Controlled venospasm-assisted foam sclerotherapy combined with high ligation—a novel minimally invasive approach for primary great saphenous vein varicosities
Chen Ya, Liu Zechao, Zhu Xuchang, Chen Boyu, Liu Zhengli, Kong Jie

TL;DR
This study shows that a new minimally invasive treatment for varicose veins is effective and safe, with high success and low complication rates.
Contribution
A novel combination of controlled venospasm and foam sclerotherapy with high ligation is introduced for treating varicose veins.
Findings
100% technical success rate was achieved in all treated limbs.
93.6% of veins remained occluded after 12 months with significant symptom improvement.
Complications were minor and resolved without serious issues.
Abstract
This study aimed to evaluate the efficacy and safety of Controlled Venospasm-Assisted Foam Sclerotherapy (CVAFS) combined with high ligation (HL) for treating primary great saphenous vein (GSV) varicosities. A retrospective cohort of 127 patients with primary GSV varicosities underwent CVAFS with high ligation between 1 Jan 2023 and 1 October 2023. Venospasm was induced by rotational mechanical stimulation of the catheter combined with external compression, resulting in a transient reduction of vessel diameter by 50%–70%, followed by DSA (Digital subtraction angiography)-guided foam injection (1:4 liquid-to-gas ratio). Technical success was defined as complete procedural execution under imaging guidance. Primary endpoints included 1-year GSV occlusion rate (assessed by duplex ultrasound) and reduction in Venous Clinical Severity Score (VCSS). Complications were recorded and managed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
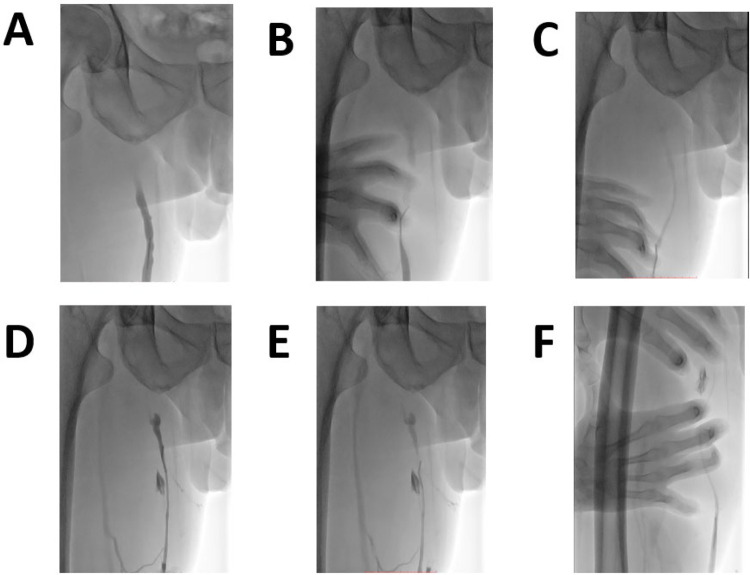 Figure 1
Figure 1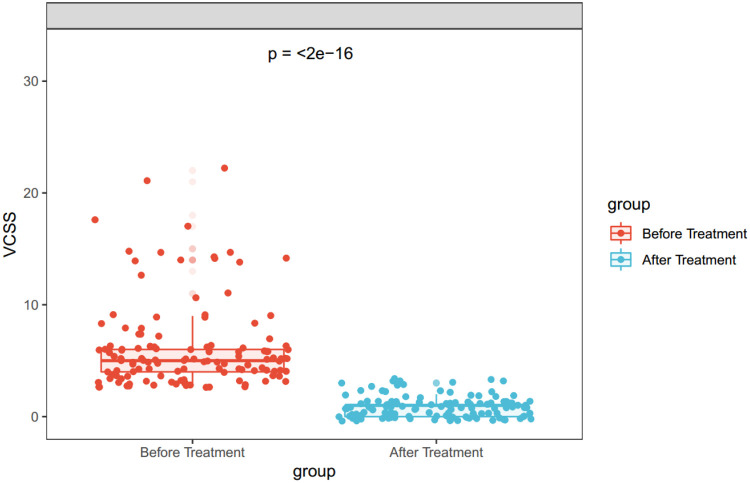 Figure 2
Figure 2| Inclusion and Exclusion criteria |
|---|
|
|
| Reflux time at saphenous-femoral valve > 1s |
| CEAP clinical grade ≥2 |
| The lower extremity deep vein was patentcy |
|
|
| Clinical state not suitable for surgery |
| Patients with contraindication to foam sclerosant treatment |
| Parameter | 127 patients (145 legs) |
|---|---|
| Age | |
| Mean (SD) | 60.2 (9.3) |
| Gender | |
| Male | 62 (48.8%) |
| Hypertension | |
| Yes | 53 (41.7%) |
| Diabete | |
| Yes | 34 (26.8%) |
| Other | |
| Yes | 13 (10.2%) |
| CEAP clinical grade | |
| C2 | 104 (71.8%) |
| C3 | 19 (13.1%) |
| C4 | 16 (11.0%) |
| C5 | 6 (4.1%) |
| C6 | 0 (0%) |
