Very low enalapril and enalaprilat exposure via human milk: a case report from the ConcePTION project
Emily Jacobs, Michael Ceulemans, Nina Nauwelaerts, Siemon de Nys, Kathleen J. Claes, Pieter Annaert, Kristel Van Calsteren, Anne Smits, Karel Allegaert, Martje Van Neste

TL;DR
A mother taking enalapril while breastfeeding had very low drug levels in her milk, posing minimal risk to her infant.
Contribution
This case report provides detailed pharmacokinetic data on enalapril and enalaprilat in human milk and estimated infant exposure.
Findings
Enalapril and enalaprilat levels in human milk were very low (0.01–1.22 ng/mL and 0.32–0.77 ng/mL, respectively).
Estimated infant dosages were 78.32 ng/kg/day for enalapril and 124.45 ng/kg/day for enalaprilat.
Infant plasma concentrations were below the lower limit of quantification for both drugs.
Abstract
Ongoing maternal and clinical hesitancy in breastfeeding-related shared decision-making is driven by limited safety data on maternal pharmacotherapy. Theoretical exposure to maternal enalapril and its active metabolite enalaprilat in breastfed infants has previously been reported in two studies of eight mother-infant pairs. However, actual infant plasma concentrations remain uncharacterized. A 30-year-old white woman started enalapril (5 mg, 1x/day) for IgA nephropathy at 11 weeks postpartum while exclusively breastfeeding. On day 101 postpartum, 25 days after therapy start, she collected six steady-state milk samples over 24 h, along with two maternal and one infant blood sample, used to calculate milk-to-plasma (M/P) ratio and estimated infant exposure. Samples were analyzed using liquid chromatography with tandem mass spectrometry. Maternal and infant health information was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
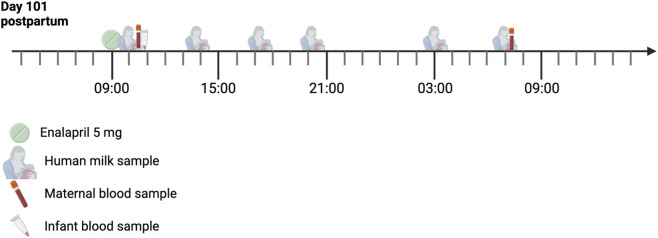 FIGURE 1
FIGURE 1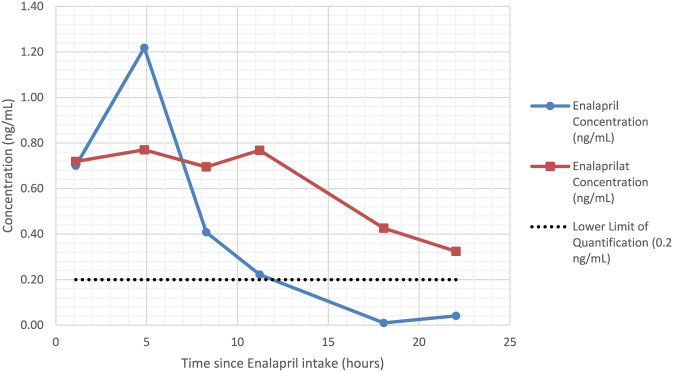 FIGURE 2
FIGURE 2| Days postpartum | Time of sampling (hh:mm) | Time since enalapril intake (hours) | Sample type | Concentration (ng/mL) | |
|---|---|---|---|---|---|
| Enalapril | Enalaprilat | ||||
| 101 | 10:06 | 1.10 | Milk | 0.70 | 0.72 |
| 10:29 | 1.48 | Plasma | 51.74 | 32.74 | |
| 13:52 | 4.87 | Milk | 1.22 | 0.77 | |
| 17:17 | 8.28 | Milk | 0.41 | 0.70 | |
| 20:13 | 11.21 | Milk | 0.22 | 0.77 | |
| 102 | 03:03 | 18.05 | Milk | 0.01 | 0.43 |
| 07:02 | 22.03 | Milk | 0.04 | 0.32 | |
| 07:27 | 22.45 | Plasma | 0.24 | 5.93 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and Medication Impact · Pharmacological Effects and Toxicity Studies · Drug Transport and Resistance Mechanisms
Introduction
1
Enalapril (molecular weight: 376.45 g/mol) is an orally active angiotensin-converting enzyme (ACE) inhibitor, widely prescribed for chronic cardiorenal conditions in adults, including hypertension, heart failure, and off-label, chronic kidney disease (CKD) (Faruqi et al., 2025). In its prodrug form, enalapril is only transiently detectable in plasma, with peak concentrations occurring within 1 hour of oral administration. Subsequently, approximately 60% is rapidly hydrolyzed by hepatic carboxylesterases to enalaprilat (Davies et al., 1984; Ulm et al., 1982). Enalapril exhibits an oral bioavailability of approximately 40%, and its antihypertensive and antiproteinuric effects are mediated by its active metabolite, enalaprilat (Kubo and Cody, 1985; Ulm et al., 1982). Oral administration of enalaprilat itself results in negligible systemic absorption, with a bioavailability of approximately 3% (Ulm, 1983)), which accounts for the clinical use of enalapril rather than enalaprilat, and is also relevant when considering human milk related exposure. Furthermore, enalaprilat has a substantially longer therapeutic half-life than enalapril, of approximately 11 h in adults (Marte et al., 2023), with peak plasma concentrations occurring 3.5–4.5 h post-administration (Ulm et al., 1982). Elimination occurs primarily via the kidneys, with 61% of the dose recovered in urine and 33% in feces (Ulm et al., 1982).
