Traditional herbal medicine for obesity-related polycystic ovary syndrome: a meta-analysis and data mining study
Lei Tang, Haijuan Liu, Ying Pang, Guohua Wang, Zheng Wang, Tianyao Lv

TL;DR
This study finds that traditional herbal medicine, when combined with standard treatment, improves outcomes for women with obesity-related PCOS.
Contribution
The study identifies a core combination of herbal ingredients using data mining and meta-analysis of clinical trials.
Findings
THM combined with conventional therapy significantly improved clinical efficacy and pregnancy rates in PCOS patients.
Key metabolic markers like HOMA-IR, BMI, and testosterone levels improved with THM treatment.
Poria cocos, Citrus reticulata, Atractylodes lancea, and Cyperus rotundus were identified as a core herbal combination.
Abstract
To systematically evaluate the clinical efficacy of traditional herbal medicine (THM) as an adjunctive therapy for obesity-related polycystic ovary syndrome (PCOS) and to identify core botanical drug combinations using evidence synthesis and data mining approaches. We searched six databases from inception to March 2025 for randomized controlled trials Meta-analyses were performed using Stata 15.1. Association rule mining was performed with the Apriori algorithm. The Cochrane Risk of Bias Assessment Tool (ROB 2.0) and the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework were used to evaluate risk of bias and evidence certainty, respectively. Seventy-two RCTs involving 5,308 patients were included. Meta-analysis indicated that THM combined with conventional therapy significantly improved the clinical efficacy rate (OR = 3.73, 95% CI: 3.12 to 4.46, p <…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
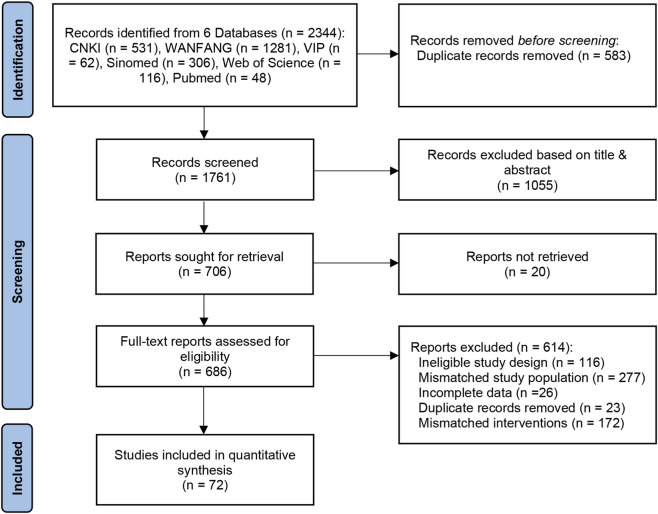 FIGURE 1
FIGURE 1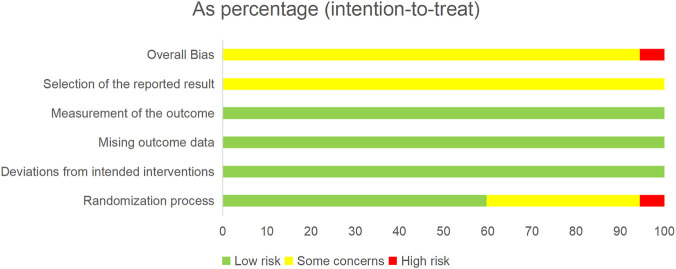 FIGURE 2
FIGURE 2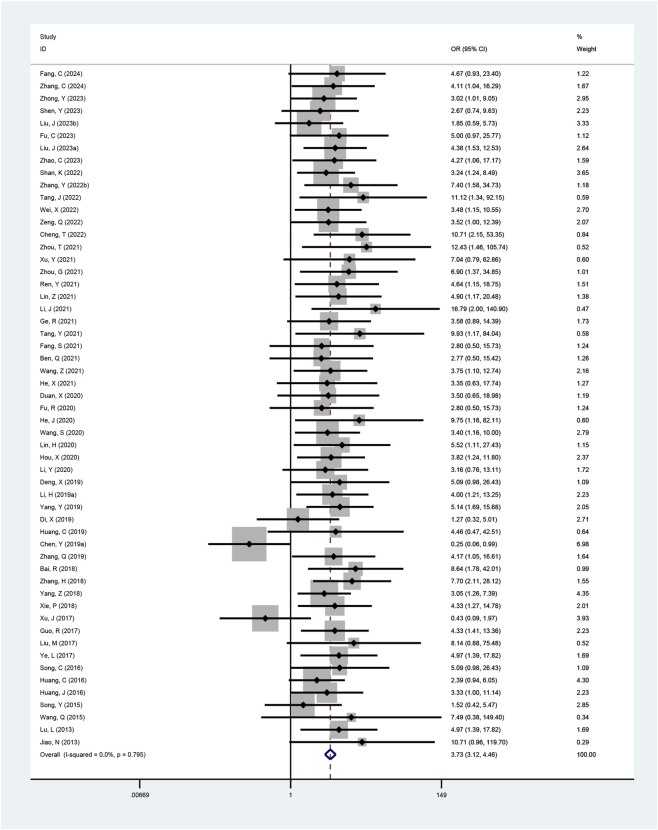 FIGURE 3
FIGURE 3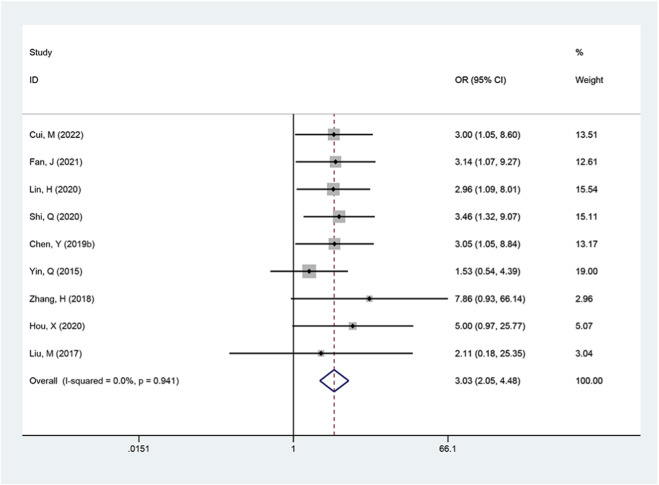 FIGURE 4
FIGURE 4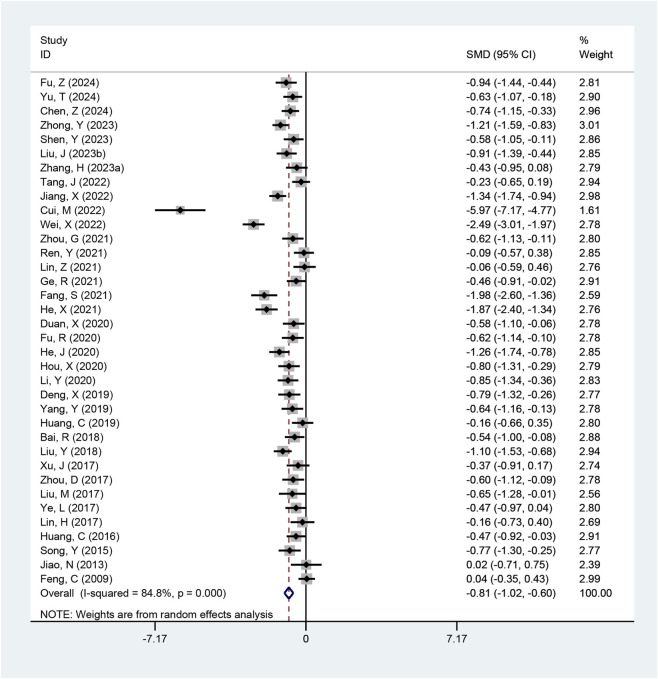 FIGURE 5
FIGURE 5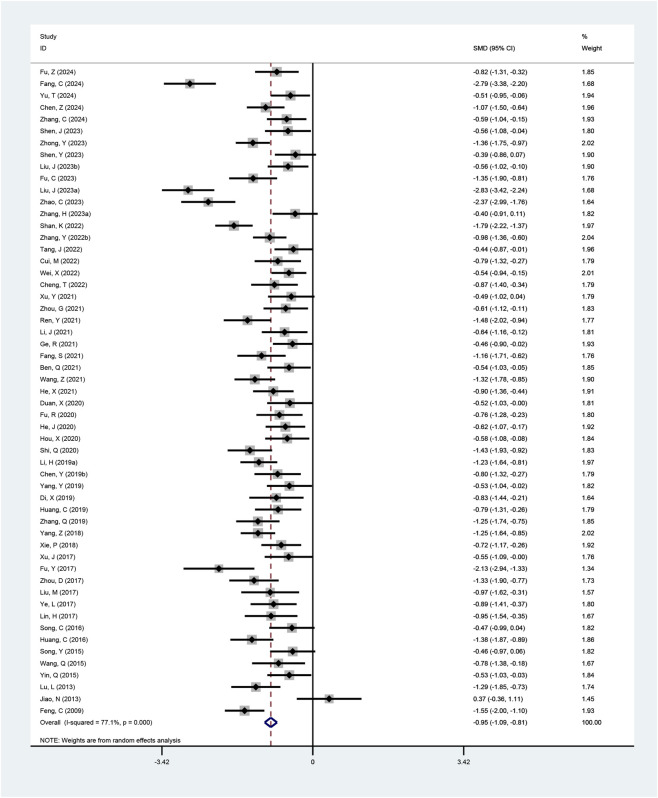 FIGURE 6
FIGURE 6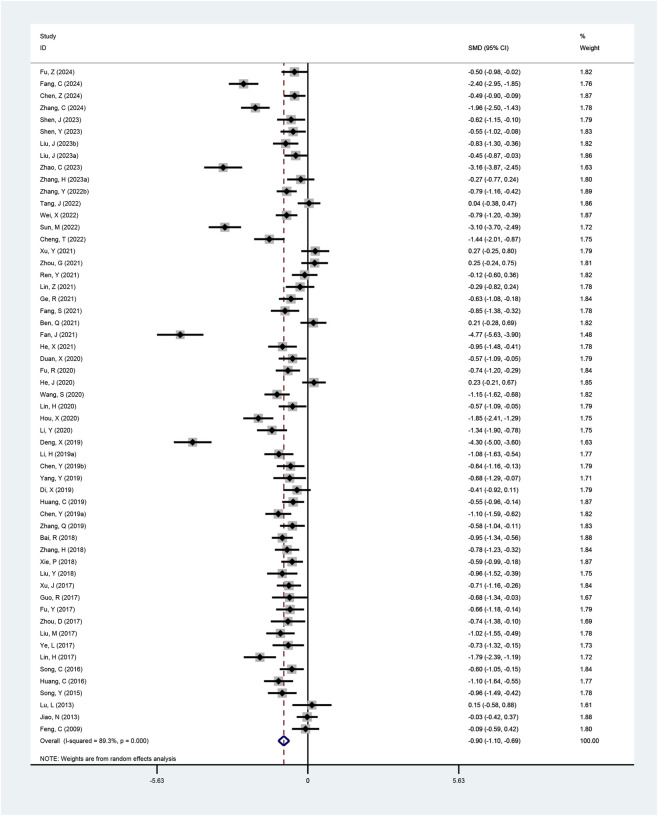 FIGURE 7
FIGURE 7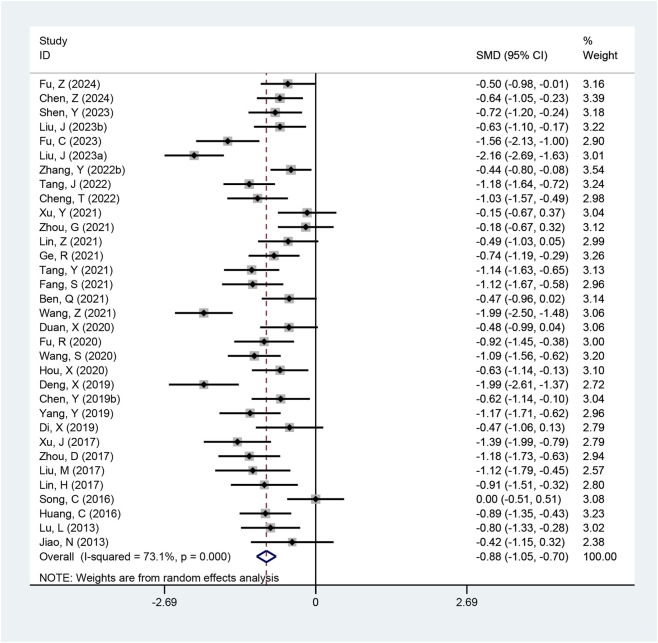 FIGURE 8
FIGURE 8 FIGURE 9
FIGURE 9| Study | Region | Sample size (E/C) | Diagnostic criteria | Experimental group | Control group | Duration | Formulation type | Outcomes |
|---|---|---|---|---|---|---|---|---|
|
| China | 34/34 |
| Erxian qiling decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (3) (4) (5) (6) |
|
| China | 44/44 |
| Modified cangfu daotan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (4) (5) |
|
| China | 40/41 |
| Gexia zhuyu decoction + metformin | Metformin | 12 weeks | Decoction | (3) (4) |
|
| China | 48/48 |
| Huazhuo jiedu decoction + drospirenone and ethinylestradiol tablets | Drospirenone and ethinylestradiol tablets | 12 weeks | Decoction | (3) (4) (5) (6) |
|
| China | 40/40 |
| Self-formulated prescription + ethinylestradiol and cyproterone acetate Tablets + Metformin | Ethinylestradiol and cyproterone acetate tablets + metformin | 24 weeks | Other | (1) (4) (5) |
|
| China | 30/30 |
| Dachaihu decoction combined with fangji huangqi decoction + metformin | Metformin | 12 weeks | Decoction | (4) (5) |
|
| China | 63/63 |
| Fangfeng tongsheng decoction + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) |
|
| China | 36/36 |
| Qutan lishi decoction + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) (6) |
|
| China | 40/40 |
| Self-formulated prescription + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) (6) |
|
| China | 32/32 |
| Yinang jianzhi decoction + dydrogesterone | Dydrogesterone | 12 weeks | Decoction | (1) (6) (4) |
|
| China | 44/44 |
| Modified danxi zhishitan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (4) (5) (6) |
|
| China | 35/35 |
| Bushen huatan decoction + metformin | Metformin | 12 weeks | Decoction | (1) (4) (5) |
|
| China | 30/30 |
| Qigong decoction + metformin | Metformin | 12 weeks | Decoction | (3) (4) (5) |
|
| China | 60/60 |
| Cangfu daotan decoction + metformin | Metformin | 12 weeks | Decoction | (1) (2) (4) |
|
| China | 60/59 |
| Cangfu daotan decoction + ethinylestradiol and cyproterone acetate tablets | Metformin + ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (4) (5) (6) |
|
| China | 43/43 |
| Ditan zhuyu decoction + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) (6) |
|
| China | 58/60 |
