Single-center experience with immune checkpoint inhibitor-related ureteritis and cystitis
Chenyu Wang, Muwen Nie, Yuan Liu, Wei Qiu, Zhiyang Zhang, Na Zhou, Xiang Wang, Lin Zhao, Hongyan Ying, Chunmei Bai

TL;DR
This study examines a rare side effect of cancer immunotherapy drugs, focusing on symptoms, diagnosis, and treatment of ureteritis and cystitis.
Contribution
The study introduces a severity grading system and explores JAK inhibitors as a treatment for steroid-dependent cases of ICI-related ureteritis and cystitis.
Findings
ICI-related ureteritis and cystitis occurred in 0.96% of patients treated with immune checkpoint inhibitors.
Imaging features like hydroureteronephrosis and ureteral wall thickening were consistently observed in diagnosed cases.
JAK inhibitors showed therapeutic potential in patients who failed steroid tapering.
Abstract
Ureteritis and cystitis is a rare immune-related adverse event (irAE) of immune checkpoint inhibitors (ICIs), challenging to distinguish from urinary tract infection (UTI), easily leading to missed diagnosis. We aim to describe clinical features, radiological characteristics and treatment of patients who suffer from ICI-related ureteritis and cystitis (ICI-UC). This was a single centre case series of patients diagnosed with solid tumor who received ICIs treatment and subsequently suffered from ICI-UC. All clinical demographic data, laboratory parameters, imaging characteristics, and treatment information were collected. Between Mar 1st, 2020 and Mar 31th 2025, 12 of 1239 patients treated at Peking Union Medical College Hospital with ICIs were confirmed to have ICI-related ureteritis and cystitis (0.96%), 10 males and 2 females. Only 1 patient received anti-programmed cell death…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
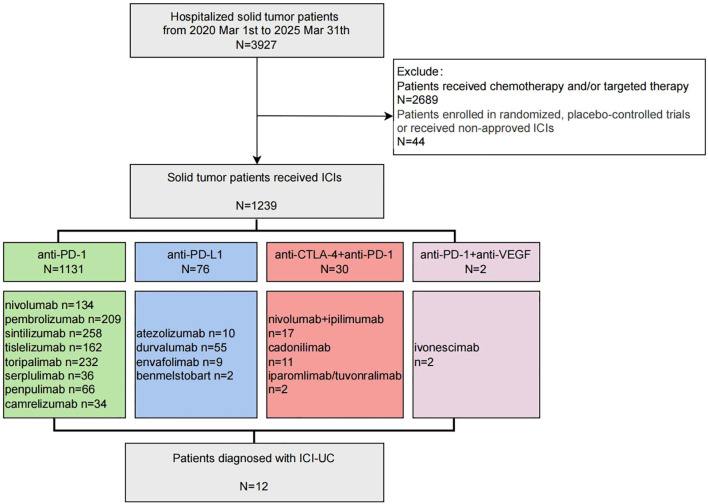 Figure 1
Figure 1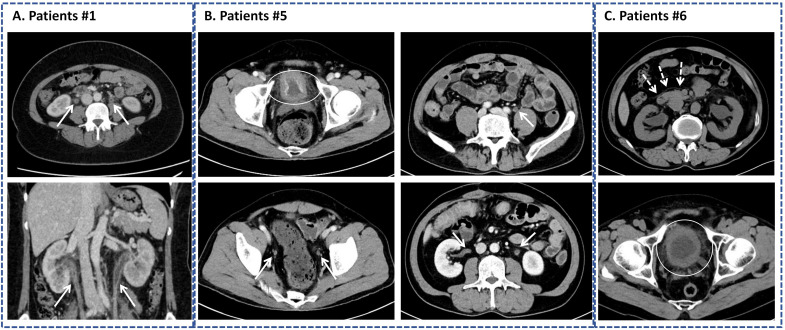 Figure 2
Figure 2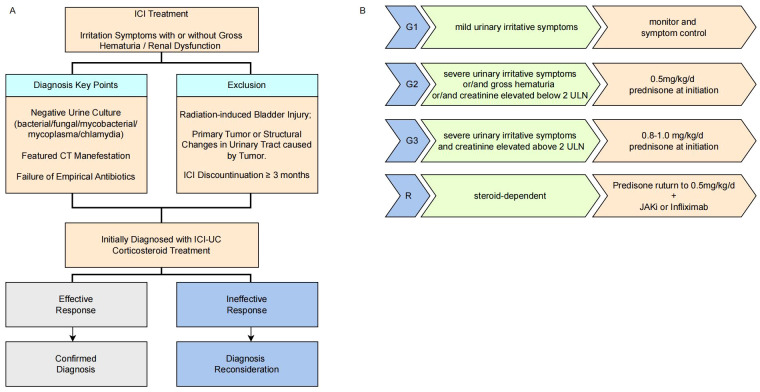 Figure 3
Figure 3| No. | Disease | Stage | ICIs | Combined treatment | Line | Cycles prior to onset | Days prior to onset | Combined irAEs | Best efficacy | Survival (months) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Gastric cancer | Stage IV | Sintilimab | Nab-paclitaxel+S-1 | 2nd | 2 | 28 | G1 | PR | Alive |
| 2 | Laryngeal cancer | Stage IV | Pembrolizumab | Nab-paclitaxel+carboplatin | 1st | 4 | 109 | G1 | PR | Alive |
| 3 | Pancreatic cancer | Stage IV | Penpulimab | Nab-paclitaxel+anlotinib | 4th | 2 | 42 | G1 | PD | Dead |
| 4 | HER2-positive gastric cancer | Stage IV | Sintilimab | Trustuzumab+XELOX | 1st | 2 | 29 | – | SD | Dead |
| 5 | HER2-positive | Stage IV | Nivolumab | Trustuzumab+nab-paclitaxel | 2nd | 6 | 165 | G1 | CR | Alive |
| 6 | Small cell lung cancer | Stage IV | Durvalumab | EP | 1st | 5 | 103 | – | PR | Dead |
| 7 | Gastric cancer | Stage IV | Nivolumab | SOX | 1st | 4 | 104 | – | SD | Dead |
| 8 | Small intestinal cancer | Stage IV | Nivolumab+ | – | 2nd | 3 | 49 | – | PR | Alive |
| 9 | Gastric cancer | Stage IV | Nivolumab | Nab-paclitaxel | 2nd | 4 | 63 | – | SD | Alive |
| 10 | Pancreatic cancer | Stage IV | Penpulimab | Nab-paclitaxel+anlotinib | 4th | 9 | 250 | G1 myocarditis | SD | Alive |
| 11 | HER2-positive | Stage IV | Sintilimab | Trustuzumab+nab-paclitaxel+S-1 | 2nd | 14 | 442 | – | SD | Dead |
| 12 | Cholangiocarcinoma | StageIV | Toripalimab | Gemcitabine+capetabine | 1st | 1 | 21 | – | PR | Alive |