| Parameter | CVAFS + HL | UGFS (ESVS 2022 Guidelines) | MOCA (ESVS 2022 Guidelines) | EVLA (ESVS 2022 Guidelines) | Surgery/HL/S (ESVS 2022 Guidelines) |
|---|---|---|---|---|---|
| Technical Success (≤6 weeks) | 100% (145/145 limbs) | 64–75% at 1–3 years | 86.5% at 3 years | 92% (meta-analysis of 28 RCTs) | 83% at 5 years |
| 1-Year Occlusion Rate | 93.6% (117/125 limbs) | 23–33% at 5 years | 80–82% at 3 years | 88% at 5 years | 83% at 5 years |
| Complication Profile | Thrombophlebitis: 9.6% | Hyperpigmentation: 10–15% | Induration: 12–18% | EHIT: 1.7% | Haematoma: 4.8% |
| Quality of Life Improvement | VCSS: 6.18 ± 3.90 to 0.86 ± 0.90 | Improves but less than thermal ablation | Comparable to thermal ablation | Significant improvement in all QoL measures | Significant improvement comparable to EVTA |
| Anesthesia Requirement | Local anesthesia + tumescence | None required | Local anesthesia | Tumescent anesthesia | General/regional anesthesia |
| Procedure Setting | Outpatient | Outpatient | Outpatient | Outpatient/Ambulatory | Operating room |
| Recovery Time | Ambulation after 6 h | Immediate ambulation | Quick recovery | 1–3 days to normal activities | 2–3 weeks recovery |
| Cost Considerations | Cost-effective (no proprietary devices) | Low cost | Moderate (proprietary device) | High (laser equipment) | High (operating room costs) |
| CEAP Class suitability | C2-C4 | Preferred for veins <6 mm diameter | Suitable for various diameters | First-line for most cases | When EVTA not available |
| Long-term Data | 12-month follow-up | 5-year data available showing lower efficacy | 3-year data available | 5-year + data robust | 5-year + data available |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiagnosis and Treatment of Venous Diseases · Dermatologic Treatments and Research · Central Venous Catheters and Hemodialysis
Introduction
1
The focus of this investigation is primary great saphenous vein (GSV) varicosities, a manifestation of chronic venous insufficiency affecting 20%–40% of Western populations (1, 2). Pathologically characterized by venous wall dilation and valvular incompetence, this condition progresses through CEAP clinical stages C2-C6, manifesting as pain, edema, skin hyperpigmentation, and ulceration (3). Beyond imposing substantial patient morbidity and quality-of-life impairment, it accounts for approximately 2% of national healthcare expenditures in developed countries (4).
