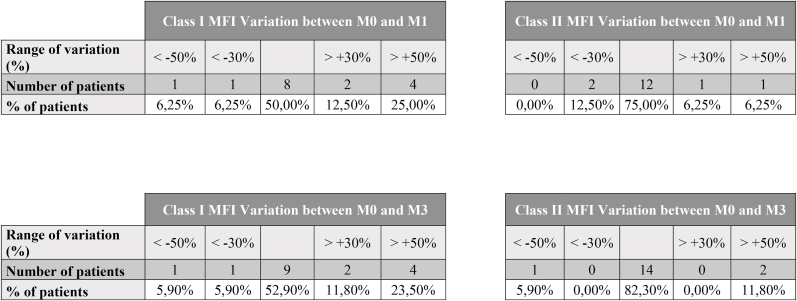 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive System and Pregnancy · Corneal Surgery and Treatments · Organ and Tissue Transplantation Research
Introduction
1
The human amniotic membrane (hAM) is defined as the membrane that forms the wall of an embryo/fetal annex known as the amnion or amniotic sac. This membrane encloses the amniotic cavity and contains amniotic fluid [1]. Histologically, the tissue is composed of a single epithelial layer containing hAM epithelial cells (hAECs), a thick basement membrane, and an avascular stroma containing hAM mesenchymal stromal cells (hAMSCs). It meets the fundamental criteria of tissue engineering scaffolds, being a three-dimensional, biodegradable, and biocompatible matrix enriched with growth factors and stem cells [2,3]. It has been used extensively as a scaffold in clinical tissue engineering applications and has also been developed into advanced formats including hAM-based hydrogels, bioinks, nanoparticles, and hybrid or multilayer composite forms [2,4,5].
The first documented instance of surgical use of hAM was in 1910 by Davis, who employed it as a material for skin grafting [6]. Since then, its applications have expanded significantly to the field of ophthalmology. In 1940, De Roth reported the first use of hAM as a biomaterial for conjunctival reconstruction [7]. Currently, it is commonly used in ophthalmology to reconstruct tissue defects on the ocular surface following the excision of a conjunctival tumor or even corneal perforation, and to treat various ocular pathologies, such as neurotrophic keratitis and pterygium [8,9]. hAM has mechanical, anti-infective, anti-fibrotic, regenerative, and anti-inflammatory properties [10]. When used as a graft, it provides mechanical support during healing and has the ability to reduce scarring and inflammation [10,11]. Its cellular components, cytokines and growth factors also have anti-inflammatory, anti-microbial, and either anti-angiogenic or angiogenic properties (depending on the application), as well as analgesic effects [[10], [11], [12], [13], [14]].
The viability of hAM as a transplantable tissue is well-documented [15,16]. Harvesting and storage procedures are well-established [17]. Furthermore, it has been demonstrated that the usual processes applied to hAM—such as decellularization, de-epithelialization, lyophilization, or dehydration [18]—as well as more advanced processing methods [[19], [20], [21]], significantly impact cell viability, often resulting in the presence of residual DNA, cell-associated proteins, and other cellular debris. It is still unclear whether these processing methods affect the inflammatory reaction.
In routine use, hAM transplantation is well tolerated, with clinical immunological and inflammatory reactions rarely observed. It is said to have low immunogenicity [[22], [23], [24]] with a high margin of clinical safety given the low number of serious adverse reactions relative to the high number of transplants [25,26]. Therefore, little biological testing has been performed to detect hAM immunogenicity, and none is required in clinical practices [14,17,[27], [28], [29], [30]]. The extant literature on the subject is limited to a single study [22]. Akle et al. observed a mild clinical and histological inflammatory reaction following fresh hAM grafts on the skin of seven volunteers. However, the authors were unable to determine whether this reaction was due to healing or to graft rejection. We previously summarized the rare and sometimes contradictory information regarding hAM immunogenicity and the methods used for its detection [31]. Kubo et al. reported the presence of human leukocyte antigens (HLA)-A, -B, -C, and more specifically -G in the hAECs. Additionally, a mild inflammatory reaction was observed in rats following xenotransplantation of hAM [24]. Similarly, Hammer et al. demonstrated that an anti-pan HLA antibody (Ab) strongly reacted with hAECs [32]. In clinical practice, there have been four documented cases of hypopyon after single or multiple hAM grafts from the same donor on the ocular surface in the same patient [[33], [34], [35], [36]], making it possible that an immune reaction occurred although no biological evidence exists.
Since the 1980s and the study of Akle et al., innovative and highly sensitive techniques have been developed to detect anti-HLA Abs. We have extensive experience in HLA detection [[37], [38], [39], [40], [41], [42], [43], [44], [45], [46], [47]] and previously described methods to determine whether antibody-mediated immune response is triggered after hAM grafting in a clinical setting. Techniques such as the Luminex Single Antigen® to detect anti-HLA Class I and II Abs and the modified MAIPA assay (Monoclonal Ab-specific Immobilization of Platelet Antigens, ApDIA®) to detect Abs directed against the non-classical HLA molecule HLA-G provide modern options for assessing hAM immunogenicity [48] since a mild humoral immune response might be induced by hAM allografting, particularly against these antigens (Ags).