| No. | Creatine (umol/L) | Urine WBC (Cells/ul) | Urine RBC (Cells/ul) | Urine Pro (g/L) | 24hUP (g) | Features of CT scan | PVR (ml) | Cystoscopy | ANA | Other antibody | Urine cytology |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Elevated | 1+ | 3+ | 2+ | 1.45 | ①②③④ | 18 | Mucosa course | Negative | ANCA (–) | Negative |
| 2 | Elevated | 3+ | 3+ | 2+ | NA | ①②③④ | 5 | Multiple lymphoid follicles | C 1:80 | PCNA(+) | NA |
| 3 | Normal | 1+ | 3+ | 3+ | NA | ①③ | 22.5 | NA | Negative | ANCA(-) | Negative |
| 4 | Elevated | 3+ | 3+ | 3+ | NA | ①②③④ | NA | Mucosa course | S 1:160 | ANCA/GBM | NA |
| 5 | Normal | 1+ | 2+ | 1+ | NA | ①②③④ | NA | NA | S 1:80 | ANCA(-) | NA |
| 6 | Elevated | 2+ | 3+ | 2+ | 0.82 | ①②③④ | NA | hyperemia | S 1:80 | ANCA/GBM/PLA2R(-) | Negative |
| 7 | Elevated | 3+ | 3+ | 2+ | 3.75 | ①②④ | 5 | rough/hyperemia | Negative | ANCA(-) | Negative |
| 8 | Elevated | 3+ | 1+ | 2+ | NA | ①②③④ | NA | NA | Negative | ANCA(-) | Negative |
| 9 | Normal | 3+ | 3+ | 3+ | 2.05 | ①②③④ | 16 | NA | Negative | ANCA(-) | NA |
| 10 | Normal | 3+ | 3+ | 1+ | NA | ①②③ | NA | hyperemia/ | Negative | ANCA(-) | NA |
| 11 | Elevated | 1+ | 3+ | 2+ | 2.90 | ①②③④ | NA | hyperemia | Negative | ANCA/GBM | NA |
| 12 | Elevated | 2+ | 3+ | 2+ | 3.41 | ①③ | 21.7 | NA | NA | NA | NA |
| No. | Time from onset to steroid (days) | Number of antibiotics type | D-J stent | ICI continued/ discontinued | Treatment | Symptom resolved (time, days) | Recurrent | Treatment after recurrent |
|---|---|---|---|---|---|---|---|---|
| 1 | 50 | 3 | Yes | Discontinued | PSL 30mg/d (80kg, 0.375mg/kg), | Yes | Yes | PSL 60mg/d |
| 2 | – | 1 | No | Continued | Spontaneous resolution without PSL | Yes | No | – |
| 3 | 15 | 2 | No | Discontinued | PSL 10mg/d (70kg, 0.15mg/kg/d)×2 weeks and discontinued after symptoms relieved | Yes | Yes | PSL 20mg/d for 2weeks |
| 4 | 131 | 3 | No | Discontinued | PSL 30mg/d (55kg, 0.55mg/kg/d), | Yes | No | – |
| 5 | – | 1 | No | Continued | Spontaneous resolution without PSL | Yes | No | – |
| 6 | 14 | 1 | No | Discontinued | PSL 60mg/d (78.5kg, 0.76mg/kg/d)×10 d | Yes | Yes | PSL 60mg/d |
| 7 | 12 | 1 | No | Discontinued | PSL 50mg/d (69kg, 0.72mg/kg/d)×10 d | Yes | Yes | PSL 50mg/d |
| 8 | 17 | 2 | No | Discontinued | MP 60mg/d (85kg, 0.88mg/kg/d)×10 d | Yes | Yes | PSL 15mg/d+ |
| 9 | 5 | 2 | No | Discontinued | PSL 30mg/d (57kg, 0.53mg/kg/d) | Yes | No | – |
| 10 | 31 | 3 | No | Discontinued | PSL 45mg/d (69kg, 0.65mg/kg/d), tapered gradully in 6 weeks | Yes | No | – |
| 11 | 48 | 1 | Yes | Discontinued | PSL 30mg/d (60kg, 0.5mg/kg/d), tapered gradully in 10 weeks | Yes | No | – |
| 12 | 44 | 3 | Yes | Continued | PSL 30mg/d (63kg, 0.48mg/kg/d), corticosteroid tapering regimen not available | Yes | Yes | D-J stent & persistent symptoms |
| No. | Author | Disease | Stage | ICIs | Combined treatment | Cycles prior to onset | Treatment | symptom resolution time (days) | ICI | Relapse | Ref |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | X He | Lung | IIIB | Pembrolizumab | CCRT | 6 | MP 40mg qd*3 | NA | Rechallenge | Yes | ( |
| 2 | Keisuke Ozak | Lung | IV | Nivolumab | No | 3 | PSL 0.5mg/kg, taper gradully | NA | Continued | No | ( |
| 3 | Fan Y | ICC | IV | Toripalimab | No | 1 | MP 120 mg/d×5d→80 mg/d×3 d, graudully taper | 5 days | Discontinued | Yes | ( |
| 4 | Obayashi A | TNBC | IV | Atezolizumab | Nab-paclitaxel | 4 | PSL 40mg/d×4d→30mg/d×7d, symptom recur→60mg/d | 2 days | Discontinued | No | ( |
| 5 | Zhu S | ICC | IV | Atezolizumab | Lenvatinib | 3 | 2mg/kg/d, taper slowly | NA | Discontinued | No | ( |
