Risk factors for residual acetabular dysplasia after closed reduction treatment of developmental dysplasia of the hip: a systematic review and meta-analysis
Min Chen, Jun Qian, Li Weng, Ai-Xia Zhang, Ru-Yi Cai

TL;DR
This study identifies female sex and femoral head coverage as risk factors for residual hip issues after treatment for developmental hip dysplasia in children.
Contribution
The study provides the first meta-analysis identifying specific risk factors for residual acetabular dysplasia after closed reduction treatment for DDH.
Findings
Female sex is a risk factor for residual acetabular dysplasia after treatment.
Femoral head coverage is a significant predictor of residual acetabular dysplasia.
Factors like treatment age and acetabular index were not found to be significant risk factors.
Abstract
Residual acetabular dysplasia (RAD) is a common complication following closed reduction (CR) for developmental dysplasia of the hip (DDH). This study aims to perform a meta-analysis to identify predictive factors for RAD in order to provide a theoretical basis for early clinical identification and prevention. A comprehensive literature search was conducted in PubMed, Embase, Web of Science, and the Cochrane Library databases, covering the period from database inception to November 2024. The quality of the included studies was assessed using the Newcastle–Ottawa Scale, and data analysis was performed using StataSE-64 and RevMan 5.4 software. The odds ratio (OR) and 95% confidence interval (CI) were used for data synthesis. Evidence for all outcomes was graded according to the GRADE system. This meta-analysis included 16 studies, including a total of 1,338 children who underwent CR for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
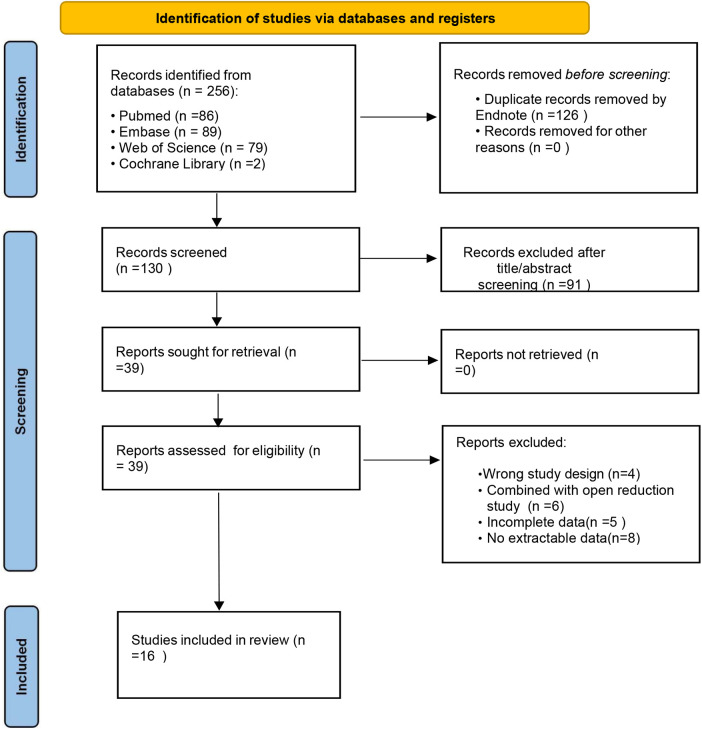 Figure 1
Figure 1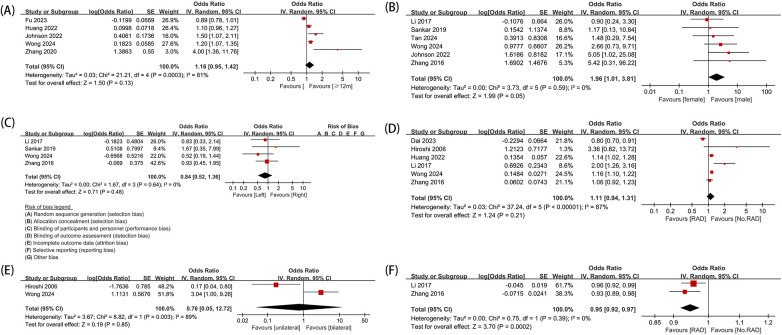 Figure 2
Figure 2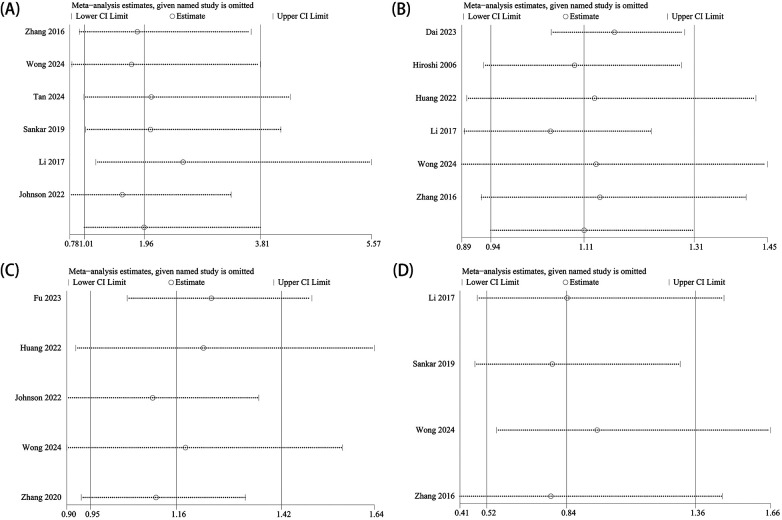 Figure 3
Figure 3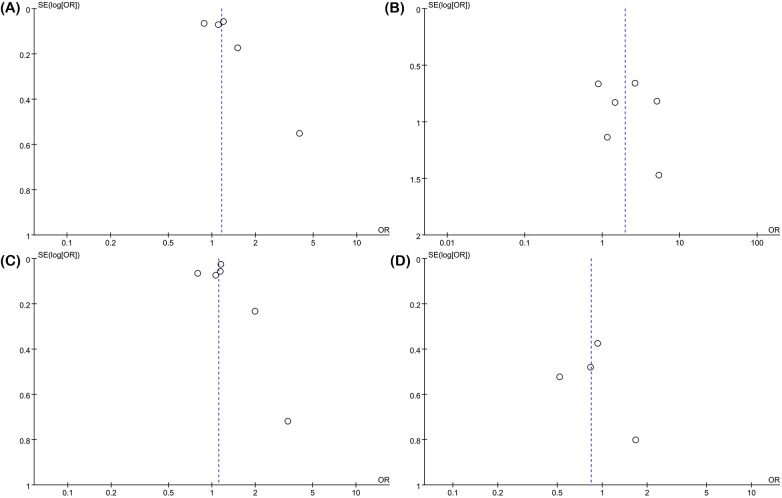 Figure 4
Figure 4| Author | Study period | Region | Study design | Population | Predictive factors | Diagnostic criteria for residual dysplasia | Total hips analyzed ( | Notes (demographics) | Number of cases | Follow-up | Mean/median age | Types of residual dysplasia | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | ||||||||||||
| William 2022 | 1980–2016 | Britain | Retrospective | 165 patients with DDH who underwent closed reduction. | Folded limbus and severity of dislocation | X-ray | 182 | (Case composition not specified in the original study) | NR | NR | 9 ± 4.9y | 9.8 ± 4.5m | Residual dysplasia, ischemic necrosis |
| Johnson 2022 | 2009–2019 | USA | Reprospective | 48 patients who underwent open or closed reduction. | Gender, age at reduction, CAI, and posterior cartilage acetabular angle | MRI | 63 | (Case composition not specified in the original study) | NR | NR | 35.3 ± 4.9m | 9.3 ± 3.2m | Residual dysplasia |
| Hiroshi 2006 | 1964–1988 | Japan | Retrospective | 40 DDH patients who underwent closed reduction with overhead traction (OHT). | Age, severity of dislocation, AI, CE, and CHDD | X-ray | 45 | [40 patients: 37 females and 3 males; 35 unilateral cases (25 left and 10 right) and 5 bilateral cases] | 3 cases | 37 cases | 15.1–29.5y | 9.3m | Acetabular dysplasia |
| Li 2017 | 2004–2013 | China | Retrospective | 89 DDH patients who underwent closed reduction. | AI, CEA, RI, and CHDD | X-ray | 99 | (89 patients: 99 hips, unilateral 79 patients and bilateral 10 patients) | 13 cases | 76 cases | 61.6 ± 17.7m | 16.1 ± 4.6m | Residual acetabular dysplasia |