The aim of our study was to assess the immunogenicity of hAM transplantation on the ocular surface with modern sensitive techniques for detecting anti-HLA Abs.
Materials and methods
2
Ethics approval
Ethics approval for the study was obtained from the “Comité de protection des personnes Sud-Est I″ committee (2023-A01447-38). Patients were enrolled in the study after providing free and informed written and oral consent.
Study design
2.1
This was a prospective cohort study conducted at the University Hospital of Besançon in the Department of Ophthalmology between August 2022 and September 2023, in collaboration with the French Blood Establishment of Bourgogne Franche-Comté (BFC), the French Blood Establishment of Nouvelle-Aquitaine (EFS NAq) and the French Blood Establishment of Provence Alpes Côte d'Azur (EFS PACA).
Eligibility criteria
2.2
The inclusion criteria for the study were as follows: patients over the age of 18 who could consent to the study protocol and who required a hAM graft on the ocular surface (cornea and/or conjunctiva) for any indication.
Patients were excluded if they met any of the following criteria: under the age of 18, pregnant or had given birth less than 6 months prior, history of organ transplantation, had received blood products within the last 6 months, were receiving immunosuppressive or immunomodulatory treatments, or were unable to provide consent or refused to participate in the study protocol.
Cohort characteristics
2.3
A comprehensive analysis of the patients' medical records was conducted to collect relevant data, including age, gender, medical history, parity, gestational age for women, vaccinations, transfusions, treatments, surgical indication, surgery date, surgery type, and clinical changes over the 3-month postoperative follow-up period. The occurrence of local inflammatory reactions or graft failure was meticulously documented.
hAM preservation and preparation
2.4
The hAM was cryopreserved and obtained from AICT bank from EFS BFC at Besançon. A piece of hAM 4.7 cm in diameter was transported with dry ice blocks to ensure it stayed frozen at −80 °C. The allografts were stored in glycerol on a nitrocellulose support, with the epithelial side facing the support. Upon receipt, they were thawed for 2 h at room temperature followed by three, 5 min rinses in saline injection solution.
Surgical procedures and follow-up
2.5
Surgery was performed under local or general anesthesia. Different surgical techniques (multilayer, inlay, overlay) were used depending on the surgical indication. All patients were treated with anti-inflammatory eye drops and ointments for 1 month after the surgery. Postoperative visits were scheduled at 15 days, 1 month, and 3 months to monitor signs of rejection or unusual local inflammatory reactions and to ensure successful treatment of the initial pathology.
Study visits were planned at baseline (M0), one month (M1), and three months (M3), with interim checks conducted at the clinician's discretion.
Blood collection
2.6
Three blood samples were collected. The first (M0) was taken in the operating room prior to hAM transplantation and served as a reference to identify any pre-existing anti-HLA Abs in the graft recipients, which could have developed during pregnancy or prior immunization. A second blood sample was taken at 1 month (M1), corresponding to the hypothetical reappearance of preformed anti-HLA Abs after stimulation. A third sample was scheduled at 3 months (M3) to study the kinetics of anti-HLA Abs, to confirm their presence and assess de novo immunization. This 3-months follow-up period is consistent with immunological surveillance recommendations after exposure to biological materials. For example, French regulations mandate the screening for irregular red cell Abs (agglutinins) 3 months after the last blood transfusion. Similarly, French national expert society [49] recommends reassessing the anti-HLA Ab profile 3 weeks after a blood transfusion (in context of pre Hematopoietic Stem Cell Transplantation). hAM grafts are typically resorbed within a maximum of 4 weeks [50]. Given the rapid and transient nature of the graft, it is unlikely that the tissue would elicit a delayed immune response if one has not occurred during the first three months. Blood samples were collected in a dry tube (5–7 mL), centrifuged, and decanted. Sera were then stored at −20 °C in a serum bank until analysis.
Anti-HLA class I, II and G analysis
2.7
Anti-HLA class I and II Abs detection was performed using Luminex® Single Antigen equipment at the EFS NAq and the EFS PACC laboratories. Briefly, the samples were incubated with a mixture of fluorescent polystyrene microbeads, each bead being coated with a high density of a single HLA Ag. The beads were washed through a filter plate. Then, Ab binding was revealed by fluorescent anti IgG secondary Ab. The bead suspension was analyzed by a Luminex® instrument. Each bead was identified through its intrinsic fluorescence. The signal linked to the quantity of Abs fixed on it was quantified as Mean Fluorescence Intensity (MFI) [51]. A MFI superior to 1000 was considered a positive result. This technique is particularly sensitive and can detect a specific signal as low as 500 of MFI. Around 100 HLA class I Ags and 100 HLA class II Ags were tested by the kit with very high sensitivity. These Ags correspond to the most frequent HLA alleles in the European population. This technique is the international reference method for anti-HLA Ab detection in medical contexts such as HSCT or solid organ transplantation [52]. For each patient and timepoint, we calculated Virtual Panel Reactive Abs (vPRA) using Eurotransplant's Virtual PRA Calculator Online Tool at the 1000 MFI threshold. The vPRA is based on the European HLA typing database. For each patient, vPRA was determined for class I and class II Abs at M0, M1 and M3. In addition, a qualitative analysis of the Ab profiles was performed. Abs profiles were independently reviewed by two expert biologists from our laboratory to determine de novo Abs apparition. Then, Abs MFI data were reviewed to determine if significant variations of the existing Abs MFI occurred during the post-transplantation period. For preformed Abs, a 50 % variation of MFI between M0 and M1 or M3 was considered significant as previously established [53].