Current guidelines recommend thermal ablation, sclerotherapy, or surgical stripping for GSV management (1, 2). Foam sclerotherapy—through detergent-induced endothelial damage leading to fibrotic occlusion—represents a minimally invasive option with reported 3-year closure rates of 70%–85% (5). However, hemodynamic limitations constrain its efficacy: in large-diameter (>8 mm) GSVs with high flow velocities (>10 cm/s), sclerosant dilution reduces endothelial contact time, diminishing foam stability and biological effectiveness (5–7). Computational fluid dynamics models indicate turbulence reduces therapeutic agent residence time by 40%–60% compared to low-flow states (8–10).
The induction of transient venospasm has been proposed as a potential strategy to treat vein varicosities. Transient vasoconstriction reduces luminal diameter and blood velocity, thereby prolonging contact between the sclerosant and the endothelium (5, 11, 12). To translate this physiological principle into a viable clinical application while addressing the limitations of existing therapies, we developed a hybrid approach: Controlled Venous Spasm-Assisted Foam Sclerotherapy (CVAFS) combined with High Ligation (HL). Controlled venous spasm was achieved through endovenous mechanical stimulation via a 4F vertebral catheter rotated and pulled back within the venous lumen, augmented by targeted external manual compression to induce transient vasoconstriction.
This retrospective cohort study evaluated the efficacy of CVAFS + HL, a technique combining high ligation for proximal flow interruption and pharmacologically-induced spasm for distal flow modulation, in 127 patients with primary great saphenous vein (GSV) varicosities (CEAP C2-C4). The primary objectives were to assess the 12-month anatomical closure rate of the GSV trunk, particularly in the thigh segment, complication rates (including thrombophlebitis and neurological injury), and improvement in Venous Clinical Severity Score (VCSS).
Materials and methods
2
Study design and treatment strategies
2.1
Approval for this retrospective cohort study was obtained from the Ethics Committee of our center. Utilizing the electronic medical record system, two independent reviewers identified individuals with primary great saphenous vein (GSV) varicosities. Between January 1, 2023, and October 1, 2023, our center conducted 145 CVAFS + HL procedures on 127 patients, including cases with bilateral interventions. Demographic and clinical characteristics, such as age, gender, and comorbid conditions (e.g., hypertension and diabetes), were documented. All participants underwent standardized CEAP classification and Venous Clinical Severity Score (VCSS) assessments during initial evaluation.
CVAFS, incorporating high ligation for proximal flow interruption, was performed only on patients meeting predefined inclusion criteria: 1) sapheno-femoral reflux duration exceeding 1 s, 2) CEAP clinical stage ≥2, 3) patent deep veins in the lower limbs, and 4) GSV diameter ≥5 mm. Exclusion criteria comprised: 1) contraindications to surgical procedures based on clinical status, 2) contraindications to foam sclerotherapy, 3) pregnancy, 4) history of DVT and 5) thrombophilia as summarized in Table 1.
Interventional procedure
2.2
Patients were positioned supine with local anesthesia (1% lidocaine) administered at the puncture site. Following sterile preparation, ultrasound-guided puncture targeted the great saphenous vein (GSV) trunk at the medial knee joint, facilitating insertion of a 5-Fr introducer sheath. Manual contrast injection subsequently localized the sapheno-femoral junction (SFJ), enabling high ligation 1.0 cm distal to the SFJ using non-absorbable sutures as described before (13). Proximal GSV occlusion was confirmed via manual contrast injection through the catheter (Figure 1A). A 4-Fr catheter was advanced into the GSV lumen, and mechanical venospasm induction ensued through combined catheter rotation/retraction and external cutaneous compression (Figures 1B,C), achieving >50% venous diameter reduction as verified by contrast imaging (Figure 1D). Mechanical venospasm was induced by rotating the 4F vertebral catheter approximately 5–7 times per segment while retracting it at a rate of ∼1 cm/s. Concurrently, targeted external manual compression was applied to achieve a transient reduction in venous diameter by 50%–70%, as confirmed by contrast venography. To minimize inter-operator variability, all procedures were performed by two experienced interventional radiologists who were trained together using a standardized protocol. Sclerosing foam—prepared immediately using the Tessari method (1:4 liquid-to-gas)—was injected through the catheter, with a total administered volume of approximately 5 mL (Figure 1E), while concurrent manual compression of perforating veins prevented foam migration into the deep venous system (Figure 1F). Below-knee varicosities received adjunctive DSA(Digital subtraction angiography)-guided foam injection followed by massage for dispersion uniformity, while ambulatory phlebectomy addressed tributaries >4 mm or clustered varicosities under local anesthesia.