| Sankar 2019 | 2010–2014 | USA | Prospective | 78 DDH patients who underwent closed reduction. | Age at reduction, previous orthotic treatment, and history of femoral head reducibility | X-ray | 87 | (78 patients: majority female; median age at CR: 8 months; 33% bilateral cases; 16% breech history; 29% family history of DDH) | 10 cases | 68 cases | 22m | 12–36m | Residual dysplasia |
| Tan 2024 | 2014–2020 | China | Retrospective | DDH children who underwent closed reduction and spica casting for more than 6 months. | FHC, MDP, labral inversion, and quality of reduction | X-ray | 110 | (102 patients: 94 females and 8 males; 60 left hips, 34 right hips, and 8 bilateral cases; mean age at CR: 14.6 months) | 8cases | 94cases | 58.5 ± 24.8m | 14.6 ± 4.7m | Residual acetabular dysplasia/AVN |
| Zhang 2016 | 2006–2013 | China | Retrospective | 126 DDH patients who underwent closed reduction under arthrography guidance. | Arthrography type, FHC, AI, and CE | X-ray | 139 | (126 patients: 103 females, 23 males; 88 left hips and 51 right hips; mean age at CR: 14 months) | 23 cases | 103 cases | 36m | 14m | Residual dysplasia |
| Meng 2021 | 2012–2018 | China | Prospective | MRI and X-ray evaluation before and after closed reduction in unilateral DDH patients. | LCC | MRI、X-ray | 63 | (63 patients: 61 females and 2 males; 39 left hips, 24 right hips; mean age at CR: 15.6 months) | 2 cases | 61 cases | 138.6 ± 24.1d | 15.6 ± 4.4 | Residual acetabular dysplasia |
| Fu 2023 | 2016–2020 | China | Retrospective | 86 DDH patients who underwent closed reduction and spica casting. | LACC and FTD | MRI | 92 | (86 patients: 81 females and 5 males; 80 unilateral and 6 bilateral; mean age at CR: 13.6 months) | 5 cases | 81 cases | ≥3y | 13.6m | Residual dysplasia |
| Dai 2023 | 2011–2017 | China | Reprospective | 82 patients older than 12 months who successfully underwent closed reduction and were followed up for at least 2 years. | AI, AWh, CEA, and FHC | MRI、X-ray | 107 | (82 patients: 69 females and 13 males; 57 unilateral cases: 33 left and 24 right, and 25 bilateral cases) | 13 cases | 69 cases | 47.8 ± 16.6m | 3.8m | Residual dysplasia |
| Wong 2024 | 1970–2010 | China | Reprospective | DDH patients who underwent closed reduction and were followed up until skeletal maturity. | AI, age, and lateral center-edge angle | X-ray | 107 | (96 females, 11 males; 62 left hips and 45 right hips; mean age at CR: 8 months; follow-up to skeletal maturity) | 11 cases | 96 cases | 20y | 8m | Residual acetabular dysplasia |
| Arenas-Díaz 2024 | 2015–2016 | Mexico | Reprospective | 66 DDH patients who underwent closed reduction with two different fixation techniques. | Modified Lange's “second position” | X-ray | 84 | [66 patients (gender distribution: 89.3% female and 10.7% male); median age 8 months] | 7 cases | 59 cases | ≥48m | 8m | Residual dysplasia, AVN, and redislocation |
| Ge 2016 | 2010–2013 | China | Prospective | 28 DDH patients who underwent closed reduction. | Hip abduction angle, initial AI, final AI, preoperative Tönnis classification, and postreduction FAD | MRI | 41 | [28 patients (4 males and 24 females); mean age 8.6 months; left 21 hips and right 20 hips] | 4 cases | 24 cases | 17.7m | 8.6m | Residual acetabular dysplasia/AVN |