In order to detect anti-HLA-G Abs, we modified the MAIPA kit (ApDIA®) so to detect Abs directed against HLA-G associated with β2m. [54]. This kit is based on the ELISA principle and allows the detection and identification of auto/allo anti-platelet glycoprotein Abs and anti-classical class I HLA Abs in serum using a platelet panel and platelet-Ag immobilized by a monoclonal Ab. Its sensitivity is similar to Luminex® Single Ag for the detection of classical HLA class I Abs [54]. All the MAIPA reagents were unchanged for our modified protocol except the platelet panel which was replaced by HLA-G transfected K562 cells and the capture Ab which was replaced by MEM-G9 (MA1-19014, Invitrogen). Briefly, patient serum was incubated with HLA-G–transfected cells, allowing the formation of a cell–patient anti-HLA-G Ab complex. After incubation with MEM-G/9 (mouse anti HLA-G), a tripartite complex (MEM-G/9–cell–patient anti-HLA-G Ab) forms. Following cell lysis, this tripartite complex was captured on the ELISA plate by a goat anti-mouse Ab recognizing MEM-G/9. A goat anti-human Ig HRP Ab was used to specifically detect patient Abs.
This method has been validated for anti-HLA-G Ab detection and published in a lung transplant cohort [48]. Each serum was tested in parallel on wild-type K562 cells and HLA-G transfected K562 cells. Each serum was first tested by a screening MAIPA using a pool of three transfected cell lines (HLA-G∗01:01, HLA-G∗01:04 and HLA-G∗01:06 cells). Serum samples were flagged as suspicious based on the optical density (OD) value obtained, taking into account the OD obtained with the corresponding wild-type control well. Suspicious samples (combination of OD > 0.1 and OD (HLA-G)/OD (wild type) ratio >2) were checked by an identification MAIPA using G101, G104 and G106 cells separately to increase sensitivity to a particular HLA-G molecule and to determine Ab specificity. The use of non-transfected K562 cells allowed us to evaluate the background noise of our system. Each plate included the positive and negative control sera of the MAIPA kit and a in-house positive control, tested on transfected and untransfected cells, as well as two blank wells. The assay was considered valid if the OD of the negative controls was <0.1 and if the OD of the positive controls was >0.2. Given that our test mimics the steps of the MAIPA assay, each plate included the MAIPA kit platelet control pool and served as an internal control for the technical steps (incubation, washing, flicking). The OD of the platelet control pool had to be within the kit's expected values to validate the entire analytical process.
Outcome measures
2.8
The primary outcome measure was the presence and identification of Class I, II and G anti-HLA Abs in serum samples at M1 and M3 after hAM transplantation on the ocular surface.
Statistical analysis
2.9
Descriptive statistics were applied to analyze numerical and nominal data, while inferential statistics were used to assess differences in MFI and PRA from M0 to the M1 and M3 follow-up visits.
Results
3
Patient characteristics
3.1
Twenty-three patients who underwent hAM transplantation were enrolled between August 2022 and September 2023. A total of 69 serum samples were collected at M0, M1 and M3.
The characteristics of the cohort are presented in Table 1. The patient population was predominantly male (65 %). The median age was 62 years old (55 years old for male participants and 66.5 years old for female participants). The most frequent indication for hAM was pterygium surgery with an inlay graft technique (20 patients, 87 %). Four patients (17 %) had a history of transfusion. Six patients (26 %) had a history of pregnancy. Nine patients (39 %) had undergone an immunizing event prior to hAM transplantation (Fig. 1).Table 1. Description of the characteristics of the study cohort (M Male, F Female, NA not applicable).Table 1. PatientAgeSexIndicationGraft surgical techniqueLocationTransfusionPregnancy172MPterygiumInlayConjunctivaYes (In 1992)NA277MPterygiumInlayConjunctivaYes (In 2013)NA381FCorneal ulcerSandwichConjunctiva-corneaNo5 times476MPterygiumInlayConjunctivaNoNA556MPterygiumInlayConjunctivaNoNA650MPterygiumInlayConjunctivaNoNA774MPterygiumInlayConjunctivaNoNA826MPterygiumInlayConjunctivaNoNA948FRosaceaInlayConjunctivaNo01052MPterygiumInlayConjunctivaYes (In 1990)NA1155MPterygiumInlayConjunctivaNoNA1274MCorneal ulcerSandwichConjunctiva-corneaNoNA1362MPterygiumInlayConjunctivaNoNA1473FPterygiumInlayConjunctivaNo3 times1577FPterygiumInlayConjunctivaYes (In 1971)5 times1632FConjunctival naevusInlayConjunctivaNo01771FPterygiumInlayConjunctivaNo6 times1844MPterygiumInlayConjunctivaNoNA1962FPterygiumInlayConjunctivaNo2 times2062FPterygiumInlayConjunctivaNo3 times2149MPterygiumInlayConjunctivaNoNA2255MPterygiumInlayConjunctivaNoNA2333MPterygiumInlayConjunctivaNoNAFig. 1An example of pre, intra- and postoperative clinical findings after pterygium surgery using cryopreserved human amniotic membrane (hAM) “inlay” technique in patient 1.Fig. 1
During the 3-month follow-up, no major local inflammatory reaction or clinical rejection were observed.