Procedural steps of controlled venous spasm-assisted foam sclerotherapy with high ligation (CVAFS + HL) under venographic guidance. (A) Proximal great saphenous vein (GSV) occlusion confirmed by manual contrast injection via catheter (white arrow indicates occlusion site). (B) Venographic validation of >50% reduction in venous diameter post-venospasm induction. (C,D) Mechanical venospasm induction: A 4-Fr catheter is rotated and retracted within the GSV lumen while external cutaneous compression is applied. (E) Injection of polidocanol foam (1% concentration) prepared via Tessari method (1:4 liquid-to-gas ratio); foam dispersion pattern shown by radiolucent bubbles. (F) Concurrent manual compression of perforating veins to prevent foam migration into deep veins; dashed arrow denotes direction of compression force.
Postprocedural management initiated eccentric compression bandaging across the limb immediately. Patients commenced ambulation 6 h postoperatively, walking 15 min every 2 h. Elastic bandages were maintained for 72 h before transitioning to daily graduated compression stockings (20–30 mmHg) worn for ≥3 months. Duplex ultrasound assessments at 12 months were performed by two sonographers who were blinded to the procedural details, using a standardized imaging protocol to ensure consistency. Complete occlusion was defined as the absence of flow signal on Doppler imaging and non-compressibility of the vein lumen on B-mode imaging. Venous Clinical Severity Score (VCSS) was concurrently quantified to evaluate symptom improvement.
Statistical analysis
2.3
Statistical analyses were conducted using R software (version 3.6.2; R Foundation for Statistical Computing). Continuous variables are presented as mean ± standard deviation (SD), while categorical data are summarized as frequencies and percentages [n (%)]. Independent samples t-tests were applied to compare normally distributed continuous variables between groups, with homogeneity of variances confirmed by Levene's test. Chi-square tests (or Fisher's exact tests for expected cell counts <5) assessed associations between categorical variables. Wilcoxon rank-sum tests analyzed non-normally distributed continuous or ordinal data. A two-sided P-value <0.05 defined statistical significance (14).
Results
3
Between January and October 2023, 127 patients underwent controlled venospasm-assisted foam sclerotherapy (CVAFS) combined with high ligation. The cohort had a mean age of 60.2 ± 9.3 years, comprising 62 males and 65 females. Comorbidities included diabetes mellitus (n = 34), hypertension (n = 53), and other cardiovascular conditions (lacunar infarction or coronary artery disease, n = 13) (Table 2).
A total of 145 affected limbs were treated, with CEAP clinical classifications distributed as follows: C2 (n = 104), C3 (n = 19), C4 (n = 16), and C5 (n = 6) (Table 2). All procedures achieved technical success (145/145 limbs, 100%). Among 127 patients, 109 (85.8%) completed the 12-month follow-up, encompassing 125 treated limbs. Ultrasound assessment confirmed sustained great saphenous vein (GSV) occlusion in 117 limbs (93.6%, 117/125, 95% CI: 89.3%–97.9%), with no cases of clinical recurrence observed. The Venous Clinical Severity Score (VCSS) demonstrated significant improvement from a preoperative baseline of 6.18 ± 3.90 to 0.86 ± 0.90 at 12 months (p < 0.001, Wilcoxon signed-rank test; V = 7,875) (Figure 2).
Preoperative versus 12-month postoperative venous clinical severity score (VCSS) comparison. Significant reduction in venous disease severity after CVAFS + HL. Boxplots display median scores (preoperative: 6.18 ± 3.90; 12-month: 0.86 ± 0.90) with interquartile ranges. The median postoperative VCSS decreased by 86.1% relative to baseline (p < 0.001, Wilcoxon signed-rank test; V = 7,875).