| Yasin 2022 | 2016–2019 | Jordan | Reprospective | 47 patients who underwent closed reduction with long or short spica casting. | Long spica casting and short spica casting | CT | 47 | [47 patients (91.5% female, 8.5% male); median age 7.83 months; 19 bilateral cases (40.4%)] | 4 cases | 43 cases | 1y | 7.83m | Residual dysplasia, AVN, redislocation |
| Huang 2022 | 2011–2017 | China | Reprospective | 104 DDH patients who underwent closed reduction and were followed up for at least 2 years. | TSL, AI, age, and IHDI classification | MRI | 125 | [104 patients (13 males and 91 females); mean age 18.3 months] | 13 cases | 91 cases | 50.2m | 18.3m | Residual acetabular dysplasia |
| Zhang 2020 | 2011–2013 | China | Reprospective | 107 DDH patients who underwent closed reduction. | Age | X-ray | 156 | [107 patients (12 males and 95 females); median age 13.0 months] | 12 cases | 95 cases | 6.7 ± 0.8y | 13.0 ± 5.4m | Residual dysplasia, AVN, and redislocation |
| Outcome | OR | 95% CI |
|
|---|---|---|---|
| Wiberg center-edge angle (CEA) | 0.0744 | 0.0208–0.2666 | 0.0001 |
| Preoperative acetabular index (AI) | 1.225 | 1.025–1.464 | 0.026 |
| Cartilage acetabular index (CAI)>23 | 1.133 | 1.006–1.276 | 0.040 |
| Posterior cartilage acetabular angle | 0.763 | 0.599–0.972 | 0.029 |
| Reimers’ index (RI) | 1.086 | 1.017–1.161 | 0.014 |
| Femoral head to triradiate cartilage distance (FTD) | 0.514 | 0.307–0.859 | 0.011 |
| Immobilization duration | 1.054 | 1.006–1.104 | 0.027 |
| Preoperative acetabular width (AWh) | 0.006 | 0.01–0.384 | 0.016 |
| Acetabular width (AWh) | 0.026 | 0.002–0.296 | 0.0053 |
| Tönnis classification grade III/IV | 4.80 | 1.147–20.085 | 0.032 |
| Teardrop and teardrop line (TSL) | 0.214 | 0.083–0.552 | 0.001 |
| Family history | 3.333 | 0.689–16.126 | 0.134 |
| Femoral head width | 1.253 | 0.97–1.617 | 0.0849 |
| Center-head distance difference (CHDD) | 0.956 | 0.814–1.123 | 0.583 |
| Femoral head ossification nucleus | 0.446 | 0.174–1.148 | 0.093 |
| Limbus inversion | 0.262 | 0.018–3.814 | 0.327 |
| Limbus folding | 1.285 | 0.599–2.756 | 0.520 |
| Complete concentric reduction | 5.4167 | 1.249–23.489 | 0.002 |
| AI <30° and CEA >5° at the age of 5 or 6 years | 4.889 | 1.246–19.190 | 0.023 |
| Risk factors | No. of studies | OR | 95% CI | Risk of bias | Inconsistency | Indirectness | Imprecision | Publication bias | Plausible confounding | Magnitude of effect | Dose–response gradient | GRADE | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender (female vs. male) | 6 | 1.96 | 1.01, 3.81 | 0%; | No serious risk | No serious | No serious | Serious | Undetected | Would not | No | No | Very low |
| Side (left vs. right) | 4 | 0.84 | 0.52, 1.36 | 0%; | No serious risk | No serious | No serious | Serious | Undetected | Would not | No | No | Very low |
| DDH involvement (unilateral vs. bilateral) | 2 | 0.76 | 0.05, 12.72 | 89%; | No serious risk | Serious inconsistency | No serious | Serious | NA | Would not | No | No | Very low |
| AI | 6 | 1.11 | 0.94, 1.31 | 87%; | No serious risk | Serious inconsistency | No serious | Serious | Undetected | Would not | No | No | Very low |
| FHC | 2 | 0.95 | 0.92, 0.97 | 0%; | No serious risk | No serious | No serious | No serious | NA | Would not | No | No | Low |
| Treatment age (<1 year vs. ≥1 year) | 5 | 1.16 | 0.95, 1.42 | 81%; | No serious risk | Serious inconsistency | No serious | Serious | Undetected | Would not | No | No | Very low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip disorders and treatments · Orthopaedic implants and arthroplasty · Bone fractures and treatments