Enalapril is contraindicated during pregnancy because of its teratogenic effects (Bullo et al., 2012) and therefore, early introduction of ACE therapy following delivery is often critical to initiate or restore disease control in women with CKD or postpartum hypertension (McCormack and Brennand, 2024). In the context of lactation, pharmacokinetic and safety data of enalapril and enalaprilat remain limited and somewhat outdated (Huttunen et al., 1989; Redman et al., 1990), which creates considerable challenges for shared decision-making (Tabacova and Kimmel, 2001). Nevertheless, enalapril remains the preferred ACE inhibitor in breastfeeding women given current evidence (Beardmore et al., 2002; Piotrkowicz et al., 2025). Furthermore, its use has long been restricted in children under 20 kg in European countries due to insufficient safety data in this population, exacerbating fears of infant exposure (Hurtado and Moffett, 2007; Van Hecken et al., 2020). Recently, however, the clinical pharmacokinetics were summarized by the Labeling of Enalapril from Neonates up to Adolescents (LENA) consortium (Faisal et al., 2021), expanding therapeutic options for pediatric heart failure (EMA, 2023).
Breastfeeding confers significant long-term health benefits for both mother and child (Chowdhury et al., 2015; Davis et al., 2022; Duijts et al., 2010; Sivasankar et al., 2025) and is widely regarded as the ideal form of infant nutrition (Andreas et al., 2015; Tain et al., 2025). Current recommendations support exclusive breastfeeding for the first 6 months, with continuation alongside gradual introduction of complementary foods for 2 years, or longer, depending on infant and maternal preference (World Health Organization, 2023). Nevertheless, global breastfeeding rates remain suboptimal: in the United States for instance, despite 83.2% initiation rates, only 35.9% of infants are breastfed at 1 year (CDC, 2022). In mothers with chronic disease outcomes are even less favorable. Affecting 10%–30% of the breastfeeding population, chronic diseases are consistently associated with lower rates of sustained exclusive breastfeeding, with this demographic up to 2.5 time more likely to cease breastfeeding prematurely than their healthy peers (Jølving et al., 2016; Pilgrim et al., 2025; Scime et al., 2022).
Among the myriad factors contributing to these suboptimal outcomes, polypharmacy, and specifically, concerns over milk-mediated drug exposure in infants appear salient (Parnizari et al., 2025; Sachs et al., 2013). In the absence of adequate safety data on human milk transmission and inconsistent regulatory guidance (ACOG, 2019; Colaceci et al., 2015; EMA, 2025; EMA, 2023; FDA, 1985), clinical decisions are often made with considerable uncertainty. Particularly as only 16% of European Medicines Agency (EMA) and US Food and Drug Administration (FDA) lactation labelling include human data (Kappel et al., 2023). Faced with the need to balance the well-established benefits of breastfeeding against optimal disease management, in a context shaped more by assumed than demonstrated risks, breastfeeding hesitancy or alternatively, maternal non-adherence and off-label use, becomes the natural outcome (Colaceci et al., 2015).