| Gexia zhuyu decoction + metformin | Metformin | 12 weeks | Decoction | (3) |
|
| China | 30/30 |
| Bushen huatan decoction + orlistat capsules | Orlistat capsules | 12 weeks | Decoction | (3) (4) (7) |
|
| China | 51/51 |
| Bushen huoxue decoction + metformin + ethinylestradiol and cyproterone acetate tablets | Metformin + ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (3) (4) (5) |
|
| China | 47/47 |
| Huoxue qushi bushen decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (5) |
|
| China | 36/36 |
| Cupailuan decoction + clomifene citrate capsules | Clomifene citrate capsules | 12 weeks | Decoction | (1) |
|
| China | 30/30 |
| Fenxiao huoxue decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (4) (5) (6) |
|
| China | 30/30 |
| Jianpi huatan decoction + metformin | Metformin | 12 weeks | Decoction | (1) |
|
| China | 28/29 |
| Modified huanglian wendan decoction + drospirenone and ethinylestradiol tablets | Drospirenone and ethinylestradiol tablets | 12 weeks | Decoction | (1) (4) (5) (6) |
|
| China | 31/32 |
| Qigong pills modified decotion + drospirenone and ethinylestradiol tablets (Ⅱ) | Drospirenone and ethinylestradiol tablets (Ⅱ) | 12 weeks | Granula | (1) (3) (4) (5) (6) |
|
| China | 35/33 |
| Shoushen tiaojing decoction + metformin | Metformin | 12 weeks | Granula | (1) (3) (4) (5) |
|
| China | 28/27 |
| Modified pingwei san + metformin | Metformin | 12 weeks | Granula | (1) (3) (4) (5) (6) |
|
| China | 30/30 |
| Jianpi huatan decoction + metformin | Metformin | 12 weeks | Decoction | (1) (4) |
|
| China | 40/40 |
| Modified erchen decoction combined with gegen decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (3) (4) (5) (6) |
|
| China | 37/37 |
| Yinang zhuyun decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (4) (6) |
|
| China | 30/30 |
| Shenling baizhu powder + beinaglutide | Beinaglutide | 12 weeks | Granula | (1) (3) (4) (5) (6) |
|
| China | 33/33 |
| Yishen xiaotan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (4) (5) (6) |
|
| China | 30/30 |
| Modified cangfu daotan decoction + progesterone + letrozole | Progesterone + letrozole | 12 weeks | Other | (5) (7) |
|
| China | 44/44 |
| Self-formulated prescription + liraglutide | Liraglutide | 12 weeks | Decoction | (1) (4) (6) |
|
| China | 40/40 |
| Jianpi bushen huoxue decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (3) (4) (5) |
|
| China | 30/30 |
| Shiying yulin decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (3) (4) (5) (6) |
|
| China | 30/30 |
| Jianpi huatan decoction + metformin | Metformin | 12 weeks | Granula | (1) (3) (4) (5) (6) |
|
| China | 40/40 |
| Jianpi bushen decoction + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) |
|
| China | 40/40 |
| Bushen quyu huatan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Other | (1) (5) (6) |
|
| China | 40/40 |
| Cangfu daotan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 4 weeks | Decoction | (1) (5) (7) |
|
| China | 32/32 |
| Bushen qutan Decoction + Metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) (6) (7) |
|
| China | 38/38 |
| Bushen huatan decoction + clomifene citrate capsules | Clomifene citrate capsules | 24 weeks | Decoction | (4) (7) |
|
| China | 35/35 |
| Self-formulated prescription + drospirenone and ethinylestradiol tablets (Ⅱ) | Drospirenone and ethinylestradiol tablets (Ⅱ) | 12 weeks | Decoction | (1) (3) (5) |
|
| China | 30/30 |
| Danggui dihuang decoction combined with taoren siwu decoction + metformin | Metformin | 12 weeks | Granula | (1) (3) (5) (6) |
|
| China | 52/52 |
| Yishen huatan decoction + clomifene citrate capsules | Clomifene citrate capsules | 12 weeks | Decoction | (1) (4) (5) |
|
| China | 30/30 |
| Self-formulated prescription + clomifene citrate capsules | Clomifene citrate capsules | 12 weeks | Granula | (4) (5) (6) (7) |
|
| China | 35/31 |
| Xiaozhi decoction + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) (6) |
|
| China | 22/22/22 |
| Cangfu daotan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (4) (5) (6) |
|
| China | 30/30 |
| Modified cangfu daotan decoction + drospirenone and ethinylestradiol tablets | Drospirenone and ethinylestradiol tablets | 12 weeks | Decoction | (1) (2) (3) (4) (5) |
|
| China | 48/48 |
| Cangfu daotan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (1) (5) |
|
| China | 38/38 |
| Modified cangfu daotan decoction + letrozole | Letrozole | 24 weeks | Decoction | (1) (4) (5) |
|
| China | 38/37 |