Introduction
1
Developmental dysplasia of the hip (DDH) is one of the most common structural deformities in children and encompasses a spectrum of abnormalities ranging from mild hip joint underdevelopment to complete hip dislocation (1). The condition occurs more frequently in females, with the left hip more commonly affected than the right (2, 3). DDH is the most common developmental disorder of the lower limbs in pediatric orthopedics and is a major cause of disability in children. Studies have indicated (4, 5) that up to 76% of hip osteoarthritis cases in adults are secondary to untreated DDH in childhood. Without timely diagnosis and intervention, DDH can lead to progressive degenerative changes in the hip joint, ultimately resulting in disability and severely affecting long-term quality of life.
Early diagnosis and treatment of DDH enable concentric reduction of the acetabulum and femoral head at an early stage, allowing the hip joint to develop to a level comparable to that of a normal hip (6, 7). For children aged 6–18 months, closed reduction (CR) under anesthesia followed by spica cast fixation is considered the gold standard for treatment (8, 9). It can successfully treat children who have failed Pavlik harness therapy as well as those with late-diagnosed DDH. However, complications such as iatrogenic avascular necrosis (AVN), redislocation, and residual acetabular dysplasia (RAD) following CR have also raised significant clinical concerns. Among these, RAD remains the most common complication after CR, affecting more than one-third of patients, with its incidence increasing with age. In a study by Huang et al. (10), the rate of incidence of RAD reached 73.6%, the highest reported to date. RAD is often asymptomatic in its early stages, making early detection challenging. If left untreated, it can lead to reduced weight-bearing capacity of the lower limb joints, gait abnormalities, and chronic osteoarthritis, potentially resulting in redislocation and the need for pelvic osteotomy (11, 12). Moreover, certain complications remain inevitable even after osteotomy (13).
Currently, the risk factors for RAD after CR have been extensively studied. Wong et al. (14) conducted a study with an average follow-up of 20 years and identified that the acetabular index and age were important predictive factors for RAD. However, in a study by Dai et al. (15), although the incidence of RAD was higher in children over 18 months and those aged 12–18 months, the age-related difference was not statistically significant. To date, there remains no consensus regarding which factors increase the risk of RAD after CR in children with DDH. This study employed the PICOS framework to define the inclusion and exclusion criteria. We then conducted a systematic review and meta-analysis to identify the risk factors associated with RAD following CR. By synthesizing current clinical evidence and evaluating all relevant variables, this study provides a robust and up-to-date foundation for evidence-based practice. This comprehensive analysis, by pooling data across studies, provides a larger aggregate sample size than individual studies, thereby enhancing statistical power and offering a more robust foundation for evidence-based practice compared with conclusions drawn from single, small-sample studies.