Here, we present a case study from the UmbrelLACT study and the Innovative Medicine Initiative (IMI) ConcePTION project1, reporting both the concentrations of enalapril and its active metabolite enalaprilat in human milk, as well as the actual and estimated infant exposure through human milk. The report was written in accordance with the CARE guidelines and the ‘Guidelines for reporting cases of medication use during lactation’ (Anderson, 2022; Gagnier et al., 2013).
Methods
2
The current research report describes a mother-infant pair enrolled in the UmbrelLACT study (NCT06042803), whose protocol and ethics approval from the Ethics Committee Research UZ/KU Leuven have been previously reported (Hansson et al., 2025; Van Neste et al., 2024). Prior to enrolment, the mother provided written informed consent forms for herself and her infant. After inclusion, she completed multiple self-report structured questionnaires, covering maternal and infant clinical data, such as biometrics, comorbidities, intake of medication in the 3 days preceding sample collection and general information concerning pregnancy and breastfeeding (Van Neste et al., 2024).
It is important to note that the mother’s decision to take enalapril while breastfeeding, as well as any aspect of her clinical care, were independent of the study team.
Sample collection
2.1
Starting from enalapril intake, six human milk samples were collected intermittently at steady state over a period of 24 h. During this time, the infant was not put to the breast; however, feeding practices were otherwise left to the discretion of the mother. Milk was expressed at home for approximately 20 min using an electric pump, respecting the usual feeding schedule of the mother-infant pair, in accordance with UmbrelLACT protocol. The total volume obtained from both breasts at each feeding session was collected, with foremilk and hindmilk combined, and the total volume was recorded. Subsequently, a 10 mL sample was retained from each timepoint for bioanalysis of enalapril and enalaprilat concentrations. For further details regarding the milk collection methodology, please refer to the previously published protocol (Van Neste et al., 2024).
Maternal blood samples were collected within 1 h of the first and last milk expression sessions in ethylenediaminetetraacetic acid (EDTA) tubes, and an infant plasma sample was obtained close to the first breastfeeding session of the study period.
All samples were stored in the mother’s refrigerator for up to 24 h, at which time they were transported for long-term storage at −80 °C on ice. Concurrent with sample collection, the mother also completed standardized questionnaires to collect maternal biometrics and clinical data, together with general health outcomes of the infant (Van Neste et al., 2024).
Bioanalytical method for enalapril and enalaprilat
2.2
The samples were analyzed using liquid chromatography with tandem mass spectrometry (LC-MS/MS), see Supplementary Material. All data analyses were conducted in Microsoft Excel v.2508, Microsoft 365. The calculations used to estimate infant exposure are detailed below.
Pharmacokinetic calculations
2.3
Pharmacokinetic parameters and exposure metrics were calculated using the following equations.
Equation 1 Milk-to-Plasma Ratio.
The milk-to-plasma ratio was calculated to estimate the extent of drug transfer from maternal plasma into human milk.
Equation 2 Relative Infant Exposure.
Relative infant exposure was calculated to quantify the proportion of the maternal dose ingested by the breastfed infant.
Equation 3 Daily Infant Dose as a function of patient data for the exclusively breastfed infant.
The daily infant dose was calculated using patient-specific data for an exclusively breastfed infant to estimate actual drug intake.
Equation 4 Daily Infant Dose as a function of standardized milk intake.
The daily infant dose was also estimated using a standardized milk intake to allow comparison across studies.
Equation 5 Relative Infant Dose.
The relative infant dose was calculated as the infant dose normalized to the maternal weight-adjusted dose to assess breastfeeding safety.
Equation 6 Relative Infant Therapeutic Dose.
The relative infant therapeutic dose was calculated by comparing the estimated infant exposure to the established therapeutic dose in infants.