| Qihuang zengmin decoction + metformin | Metformin | 12 weeks | Granula | (1) (3) (5) |
|
| China | 56/56 |
| Modified cangfu daotan decoction + clomifene citrate capsules | Clomifene citrate capsules | 12 weeks | Decoction | (1) (2) (5) (7) |
|
| China | 60/60 |
| Modified guizhi fuling pill combined with danggui shaoyao decoction + metformin | Metformin | 24 weeks | Granula | (1) (4) |
|
| China | 40/40 |
| Bushen shugan huayu qutan decoction + metformin | Metformin | 12 weeks | Decoction | (1) (4) (5) |
|
| China | 49/49 |
| Self-formulated prescription + metformin | Metformin | 12 weeks | Decoction | (3) (5) |
|
| China | 29/25 |
| Tanzhixiao granula + metformin | Metformin | 12 weeks | Granula | (1) (3) (4) (5) (6) |
|
| China | 22/20 |
| Modified cangfu daotan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets | 12 weeks | Decoction | (4) (5) |
|
| China | 30/30 |
| Heqi powder + metformin | Metformin | 12 weeks | Granula | (3) (4) (5) (6) |
|
| China | 20/20 |
| Bushen huatan decoction + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) (6) (7) |
|
| China | 32/30 |
| Sanhuang decoction + metformin | Metformin | 12 weeks | Granula | (1) (3) (4) (5) |
|
| China | 40/40 |
| Cangfu daotan decoction + clomifene citrate capsules | Clomifene citrate capsules | 12 weeks | Decoction | (1) (5) |
|
| China | 24/24 |
| Huatan tongmai decoction + metformin | Metformin | 12 weeks | Decoction | (3) (4) (5) (6) |
|
| China | 30/30 |
| Jianpi lishi yiqi yangyin decoction + metformin | Metformin | 12 weeks | Granula | (1) (4) (5) (6) |
|
| China | 40/40 |
| Buqi huatan xingqi decoction + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) (6) |
|
| China | 30/30 |
| Self-formulated prescription + progesterone injection | Progesterone injection | 2 weeks | Granula | (1) |
|
| China | 30/30 |
| Yishen huatan decoction + metformin | Metformin | 12 weeks | Decoction | (1) (3) (4) (5) |
|
| China | 22/24 |
| Self-formulated prescription + letrozole | Letrozole | 12 weeks | Decoction | (1) (4) |
|
| China | 32/32 |
| Bushen huatan decoction + ethinylestradiol and cyproterone acetate tablets | Ethinylestradiol and cyproterone acetate tablets + letrozole | 16 weeks | Decoction | (4) (7) |
|
| China | 30/30 |
| Chushi huatan decoction + metformin | Metformin | 12 weeks | Granula | (1) (4) (5) (6) |
|
| China | 26/10 |
| Zaoshi huatan bushen decoction + metformin | Metformin | 12 weeks | Granula | (1) (3) (4) (5) (6) |
|
| China | 50/50 |
| Modified erchen decoction + ethinylestradiol and cyproterone acetate tablets + metformin | Ethinylestradiol and cyproterone acetate tablets + metformin | 12 weeks | Decoction | (3) (4) (5) |
| Outcome | Subgroup | Studies, n | SMD (95% CI) | P-value | Heterogeneity (I2, τ2, P-value) |
|---|---|---|---|---|---|
| LH/FSH ratio | |||||
| |
|
|
|
|
|
| | By diagnostic criteria | | | | |
| | Chinese diagnostic criteria | 17 | −0.89 (−1.08, −0.70) | <0.001 | 59.5%, τ2 = 0.10, = 0.001 |
| | Rotterdam criteria | 16 | −0.86 (−1.16, −0.56) | <0.001 | 81.0%, τ2 = 0.30, <0.001 |
| | By formulation type | | | | |
| | Decoction | 21 | −0.90 (−1.11, −0.68) | <0.001 | 74.2%, τ2 = 0.18, <0.001 |
| | Granula | 12 | −0.82 (−1.15, −0.49) | <0.001 | 74.8%, τ2 = 0.24, <0.001 |
| HOMA-IR | |||||
| |
|
|
|
|
|
| | By diagnostic criteria | | | | |
| | Chinese diagnostic criteria | 15 | −0.76 (−1.08, −0.44) | <0.001 | 84.0%, τ2 = 0.33, <0.001 |
| | Rotterdam criteria | 21 | −0.85 (−1.14, −0.56) | <0.001 | 85.9%, τ2 = 0.39, <0.001 |
| | By formulation type | | | | |
| | Decoction | 25 | −0.93 (−1.20, −0.66) | <0.001 | 87.3%, τ2 = 0.41, <0.001 |
| | Granula | 11 | −0.55 (−0.84, −0.27) | <0.001 | 67.7%, τ2 = 0.15, = 0.001 |
| BMI | |||||
| |
|
|
|
|
|
| | By diagnostic criteria | | | | |
| | Chinese diagnostic criteria | 25 | −0.94 (−1.14, −0.75) | <0.001 | 76.2%, τ2 = 0.19, <0.001 |
| | Rotterdam criteria | 30 | −0.96 (−1.16, −0.76) | <0.001 | 78.5%, τ2 = 0.25, <0.001 |
| | By treatment duration | | | | |
| | ≤12 weeks | 50 | −1.00 (−1.15, −0.85) | <0.001 | 77.5%, τ2 = 0.22, <0.001 |
| | >12 weeks | 5 | −0.53 (−0.85, −0.21) | = 0.001 | 46.2%, τ2 = 0.06, = 0.115 |
| | By formulation type | | | | |
| | Decoction | 42 | −0.98 (−1.15, −0.81) | <0.001 | 79.9%, τ2 = 0.25, <0.001 |
| | Granula | 12 | −0.90 (−1.14, −0.66) | <0.001 | 61.9%, τ2 = 0.11, = 0.002 |
| | Other | 1 | −0.59 (−1.04, −0.15) | = 0.009 | NA |
| TT | |||||
| |
|
|
|
|
|
| | By diagnostic criteria | | | | |