Materials and methods
2
Protocol and registration
2.1
This systematic review and meta-analysis was conducted in accordance with the PRISMA 2020 statement and was registered in the PROSPERO database (CRD420251016618).
Literature search
2.2
The literature search was conducted using PubMed, Web of Science, Embase, and the Cochrane Library. The following terms were used in the search: “residual dysplasia,” “closed reduction,” and “developmental dysplasia of the hip.” The PubMed search query was as follows: [(residual dysplasia) AND (closed reduction)] AND [“Developmental Dysplasia of the Hip"(Mesh) OR Developmental Hip Dysplasia OR Developmental Hip Dislocation OR DDH”]. The search period covered all publications from database inception to November 2024. The search was conducted using a combination of Medical Subject Headings (MeSH) terms and free-text keywords, while also reviewing the references of included studies. EndNote X9 was used to manage and screen all the collected studies. The detailed literature search strategy is depicted in Supplementary Table S1.
Inclusion and exclusion criteria for literature
2.3
This study establishes strict inclusion and exclusion criteria based on the PICOS (Population, Intervention, Comparison, Outcome, Study design) framework to ensure a systematic and transparent approach to the clinical question. The inclusion criteria are as follows: (1) The study subjects are DDH patients who have undergone CR; (2) the study reports predictive factors/risk factors for RAD after CR and provides OR values and 95% CI, or OR values and 95% CI can be obtained through data conversion; (3) the study contains clear diagnostic criteria for RAD; and (4) the study is a cohort or case-control study. Exclusion criteria: (1) articles published more than once or based on the same sample; (2) studies with no data or incomplete data; (3) articles unrelated to this study; (4) conference papers, case reports, reviews, or meta-analyses; and (5) articles not published in English.
Literature screening and data extraction
2.4
Two researchers independently screened the literature, extracted data, and cross-checked the studies according to the inclusion and exclusion criteria. Any disagreements during this process were discussed and resolved through negotiation between the two researchers. If the disagreement persisted, a senior researcher was consulted to make the final decision. The extracted data included the following: author, publication year, study year, study type, characteristics of the study subjects, predictive factors, diagnostic criteria for RAD, the number of cases by sex (male/female), follow-up duration, treatment age at CR (categorized as <1 year or ≥1 year), and other relevant risk factors.
Literature quality assessment
2.5
The quality of the cohort studies and case-control studies was evaluated using the Newcastle–Ottawa Scale (NOS) (16). The NOS evaluates studies across three domains: selection of study groups, comparability between groups, and assessment of exposure or outcome. The maximum score is 9 points, with scores of 0–5 indicating low-to-moderate quality and scores ≥6 indicating high quality. Only high-quality studies were included in this review. The quality assessment was performed independently by two researchers, and any disagreements were resolved through discussion. If consensus could not be reached, a third senior researcher was consulted to make the final decision.
Statistical methods
2.6
Statistical analyses were conducted using RevMan 5.4 and StataSE-64 software. The odds ratio (OR) with a 95% confidence interval (CI) was used as the effect measures, and a random-effects model was applied to calculate pooled estimates. A sensitivity analysis was conducted using the leave-one-out method to evaluate the reliability and stability of the results. Publication bias was assessed using funnel plots and Egger's test, with a p-value < 0.05 regarded as the threshold for statistical significance. The GRADE framework was applied to assess the quality of evidence for each outcome and classify it as “high,” “moderate,” “low,” or “very low” (17).
Results
3
Literature search results
3.1
A total of 256 records were retrieved from the databases. After removing 126 duplicates, 91 records were eliminated by reviewing the titles and abstracts. Based on the inclusion and exclusion criteria, the full texts were then thoroughly examined, and studies that were unrelated to the research topic, lacked data, or were not published in English were excluded. Finally, 16 studies were included in the analysis. Among these, 13 were retrospective, and three were prospective, covering a total of 1,338 children who underwent closed reduction treatment for DDH. A flowchart of literature screening is presented in Figure 1, and the basic characteristics of the included studies are presented in Table 1.
A PRISMA flowchart for the systematic review and meta-analysis.
Literature quality assessment
3.2
The 16 included studies (10, 14, 15, 18–30) were evaluated for methodological quality using the NOS, with scores ranging from 6 to 9, indicating that the overall quality of the included literature was high. The detailed quality assessment results can be found in Supplementary Tables S2, S3.
Meta-analysis
3.3
Treatment age (<1 year vs. ≥1 year)
3.3.1
A total of five studies were included. The results showed no statistically significant difference between children aged <1 year and those aged ≥1 year (OR: 1.16; 95% CI: 0.95–1.42); however, the substantial heterogeneity (I^2^ = 81%) precludes a definitive conclusion regarding the association between treatment age (dichotomized at 1 year) and RAD (Figure 2A).