Results
3
Case description: patient information and therapeutic interventions
3.1
The patient was a 30-year-old, primigravida, white woman, diagnosed with biopsy-confirmed IgA nephropathy during pregnancy, and treatment with 5 mg Enalapril, E.G., (Eurogenerics NV, Brussels, Belgium), a generic formulation of the ACE inhibitor enalapril was initiated in postpartum at 11 weeks (day 76) postpartum after the patient presented with proteinuria. At the time of sample collection, she was 14 weeks postpartum (day 101), weighed 61.8kg, and measured 168cm, corresponding to a BMI of 21.9 kg/m^2^. She reported following a normal diet and no recreational drug, alcohol or cigarette use. No comorbidities or chronic diseases were reported, aside from her kidney condition, and she reported not taking any other medications or supplements in the weeks preceding sample collection. At time of sampling, the patient’s serum creatinine was 1.26 mg/dL and her eGFR was 57 mL/min/1.73 m^2^ corresponding to stage 3 chronic kidney disease (CKDG3). The dose of enalapril was not further increased because of low blood pressure.
The infant was a healthy, term male (38 weeks gestation), weighing 3.04 kg and measuring 48 cm at birth. At the time of sample collection (aged 101 days), the infant was exclusively breastfed, thus was exposed to maternal pharmacotherapy, and weighed 5.84 kg and measured 59 cm. The infant received daily vitamin D supplementation (D-Cure 2400 IU/mL, SMB-GALEPHAR, Marche-en-Famenne, Belgium), in line with the current recommendations (Van de Walle et al., 2024).
Timeline
3.2
The timeline of the 24-h sampling day is illustrated in Figure 1. The first milk sample was collected 1 hour after enalapril intake, with both maternal and infant plasma samples within 30 min of milk sample collection.
Timeline of the 24-h sampling day. The mother took 5 mg enalapril once daily, and all samples were obtained within 24 h.
Follow-up and outcomes
3.3
Maternal and infant health
3.3.1
Maternal clinical data and medication use, as well as infant data, including clinical information, growth, hospitalizations, adverse effects, and medication use, were collected via a standardized self-report questionnaire completed by the mother. No adverse events or hospital admissions were reported for the infant during the 2 months following sample collection (21 weeks postpartum). Continued daily vitamin D supplementation was confirmed for the infant.
Collection of maternal samples
3.3.2
Six human milk samples were collected over the 24-h period at steady-state, as the medicine had been taken consistently prior to sampling, 5 mg once every 24 h, according to the mother’s report. Two maternal blood samples were collected within 30 min of the first and final milk expression sessions, with the first sample taken within 2 h of the enalapril intake (Figure 1). The total milk volume expressed per session ranged from 100–190 mL, with an average of 135 mL. A summary of the maternal sample characteristics is provided in Table 1. In these maternal milk samples, two enalapril concentrations were below the lower limit of quantification (LLOQ; 0.2 ng/mL) and were estimated, albeit with greater uncertainty.
Human milk and maternal plasma pharmacokinetics
3.3.3
The concentration time profiles of enalapril and enalaprilat in the six human milk samples are shown in Figure 2. Enalapril concentrations in human milk samples ranged from below the LLOQ (estimated at 0.01 ng/mL) to 1.22 ng/mL, while enalaprilat concentrations ranged from 0.32 to 0.72 ng/mL. In maternal plasma, concentrations of enalapril and enalaprilat ranged from 0.24–51.74 ng/mL and 5.93–32.74 ng/mL, respectively. Calculated using the trapezoidal rule, the mean AUC_24h_ in human milk was 8.21 ngh/mL for enalapril and 13.03 ngh/mL for enalaprilat, with mean average steady-state concentration (C_av,ss_) values of 0.39 ng/mL and 0.62 ng/mL, respectively.
Steady-state human milk concentration-time profiles of enalapril and enalaprilat at 13 weeks postpartum.
Milk-to-plasma (M/P) ratio
3.3.4
The plasma AUC_24h_ could not be calculated for the patient, as only two plasma samples were obtained, preventing accurate calculation. Therefore, the mean plasma of both enalapril and enalaprilat were taken from the literature (137 ngh/mL and 265 ngh/mL respectively), as AUC_24h_ could not be extracted from this publication (Schwartz et al., 1985). To our knowledge however, this is the only study reporting the pharmacokinetics of a single daily 5 mg dose of enalapril, albeit in non-pregnant, non-postpartum adults, with unknown kidney function.
The patient’s milk AUC_24h_ was therefore combined with the plasma from Schwartz et al. (1985) to calculate the milk-to-plasma (M/P) ratio (see Equation 1). The M/P ratios were 0.060 and 0.049 for enalapril and enalaprilat, respectively.