Anti-HLA class I, II and G analysis
3.2
Abs assigned at the MFI threshold of 1000, along with their respective MFI values, are summarized in Table 2. With the exception of the appearance of B82 in patient 17, no de novo Ab development was observed in our patients. Five patients showed a significant increase (>50 %) of MFI for preformed Abs between M0 and M3: patients 4, 13 and 16 for class I Abs; patient 20 for class II Abs; patient 23 for both class I and II Abs. For patient 4, 13 and 23, the MFI increases were already significant by M1 contrary to patient 16 and 20. In addition, Patient 14 exhibited a transient significant increase of class I Abs MFI at M1 that regressed by M3 (Fig. 2).Table 2. Patients immunization follow-up based on Luminex Single Antigen (One lambda) results. Antibody specificities and MFI (Mean Fluorescence Intensity) are displayed for each timepoint. Positivity threshold is 1000 of MFI. Antibodies with MFI >1000 are highlighted in bold and were used for vPRA calculation. Antibodies which did not exceed an MFI of 1000 at all time points, are reported but not highlighted in bold.Table 2. PatientHLA classAnti-HLA Abs specificity (and MFI) at M0Anti-HLA Abs specificity (and MFI) at M1Anti-HLA Abs specificity (and MFI) at M3Patient 1Class INegNegNegClass IINegNegNegPatient 2Class INegNegNegClass IINegNegNegPatient 3Class INegNegNegClass IINegNegNegPatient 4Class IB45 (1710)B50 (440)B45 (2690)B50 (810)B45 (4520)****B50 (2310)Class IINegNegNegPatient 5Class IB46 (1570)****B46 (1510)****B46 (1550)Class IINegNegNegPatient 6Class IA∗11:02 (2260)****A∗11:02 (3390)****A∗11:02 (2880)Class IIDRB5∗01:01 (1700)****DRB5∗01:01 (1150)****DRB5∗01:01 (1720)****Patient 7Class IB45 (2350)****B45 (2750)****B45 (1740)Class IINegNegNegPatient 8Class I**A26 (1880)****A43 (1610)****A66 (1510)****A25 (1300)****Cw17 (1920)**A26 (920)A43 (690)A66 (560)A25 (790)Cw17 (980)A26 (1550)****A43 (1270)****A66 (1160)****A25 (1180)****Cw17 (1790)Class IINegNegNegPatient 9Class IA66 (660)B8 (680)**Cw17 (3510)**A66 (850)**B8 (1040)****Cw17 (4660)****A66 (1030)**B8 (980)Cw17 (4300)Class IINegNegNegPatient 10Class IA25 (990)B75 (2950)****A25 (1130)****B75 (2540)A25 (620)B75 (1910)Class IIDQA1∗03 (2170)****DP19 (3160)****DQA1∗03 (2190)****DP19 (3460)****DQA1∗03 (2020)****DP19 (3170)****Patient 11Class ICw1 (1150)Cw1 (960)Cw1 (210)Class IINegNegNegPatient 12Class IB82 (820)B82 (930)B82 (1160)Class IINegNegNegPatient 13Class IB63 (640)B63 (970)**B63 (1020)Class IINegNegNegPatient 14Class IA24 (4490)A23 (3780)A2 (610)A69 (400)A68 (350)B48 (5620)B60 (2370)B81 (820)A24 (8670)A23 (7610)A2 (1520)A69 (1220)A68 (1140)B48 (8600)B60 (4080)B81 (1590)A24 (6260)A23 (5350)A2 (1040)A69 (750)A68 (700)B48 (6560)B60 (3300)B81 (1240)Class IIDR9 (4320) DR4 (3360) DR18 (2420) DR52 (2460) DR17 (1940) DR13 (1200) DR11 (1150) DR14 (900) DR8 (770) DR7 (1180) DQ7 (6790) DQ9 (4900) DQ8 (5080) DQ4 (880)DR9 (4400) DR4 (3870) DR18 (3560) DR52 (2930) DR17 (2820) DR13 (1510) DR11 (1430) DR14 (1300) DR8 (1170) DR7 (1090) DQ7 (8600) DQ9 (6190) DQ8 (6060) DQ4 (1310)DR9 (2820) DR4 (2140) DR18 (1740) DR52 (1700) DR17 (1510) DR13 (840) DR11 (770) DR14 (600) DR8 (540) DR7 (630) DQ7 (5830) DQ9 (4380) DQ8 (4480) DQ4 (620)Patient 15Class INAB57 (1520)****B57 (1780)Class IINADR9 (940)DR9 (1180)****Patient 16Class IA1 (5120)****A30 (4410)****A3 (2180)****A31 (1990)****A36 (1520)****A32 (1350)****A11 (1290)****A74 (1210)****B73 (5540)**B47 (230)Cw18 (930)**A1 (6620)****A30 (6010)****A3 (2790)****A31 (2280)****A36 (2000)****A32 (1310)****A11 (1240)****A74 (1410)****B73 (7060)B47 (470)Cw18 (1540)****A1 (8030)****A30 (7330)****A3 (4270)****A31 (4010)****A36 (2970)****A32 (2530)****A11 (3120)****A74 (2490)****B73 (7570)****B47 (1160)****Cw18 (1690)Class IINegNegNegPatient 17Class IA80 (3420)****B37 (1420)**B82 (200)**Cw17 (1560)****A80 (2620)****B37 (1170)**B82 (480)**Cw17 (1170)****A80 (2830)**B37 (900)**B82 (2330)Cw17 (980)Class IIDR7 (2340)****DR53 (2430)****DR7 (1660)****DR53 (2190)DR7 (900)DR53 (1920)****Patient 18Class IB76 (570)B76 (1270)B76 (630)Class IINegNegNegPatient 19Class IA33 (3800)A66 (2220)Bw6 (14200)B51 (4970)B52 (1370)B59 (1230)Cw5 (10320)Cw18 (1580)Cw6 (1020)NAA33 (3470)A66 (1920)Bw6 (13770)B51 (4430)B52 (1230)B59 (1160)Cw5 (9510)Cw18 (1360)Cw6 (930)Class IIDR11 (13450) DRB1∗13:03 (12240) DR8 (10520) DR4 (5610) DQ7 (>20000) DQ9 (18610) DQ8 (18120) DQ2 (14920) DQ4 (10870)NADR11 (13040) DRB1∗13:03 (11440) DR8 (10460) DR4 (5240) DQ7 (>20000) DQ9 (17770) DQ8 (17820) DQ2 (14850) DQ4 (11330)Patient 20Class IB53 (17760)****B35 (17710)****B51 (15660)****B78 (14490)****B75 (9090)****B18 (3740)****Cw17 (1040)****B53 (17910)****B35 (18880)****B51 (16230)****B78 (14710)****B75 (8140)****B18 (2770)Cw17 (740)B53 (15920)****B35 (17250)****B51 (14300)****B78 (13220)****B75 (7640)****B18 (2980)Cw17 (670)Class IIDQ8 (730)DQ9 (610)DQ8 (610)DQ9 (440)DQ8 (1210)****DQ9 (1690)****Patient 21Class INegNegNegClass IINegNegNegPatient 22Class IB75 (4650)****B75 (3970)****B75 (4310)Class IIDR1 (1120)****DR52 (2750)****DR1 (1610)****DR52 (3870)****DR1 (1570)****DR52 (3330)****Patient 23Class ICw17 (1280)****Cw17 (2800)****Cw17 (2000)**Class IIDR53 (650)**DQ9 (1460)****DQ8 (1450)****DR53 (1140)****DQ9 (6880)****DQ8 (6900)**DR53 (600)**DQ9 (2650)****DQ8 (2690)**Fig. 2. Distribution of patients according to the range of MFI variation of the immunodominant Ab. The figure shows the number of patients in each MFI variation range and the corresponding percentage of patients within the sensitized cohort between M0 and M1 (n = 16) and between M0 and M3 (n = 17).Fig. 2
vPRA data are summarized in Table 3. Significant disparity was observed in the initial PRAs, with higher values recorded for the female participants compared to the male ones (mean 32.7 % vs 5.9 %, respectively; p = 0.043). For some patients, important variations of vPRA values occurred during follow up. The most noticeable variations involved antibodies near the positivity threshold (MFI: 1000), which fluctuated around this cutoff from one sample to another.Table 3. Patients immunization follow-up based on class I and class II virtual Panel Reactive Antibody (vPRA, Eurotransplant, threshold used for calculation: MFI >1000) before transplantation (M0), at 1 month postoperative (M1) and 3 months postoperative (M3) (∗no significant modification of the specificities, NA non-available data, M Male, F Female).Table 3. PatientGenderPRAM0M1M3PatientGenderPRAM0M1M3Patient 1MPRA class I0,00 %0,00 %0,00 %Patient 13MPRA class I0,00 %0,00 %0,87 %PRA class II0,00 %0,00 %0,00 %PRA class II0,00 %0,00 %0,00 %Patient 2MPRA class I0,00 %0,00 %0,00 %Patient 14FPRA class I29,00 %71,93 % ∗67,26 %PRA class II0,00 %0,00 %0,00 %PRA class II90,20 %92,08 %84,06 %Patient 3FPRA class I0,00 %0,00 %0,00 %Patient 15FPRA class INA6,62 %6,62 %PRA class II0,00 %0,00 %0,00 %PRA class IINA0,00 %1,83 %Patient 4MPRA class I0,84 %0,84 %3,2 % ∗Patient 16FPRA class I69,10 %69,12 %69,16 %PRA class II0,00 %0,00 %0,00 %PRA class II0,00 %0,00 %0,00 %Patient 5MPRA class I0,04 %0,04 %0,04 %Patient 17FPRA class I4,76 %4,76 %1,88 % ∗PRA class II0,00 %0,00 %0,00 %PRA class II44,80 %44,80 %40,05 %Patient 6MPRA class I0,00 %0,00 %0,00 %Patient 18MPRA class I0,00 %0,00 %0,00 %PRA class II23,84 %23,84 %23,84 %PRA class II0,00 %0,00 %0,00 %Patient 7MPRA class I0,84 %0,84 %0,84 %Patient 19FPRA class I97,12 %NA93,92 %PRA class II0,00 %0,00 %0,00 %PRA class II81,78 %NA81,78 %Patient 8MPRA class I12,50 %0 % ∗12,50 %Patient 20FPRA class I40,60 %39,16 %39,16 %PRA class II0,00 %0,00 %0,00 %PRA class II0,00 %0,00 %25 % ∗Patient 9FPRA class I1,83 %21,96 % ∗2,11 %Patient 21MPRA class I0,00 %0,00 %0,00 %PRA class II0,00 %0,00 %0,00 %PRA class II0,00 %0,00 %0,00 %Patient 10MPRA class I0,08 %4,08 % ∗0,08 %Patient 22MPRA class I0,08 %0,08 %0,08 %PRA class II27,58 %27,58 %27,58 %PRA class II77,40 %77,40 %77,40 %Patient 11MPRA class I7,41 %0 % ∗0,00 %Patient 23MPRA class I1,83 %1,83 %1,83 %PRA class II0,00 %0,00 %0,00 %PRA class II25,00 %45 % ∗25,00 %Patient 12MPRA class I0,00 %0,00 %0,00 %PRA class II0,00 %0,00 %0,00 %
Anti-HLA-G analysis
3.3
OD results for our adapted MAIPA-assay are summarized in Table 4. No anti HLA-G Abs were detected in the cohort's serum samples, neither prior to transplantation (M0) nor at M1 or M3. Patient 7 at M0 and patients 10 and 11 at M1 had suspicious results but these results were not confirmed by the identification MAIPA assay.Table 4. Optical density (OD) values for modified MAIPA assay before transplantation (M0), at 1 month postoperative (M1) and 3 months postoperative (M3) on Wild Type cells and HLA-G transfected pooled cells (∗not confirmed, NA non-available data).Table 4. PatientM0M1M3PatientM0M1M310,0350,0260,045130,0820,0210,0160,0290,0180,0140,0850,0440,02620,0890,0170,020140,1240,0310,0270,0350,0150,0200,1070,0380,03730,0790,0680,04015NA0,0310,0120,1290,0270,030NA0,0690,02240,0990,0120,063160,0830,0330,0580,1110,0170,0660,0890,0360,04250,0490,1040,021170,1380,0450,0280,0650,0200,0190,1290,0290,02060,1590,0100,091180,0530,0540,0280,1140,0160,1050,0920,0600,02670,1360,0220,031190,080NA0,135**0,264∗0,0240,0630,056NA0,09880,0310,0190,024200,0150,0600,0930,0330,0340,0620,0360,0630,03690,0890,0630,038210,0650,0700,1580,1690,0410,0520,0780,0520,093100,3870,0590,097220,1110,0600,0300,1200,125∗0,0740,0710,0950,035110,0540,1050,081230,0750,0140,0320,1020,314∗**0,0210,0850,0110,044120,0490,0210,0680,0670,0550,096OD on Wild Type cells.OD on HLA-G transfected cells pool.
Discussion
4
This is the first study to describe anti-HLA-I, -II and -G antibodies in a clinical setting of hAM transplantation using highly sensitive methods. The hAM used for grafting in our 23 patients were not specifically tested for their expression of classical HLA or HLA-G before the transplantation. However, the expression of these Ags by amniotic membranes, including after processing and preservation, has been well demonstrated in previous studies [24,32].
Classic anti-HLA class I and II Abs
4.1
In most patients (16/23), no change in the profile of anti-classical HLA Abs was observed at M1 or M3 post-transplantation compared to M0, despite using a high-sensitivity detection technique (Table 2). De novo Abs apparition occurred in only one patient: patient 17 developed anti HLA-B82 Abs at M3. But B82 in an extremely rare Ag in the general population making it unlikely to represent a specific reaction against the donor.