| | Chinese diagnostic criteria | 24 | −1.11 (−1.46, −0.76) | <0.001 | 91.3%, τ2 = 0.69, <0.001 |
| | Rotterdam criteria | 32 | −0.74 (−0.98, −0.50) | <0.001 | 86.7%, τ2 = 0.42, <0.001 |
| | By treatment duration | | | | |
| | ≤12 weeks | 54 | −0.88 (−1.09, −0.68) | <0.001 | 89.2%, τ2 = 0.54, <0.001 |
| | >12 weeks | 2 | −1.26 (−2.62, −0.10) | = 0.068 | 93.2%, τ2 = 0.89, <0.001 |
| | By formulation type | | | | |
| | Decoction | 39 | −0.84 (−1.05, −0.63) | <0.001 | 85.6%, τ2 = 0.38, <0.001 |
| | Granula | 14 | −0.72 (−1.16, −0.28) | = 0.004 | 90.7%, τ2 = 0.64, <0.001 |
| | Other | 3 | −2.59 (−4.34, −0.84) | = 0.001 | 96.1%, τ2 = 0.29, <0.001 |
| Rank | Botanical drug (scientific name) | Frequency of utilization | Relative frequency (%) |
|---|---|---|---|
| 1 |
| 50 | 69.44% |
| 2 |
| 45 | 62.50% |
| 3 |
| 41 | 56.94% |
| 4 |
| 40 | 55.56% |
| 5 |
| 38 | 52.78% |
| 6 |
| 35 | 48.61% |
| 7 |
| 30 | 41.67% |
| 8 |
| 29 | 40.28% |
| 9 |
| 27 | 37.50% |
| 10 |
| 26 | 36.11% |
| Rank | Consequent | Antecedent | Support (%) | Confidence (%) | Lift |
|---|---|---|---|---|---|
| 1 |
|
| 62.50 | 82.22 | 1.18 |
| 2 |
|
| 56.94 | 80.49 | 1.29 |
| 3 |
|
| 45.83 | 81.82 | 1.18 |
| 4 |
|
| 43.06 | 87.10 | 1.39 |
| 5 |
|
| 41.67 | 86.67 | 1.52 |
| 6 |
|
| 41.67 | 80.00 | 1.40 |
| 7 |
|
| 41.67 | 90.00 | 1.30 |
| 8 |
|
| 41.67 | 90.00 | 1.44 |
| 9 |
|
| 37.50 | 96.30 | 1.54 |
| 10 |
|
| 37.50 | 88.89 | 1.28 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOvarian function and disorders · Pharmacology and Obesity Treatment · Ginseng Biological Effects and Applications
Introduction
1
Polycystic ovary syndrome (PCOS) is a common endocrine and metabolic disorder affecting women of reproductive age, with rising global prevalence and increasingly younger age at diagnosis (Singh et al., 2023). Obesity and PCOS are closely intertwined, and their coexistence significantly increases the long-term risks of cardiometabolic diseases and infertility (Anagnostis et al., 2018; Zhang et al., 2020). While modern medicine offers various treatments for PCOS, such as metformin and combined oral contraceptives, these options are often associated with side effects during long-term use (Renato, 2015). Consequently, many patients seek gentler and more comprehensive therapeutic approaches.
Traditional herbal medicine (THM), comprising medicinal plants used across multiple traditional medical systems, has shown potential in modulating endocrine and metabolic functions (Chen et al., 2023). However, robust evidence specifically supporting its efficacy in obesity-related PCOS remains limited. A key challenge lies in identifying and validating core botanical drug combinations derived from clinical practice.
Therefore, this study aimed to rigorously and comprehensively evaluate the efficacy of THM as an adjunctive therapy for obesity-related PCOS in adults. We conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) that met strict inclusion criteria, with a focus on synthesizing patient-important clinical outcomes to ensure the relevance of our findings. Beyond quantifying clinical effects, we applied association rule mining to analyze the composition of the THM formulas, to identify core botanical drug combinations associated with positive therapeutic outcomes. This integrated approach provides both a conclusive summary of clinical efficacy and data-driven insights into the characteristic combinations that define this treatment strategy, thereby offering a more nuanced understanding of the existing evidence base.
Materials and methods
2
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) statement (Page et al., 2021) and was registered in the Prospective Register of Systematic Review (PROSPERO) database (Registration number: CRD420251111078).
Data sources and search strategy
2.1
A systematic search was performed across six databases: China National Knowledge Infrastructure (CNKI), Wanfang Data, VIP Chinese Science and Technology Periodical Database (VIP), Chinese Biomedical Literature Service System (SinoMed), PubMed, and Web of Science. The search covered the period from database inception to 15 March 2025. Both computerized and manual search methods were used to ensure comprehensiveness. Search strategies incorporated Medical Subject Headings (MeSH) and free-text terms. Search terms were standardized using the Thesaurus of Chinese Traditional Medicine and MeSH terminology. Detailed search strategies are provided in Supplementary Table S1.