Single time point M/P ratios were also calculated using the coincident milk and plasma samples (M1/P1 within ∼30 post-dose and M6/P2 ∼22 h post dose), yielding a mean M/P ratio of 0.093 for enalapril (0.21 LLOQ/2) and 0.038 for enalaprilat.
Infant plasma sample and drug exposure
3.3.5
A single plasma sample was collected from the breastfed infant, in which both enalapril and enalaprilat were below the LLOQ (0.2 ng/mL). Because enalapril and enalaprilat concentrations in infant plasma samples were below the LLOQ, pharmacokinetic calculations were estimated using the LLOQ value to derive a conservative upper-bound estimate. Calculated according to Equation 2, the relative infant exposure was found to be ≤0.0039% for enalapril and ≤0.0061% for enalaprilat.
As DID can fluctuate considerably depending on an infant’s milk intake, exposure was also calculated using the standardized milk intakes of 200 mL/kg/day (early infancy intake) and 150 mL/kg/day (standard infancy intake) to enhance generalizability for exclusively breastfed infants (Cloostermans et al., 2024) (Equations 4 and 5). The relative infant dose (RID), which relates the infant-specific DID (Equation 3) via human milk to the maternal daily dose corrected for weight (Equation 5), was 0.086% for enalapril. Accounting for molar exposure to both enalapril and enalaprilat respectively, the combined RID was 0.202%. When adjusted for standardized milk intake (DID derived from Equation 4), the RID for enalapril was 0.097% and 0.073% for 200 mL/kg/day and 150 mL/kg/day respectively. Total RID accounting for molar exposure to both prodrug and metabolite was then 0.261% and 0.196% for 200 mL/kg/day and 150 mL/kg/day respectively.
Discussion
4
This paper reports the concentrations of enalapril and enalaprilat in human milk, the maternal M/P ratio and the infant exposures, assessed by an infant blood sample, as well as the health outcomes of the breastfed infant at 13 and 21 weeks postpartum.
Our findings show that both enalapril and enalaprilat were detectable in human milk at very low levels, corresponding to an RID of <1%, well below the generally accepted threshold of 10% (Anderson, 2018). The low transfer to the infant was further supported by infant plasma concentrations of both enalapril and enalaprilat below the LLOQ, as well as the absence of reported adverse events during follow-up. It is worth noting, however, that infant blood pressure, which may act as an indicator of adverse events, was not measured (Kiesel et al., 2023). Furthermore, it must be acknowledged that, aside from hospitalizations, unspecified health problems and prescribed medication, no additional adverse events were explicitly monitored in the 2 months following sampling. When comparing the daily infant dose to the therapeutic pediatric dose of enalapril (0.1 mg/kg), the exposure via milk represented less than 0.08%, reinforcing the minimal risk of clinically-relevant drug exposure, particularly in the face of the well-established benefits of breastfeeding. These data add to the limited existing literature on the pharmacokinetics and safety of enalapril during lactation, which to date includes only eight historically reported mother-infant pairs (Huttunen et al., 1989; Redman et al., 1990), and provide further support for the safety of enalapril during lactation. Moreover, this paper is the first of its kind to measure infant plasma concentrations of enalapril and enalaprilat in a breastfed infant whose mother was receiving 5 mg of enalapril daily, thereby providing direct evidence of minimal exposure through human milk during pharmacotherapy.
Notably, our quantitative results align with previous case series of enalapril during breastfeeding, where milk concentrations were low (M/P ratios ≤0.043 and 0.31) and infant outcomes were reassuring (Huttunen et al., 1989; Redman et al., 1990). Interestingly, although the studies suggested a dose-dependent relationship between enalapril dose and enalaprilat detection in human milk, with Huttunen et al. unable to detect enalaprilat 4 hours after a 5–10 mg dose, we detected enalaprilat in human milk up to 22 h post-administration, albeit at low concentrations. This prolonged presence may be explained by the impaired renal function in our patient, which is associated with higher plasma drug concentrations (Elung-Jensen et al., 2003; Kelly et al., 1986). Among the mothers in previous studies, renal function was reported for only one participant with chronic glomerulonephritis (serum creatinine: 0.89 mg/dL, creatinine clearance: 60 mL/min/1.73 m^2^). Our findings are therefore particularly reassuring, even in the context of moderate renal impairment (CKDG3), since infant exposure remained well below clinically relevant thresholds. Furthermore, given the enhanced sensitivity of contemporary bioanalysis techniques, our results are even more compelling.