| 6 | Li J | ESCC | IV | Tislelizumab | Doxetaxel+ | 6 | MP 60mg/d×2w and taper gradully | 3 days | Discontinued | Yes | ( |
| 7 | Li J | GC | IV | Sintilimab | Paclitaxel+S-1 | 3 | MP 60mg/d×7d and taper gradully | 7 days | Discontinued | Yes | |
| 8 | Li J | GC | IV | Nivolumab | No | 2 | MP 60mg/d×7d | 3 days | Discontinued | Yes | |
| 9 | Zhang P | Lung SCC | IV | Sintilimab | Paclitaxel | 6 | MP 40mg/d×3d and gradully reduced in 8 weeks | 4 days | Discontinued | No | ( |
| 10 | Zhang P | Lung | III | Pembrolizumab | Nab-paclitaxel | 6 | MP 40mg/d×2d and gradully reduced in 8 weeks | 4 days | Rechallenge | Yes | |
| 11 | Shimatani K | Lung | IV | Nivolumab | No | 7 | PSL 60mg/d | NA | Continued | Yes | ( |
| 12 | Shimatani K | Lung | IV | Nivolumab | No | 12 | Stop and relief | NA | Discontinued | No | ( |
| 13 | Zhu L | SCLC | IV | Nivolumab | Paclitaxel | 5 | MP 80mg twice a day ×3d and gradully reduced in 6 weeks | 3 days | Discontinued | No | ( |
| 14 | Schneider S | melanoma | – | Nivolumab | No | 2 | Discontinued | NA | Rechallenge | NA | ( |
| 15 | Fukunaka H | Lung cancer | IIIB | Nivolumab | No | 77 | 60 mg/day (1 mg/kg) | immediately | Discontinued | Yes | ( |
| 16 | Anraku T | salivary duct carcino-ma | IVB | Pembrolizumab | No | 2 | spontaneous resolution | NA | Discountined | No | ( |
| 17 | Ji J | GC | III | Sintilimab | Oxaplatin+S-1 | 3 | spontaneous resolution | NA | Discountined | No | ( |
| 18 | Yajima S | Lung adenocarcinoma | IV | Nivolumab | No | 18 | symptoms disappeared after biopsy | NA | Continued | No | ( |
| 19 | Ueki Y | Lung adenocarcinoma | IV | Pembrolizumab | No | 17 | PSL 25mg/d, taper 2months | 19 days | Continued | No | ( |
| 20 | Tu L | Lung adenocarcinoma | IV | Sintilimab | Nab-paclitaxel+Bevacuzumab | 3 | MP 80mg/d, taper in 8weeks | 2 days | Discontinued | No | ( |
| 21 | Wang Z | GC | IV | Sintilimab | Nab-paclitaxel+S-1 | 5 | Chinese medicine | NA | Continued | No | ( |
| 22 | Di C | Lung adenocarcinoma | IVB | Pembroalizumb | Pemetrexed | 5 | Observation and showed relief after discoutinued | NA | Continued | Yes | ( |
| 23 | Zhou Q | Thymic | IV | Tislelizumab | Nab-paclitaxel+ | 6 | MP 1mg/kg/d×3d and reduced to PSL 12mg, tapered gradully in 40 days | 3 days | Discontinued | No | ( |
| 24 | Kihira H | HER2- | IV | Nivolumab | Oxaplatin+S-1 | 6 | MP 50 mg(1 mg/kg/day) | quickly | Discontinued | No | ( |
| 25 | Alhusari L | Lung adenocarcinoma | IIB | Pembrolizumb | Pemetrexed | 8 | PSL 1mg/kg/d and tapered off | NA | Discontinued | No | ( |
| 26 | Ni C | Pancreatic cancer | IV | Sintilimab | Gemcitabine | 6 | Dexamethasone 5mg/d×6d | 6 days | Rechallenge | No | ( |
| 27 | El Husseini K | NSCLC | IV | Pembrolizumb | No | 5 | PSL 1 mg/kg/day | NA | Discontinued | No | ( |
| 28 | Li S | Lung adenocarcinoma | IVA | Pembrolizumb | Pemetrexed | 14 | PSL 30mg/d×14d and reduced by 5mg per week | 2 days | NA | NA | ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Bladder and Urothelial Cancer Treatments · Renal cell carcinoma treatment
Introduction
Immune checkpoint inhibitors (ICIs), a novel advancement in cancer therapy, activate T cell-mediated antitumor immune responses by blocking immune checkpoints. such as cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1), leading to a marked improvement in clinical outcomes across multiple advanced cancers (1). However, this nonspecific immune activation may lead to immune system attacks on healthy tissues, triggering a spectrum of immune-related adverse events (irAEs). Skin, gastrointestinal tract and endocrine organs are commonly affected (2, 3).