Postprocedural complications included saphenous junction pain (n = 41, 32.8%) and thrombophlebitis (n = 12, 9.6%), all resolving within two weeks without intervention. No instances of deep venous thrombosis or other severe complications occurred during follow-up.
We compared our results with previous studies to evaluate the performance of CVAFS + HL relative to established treatments for great saphenous vein (GSV) incompetence, as summarized in Table 3. The results demonstrate that CVAFS + HL achieved a technical success rate of 100% (145/145 limbs) within 6 weeks, with a 1-year occlusion rate of 93.6% (117/125 limbs). In comparison, ultrasound-guided foam sclerotherapy (UGFS) showed lower long-term efficacy, with occlusion rates of 23%–33% at 5 years, while endovenous laser ablation (EVLA) and mechanochemical ablation (MOCA) exhibited 1-year occlusion rates of approximately 88% and 80%–82%, respectively (22–24). Surgery (high ligation and stripping, HL/S) had a 5-year occlusion rate of 83%. The complication profile for CVAFS + HL included thrombophlebitis (9.6%) and saphenous junction pain (32.8%), with no instances of deep vein thrombosis (DVT), pulmonary embolism (PE), or skin necrosis. This contrasts with UGFS, which had higher rates of hyperpigmentation (10%–15%) and superficial vein thrombosis (SVT; 5.9–13.7%), and surgery, which was associated with nerve injury (11.3%). Quality of life improvement, measured by the Venous Clinical Severity Score (VCSS), showed a significant reduction from 6.18 ± 3.90 to 0.86 ± 0.90 (86.1% improvement, p < 0.001) for CVAFS + HL, comparable to the significant improvements seen with EVLA and MOCA. CVAFS + HL required only local anesthesia with tumescence, allowed outpatient procedures, and facilitated rapid recovery (ambulation within 6 h, return to normal activities in 1–2 days), outperforming surgery which typically necessitated general/regional anesthesia and longer recovery (2–3 weeks). Cost-effectiveness was a key advantage of CVAFS + HL due to the absence of proprietary devices, whereas EVLA and MOCA involved higher costs. CEAP class suitability for CVAFS + HL was confirmed for C2–C4 cases, aligning with guidelines for first-line treatments like EVLA. Long-term data for CVAFS + HL are currently limited to 12 months, whereas other modalities have 3- to 5-year follow-up data available. Overall, these results contextualize CVAFS + HL as a competitive alternative to existing therapies, with efficacy and safety profiles that support its use in clinical practice.
Discussion
4
The global burden of great saphenous vein (GSV) varicosities remains substantial, with an estimated 30% prevalence among adults imposing significant healthcare costs (4, 15). While established modalities like surgical ligation, endothermal ablation (EVLA/RFA), and ultrasound-guided foam sclerotherapy (UGFS) offer therapeutic options, each carries inherent limitations. Foam sclerotherapy—despite its minimally invasive appeal—demonstrates reduced efficacy in larger-diameter veins (>6 mm), where diminished foam-fill ratios and accelerated blood flow compromise endothelial contact time and promote sclerosant dilution (1, 2, 9). This pathophysiological limitation is corroborated by mechanistic studies highlighting the inverse relationship between venous diameter and sclerotherapy success rates (4, 16, 17).