Forest map. (A)Treatment age; (B) gender; (C) side (left/right); (D) acetabular index (AI); (E) number of affected sides in DDH (unilateral/bilateral); and (F) femoral head coverage (FHC).
Gender
3.3.2
A total of six studies were included. The results showed a significant difference in the occurrence of RAD after CR between females and males (OR: 1.96; 95% CI: 1.01–3.81; I^2^ = 0%), indicating that being female is a risk factor for RAD, with a significantly higher incidence in females compared with males (Figure 2B).
Side (left/right)
3.3.3
A total of four studies were included. The statistical analysis showed no significant difference in the occurrence of RAD between the left and the right hips (OR: 0.84; 95% CI: 0.52–1.36; I^2^ = 0%), suggesting that the side of the affected hip is not a risk factor for RAD after CR treatment (Figure 2C).
Acetabular index
3.3.4
A total of six studies were included. The results did not show a significant association between the acetabular index (AI) after CR and the occurrence of RAD (OR: 1.11; 95% CI: 0.94–1.31; I^2^ = 87%), indicating that AI is not a risk factor for this complication (Figure 2D).
Number of affected sides in DDH (unilateral/bilateral)
3.3.5
A total of two studies were included. The results of the analysis showed no significant difference in the occurrence of RAD after CR treatment, regardless of whether the hip joint had unilateral or bilateral DDH (OR: 0.76; 95% CI: 0.05–12.72; I^2^ = 89%) (Figure 2E).
Femoral head coverage
3.3.6
A total of 2 studies were included. The results showed a significant association between femoral head coverage (FHC) and the occurrence of RAD after CR (OR: 0.95; 95% CI: 0.92–0.97; I^2^ = 0%). These findings indicate that FHC can serve as a predictive factor for RAD after closed reduction treatment (Figure 2F).
Other indicators
3.3.7
In addition to the above indicators, which were analyzed based on two studies, there are 18 other indicators, each examined in only one study. Because of the limited data, these indicators were not included in the meta-analysis. A systematic summary of these factors is presented below.
The Wiberg center-edge angle (CEA) (21) (OR = 0.0744, 95% CI: 0.0208–0.2666, p = 0.0001), preoperative AI (15) (OR = 1.225, 95% CI: 1.025–1.464, p = 0.026), cartilage acetabular index (CAI) > 23 (26) (OR = 1.133, 95% CI: 1.006–1.276, p = 0.040), posterior cartilage acetabular angle (26) (OR = 0.763, 95% CI: 0.599–0.972, p = 0.029), Reimers’ index (RI) (21) (OR = 1.086, 95% CI: 1.017–1.161, p = 0.014), femoral head to triradiate cartilage distance (FTD) (26) (OR = 0.514, 95% CI: 0.307–0.859, p = 0.011), immobilization duration (26) (OR = 1.054, 95% CI: 1.006–1.104, p = 0.027), preoperative acetabular width (AWh) (15) (OR = 0.006, 95% CI: 0.01–0.384, p = 0.016), AWh (15) (OR = 0.026, 95% CI: 0.002–0.296, p = 0.0053), Tönnis classification grade III/IV (14) (OR = 4.80, 95% CI: 1.147–20.085, p = 0.032), and teardrop line (TSL) (10) (OR = 0.214, 95% CI: 0.083–0.552, p = 0.001) were identified as risk factors for RAD.
On the other hand, family history (22) (OR = 3.333, 95% CI:0.689–16.126, p = 0.134), femoral head width (26) (OR = 1.253, 95% CI:0.97–1.617, p = 0.0849), center-head distance difference (CHDD) (21) (OR = 0.956, 95% CI:0.814–1.123, p = 0.583), femoral head ossification nucleus (23) (OR = 0.446, 95% CI:0.174–1.148, p = 0.093), limbus inversion (23) (OR = 0.262, 95% CI:0.018–3.814, p = 0.327), and limbus folding (18) (OR = 1.285, 95% CI:0.599–2.756, p = 0.520) were not considered risk factors for RAD (Table 2).
Complete concentric reduction (28) (OR = 5.4167, 95% CI: 1.249–23.489, p = 0.002) and AI <30° and CEA >5° at the age of 5 or 6 years (20) (OR = 4.889, 95% CI: 1.246–19.190, p = 0.023) were identified as protective factors against RAD (Table 2).
Sensitivity analysis
3.4
A leave-one-out approach was applied for the sensitivity analysis to evaluate the risk factors for RAD after CR in children with DDH. The results showed that after excluding the studies by Zhang et al. (24), Wong et al. (14), and Johnson et al. (19), the significance of the sex indicator changed from significant to non-significant (Figure 3A). After excluding the studies by Hiroshi et al. (20), Huang et al. (10), Li et al. (21), Wong et al. (14), and Zhang et al. (24), the significance of the AI indicator changed from non-significant to significant (Figure 3B). After excluding the studies by Huang et al. (10), Johnson et al. (19), Wong et al. (14), and Zhang et al. (30), the significance of the treatment age indicator in the combined subgroup changed from non-significant to significant (Figure 3C). Excluding any individual study did not affect the significance of the left/right side combined subgroup (Figure 3D).