With the expanding clinical use of ICIs, urinary tract involvement has emerged as a newly recognized phenotype of rare irAE, which was first reported in 2017 (4). Early reports characterized this irAE as isolated cystitis, but subsequent evidence demonstrated this irAE could involved the entire urothelium (5, 6). This irAE has been variably termed as (nonbacterial) cystitis, uretitis, ureteritis/cystitis, or cystoureteritis in previous case reports (7–9). For consistency in this study, we will uniformly refer to this condition as immune checkpoint inhibitor related uretitis and cystitis (ICI-UC). Currently, fewer than 30 cases of ICI-UC have been reported in the literature. The majority of reported ICI-UC cases were associated with anti-PD-1 monotherapy, with additional cases reported following anti-PD-L1 therapy or PD-1/CTLA-4 blockade (10–14). The cycles prior to symptom onset varied widely from 1 to 77 (12, 15).
The diagnosis of ICI-UC remains clinically challenging, patients usually presented with symptoms such as dysuria, urinary frequency, hematuria, suprapubic or lower lumbar pain, often mimicking bacterial cystitis. However, urinalysis cannot reliably differentiate between these two conditions. Although cystoscopy and biopsy were performed in some cases, findings were non-specific (4, 5, 12). Key distinctions included sterile urine cultures and history of ICI administration.
Common irAEs already have standard grading systems, such as checkpoint inhibitor pneumonitis (CIP), however, current literature uniformly employed Common Terminology Criteria for Adverse Events (CTCAE) for ICI-UC severity assessment relying on symptoms (such as urinary frequency, hematuria) (14, 16). The lack of consensus grading system for ICI-UC contributed to significant heterogeneity in therapeutic decision-making. While corticosteroids remained the mainstay of ICI-UC management, significant variations existed in initial dosing and treatment duration (17–19). Furthermore, clinical experience remains limited for steroid-dependent cases, posing unique therapeutic challenges (15).
While emerging case reports provided recognition of ICI-UC, though systematic characterization remains lacking. This is the first single-center cohort focus on ICI-UC, we aim to characterize the onset and clinical features of ICI-UC, explore distinctive imaging characteristics and establish the grading system and therapeutic framework for this emerging toxicity.
Materials and methods
This single-institution case series of adult solid tumor patients treated at the Department of Oncology, Peking Union Medical College Hospital (PUMCH), Chinese Academy of Medical Sciences (CAMS). The study protocol received approval from the PUMCH Institutional Review Board(I-25PJ1701).
We identified patients treated with ICIs through a review of electronic medical records between Mar 1st, 2020 to Mar 31th, 2025, the flowchart was shown in Figure 1. The ICIs included PD-1 monoclonal antibody (sintilimab, pembrolizumab, nivolumab, tislelizumab, toripalimab, serplulimab, camrelizumab, and penpulimab), PD-L1 monoclonal antibody (atezolizumab, durvalumab, envafolimab and benmelstobart), CTLA-4 antibody (ipilimumab), PD-1/CTLA-4 bispecific antibody (cadonilimab, iparomlimab/tuvonralimab) and PD-1/VEGF bispecific antibody (ivonescimab), patients enrolled in randomized controlled trials or receiving non-approved immunotherapies were excluded from the analysis.
Flowchart of patients enrollment.