In addressing this challenge, mechanochemical ablation (MOCA) emerged as an innovative approach combining rotational mechanical endothelial injury with liquid sclerosant infusion (18, 19). Contemporary evidence confirms MOCA's short-term efficacy, achieving 88.2% 1-year anatomical occlusion and 93% clinical improvement (19). Its non-thermal nature significantly reduces postoperative pain (mean VAS: 4.8–19.3 mm vs. 18.6–34.5 mm for RFA/EVLA) and accelerates return to normal activities (median 1 day) (19, 20). Nevertheless, MOCA exhibits declining long-term efficacy—3-year occlusion rates drop to 80%–82%, with veins >7 mm demonstrating substantially higher recanalization risk (20). Additionally, a significant advantage of the CVAFS + HL technique is its potential for improved cost-effectiveness compared to MOCA, which relies on proprietary devices such as the ClariVein® catheter (20). Published studies have reported the cost of the single-use ClariVein® device to be approximately 700. In contrast, the CVAFS + HL technique induces venospasm using a conventional and reusable 4F vertebral catheter, which represents a minimal and recurrent cost. By eliminating the need for a dedicated, single-use device, CVAFS + HL substantially reduces the per-procedure material cost, potentially enhancing its viability and adoption in healthcare settings with limited resources.
Our study introduces Controlled Venospasm-Assisted Foam Sclerotherapy with High Ligation (CVAFS + HL) as a strategically optimized alternative. This technique replicates MOCA's mechanical endothelial stimulation through controlled manual catheter rotation within the GSV lumen, intentionally inducing localized venospasm. Crucially, CVAFS substitutes liquid agents with foam sclerotherapy while incorporating proximal high ligation (HL) to mitigate reflux and augment closure. The synergistic mechanism operates through:1, Mechanical venospasm reducing venous diameter by >40%, enhancing foam-wall contact; 2, Endothelial microtrauma increasing sclerosant absorption; 3, HL eliminating saphenofemoral reflux, reducing hemodynamic stress on treated segments.
Our results demonstrate that Controlled Venospasm-Assisted Foam Sclerotherapy with High Ligation (CVAFS + HL) achieves clinical outcomes comparable to mechanochemical ablation (MOCA) while offering distinct advantages. Regarding safety equivalence, no deep vein thrombosis, nerve injuries, or clinically significant hematomas occurred. Minor complications, such as transient thrombophlebitis (≤9%), resolved with conservative management, thereby aligning with MOCA's established safety profile. Notably, saphenous junction pain is a recognized and typically transient effect attributable to the high ligation component, and its spontaneous resolution in all our cases within two weeks aligns with this expectation. In terms of technical efficacy, 1-year occlusion rates and symptom improvement (quantified by VCSS reduction) paralleled MOCA benchmarks, while the addition of high ligation (HL) specifically mitigated proximal recurrence risks inherent in pure endovenous techniques. Concerning economic superiority, eliminating proprietary devices like ClariVein® substantially reduced per-procedure costs, enhancing viability in resource-constrained settings. These collective findings affirm CVAFS + HL as a cost-effective refinement of mechanochemical principles. The manual catheter rotation maneuver proved exceptionally safe, with no perforations occurring despite aggressive manipulation—a result attributable to the flexible catheter tip design. Furthermore, integrating HL counteracts the weakness of ultrasound-guided foam sclerotherapy (UGFS) in managing junctional reflux, synergistically improving long-term durability.
Despite these promising outcomes, this retrospective single-center analysis carries inherent limitations, including potential selection bias and unmeasured confounders, which are intrinsic to its non-randomized, observational design (21). Furthermore, the 12-month follow-up period, while adequate for initial efficacy and safety assessment, is insufficient to evaluate long-term durability and recurrence rates, which often manifest beyond 2–5 years. The study also did not formally analyze the learning curve associated with CVAFS + HL; however, anecdotal observation suggests that operator proficiency, reflected in procedural time and consistency, improved with cumulative experience, a factor that should be quantitatively assessed in future prospective studies to inform training requirements. Although the abstract mentions potential cost-effectiveness, a formal economic analysis comparing this hybrid technique to established therapies like EVLA or UGFS was beyond the scope of this initial investigation and remains a critical area for future research. Therefore, future multi-center, randomized controlled trials with longer follow-up, integrated learning curve assessments, and comprehensive cost-effectiveness analyses are essential to validate these findings and thoroughly evaluate the technique's broader applicability and economic value. Specific priority areas for such research include investigating diameter-dependent efficacy—specifically whether CVAFS + HL overcomes MOCA's known diminished efficacy in veins exceeding 7 mm—assessing long-term outcomes such as 3- to 5-year occlusion durability and retreatment rates, and exploring optimal foam formulation parameters, including ideal sclerosant type, concentration, and foam stability characteristics.