Sensitivity analysis. (A) Gender; (B) acetabular index (AI); (C) treatment age; and (D) side (left/right).
Publication bias
3.5
Egger's test and funnel plots were used to assess publication bias. The results of Egger's test indicated no significant publication bias for treatment age (P = 0.281), sex (P = 0.589), AI (P = 0.892), and side (P = 0.702). Similarly, the funnel plots confirmed the absence of publication bias for treatment age (Figure 4A), sex (Figure 4B), AI (Figure 4C), and side (Figure 4D). For the remaining indicators, due to the limited number of studies, publication bias analysis could not be performed.
Funnel map. (A) Treatment age; (B) gender; (C) acetabular index (AI); and (D) side (left/right).
GRADE rating
3.6
In the GRADE assessment of indicators such as sex, side (left/right), number of affected hip joints (unilateral/bilateral), AI, FHC, and treatment age, the FHC indicator was classified as “low.” Meanwhile, the indicators sex, side, number of affected hip joints, AI, and treatment age were classified as “very low” quality. Detailed GRADE analysis results can be found in Table 3.
Discussion
4
RAD is the most common complication after CR for DDH. Multiple long-term follow-up studies have found that the rate of RAD after CR is as high as 35%–58% (11, 31, 32). In addition, the rate of prevalence of secondary osteoarthritis caused by acetabular dysplasia after DDH treatment is reported to range between 43% and 50% (33, 34). Therefore, early identification of hips that do not demonstrate adequate improvement and are at risk for RAD after CR is crucial for guiding subsequent management.
This study identified several potential risk factors for RAD after CR, including female sex, FHC, CEA, preoperative AI, CAI > 23, cartilage acetabular posterior angle, RI, distance from the femoral head to the triradiate cartilage, duration of immobilization, AWh, AWh, and Tönnis classification III/IV, as well as the teardrop and TSL. Conversely, complete concentric reduction and an AI <30° or CEA >5° at 5 or 6 years of age were identified as protective factors against RAD after CR. However, there remains disagreement regarding the relationship between treatment age (at 1-year cutoff) and the occurrence of RAD.
Our findings primarily revealed that female sex and the FHC were the main risk factors for the occurrence of RAD after CR. It also found that factors such as the side of DDH occurrence, the number of affected hip joints, AI, and treatment age did not appear to have a clear association with RAD. In the sensitivity analysis of indicators with more than three studies, the study found that the factor of the side of DDH occurrence was stable, while factors such as sex, AI, and treatment age (as dichotomized) were unstable. For these unstable indicators, further research may be needed to confirm these findings, as instability suggests that the results may vary and be overly influenced by individual studies. Therefore, additional evidence is needed to reinforce these conclusions.
In addition, this analysis confirmed that none of the indicators showed publication bias, suggesting that these findings are relatively reliable. All risk factors were analyzed using the GRADE system, in which FHC was identified as the most reliable indicator, with a “low quality” level. The remaining indicators were all classified as “very low quality.” Therefore, in clinical practice, more attention should be paid to FHC, as it demonstrates a relatively stable and reliable association with RAD.
This study is the first meta-analysis to systematically evaluate the risk factors associated with RAD following CR in children with DDH. The results indicate that female sex is a significant predictor of RAD, extending the understanding of its influence beyond the initial onset of DDH to treatment outcomes. Notably, our findings align with those of a recent meta-analysis by Chen et al., which identified female sex as an important risk factor for the development of DDH (35). Rather than representing a repetition of existing knowledge, our results highlight the consistently critical role of female sex across the spectrum of DDH, right from its occurrence and treatment to long-term prognosis.
Existing literature primarily explains the observed sex differences from two perspectives. First, differences in skeletal anatomy may be a fundamental cause. Studies suggest that, compared with males, the inherent structural characteristics of the female acetabulum may render the hip joint less stable during development. This may predispose females to DDH and may also negatively influence postreduction acetabular remodeling outcomes (36). Second, endocrine factors are considered crucial. Some researchers propose that higher estrogen levels in females may lead to increased ligamentous laxity, thereby further exacerbating hip joint instability (37, 38). This hormone-mediated biomechanical environment may simultaneously influence both the susceptibility to DDH and the potential for posttreatment recovery.
Based on the above findings and discussion, this study carries clear clinical significance. It suggests that in the clinical management of DDH, particularly during post-treatment follow-up, special attention should be paid to female patients. For these children, clinicians should consider implementing closer and longer-term imaging follow-up and monitoring to facilitate the timely detection of RAD signs and enable intervention. This approach helps optimize the allocation of medical resources and ultimately improves the long-term prognosis for female DDH patients.