After screening ICI-treated cohort, we identified ICI-UC patients through the following criteria: 1) prominent urinary tract irritation symptoms after receiving ICI treatment; 2) dilation of the renal pelvis and ureters and/or the ureteral or bladder wall appeared thickened; 3) negative urine culture and ineffective antibiotics treatment. Patients were excluded due to the following reasons: 1) Presence of underlying urological conditions that could cause similar symptoms, such as symptomatic benign prostatic hyperplasia, urinary tract stones, neurogenic bladder, or urinary tract infection (UTI); 2) History of radiation-induced bladder injury; 3) History of invasive urological procedures; 4) Imaging or cystoscopy suggested a primary tumor or structural changes in the urinary tract caused by tumor; 5) Immunotherapy discontinuation for at least 3 months; 6) History of systemic NSAID or immunosuppressant or medications affecting lower urinary tract function (e.g., alpha-blockers, anticholinergics) use within 3 months before ICI-UC symptom oneset.
For the included patients, information about demographic characteristics, disease stage, ICI type, combined treatment, treatment response, combined irAEs, analysis of urine, peak value of creatinine, radiology presentations including computed tomography (CT) and/or ultrasound findings of the urinary system, cystoscopic appearance, treatment of ICI-UC, overall survival (OS) were collected. Staging was based on the American Joint Committee on Cancer’s Cancer Staging Manual, 8th edition. The onset time of ICI-UC was calculated from ICI initiation to the beginning symptom of ICI-UC. OS was defined as the time from diagnosis to death from any cause.
Results
Patients demographics and oncologic outcomes
From Mar 1st, 2020 to Mar 31th, 2025, 1239 patients had received ICIs (Supplementary Table 1), A total of 12 patients (10 male and 2 female) were diagnosed with ICI-UC, accounting for 0.96% of the ICI-treated population. As Table 1 shown, the median age was 61.5 (range 30-78). None of these patients had past medical history of urinary tract diseases. Malignancies included 5 gastric cancers (all proficient mismatch repair (pMMR), including 3 HER2-positive patients), 1 head and neck cancer, 2 pancreatic cancer, 1 small cell lung cancer, 1 cholangiocarcinoma and 1 microsatellite instability-high (MSI-H) small intestinal cancer, all the patients were diagnosed with stage IV at initiation of ICI treatment. 10 of 12 patients received anti-PD-1 monoclonal antibody (3 nivolumab, 3 sintilimab, 2 penpulimab, 1 toriparimab and 1 pembrolizumab) combined with chemotherapy, 1 patient received anti-PDL1 monoclonal antibody (durvalumab) combined with etoposide and cisplatin regimen and 1 patient received PD-1/CTLA-4 dual-checkpoint blockade (nivolumab and ipilimumab). Except the patient who received PD-1/CTLA-4 dual-checkpoint blockade, all other 11 patients received combination of ICI and chemotherapy (7 patients nab-paclitaxel based regimen, 58.3%), besides, 3 HER2-positive gastric cancer patients (25.0%) received Trustuzumab and 2 pancreatic cancer patient (16.7%) received anlotinib simutaneously in a single-arm phase II study. In terms of best overall response, complete remission (CR) was observed in 1 patient, partial remission (PR) in 5 patients, stable disease (SD) in 5 patients, and progressive disease (PD) in 1 patient. At the cutoff date of May 31th, 2025, with a median follow-up of 46.5 months, median OS was 51.8m (95%CI 25.1m ~ 78.5m) for the all 12 patients.
Onset and clinical features of ICI-UC
The median time to onset of ICI-UC was 83 days (range 28–442 days), median number of cycles prior to onset of ICI-UC was 4 (range 2-14) (Table 1). 12 patients (100%) presented with prominent urinary tract irritation symptoms such as urinary frequency, urgency, dysuria or difficulty urinating. 4 patients (33.3%) manifested with notable gross hematuria. 4 patients (33.3%) experienced with low back pain. The diagnosis of ICI-UC was complicated, all of 12 patients showed negative urine culture and had received at least one empirical antibiotic treatment, with 4 patients (25.0%) having been treated with three different antibiotics. Considering urinalysis, all of 12 patients demonstrated microscopic hematuria, proteinuria and leukocyturia. Among 12 patients, 6 underwent 24-hour urine protein (24hUP) quantification, median 2.48g, span from 0.82g to 3.75g. 8 patients (8/12, 66.7%) experienced creatine elevated (median 1.6mg/dL, range 1.2-2.6mg/dL) (Table 2).
All patients underwent ultrasound and non-contrast or contrast-enhanced CT to evaluate urinary tract. Computed tomography (CT) findings of ICI-UC include the following features: 1) dilation of the renal pelvis and ureters, ureters exhibited “beaded appearance”, typically involving bilateral sides; 2) the ureteral walls appeared thickened with irregular margins, often demonstrating abnormal enhancement on contrast-enhanced CT; 3) The bladder wall often appears thickened and irregular, with poor distension; 4) the renal fascia can be visualized on CT imaging (Table 2), featured CT manifestation was shown in Figure 2. The presentation of cystoscopy including hyperemia (5 patients), mucosa rough (3 patients), edema (1 patient) and multiple lymphoid follicles (1 patient). Residual urine was measured by ultrasound in 6 out of 12 patients, with a median postvoid residual (PVR) volume of 17 mL (range 5-22.5ml). The combination of negative urine cultures and ≥2 characteristic CT findings demonstrated 100% diagnostic specificity in our cohort.