The limited transfer of enalapril and enalaprilat to human milk, even in the context of CKDG3, can be explained by their pharmacological properties. Both enalapril and enalaprilat are weak acids with low lipophilicity, low-to-moderate molecular weights (enalapril 376.45 and enalaprilat 384.43), and moderate protein binding, up to 50% (Davies et al., 1984; European Bioinformatics Institute, 1985; Ranadive et al., 1992). While their small size and moderate protein binding could favor passive diffusion, the combination of weak acidity and low lipophilicity likely limits transfer into slightly acidic human milk (Anderson, 2018; Beardmore et al., 2002). Consequently, ACE inhibitors, and therefore enalapril, present some of the safest medications to use during breastfeeding in the management of hypertension (Piotrkowicz et al., 2025). Although enalapril currently remains the preferred option, captopril use during breastfeeding is also accepted (Devlin and Fleiss, 1981; Ghelfi et al., 2021; Huttunen et al., 1989; Parnizari et al., 2025; Piotrkowicz et al., 2025; Redman et al., 1990). Exploratory findings further support the safe use of quinapril, benazepril, perindopril and lisinopril, which appear to demonstrate RIDs of 1.6%, <0.14%, 0.0005%–0.2% and 0.06%, respectively, with no documented infant adverse effects (Begg et al., 2001; Chugh et al., 2025; Kaiser et al., 1989; Leggett et al., 2020).
Despite these reassuring findings, current clinical guidelines remain inconsistent, contributing to ongoing uncertainty among clinicians and mothers (Parnizari et al., 2025). While the American College of Obstetricians and Gynecologists (ACOG, 2019) considers low-dose use compatible with breastfeeding, the FDA, as well as the EMA adopt a more cautious stance, advising mothers to choose between treatment and breastfeeding, particularly in preterm infants and neonates (Colaceci et al., 2015; EMA, 2025; FDA, n.d.; MHRA, 2009). This hesitance is likely maintained by the understanding of ontogenetic changes in enalapril metabolism and increased ACE-sensitivity of neonatal kidneys (Boberg et al., 2017; Kearns et al., 2003; Ku et al., 2017). Furthermore, case reports have been published, albeit infrequently, detailing enalapril-induced adverse renal events including hypotension, renal failure and acute kidney injury in neonates who had received therapeutic doses of enalapril (0.07–0.1 mg/kg) for hypertension (Kanic et al., 2021; Schilder and Van den Anker, 1995). It is, however, worth noting that no adverse events have been reported in infants following exposure to enalapril through human milk (Piotrkowicz et al., 2025) and that the European project LENA is expected to address the knowledge gap surrounding pediatric use of the drug in the context of pediatric heart disease (Bajcetic et al., 2019).
Several methodological limitations should be acknowledged. First, milk sampling and preliminary storage were completed at the patient’s home, which may introduce uncertainty regarding strict protocol adherence and storage conditions, but also reflects the pragmatism and feasibility of the UmbrelLACT study (Van Neste et al., 2024). Second, milk volume measurements using an electric pump may be inaccurate. Yield could be overestimated because infants do not routinely empty both breasts (Anderson and Sauberan, 2016), or underestimated in some mothers due to suboptimal stimulation or stress associated with pumping (Kent et al., 2003). Although the risk of intraindividual variability remains low (Gardner et al., 2015), variability in hind- and foremilk fat content could influence measured drug concentrations. While enalapril is not strongly lipophilic, differences in milk composition may still affect sample concentrations and remain unknown for enalapril. Third, insufficient maternal plasma samples were available to calculate M/P ratios over the full 24 h, necessitating reliance on literature-derived plasma AUC from non-breastfeeding, non-postpartum adults, which do not account for the physiological changes of pregnancy or lactation (Van Neste et al., 2023). Furthermore, these reference AUC values were obtained from adults without CKD and represented rather than 24-h values, likely increasing the error margins in M/P ratios and overall infant exposure estimates, leading to an overall underestimation, although this would not impact calculations of DID and RID. Finally, the infant included in this report was older than 3 months, limiting generalizability of our findings to neonates in the first weeks of life and to prematurely born infants, who may be more vulnerable. Nevertheless, the low measured infant plasma concentration provides direct evidence that systemic exposure was minimal.