According to the results, FHC was identified as the most significant risk factor compared with the other variables. FHC refers to the proportion of the femoral head covered by the acetabulum, reflecting both the depth of femoral head insertion and acetabulum stability. One study (23) pointed out that during intraoperative joint imaging, an FHC <30% was associated with persistent developmental dysplasia in more than 80% of hips. FHC may serve as an early warning indicator for RAD, aiding in the identification of high-risk patients. For those with lower FHC values, enhanced postoperative monitoring is warranted. Future studies should investigate whether adjunctive interventions—such as bracing or early osteotomy—can improve outcomes in this high-risk subgroup. Greater clinical attention should be devoted to this indicator. Protective factors such as complete concentric reduction and an AI < 30° or CEA > 5° at 5–6 years of age may serve as useful references for prognostic evaluation. The inconsistent findings regarding other variables such as AI and treatment age suggest the need for individualized assessment and caution against reliance on any single parameter.
This analysis has several limitations. First, the overall sample size is relatively small, and each indicator is supported by only a limited number of studies, which may introduce selection bias or confounding factors. Second, most of the included studies are from Asian countries, leading to greater heterogeneity for some indicators, which could affect the results, and the generalizability of the conclusions requires further validation. Third, the sensitivity analysis revealed that indicators such as sex, AI, and treatment age were unstable, and their evidence level may be reduced due to individual studies. Fourth, in the GRADE assessment, only one indicator was rated as low-quality evidence, while the rest were classified as very low quality. Fifth, this study was unable to perform a meta-analysis on the severity of preoperative dislocation (such as Tönnis or IHDI classification). Sixth, this study was also unable to quantify the impact of intraoperative techniques and surgeon-related factors—such as surgeon experience, specific reduction maneuvers, stability assessment, and postoperative immobilization protocols—on the occurrence of RAD. Finally, this study did not analyze the potential interaction between RAD and another significant complication—AVN.
Conclusion
5
This study is the first to rigorously demonstrate, through a meta-analysis, that female sex and FHC are the primary risk factors for RAD following CR in children with DDH, providing an important basis for early clinical identification and risk stratification of high-risk patients. Notably, FHC can serve as an objective intraoperative assessment indicator. Although this study lays a foundation for future research, its conclusions are limited by the small sample size and evidence quality. Consequently, further multicenter prospective clinical studies are warranted to validate these associations and to develop effective preventive strategies for improving long-term patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen M Cai R Zhang A Chi X Qian J. The diagnostic value of artificial intelligence-assisted imaging for developmental dysplasia of the hip: a systematic review and meta-analysis. J Orthop Surg Res. (2024) 19(1):522. 10.1186/s 13018-024-05003-439210407 PMC 11360681 · doi ↗ · pubmed ↗
- 2Tao Z Wang J Li Y Zhou Y Yan X Yang J Prevalence of developmental dysplasia of the hip (DDH) in infants: a systematic review and meta-analysis. BMJ Paediatr Open. (2023) 7(1):e 002080. 10.1136/bmjpo-2023-00208037879719 PMC 10603435 · doi ↗ · pubmed ↗
- 3Wen J Ping H Kong X Chai W. Developmental dysplasia of the hip: a systematic review of susceptibility genes and epigenetics. Gene. (2023) 853:147067. 10.1016/j.gene.2022.14706736435507 · doi ↗ · pubmed ↗
- 4Weinstein SL Casteñada PG Sankar WN Campbell HT Badrinath R. Developmental dysplasia of the hip from birth to adolescence: clear indications and new controversies. Instr Course Lect. (2023) 72:659–72.36534887 · pubmed ↗
- 5de Courtivron B Brulefert K Portet A Odent T. Residual acetabular dysplasia in congenital hip dysplasia. Orthop Traumatol Surg Res. (2022) 108(1S):103172. 10.1016/j.otsr.2021.10317234896582 · doi ↗ · pubmed ↗
- 6Kuitunen I Uimonen MM Haapanen M Sund R Helenius I Ponkilainen VT. Incidence of neonatal developmental dysplasia of the hip and late detection rates based on screening strategy: a systematic review and meta-analysis. JAMA Netw Open. (2022) 5(8):e 2227638. 10.1001/jamanetworkopen.2022.2763835980635 PMC 9389349 · doi ↗ · pubmed ↗
- 7Ma S Zhou W Li L Wang E Zhang L Li Q. Retrospective comparison of outcomes between closed and open reduction for developmental dysplasia of the hip in children aged 6–24 months. Indian J Orthop. (2022) 56(9):1640–6. 10.1007/s 43465-022-00690-936052390 PMC 9385909 · doi ↗ · pubmed ↗
- 8Tomlinson J O'Dowd D Fernandes JA. Managing developmental dysplasia of the hip. Indian J Pediatr. (2016) 83(11):1275–9. 10.1007/s 12098-016-2160-927246825 · doi ↗ · pubmed ↗