Characteristic computed tomography (CT) manifestation of immune checkpoint inhibitors (ICIs)-related ureteritis and cystitis. (A) Patients No. 1. (B) Patient No.5 with mild urinary irritative symptoms. (C) Patient No.6 with visualization of the anterior renal fascia.Thickening of bladder wall is outlined by a white oval. (⇢) represents anterior renal fascia. (→) represents thickening or enhancement of the ureteral wall and dilation of the renal pelvis and ureter.
Among 11 patients, 4 (36.4%) were ANA-positive at baseline, with low-level positivity, range from 1:80 to 1:160. Patient 2 tested positive for anti-proliferating cell nuclear antigen (PCNA) antibodies, no positivity detected for anti-neutrophil cytoplasmic antibodies (ANCA) (11 patients), anti-Glomerular Basement Membrane (GBM) (4 patients), anti-phospholipase A2 receptor (PLA2R) (1 patient) or anti-bullous pemphigoid 180 (BP180) (1 patient) (Table 2).
Combined other irAEs
5 of 12 patients (41.7%) developed other immune-related adverse events (irAEs) concurrently or sequentially during immunotherapy, in addition to cystitis and ureteritis. 5 patients presented with thyroid immune-related adverse events (Grade 1), 1 patient experienced with myositis (Grade 2), and 1 patient developed myocarditis (Grade 1) with only cardiac troponin I increased (as Table 1 shown).
Treatment of ICI-UC
As Table 3 shown, Two patients (No. 2 and No. 5) demonstrated a spontaneous resolution of symptoms without corticosteroid treatment at onset, presenting with mild urinary frequency and pain. Clinically, they exhibited classic urinalysis and CT findings indicative of ICI-UC, CT imaging was shown in Figure 2A. Both cases resolved within approximately one month, allowing them to continue ICI treatment without symptom recurrence. Out of 12 patients, 10 (83.3%) had received steroids treatment. The median time from symptom onset to the initiation of steroids was 24 days, and the median prednisone dose among these patients was 0.60 mg/kg/day (ranging from 0.15 to 0.96 mg/kg/day). Six patients experienced disease recurrence during the corticosteroid tapering phase, necessitating dose re-escalation. Among which, 2 patients received salvage therapy with prednisone re-escalation and Janus kinase (JAK) inhibitors (tofacitinib 5mg twice a day) simultaneously. Patient No. 9 experienced a disease flare-up as prednisone was tapered to 5 mg/day. Given the planned subsequent surgical intervention, the patient was transitioned to a low-dose steroid and JAK inhibitor regimen (prednisone 15 mg/day and tofacitinib 5 mg twice daily) instead of a high-dose steroid re-challenge. The patient maintained disease remission with rapid steroid discontinuation and JAK inhibitor maintenance, successfully underwent surgery without experiencing an ICI-UC flare, based on our experience we set up a grading system and relative treatment instruction as Figure 3 shown.
Diagnostic workflow for ICI-UC (A), grading and therapeutic strategies for ICI-UC (B).
Discussion
Currently, due to the low incidence rate and insufficient awareness among physicians, ICI-UC were only reported as individual cases. To our knowledge, this is the largest single-center cohort of ICI-UC, encompassing various aspects such as incidence, time of onset, clinical manifestations, imaging features, treatment and oncological outcomes.
Currently, the most widely used immune checkpoint inhibitors in clinical practice include PD-1/PD-L1 inhibitors and CTLA-4 inhibitors. However, patients may experience irAEs during ICI therapy, and irAEs could affect any organ system (20). The administration of PD-1/PD-L1 inhibitors was associated with an overall irAE incidence rate of 66.0% for all-grade events and 14.0% for grade ≥3 adverse events, and the incidence of irAEs of all grade and grade ≥3 adverse events for PD-1/PD-L1 plus CTLA-4 combination therapy was relatively higher with 89% and 67% (21, 22), the most commonly affected organs in immunotherapy include the skin, thyroid and colon (23). Some rare irAEs have also been documented, including type 1 diabetes mellitus (0.48%) and renal irAEs (around 1%) (24). However, only case reports of ICI-UC were available previously, the incidence and clinical characteristics of ICI-UC could not be fully understood, through our cohort, the incidence was first reported 0.95%. Due to limited number of ICI-UC patients, the study did not calculate the incidence separately in CTLA-4 plus PD-1 subgroup and PD-1/PD-L1 inhibitor subgroups. The majority of irAEs occur within 1–3 months after treatment initiation, early-onset irAEs (median time to onset approximately 1 month) include myocarditis and myositis, while delayed-onset events such as pancreatitis and diabetes mellitus typically manifest later, with a median onset of approximately 4 months (25). The median time to onset of ICI-UC was 83 days, but the onset exhibited a wide temporal distribution (range 28–442 days). Among 28 ICI-UC patients identified from 24 case reports, the median time to symptom onset was 5.5 cycles (range: 1–77 cycles), in our cohort, the onset cycle was 4 (4–19, 22, 26–33). The earliest-onset previous case report was a cholangiocarcinoma patient who developed urinary irritation symptoms just 8 days after initiating toripalimab (a PD-1 monoclonal antibody) plus ipilimumab combination therapy (12).