Despite these limitations, our findings add to the reassuring evidence base for enalapril during lactation in patients with mildly impaired renal function. Infant exposure appears negligible, with no short-term adverse outcomes reported. Given the substantial benefits of breastfeeding for both mother and infant, these results suggest that maternal enalapril therapy may be compatible with breastfeeding in similar clinical scenarios. To strengthen the evidence base, further systematic pharmacokinetic studies are needed, particularly in the early postpartum period and among high-risk populations, following structured frameworks such as the Milk4Baby decision tree to guide the selection of appropriate methodologies (Monfort et al., 2025). In addition, physiologically based pharmacokinetic (PBPK) modeling present a way to predict infant exposure using minimal clinical samples, with the ability to account for changes in maternal physiology and infant enzyme maturation (Nauwelaerts et al., 2023). This approach, evaluated by clinical real-world data, could be used to refine clinical recommendations and reduce unnecessary treatment discontinuation or avoidance of breastfeeding, in addition to contributing to the establishment of much needed teratology and breastfeeding-related information services (Ceulemans et al., 2022).
In conclusion, this case report is the first to include infant plasma sampling in the investigation of mother-infant enalapril and enalaprilat transfer. Overall, we found low concentrations of enalapril and enalaprilat in human milk, resulting in negligible infant exposure, with no short-term adverse events observed. Taken with prior reports, these findings support the safety of enalapril therapy during breastfeeding. However, additional data collection and PBPK simulations, are needed to capture pharmacokinetic variability, particularly in neonates and preterm infants, and to confirm safety across different maternal and infant populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ACOG (2019). ACOG practice bulletin no. 203: chronic hypertension in pregnancy. Obstet. Gynecol. 133, e 26–e 50. 10.1097/AOG.0000000000003020 30575676 · doi ↗ · pubmed ↗
- 2Anderson P. O. (2018). Drugs in lactation. Pharm. Res. 35, 1–13. 10.1007/s 11095-017-2287-z 29411152 · doi ↗ · pubmed ↗
- 3Anderson P. O. (2022). Guidelines for reporting cases of medication use during lactation. Breastfeed. Med. 17, 93–97. 10.1089/bfm.2021.0357 35073165 · doi ↗ · pubmed ↗
- 4Anderson P. O. Sauberan J. B. (2016). Modeling drug passage into human milk. Clin. Pharmacol. Ther. 100, 42–52. 10.1002/cpt.377 27060684 · doi ↗ · pubmed ↗
- 5Andreas N. J. Kampmann B. Mehring Le-Doare K. (2015). Human breast milk: a review on its composition and bioactivity. Early Hum. Dev. Spec. Issue Neonatal Update 91, 629–635. 10.1016/j.earlhumdev.2015.08.013 26375355 · doi ↗ · pubmed ↗
- 6Bajcetic M. de Wildt S. N. Dalinghaus M. Breitkreutz J. Klingmann I. Lagler F. B. (2019). Orodispersible minitablets of enalapril for use in children with heart failure (LENA): rationale and protocol for a multicentre pharmacokinetic bridging study and follow-up safety study. Contemp. Clin. Trials Commun. 15, 100393. 10.1016/j.conctc.2019.100393 31249901 PMC 6586986 · doi ↗ · pubmed ↗
- 7Beardmore K. S. Morris J. M. Gallery E. D. M. (2002). Excretion of antihypertensive medication into human breast milk: a systematic review. Hypertens. Pregnancy 21, 85–95. 10.1081/PRG-120002912 12044345 · doi ↗ · pubmed ↗
- 8Begg E. J. Robson R. A. Gardiner S. J. Hudson L. J. Reece P. A. Olson S. C. (2001). Quinapril and its metabolite quinaprilat in human milk. Br. J. Clin. Pharmacol. 51, 478–481. 10.1046/j.1365-2125.2001.01327.x 11422007 PMC 2014479 · doi ↗ · pubmed ↗