Conclusions
5
CVAFS + HL represents a technically feasible, economically advantageous evolution in minimally invasive varicose vein management. By integrating targeted mechanical venospasm induction with foam sclerotherapy and high ligation, it addresses critical limitations of standalone UGFS while circumventing MOCA's cost barriers. Our results establish its short-term safety and efficacy equivalence to established techniques. Future prospective studies should prioritize long-term outcomes and standardized protocols to solidify its role in evidence-based therapeutic algorithms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gloviczki P Lawrence PF Wasan SM Meissner MH Almeida J Brown KR The 2022 society for vascular surgery, American venous forum, and American vein and lymphatic society clinical practice guidelines for the management of varicose veins of the lower extremities. Part I. Duplex scanning and treatment of superficial truncal reflux: endorsed by the society for vascular medicine and the international union of phlebology. J Vasc Surg Venous Lymphat Disord. (2023) 11(2):231–261.e 6. 10.1016/j.jvsv.2022.09.0043632 · doi ↗ · pubmed ↗
- 2Gloviczki P Lawrence PF Wasan SM Meissner MH Almeida J Brown KR The 2023 society for vascular surgery, American venous forum, and American vein and lymphatic society clinical practice guidelines for the management of varicose veins of the lower extremities. Part II: endorsed by the society of interventional radiology and the society for vascular medicine. J Vasc Surg Venous Lymphat Disord. (2024) 12(1):101670. 10.1016/j.jvsv.2023.08.01137652254 PMC 11523430 · doi ↗ · pubmed ↗
- 3Cragg J Nyamekye I. The recommended goal in the United Kingdom’s national institute for health and care excellence clinical guideline 168 for immediate referral of patients with bleeding varicose veins is not being achieved. J Vasc Surg Venous Lymphat Disord. (2021) 9(2):377–82. 10.1016/j.jvsv.2020.06.01832726670 · doi ↗ · pubmed ↗
- 4Lu PYJ Fung CHC Brooks C. Real-world safety and efficiency of treating symptomatic varicose veins with endovenous closure of great, small, and anterior accessory veins using cyanoacrylate glue (Vena Seal™): a single-surgeon multicenter retrospective study. Ann Vasc Surg. (2025) 112:3–9. 10.1016/j.avsg.2024.11.10139672268 · doi ↗ · pubmed ↗
- 5KovacevićJ. European Guidelines for sclerotherapy in chronic venous disorders. Acta Med Croatica. (2014) 68(Suppl 1):127–44. 10.1177/026835551348328025327003 · doi ↗ · pubmed ↗
- 6Barrett JM Allen B Ockelford A Goldman MP. Microfoam ultrasound-guided sclerotherapy treatment for varicose veins in a subgroup with diameters at the junction of 10 mm or greater compared with a subgroup of less than 10 mm. Dermatol Surg. (2004) 30(11):1386–90. 10.1111/j.1524-4725.2004.30430.x 15522019 · doi ↗ · pubmed ↗
- 7Mariani F Carbone L Sozio G Massaroni R Andreucci E Bianchi V Ultrasound-guided foam sclerotherapy of the saphenous trunks is associated with a low 5-year recurrence rate and improved quality of life in patients with chronic venous disease: a multicenter study. J Vasc Surg Venous Lymphat Disord. (2025) 13(4):102212. 10.1016/j.jvsv.2025.10221239983866 PMC 11964736 · doi ↗ · pubmed ↗
- 8Esmaily-Moghadam M Hsia TY Marsden AL. A non-discrete method for computation of residence time in fluid mechanics simulations. Phys Fluids. (2013) 25(11):110802. 10.1063/1.4819142 PMC 376529824046509 · doi ↗ · pubmed ↗