Considering the similarities between UTI and ICI-UC, the diagnosis of ICI-UC was highly challenging, with a median time of 24 days from symptom onset to the initiation of empirical glucocorticoid therapy in our study. All ICI-UC cases clinically presented with urinary irritation symptoms and exhibited varying degrees of urinary laboratory abnormalities, which was indistinguishable from urinary tract infection (UTI), but no patients had fever in our study. Majority of patients (66.7%) presented with mild to moderate elevation in serum creatinine levels (median 1.6mg/dL, range 1.2-2.6mg/dL), commonly demonstrating ureteral and pelvic dilation, which indicated postrenal obstruction could be considered as a potential cause of creatinine elevation. Considering creatine elevation, it is necessary to differentiate it from ICI-related acute kidney injury (ICI-AKI). ICI-AKI typically lacks irritative urinary symptoms, with less common microscopic hematuria and higher peak serum creatinine level (median 4.5 mg/dL, IQR [3.6–7.3 mg/dl]) (34). Meanwhile, cystoscopic findings and inconclusive biopsy pathology were non-specific. Based on our experience, the most diagnostically significant features for ICI-UC were repeated negative urine cultures and CT findings. ICI-UC exhibited highly characteristic imaging manifestations such as bladder and/or ureteral wall thickening with irregular margins, involvement of the anterior renal fascia may be observed when cases with severe inflammation, which were described in previous cases (10, 30). Urine culture and microbiological workup typically require extended processing time, thus metagenomic next-generation sequencing was also used to exclude UTI in a case report, which could facilitate rapid clinical judgment and exhibited promising apllied significance (10). Besides, failure of empirical antibiotic therapy and rapid symptomatic relief with corticosteroid were key distinctive features to confirm the diagnosis of ICI-UC (7, 35).
Drug-induced hemorrhagic cystitis most commonly occurs with cyclophosphamide and ifosfamide, but the cystitis induced by taxane-based treatment was rare (36, 37). Prior case reports have documented albumin-bound paclitaxel-induced cystitis with gross hematuria, however, onset of cystitis induced by nab-paclitaxel was early (3–10 days), urine leukocyte was negative and low dose of prednisone demonstrated clinical efficacy with no featured ultrasound or CT manifestation (38, 39). In our cohort, 7 out of 12 patients (58.3%) had received nab-paclitaxel based regimens. And several patients in previous case reports about ICI-UC received ICIs combined with paclitaxel-based chemotherapy (5, 7, 10, 14, 19, 32). Whether ICIs and taxane-based chemotherapy play a synergistic role in the development of ICI-UC remains unclear. In addition, attention should be paid to patients with a history of pelvic radiotherapy, to differentiate from radiation-induced cystitis (40).
The potential mechanisms of immune checkpoint inhibitor (ICI)-induced cystitis and ureteritis, as inferred from existing case reports and literature reviews, primarily center on the dysregulation of immune tolerance and aberrant immune activation triggered by ICI therapy. ICIs disrupt the PD-1/PD-L1 signaling pathway to enhance antitumor immunity, but this process concurrently breaks down self-tolerance, leading to autoimmune attacks on normal urothelial and ureteral tissues (10, 14, 20). Key pathological findings, such as predominant infiltration of CD3^-^ and CD8^-^ cytotoxic T lymphocytes (and occasionally TIA-1^-^ lymphocytes) in the bladder and ureteral mucosa, support the role of activated T cells in mediating tissue damage by recognizing unknown autoantigens expressed on urinary tract epithelial cells (8, 19, 26). Emerging evidence suggested certain autoantibodies may correlate with the development of immune-related adverse events after the application of ICIs (41). Patients with positive antithyroid antibodies showed higher immune-related thyroid adverse effect rates (75.0% vs 13.8%). Tahir et al. demonstrated serological associations of anti-CD74 with pneumonitis (42). A significant elevation in anti-BP180 antibodies and anti-integrin α6β4 antibodies levels, which was associated with tight junction structure attaching urothelial basal cells to the basement membrane, was observed in a case of immune checkpoint inhibitor (ICI)-induced ureteritis and cystitis (17). However, in our study, a patient had negative result of BP180, which underscore the need to identify potential biomarkers of ICI-UC to facilitate differential diagnosis.