The present study has an important limitation regarding the interpretability of the results: we were unable to retrieve the HLA typing of the placentas used for hAM recovery. Therefore, we could not determine donor-specific Abs (DSA). Instead, we relied on careful analysis of the MFI data at each timepoint and on the vPRA. Although the vPRA is routinely used in transplantation as a reflection of the patient's overall immunization status, it has some limitations. For instance, it may remain unchanged despite an increase in MFI values or, on the contrary, change dramatically according to the MFI cut-off used for calculation. The apparent vPRA variation seen in 9 patients (Table 3: patients 4, 8, 9, 10, 11, 14, 17, 20, and 23) can be explained by low MFI Abs that were fluctuating slightly below or above the 1000 MFI threshold depending on the timepoint. Therefore, no significant variation in vPRA was observed over time in any of the 23 patients.
Interestingly, Patients 4, 13, 16, 20 and 23 had a significant increase of performed Abs MFI value between M0 and M3. Also, patient 14 showed a transient increase of the MFI which was not confirmed at M3.(Fig. 2). These results are difficult to interprete in the absence of the hAM typings. It could be either an increase following a specific stimulation of preformed Abs by the graft or, since these Abs are preformed, the increase could reflect non-specific external factors such as the patient's hydration status at the time of sampling or an inflammatory state which can boost all preformed Abs non-specifically. In these patients, we observe a global increase of the MFI of all the preformed Abs, which is not in favor of a specific stimulation, especially when the MFI increase in transient. The Luminex® Single Antigen method is known for having an important coefficient of variation, especially for low MFI results which is the case for Patient 13 and 20. In addition, patients with high levels of immunization such as Patient 14 or 16 frequently display MFI fluctuations during long term follow-up for example on organ transplant waiting list. Class II Abs MFI elevation observed in Patients 20 and 23 also seems unrelated to the hAM itself, since this tissue lacks the expression of HLA class II antigens [55].
Therefore, given that no local inflammation or adverse event was reported during the 3 months follow-up period, the Abs profile changes noted in some patients don't apparently have a clinical relevance in the context of hAM transplantation on the ocular surface. However, the observed increases in MFI may have implications for a subsequent organ transplantation. For example, in France, Abs with an MFI exceeding 2000 are considered a contraindication for transplantation with a graft expressing the corresponding antigen.
Thus our results, showing minimal anti HLA humoral response corroborate and update the findings from the 1980s [22]. The low expression of classical HLA molecules by the hAM and the low vascularization of the graft are widely accepted explanations for the lack of immunization in this context, despite the otherwise high immunogenicity of HLA molecules [9,24]. The abundant presence of HLA-G in the hAM graft likely induces local immune tolerance. The immunomodulatory properties of HLA-G are well documented. Binding of HLA-G to human inhibitory receptors Ig-like transcript 2 and 4 (ILT2 and ILT4) receptors, which are expressed by a wide range of immune effectors, induces phenotypic changes and lymphocyte anergy [56]. A tolerogenic microenvironment forms around cells expressing HLA-G, which benefits patients in the context of corneal and organ transplantation but harms them in tumor settings [57,58].
Anti-HLA-G Abs
4.2
Since hAM transplantation is a rare instance of encountering allogeneic HLA-G outside of pregnancy, it is a fascinating opportunity to explore the possibility of alloimmunization against graft-derived HLA-G. This assertion is substantiated by a recent report, which provides the first description of anti-HLA-G Abs [59]. The transduced cells used in our study do not express classical HLA Ags, as confirmed by flow cytometry. Consequently, the possibility of interference due to the presence of anti-classical HLA Abs, which may be present in sera, can be ruled out.
Yet, no anti HLA-G Ab was confirmed in our cohort, neither prior to transplantation (M0) nor at M1 or M3. The signal detected in two patients at M1 post-transplantation could have been indicative of an alloimmune response, emerging 1 month after the immunizing event. Conversely, the observed attenuation of the signal at M3 was in favor of weak alloimmunization, which falls below the limits of detection over time. However, these results were not confirmed by the identification test, thereby supporting the validity of our strategy, which entailed a screening step with pooled cells followed by a specific identification step to confirm the findings.
HLA-G has a significantly lower degree of polymorphism compared to classic class I HLA. The selected cell lines were chosen specifically to allow detection of the vast majority of anti-HLA-G Abs. Indeed, HLA-G∗01:01, ∗01:04, and ∗01:06 are the predominant haplotypes, accounting for 81 % of all known haplotypes and 88.5 % of those found in the European population [60]. Notably, HLA-G∗01:01 alone represents 80 % of European haplotypes. It is therefore unlikely that our negative results are due to the detection system being limited to only three HLA-G alleles. However, alloimmunization can only occur in the presence of a HLA-G mismatch between the donor and the patient. A mismatch is statistically improbable in our cohort, which further reduces the likelihood of a false-negative result [61]. A limitation of our study is therefore the absence of HLA-G genotyping data for placenta donors and patients. This information would have strengthened the alloimmunization hypothesis [60].