Study selection
2.2
Two investigators (LT and HjL) independently screened titles and abstracts of all retrieved records against pre-defined eligibility criteria. Full texts of potentially relevant studies were then reviewed for final inclusion. Discrepancies were resolved through consensus or consultation with a third researcher (YP).
Inclusion criteria
2.2.1
(1) Study Types: RCTs. (2) Participants: Adult women (age ≥18 years) with a confirmed diagnosis of PCOS and obesity, as defined by study-specific criteria. (3) Interventions: The experimental group received oral THM as an add-on to conventional therapy, with a clearly documented botanical composition. The control group received conventional pharmacotherapy combined with the same background therapy. (4) Outcome Measures: Primary outcomes were clinical efficacy rate and clinical pregnancy rate. Secondary outcomes included Homeostatic Model Assessment of Insulin Resistance (HOMA-IR), body mass index (BMI), total testosterone (TT), and the luteinizing hormone/follicle-stimulating hormone (LH/FSH) ratio.
Exclusion criteria
2.2.2
(1) Studies where the experimental group received any non-oral THM therapy; (2) Studies using patented THM formulas with undisclosed composition; (3) Ambiguous author details or data sources; (4) Non-randomized trials, reviews, case reports, or animal studies.
Data processing and methodological quality assessment
2.3
Two researchers independently extracted the following data from each included study: title, first author, publication year, sample size, diagnostic criteria for PCOS and obesity, interventions (including the specific botanical composition of the THM formulas), treatment duration, and all reported outcome measures. To ensure transparent reporting of THM formulas, the ConPhyMP guidelines were followed. (Heinrich et al., 2022). For accurate taxonomic identification, the scientific nomenclature of all botanical materials was verified and standardized using authoritative databases, including Medicinal Plant Names Services, Species Fungorum, the Global Biodiversity Information Facility (GBIF), and the Integrated Taxonomic Information System (ITIS). Additional specialized databases were consulted as needed to confirm the nomenclature of less common organismal groups. Corresponding authors were contacted for missing summary statistics, and any unrecoverable data were excluded from the synthesis.
The methodological quality of the included studies was assessed independently by two researchers using the revised Cochrane risk-of-bias tool (RoB 2.0) for randomized trials (Sterne et al., 2019). Any discrepancies arising during data extraction or quality assessment were resolved through consensus discussion between the reviewers or, when necessary, by arbitration from a senior researcher.
Statistical analysis
2.4
Evidence synthesis
2.4.1
All meta-analyses were performed using Stata 15.1. Odds ratios (OR) were calculated for dichotomous outcomes and standardized mean differences (SMD) for continuous variables. Heterogeneity was assessed using Cochran’s Q test and I^2^ statistics. A fixed-effects model was applied when I^2^ ≤ 50% and P ≥ 0.10; otherwise, a random-effects model was used. For the random-effects model, the between-study variance (τ^2^) was estimated using the DerSimonian–Laird (DL) method. For outcomes with substantial heterogeneity and the impact of intervention characteristics, pre-specified subgroup analyses were conducted based on the formulation type of THM (decoction, granule, other), treatment duration (≤12 weeks, >12 weeks) and PCOS diagnostic criteria. Publication bias was evaluated using funnel plots, supplemented by Egger’s regression test and trim-and-fill adjustment with a maximum of 10 iterations (Lin and Chu, 2018; Rodgers and Pustejovsky, 2021).
Association rule mining of botanical drug formulas
2.4.2
To systematically characterize the compositional profiles of the THM formulas included in the meta-analysis, we performed association rule mining to identify recurrent botanical drug combinations and patterns of co-occurrence. The analysis was implemented using the Apriori algorithm in IBM SPSS Modeler 18.0 (Wu et al., 2021; Zhang S. et al., 2023). In this analysis, each included RCT was treated as a distinct “transaction.” For multi-arm RCTs, each treatment arm receiving a distinct herbal intervention was considered an independent transaction. Key analysis thresholds were predefined to balance the discovery of robust, interpretable patterns against the exclusion of spurious associations, guided by common practices in herbal medicine data mining (Agrawal et al., 1993; Tan et al., 2019). The minimum support was set at 10% to focus on sufficiently frequent botanical drug combinations (Zhang S. et al., 2023). A minimum confidence of 80% was required to ensure high predictive reliability for the derived rules (Wu et al., 2021). A lift value greater than 1 was used to identify meaningful, non-random associations. The maximum antecedent count was limited to 2 herbs to prioritize concise and clinically interpretable botanical drug pairs or triplets (Tan et al., 2019). These parameter choices aimed to highlight core combinations without generating an excessive number of rules. Finally, a network diagram was generated using Cytoscape 3.10.1 to visualize co-occurrence patterns.
Assessment of evidence certainty
2.5
The certainty of evidence for each outcome was appraised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework via the GRADEpro GDT tool. Evidence was categorized as high, moderate, low, or very low based on study limitations, inconsistency, indirectness, imprecision, and publication bias.
Results
3
Results of literature retrieval
3.1
A total of 2,344 records were initially retrieved from the six databases. After removing duplicates and applying the eligibility criteria, 72 RCTs were finally included. The detailed screening process is presented in Figure 1.
Literature screening flowchart.