Current management of ICI-UC remains primarily based on case reports (Table 4), highlighting an urgent need for systematic studies to establish standardized grading criteria and treatment guidelines. However, CTCAE criteria fails to comprehensively reflect the full spectrum and clinical severity of irAEs (43). Based on our cohort and experience, we have preliminarily established a grading system and therapeutic strategies for ICI-UC, illustrated as Figure 3. Mild urinary tract irritation symptoms may potentially resolve spontaneously without ICI discountinuation (30). For patients with urinary tract irritation symptoms affecting quality of life, gross hematuria, or elevated creatinine, corticosteroid therapy may be required as initial treatment. Based on current reported cases of ICI-UC, patients generally achieve rapid symptomatic relief following corticosteroid therapy (5, 9, 10, 14, 15, 17, 35). However, disease recurrence during steroid tapering has been observed, majority of patients attempted steroid rechallenge. Based on this phenomenon, despite rapid initial response to corticosteroids, a gradual 6–8 week taper is mandatory to prevent rebound, even in clinically improved patients. However, prolonged corticosteroid therapy may potentially compromise the efficacy of immunotherapy, biological agents may represent a viable therapeutic alternative, a steroid-dependent ICI-UC patient successfully managed through combination therapy incorporating infliximab (15). Tofacitinib is a JAK-STAT inhibitor and has shown efficacy in immune-related adverse events, which demonstrated extraordinary clinical remission rate in steroid-resistant patients (96.7%) and patients with steroid taper failure (100%) (44). The two ICI-UC cases with steroid taper failure in our cohort showed great clinical remission with Tofacitinib and successful steroid taper.
Limitation
This study has the following limitations: 1) As a single-center retrospective analysis, it provided preliminary insights into the incidence and clinical characteristics of ICI-UC. However, due to limited understanding of this condition, it is possible some ICI-UC patients were not included in our study, and treatment approaches were highly individualized. Therefore, we plan to conduct a prospect study to optimize therapeutic strategies. 2) In patients with ICI-UC who exhibited mild-to-moderate creatinine elevation, we primarily attribute this to postrenal obstruction secondary to ureteral/bladder wall thickening. Notably, these renal function abnormalities demonstrated rapid resolution following corticosteroid therapy. However, the potential coexistence of ICI-associated acute kidney injury (ICI-AKI) in this setting requires exclusion through confirmatory renal biopsy. 3) Our study lacked histopathological characterization of bladder or ureteral mucosal biopsies because the procedure at our institution requires general anesthesia and rigid cystoscopy. To minimize patient risk, we prioritized clinical diagnosis based on: medication history, characteristic clinical presentation, diagnostic imaging features, steroid responsiveness, and this approach maintained diagnostic accuracy while reducing invasive procedures.
Conclusion
This article represents the first cohort study specifically investigating ICI-UC, we report incidence rate for the first time and make a detailed description of ICI-UC clinical and imaging characteristics. Based on our cohort analysis and existing literature, we have established a grading system and treatment strategy for ICI-UC, besides, we give a insight in therapeutic potential of JAK inhibitors in steroid-dependent ICI-UC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sullivan RJ Weber JS . Immune-related toxicities of checkpoint inhibitors: mechanisms and mitigation strategies. Nat Rev Drug Discov. (2022) 21:495–508. doi: 10.1038/s 41573-021-00259-5, PMID: 34316029 · doi ↗ · pubmed ↗
- 2Geisler AN Phillips GS Barrios DM Wu J Leung DYM Moy AP . Immune checkpoint inhibitor-related dermatologic adverse events. J Am Acad Dermatol. (2020) 83:1255–68. doi: 10.1016/j.jaad.2020.03.132, PMID: 32454097 PMC 7572894 · doi ↗ · pubmed ↗
- 3Alruwaii ZI Montgomery EA . Gastrointestinal and hepatobiliary immune-related adverse events: A histopathologic review. Adv Anat Pathol. (2023) 30:230–40. doi: 10.1097/PAP.0000000000000401, PMID: 37037419 · doi ↗ · pubmed ↗
- 4Ozaki K Takahashi H Murakami Y Kiyoku H Kanayama H . A case of cystitis after administration of nivolumab. Int Cancer Conf J. (2017) 6:164–6. doi: 10.1007/s 13691-017-0298-6, PMID: 31149494 PMC 6498356 · doi ↗ · pubmed ↗
- 5Tu L Ye Y Tang X Liang Z You Q Zhou J . Case report: A case of sintilimab-induced cystitis/ureteritis and review of sintilimab-related adverse events. Front Oncol. (2021) 11:757069. doi: 10.3389/fonc.2021.757069, PMID: 35004277 PMC 8733470 · doi ↗ · pubmed ↗
- 6Shimatani K Yoshimoto T Doi Y Sonoda T Yamamoto S Kanematsu A . Two cases of nonbacterial cystitis associated with nivolumab, the anti-programmed-death-receptor-1 inhibitor. Urol Case Rep. (2018) 17:97–9. doi: 10.1016/j.eucr.2017.12.006, PMID: 29541592 PMC 5849865 · doi ↗ · pubmed ↗
- 7Zhou Q Qin Z Yan P Wang Q Qu J Chen Y . Immune-related adverse events with severe pain and ureteral expansion as the main manifestations: a case report of tislelizumab-induced ureteritis/cystitis and review of the literature. Front Immunol. (2023) 14:1226993. doi: 10.3389/fimmu.2023.1226993, PMID: 37869004 PMC 10587548 · doi ↗ · pubmed ↗
- 8Ueki Y Matsuki M Kubo T Morita R Hirohashi Y Sato S . Non-bacterial cystitis with increased expression of programmed death-ligand 1 in the urothelium: An unusual immune-related adverse event during treatment with pembrolizumab for lung adenocarcinoma. IJU Case Rep. (2020) 3:266–9. doi: 10.1002/iju 5.12211, PMID: 33163921 PMC 7609190 · doi ↗ · pubmed ↗