Recently, the detection of Abs against HLA-G in autoimmune diseases has led to the hypothesis that anti-HLA-G auto-Abs may exist [59]. This possibility could explain the non-confirmed reactions observed in a small number of our patients. Indeed, autoAbs—such as anti-platelet autoAbs detected using MAIPA, from which our detection technique is derived—are characterized by weak and fluctuating signals between samples. Additionally, these materials have heightened sensitivity to freeze–thaw cycles. The sera in our cohort underwent multiple freeze–thaw cycles prior to HLA-G analysis. In particular, sera that tested positive in the screening phase were frozen again before the identification test, which could explain the loss of signal.
Subsequent studies with well-controlled pre-analytical conditions will be necessary to confirm or refute the existence of anti-HLA-G Abs in this and other (transplantation, pregnancy, etc.) clinical settings. In a previous study, our attempts to detect anti-HLA-G Abs in a cohort of lung transplant recipients were unsuccessful. These Abs, whether classified as auto- or alloAbs, could have pathological implications by impeding HLA-G interaction with its receptors, thereby reducing its inhibitory functions.
Conclusion
5
Given the advances in the knowledge about HLA expression by the hAM and in detection methods sensitivity, it was important to confirm previous results in a larger cohort. This is the first study to investigate anti-HLA class I, II, and anti HLA-G Abs in a clinical setting after cryopreserved hAM transplantation using high-sensitivity methods. Our results corroborate and modernize those obtained in the 1980s. The main finding of this study is the minimal humoral immune response regarding HLA class I and II and the absence of anti-HLA-G Abs development in patients who underwent this procedure. Our findings align with our experience of excellent clinical tolerance of the hAM used on the ocular surface.
CRediT authorship contribution statement
Jean-Baptiste Baudey: Writing – review & editing, Writing – original draft, Visualization, Validation, Resources, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Lauriana Solecki: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Resources, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. Christophe Picard: Visualization, Validation, Resources, Methodology, Investigation, Funding acquisition, Conceptualization. Bastien Mathéaud: Resources, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Pauline Jamain: Validation, Resources, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Isabelle Jollet: Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Lucas Hubert: Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Alain Coaquette: Methodology, Investigation, Formal analysis, Conceptualization. Adeline Desanlis: Methodology, Formal analysis, Conceptualization. Xavier Lafarge: Visualization, Supervision, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. Pascal Pedini: Visualization, Validation, Supervision, Resources, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. Florelle Gindraux: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Resources, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization.
Funding
Call for proposals 2023, French Agency of Biomedicine.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Silini A.R.Di Pietro R.Lang-Olip I.Alviano F.Banerjee A.Basile M.Borutinskaite V.Eissner G.Gellhaus A.Giebel B.Huang Y.-C.Janev A.Kreft M.E.Kupper N.Abadía-Molina A.C.Olivares E.G.Pandolfi A.Papait A.Pozzobon M.Ruiz-Ruiz C.Soritau O.Susman S.Szukiewicz D.Weidinger A.Wolbank S.Huppertz B.Parolini O.Perinatal derivatives: where do we stand? A roadmap of the human placenta and consensus for tissue and cell nomenclature Front. Bioeng. Biotechnol.8202061054410.3389/fbioe.2020.610544 PMC 777393333392174 · doi ↗ · pubmed ↗
- 2Jahanafrooz Z.Bakhshandeh B.Behnam Abdollahi S.Seyedjafari E.Human amniotic membrane as a multifunctional biomaterial: recent advances and applications J. Biomater. Appl.3720231341135410.1177/0885328222113760936331116 · doi ↗ · pubmed ↗
- 3Fénelon M.Catros S.Meyer C.Fricain J.-C.Obert L.Auber F.Louvrier A.Gindraux F.Applications of human amniotic membrane for tissue engineering Membranes 11202138710.3390/membranes 1106038734070582 PMC 8227127 · doi ↗ · pubmed ↗
- 4Deus I.A.Santos S.C.Custódio C.A.Mano J.F.Designing highly customizable human based platforms for cell culture using proteins from the amniotic membrane, biomater Adv 134202211257410.1016/j.msec.2021.11257435525741 · doi ↗ · pubmed ↗
- 5Fenelon M.Galvez P.Kalbermatten D.Scolozzi P.Madduri S.Emerging strategies for the biofabrication of multilayer composite amniotic membranes for biomedical applications Int. J. Mol. Sci.2420231442410.3390/ijms 241914424 PMC 1057228737833872 · doi ↗ · pubmed ↗
- 6Davis J.S.SKIN grafting at the johns hopkins hospital Ann. Surg.50190954254910.1097/00000658-190909000-0000217862406 PMC 1407162 · doi ↗ · pubmed ↗
- 7de Rotth A.Plastic repair of conjunctival defects with fetal membranes Arch. Ophthalmol.23194052252510.1001/archopht.1940.00860130586006 · doi ↗
- 8Munoz-Torres J.R.Martínez-González S.B.Lozano-Luján A.D.Martínez-Vázquez M.C.Velasco-Elizondo P.Garza-Veloz I.Martinez-Fierro M.L.Biological properties and surgical applications of the human amniotic membrane Front. Bioeng. Biotechnol.102023106748010.3389/fbioe.2022.1067480 PMC 986819136698632 · doi ↗ · pubmed ↗