Study characteristics and quality assessment
3.2
The 72 included RCTs, published between 2009 and 2024, enrolled a total of 5,308 patients. Sample sizes of individual studies ranged from 36 to 126, and treatment durations varied from 2 to 24 weeks. Among the 72 included studies, BMI was reported in 57 studies (Feng, 2009; Jiao et al., 2013; Lu, 2013; Song et al., 2015; Wang et al., 2015; Yin et al., 2015; Huang, 2016; Huang, 2019; Huang et al., 2016; Song, 2016; Fu and Li, 2017; Lin et al., 2017; Liu, 2017; Liu, 2023b; Liu, 2023a; Xu et al., 2017; Ye et al., 2017; Zhou, 2017; Zhou, 2021; Xie, 2018; Yang and Yan, 2018; Chen, 2019b; Di, 2019; Li et al., 2019; Yang, 2019; Zhang et al., 2019; Zhang et al, 2022; Zhang H. et al., 2023; 2024; Duan, 2020; Fu, 2020; Fu, 2023; Fu, 2024; He, 2020; He, 2021; Hou, 2020; Shi, 2020; Ben, 2021; Fang, 2021; Ge, 2021; Li, 2021; Lin, 2021; Ren, 2021; Tang, 2021; Tang, 2022; Wang, 2021; Xu, 2021; Cheng et al., 2022; Cui, 2022; Shan and Gao, 2022; Wei, 2022; Shen, 2023; Shen et al., 2023; Zhao, 2023; Zhong et al., 2023; Chen et al., 2024; Fang and Zhu, 2024; Yu, 2024), TT in 56 studies (Feng, 2009; Jiao et al., 2013; Lu, 2013; Song et al., 2015; Huang et al., 2016; Song, 2016; Fu and Li, 2017; Guo, 2017; Lin et al., 2017; Liu, 2017; Liu, 2023b; Liu, 2023a; Xu et al., 2017; Ye et al., 2017; Zhou, 2017; Zhou, 2021; Bai et al., 2018; Liu and Zhu, 2018; Xie, 2018; Zhang, 2018; Chen, 2019b; Chen, 2019a; Deng, 2019; Di, 2019; Huang, 2019; Li et al., 2019; Li et al, 2020; Yang, 2019; Zhang et al., 2019; Zhang et al, 2022; Zhang H. et al., 2023; Zhang et al, 2024; Duan, 2020; Fu, 2020; Fu, 2024; He, 2020; He, 2021; Hou, 2020; Lin, 2020; 2021; Wang and Tian, 2020; Ben, 2021; Fan and Lin, 2021; Fang, 2021; Ge, 2021; Ren, 2021; Xu, 2021; Cheng et al., 2022; Sun, 2022; Tang, 2022; Wei, 2022; Shen, 2023; Shen et al., 2023; Zhao, 2023; Chen et al., 2024; Fang and Zhu, 2024), and the clinical efficacy rate in 55 studies (Jiao et al., 2013; Lu, 2013; Song et al., 2015; Wang et al., 2015; Huang, 2016; 2019; Huang et al., 2016; Song, 2016; Guo, 2017; Liu, 2017; 2023b; 2023a; Xu et al., 2017; Ye et al., 2017; Bai et al., 2018; Xie, 2018; Yang and Yan, 2018; Zhang, 2018; Chen, 2019a; Deng, 2019; Di, 2019; Li et al., 2019; Li et al, 2020; Yang, 2019; Zhang et al., 2019; Zhang et al, Zhang et al, 2022; Zhang et al, 2024; Duan, 2020; Fu, 2020; Fu, 2023; He, 2020; He, 2021; Hou, 2020; Lin, 2020; 2021; Wang and Tian, 2020; Ben, 2021; Fang, 2021; Ge, 2021; Li, 2021; Ren, 2021; Tang, 2021; Tang, 2022; Wang, 2021; Xu, 2021; Zhou, 2021; Zhou et al., 2021; Cheng et al., 2022; Shan and Gao, 2022; Wei, 2022; Zeng et al., 2022; Shen, 2023; Zhao, 2023; Zhong et al., 2023; Fang and Zhu, 2024), which were the most frequently assessed outcomes. Furthermore, the LH/FSH ratio was documented in 33 studies (Jiao et al., 2013; Lu, 2013; Huang et al., 2016; Song, 2016; Lin et al., 2017; Liu, 2017; 2023b; 2023a; Xu et al., 2017; Zhou, 2017; 2021; Chen, 2019b; Deng, 2019; Di, 2019; Yang, 2019; Duan, 2020; Fu, 2020; Fu, 2023; Fu, 2024; Hou, 2020; Wang and Tian, 2020; Ben, 2021; Fang, 2021; Ge, 2021; Lin, 2021; Tang, 2021; Tang, 2022; Wang, 2021; Xu, 2021; Cheng et al., 2022; Zhang et al., 2022; Shen, 2023; Chen et al., 2024), and the HOMA-IR in 36 studies (Feng, 2009; Jiao et al., 2013; Song et al., 2015; Huang et al., 2016; Lin et al., 2017; Liu, 2017; Liu, 2023b; Xu et al., 2017; Ye et al., 2017; Zhou, 2017; Zhou, 2021; Bai et al., 2018; Liu and Zhu, 2018; Deng, 2019; Huang, 2019; Yang, 2019; Duan, 2020; Fu, 2020; Fu, 2024; He, 2020; 2021; Hou, 2020; Li et al., 2020; Fang, 2021; Ge, 2021; Lin, 2021; Ren, 2021; Cui, 2022; Jiang et al., 2022; Tang, 2022; Wei, 2022; Shen, 2023; Zhang H. et al., 2023; Zhong et al., 2023; Chen et al., 2024; Yu, 2024). For reproductive outcomes, the clinical pregnancy rate was reported in 9 studies (Yin et al., 2015; Liu, 2017; Zhang, 2018; Chen, 2019b; Hou, 2020; Lin, 2020; Shi, 2020; Fan and Lin, 2021; Cui, 2022). The basic characteristics of the included studies are summarized in Table 1. The ConPhyMP checklist assessing the reporting completeness of each THM formula is provided in the Supplementary Data Sheet.
Risk of bias
3.3
Assessment using the Cochrane RoB 2.0 tool revealed significant concerns regarding the reporting of methodological rigor in the included studies. While all studies claimed randomization, the reporting was generally inadequate: only one study was double-blinded, five employed inappropriate randomization methods, and thirty-two mentioned “randomization” without providing details. The absence of prospective protocol registration for all studies led to a judgment of “some concerns” or “high risk” of bias in the randomization process (Domain 1) and in the selection of the reported result (Domain 5). A summary of the risk of bias assessment is presented in Figure 2, with the full evaluation available in Supplementary Table S2.
Risk of bias summary.
Meta-analysis
3.4
Clinical efficacy rate
3.4.1
Fifty-five studies reported the clinical efficacy rate. Due to low heterogeneity among the studies (I^2^ = 0%, p = 0.795), a fixed-effects model was applied for the meta-analysis. The results demonstrated that the combined therapy significantly improved clinical efficacy rates compared to conventional pharmacotherapy alone (OR = 3.73, 95% CI: 3.12 to 4.46, p < 0.001; Figure 3).
Meta-analysis results of clinical efficacy rate.
Clinical pregnancy rate
3.4.2
Nine studies provided data on clinical pregnancy rate. Heterogeneity testing indicated no significant heterogeneity across studies (I^2^ = 0%, p = 0.941), and the fixed-effect model was applied. Meta-analysis showed that the combined therapy markedly increased the clinical pregnancy rate in obese women with PCOS (OR = 3.03, 95% CI: 2.05 to 4.48, p < 0.001; Figure 4).
Meta-analysis results of clinical pregnancy rate.
HOMA-IR
3.4.3
Thirty-six studies reported HOMA-IR values. Substantial heterogeneity was observed among studies (I^2^ = 84.8%, p < 0.001; τ^2^ = 0.35), leading to the use of a random-effects model for pooling. The analysis indicated that the combined therapy was superior to conventional medication in reducing HOMA-IR (SMD = −0.81, 95% CI: −1.02 to −0.60, p < 0.001; Figure 5). Subgroup analyses were consistent (Table 2; Supplementary Figures S1, S2).
Meta-analysis results of HOMA-IR.
BMI
3.4.4
Fifty-seven studies reported BMI outcomes, with two excluded from the pooled analysis due to incompatible data formats (Feng, 2009; Jiao et al., 2013). Given the high heterogeneity among studies (I^2^ = 77.1%, p < 0.001; τ^2^ = 0.22), the random-effects model was selected. The results showed that the combined therapy achieved a greater reduction in BMI than conventional treatment (SMD = −0.95, 95% CI: −1.09 to −0.81, p < 0.001; Figure 6), with subgroup analyses corroborating this result (Table 2; Supplementary Figures S3–S5).
Meta-analysis results of BMI.
TT
3.4.5
Fifty-six studies reported total testosterone levels. Significant heterogeneity was detected (I^2^ = 89.3%, p < 0.001; τ^2^ = 0.54), prompting the use of a random-effects model. The pooled results indicated a more pronounced reduction in total testosterone with the combined therapy (SMD = −0.90, 95% CI: −1.10 to −0.69, p < 0.001; Figure 7), and subgroup analyses confirmed this finding (Table 2; Supplementary Figures S6–S8).
Meta-analysis results of TT.
LH/FSH ratio
3.4.6
Thirty-three studies evaluated the LH/FSH ratio. Marked heterogeneity was present (I^2^ = 73.1%, p < 0.001; τ^2^ = 0.18), so a random-effects model was applied. The meta-analysis suggested that the combined therapy was more effective in improving the LH/FSH ratio (SMD = −0.88, 95% CI: −1.05 to −0.70, p < 0.001; Figure 8). Subgroup analysis based on diagnostic criteria produced similar conclusions (Table 2; Supplementary Figures S9, S10).
Meta-analysis results of LH/FSH ratio.
Sensitivity analysis
3.4.7
Leave-one-out sensitivity analyses were conducted for all outcome indicators. The results confirmed that the pooled effect sizes remained stable after sequentially excluding individual study, indicating robust findings across all meta-analyses (Supplementary Figure S11).
Publication bias
3.4.8
For outcomes with at least 10 included studies, publication bias was assessed using funnel plots (Supplementary Figure S12) and Egger’s linear regression test (Supplementary Figure S13). Significant bias was detected for clinical efficacy rate (Egger’s test P = 0.007), total testosterone (P < 0.001), and HOMA-IR (P = 0.035). Trim-and-fill analysis was subsequently applied to these outcomes (Supplementary Figure S14), which showed that the adjusted effect estimates remained statistically significant for clinical efficacy rate (OR = 3.05, 95% CI 2.57–3.61, P < 0.001), total testosterone (SMD = −1.20, 95% CI −1.42 to −0.98, P < 0.001), and HOMA-IR (SMD = −1.06, 95% CI −1.27 to −0.84, P < 0.001). In contrast, no significant publication bias was observed for BMI (P = 0.332) or LH/FSH ratio (P = 0.097). Overall, these findings suggest that the main conclusions are unlikely to be substantially influenced by publication bias.
Certainty of the evidence
3.4.9
According to the GRADE assessment, the certainty of evidence for the reported outcomes varied from moderate to low (Supplementary Table S3). The evidence for clinical pregnancy rate was rated as moderate, while the evidence for other outcomes, including clinical efficacy rate, BMI, TT, LH/FSH ratio, and HOMA-IR, was rated as low. Downgrading was primarily due to concerns regarding risk of bias in the included studies, inconsistency among results for certain outcomes, and suspected publication bias.
Data mining analysis
3.5
Frequency of botanical drug use
3.5.1
Across the included studies, a total of 137 distinct botanical drugs were utilized, with a cumulative frequency of 891 applications. The complete list of constituent botanical drugs is detailed in Supplementary Table S4. Table 3 presents the ten most frequently used botanical drugs, with usage frequencies ranging from 36.11% to 69.44%. Among these, five botanical drugs were employed in over 50% of the prescriptions: Poria cocos (Schw.) Wolf [Polyporaceae, Poria] (69.44%), Citrus reticulata Blanco [Rutaceae, Citri Reticulatae Pericarpium] (62.50%), Atractylodes lancea (Thunb.) DC. [Asteraceae, Atractylodis Rhizoma] (56.94%), Angelica sinensis (Oliv.) Diels [Apiaceae, Angelicae Sinensis Radix] (55.56%), and Cyperus rotundus L. [Cyperaceae, Cyperi Rhizoma] (52.78%).
Association rule mining
3.5.2
Association rule mining on the included formulas generated a total of 231 rules. The top 10 rules, ranked in descending order by support, are listed in Table 4. The rule with the highest support (62.50%) was {C. reticulata Blanco [Rutaceae, Citri Reticulatae Pericarpium]} => {P. cocos (Schw.) Wolf [Polyporaceae, Poria]}, with a confidence of 82.22%. Furthermore, the rule {A. lancea (Thunb.) DC. [Asteraceae, Atractylodis Rhizoma], C. rotundus L. [Cyperaceae, Cyperi Rhizoma]} => {C. reticulata Blanco [Rutaceae, Citri Reticulatae Pericarpium]} achieved both the highest confidence (96.30%) and the highest lift value (1.54) among all rules.
A network diagram was constructed to visualize the pairwise co-occurrence relationships among botanical drugs (Figure 9), where the thickness of connecting lines represents the association strength. The network analysis identified five botanical drugs as the most central and densely interconnected nodes: P. cocos (Schw.) Wolf [Polyporaceae, Poria], C. reticulata Blanco [Rutaceae, Citri Reticulatae Pericarpium], A. lancea (Thunb.) DC. [Asteraceae, Atractylodis Rhizoma], C. rotundus L. [Cyperaceae, Cyperi Rhizoma], and A. sinensis (Oliv.) Diels [Apiaceae, Angelicae Sinensis Radix].
Network visualization of botanical drug co-occurrence patterns.
Discussion
4
Summary of main findings
4.1
This systematic review and meta-analysis evaluated the adjunctive use of THM with conventional therapy for obesity-related PCOS. The pooled results indicate that the combined regimen was significantly superior to conventional therapy alone in improving key clinical, reproductive, and metabolic outcomes, including clinical efficacy rate, clinical pregnancy rate, HOMA-IR, BMI, total testosterone, and the LH/FSH ratio. However, the certainty of this evidence, as assessed by the GRADE framework, was predominantly low to very low. This was largely attributable to methodological shortcomings in the included studies, such as inadequate reporting of randomization and blinding procedures, alongside considerable heterogeneity among studies, which may reflect the distinct metabolic and reproductive subtypes of the PCOS population (Gao et al., 2025).
A central challenge in interpreting these meta-analytic results lies in the substantial heterogeneity, which primarily stems from the diverse and non-standardized compositions of the THM formulas. We therefore employed data mining to systematically explore the formulation data, aiming to identify recurrent patterns that characterize the heterogeneous interventions. Frequency analysis identified the most commonly used botanical drugs. Association rule mining, which prioritizes the strength and reliability of pairwise relationships, revealed that the most robust statistical associations centered on a specific combination of P. cocos (Schw.) Wolf [Polyporaceae, Poria], C. reticulata Blanco [Rutaceae, Citri Reticulatae Pericarpium], A. lancea (Thunb.) DC. [Asteraceae, Atractylodis Rhizoma], and C. rotundus L. [Cyperaceae, Cyperi Rhizoma]. Network visualization of botanical drug co-occurrence further highlighted these four substances, along with A. sinensis (Oliv.) Diels [Apiaceae, Angelicae Sinensis Radix], as the most central and interconnected nodes. A notable observation emerged from comparing these results: while A. sinensis (Oliv.) Diels [Apiaceae, Angelicae Sinensis Radix] was a high-frequency botanical drug and a central network node, it was not part of the strongest pairwise associations defined by the rule mining. This pattern suggests that A. sinensis (Oliv.) Diels [Apiaceae, Angelicae Sinensis Radix] may have a broader, more generalized pattern of co-use across various formula contexts in the studied dataset, whereas the core four-botanical drug combination exhibits a more distinct and strongly correlated co-occurrence profile. This empirically derived combination offers a data-driven candidate for future research aimed at developing targeted phytotherapeutic strategies.
Limitations
4.2
The interpretation of our findings is subject to several important limitations. First, the methodological quality of the included studies substantially constrains the reliability of the evidence. Most studies failed to report allocation concealment or blinding, and none were prospectively registered. These shortcomings introduce a high risk of performance and detection bias, as well as concerns regarding selective outcome reporting, which may collectively inflate the observed effect sizes. Second, the high statistical heterogeneity underscores a fundamental issue in the field: the lack of intervention standardization. Although our data mining identified a recurrent core combination, it does not validate its efficacy nor does it statistically control for the heterogeneity in the meta-analysis. The pooled estimates thus represent an average effect across a wide spectrum of different herbal interventions, limiting their precision and direct clinical interpretability. Third, the exclusive reliance on studies from Chinese databases may affect the generalizability of our findings to other populations and settings. Finally, while association rule mining effectively revealed frequently co-occurring species, it identifies correlation rather than causation. Therefore, the presumed efficacy and any synergistic effects of the identified core combination remain hypothetical and require validation through rigorously controlled experimental and clinical studies.
Implications for practice and future research
4.3
The findings of this review, tempered by its significant methodological limitations, inform both cautious clinical consideration and a clear direction for future research. Given the predominantly low-certainty evidence, no definitive recommendations for practice can be made. However, for patients and clinicians interested in an evidence-informed integrative approach, the use of quality-controlled THM formulas, particularly those incorporating the core botanical drug combination identified here, may be considered an option for adjunctive use under professional supervision.
Future clinical research must be designed to address the flaws that limited the primary studies in this meta-analysis. This necessitates conducting large-scale, multi-center, randomized controlled trials that are prospectively registered and adhere strictly to CONSORT reporting guidelines. These trials should employ rigorous methodology including allocation concealment and double-blinding. Where ethically feasible, the use of placebo controls is essential to isolate the specific effects of the botanical intervention. Crucially, to enhance the interpretability and reproducibility of future evidence, such trials could utilize standardized, chemically characterized preparations based on the core botanical drug combination identified here.
Implications of mechanism research
4.4
If the preliminary meta-analytic signal that THM may improve outcomes is validated in future rigorous trials, the core botanical drug combination of P. cocos (Schw.) Wolf [Polyporaceae, Poria], C. reticulata Blanco [Rutaceae, Citri Reticulatae Pericarpium], A. lancea (Thunb.) DC. [Asteraceae, Atractylodis Rhizoma], and C. rotundus L. [Cyperaceae, Cyperi Rhizoma] emerges as a prime candidate for investigating multi-targeted botanical drug therapy. This prompts a shift from traditional descriptive frameworks toward a testable hypothesis grounded in contemporary systems pathophysiology of PCOS.
We propose that the therapeutic potential of this combination likely resides in its capacity to concurrently modulate several interconnected pathological axes that sustain PCOS. Modern conceptualizations highlight a self-perpetuating cycle involving insulin resistance, chronic low-grade inflammation, hyperandrogenism, and dysregulated tissue microenvironments (Ren et al., 2019; Mizgier et al., 2024; Zhang et al., 2025). In this cycle, hyperinsulinemia exacerbates androgen excess, which in turn promotes visceral adiposity and immune activation, fueling a state of chronic inflammation (Sanchez-Garrido and Tena-Sempere, 2020; Rudnicka et al., 2021). The resulting inflammatory milieu then impairs insulin signaling, thereby reinforcing insulin resistance (Lonardo et al., 2024). This entire process is embedded within and amplifies dysfunction in key tissue microenvironments, such as adipose tissue, the ovary, and the endometrium, contributing to the characteristic metabolic and reproductive dysfunction of PCOS (Siddiqui et al., 2022; Xiang et al., 2023).
This pathological framework provides a basis for hypothesizing the combination’s mechanism of action. The constituent botanical drugs possess distinct yet complementary pharmacological profiles that may target these interconnected pathways. For instance, metabolites from C. reticulata Blanco [Rutaceae, Citri Reticulatae Pericarpium] and A. lancea (Thunb.) DC. [Asteraceae, Atractylodis Rhizoma] have been linked to improved insulin sensitivity and glucose metabolism in preclinical studies (Castro et al., 2020; Wang et al., 2025). Poria cocos (Schw.) Wolf [Polyporaceae, Poria] is recognized for its anti-inflammatory and gut microbiota-modulating properties, which may address systemic inflammation (Zhu et al., 2022; Liu et al., 2025). Cyperus rotundus L. [Cyperaceae, Cyperi Rhizoma] contains metabolites with reported potential influences on steroidogenic activity and hormonal balance (Pirzada et al., 2015; Huang et al., 2025). Crucially, we hypothesize that the clinical benefit arises not merely from the sum of these isolated actions, but from their synergistic interaction. The combination might disrupt the core pathologic network more effectively than any single botanical drug by simultaneously attenuating inflammation, enhancing metabolic function, and fine-tuning endocrine signaling, thereby breaking the self-perpetuating cycle of PCOS.
Validating this integrative hypothesis requires a stepwise translational approach. Initial work should employ computational methods like network pharmacology to predict the combination’s multi-target interactions within established PCOS molecular networks (Wu et al., 2023). Consistent with best practice guidelines in ethnopharmacology, these in silico predictions must be followed by experimental confirmation. Subsequent empirical validation should utilize suitable preclinical models to compare the effects of the full combination against its individual constituents. Key readouts must extend beyond single biomarkers to encompass interconnected pathways relevant to immunometabolic crosstalk, ovarian follicle development, and hormonal regulation. This approach will help elucidate the synergistic mechanisms and key bioactive metabolites underlying the observed clinical effects.
Conclusion
5
This systematic review indicates that adjunctive therapy with THM may improve key clinical, metabolic, and reproductive outcomes in women with obesity-related PCOS, compared to conventional therapy alone. Data mining of prescription patterns identified a core combination of P. cocos (Schw.) Wolf [Polyporaceae, Poria], C. reticulata Blanco [Rutaceae, Citri Reticulatae Pericarpium], A. lancea (Thunb.) DC. [Asteraceae, Atractylodis Rhizoma], and C. rotundus L. [Cyperaceae, Cyperi Rhizoma] as a candidate for further phytotherapeutic research. The overall evidence is, however, limited by the methodological shortcomings and substantial heterogeneity observed among the included studies. To definitively establish efficacy and safety, future research should prioritize rigorously designed, large-scale clinical trials utilizing standardized preparations based on this core combination. In parallel, experimental studies are warranted to elucidate the underlying synergistic mechanisms of action.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agrawal R. Imieliński T. Swami A. (1993). Mining association rules between sets of items in large databases. ACM SIGMOD Rec. 22 (2), 207–216. 10.1145/170035.170072 · doi ↗
- 2Anagnostis P. Tarlatzis B. C. Kauffman R. P. (2018). Polycystic ovarian syndrome (PCOS): long-term metabolic consequences. Metabolism 86, 33–43. 10.1016/j.metabol.2017.09.016 29024702 · doi ↗ · pubmed ↗
- 3Bai R. Chen W. Li S. (2018). Clinical observation on treatment for obesity-induced polycystic ovary syndrome with qihuang zengmin formula. Guangxi J. Traditional Chin. Med. 41 (03), 7–10. 10.3969/j.issn.1003-0719.2018.03.003 · doi ↗
- 4Ben Q. (2021). Clinical study of yishenxiaotan decoction combined with Daying-35 in the treatment of polycystic ovary syndrome with kidney deficiency and phlegm stasis. Shijiazhuang, China: Hebei University of Chinese Medicine.
- 5Castro M. A. Llanos M. A. Rodenak-Kladniew B. E. Gavernet L. Galle M. E. Crespo R. (2020). Citrus reticulata peel oil as an antiatherogenic agent: hypolipogenic effect in hepatic cells, lipid storage decrease in foam cells, and prevention of LDL oxidation. Nutr. Metabolism Cardiovasc. Dis. 30 (9), 1590–1599. 10.1016/j.numecd.2020.04.033 32605883 · doi ↗ · pubmed ↗
- 6Chen Y. (2019 a). Cangfu daotan decoction combined with ethinylestradiol and cyproterone acetate tablets for Obese polycystic ovary syndrome. Henan Med. Res. 28 (18), 3391–3392. 10.3969/j.issn.1004-437X.2019.18.070 · doi ↗
- 7Chen Y. (2019 b). The clinical observation of bushen Huatan huoxue therapy combined with clomiphene citrate in treating infertility caused by obese PCOS. Jinan, China: Shandong University of Chinese Medicine.
- 8Chen H. Deng C. Meng Z. Meng S. (2023). Effects of TCM on polycystic ovary syndrome and its cellular endocrine mechanism. Front. Endocrinol. (Lausanne) 14, 956772. 10.3389/FENDO.2023.956772 37260441 PMC 10228207 · doi ↗ · pubmed ↗