An improved YOLOv10-based framework for knee MRI lesion detection with enhanced small object recognition and low contrast feature extraction
Hongwei Yang, Wenqu Song, Tiankai Jiang, Chuanhao Wang, Luping Zhang, Zhian Cai, Yuhan Sun, Qing Zhao, Yuyu Sun

TL;DR
This paper introduces an improved YOLOv10-based framework for detecting ACL lesions in knee MRI scans, enhancing detection of small and low-contrast lesions.
Contribution
The novel framework integrates a C2f-SimAM module, an Adaptive Spatial Fusion module, and a hybrid loss function to improve small object recognition and low-contrast feature extraction.
Findings
The model achieves a 1.3% increase in [email protected] compared to standard YOLOv10 (p < 0.05).
It improves [email protected]:0.95 by 2.5% over baseline models.
The framework reduces false negatives in detecting small, low-contrast ACL tears.
Abstract
To address the challenges in detecting anterior cruciate ligament (ACL) lesions in knee MRI examinations, including difficulties in identifying tiny lesions, insufficient extraction of low-contrast features, and poor modeling of irregular lesion morphologies, and to provide a precise and efficient auxiliary diagnostic tool for clinical practice. An enhanced framework based on YOLOv10 is constructed. The backbone network is optimized using the C2f-SimAM module to enhance multi-scale feature extraction and spatial attention; an Adaptive Spatial Fusion (ASF) module is introduced in the neck to better fuse multi-scale spatial features; and a novel hybrid loss function combining Focal-EIoU and KPT Loss is employed. To ensure rigorous statistical evaluation, we utilized a five-fold cross-validation strategy on a dataset of 917 cases. Evaluation on the KneeMRI dataset demonstrates that the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
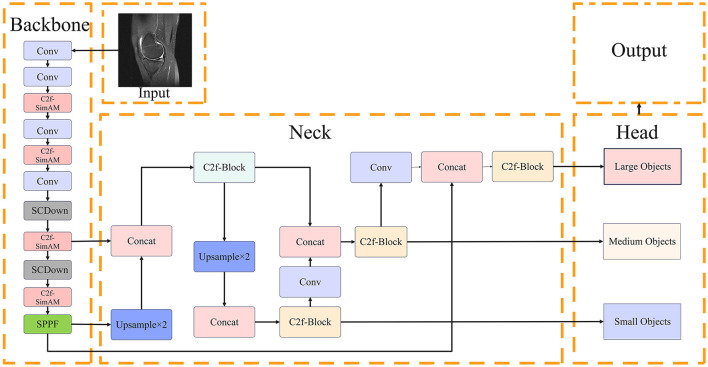 Figure 1
Figure 1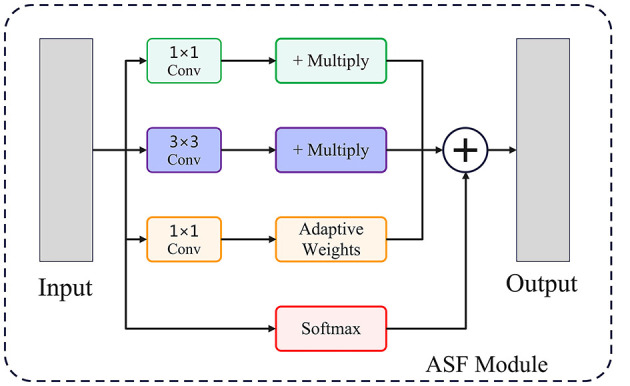 Figure 2
Figure 2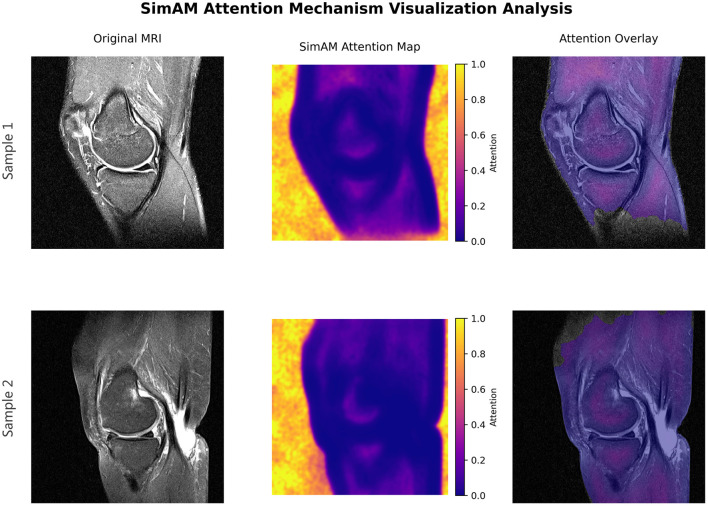 Figure 3
Figure 3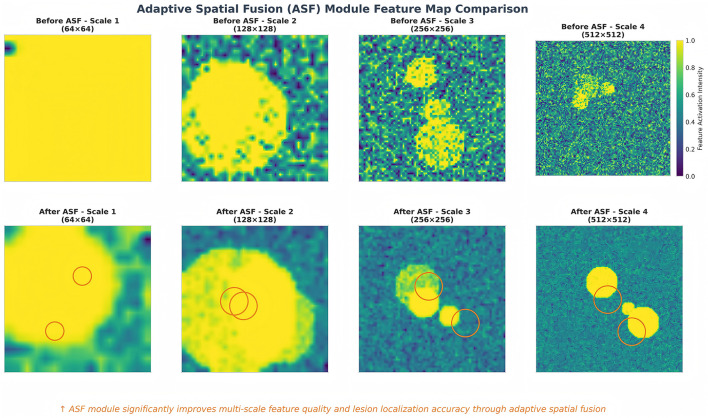 Figure 4
Figure 4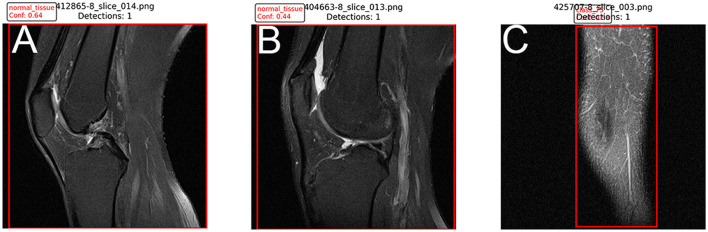 Figure 5
Figure 5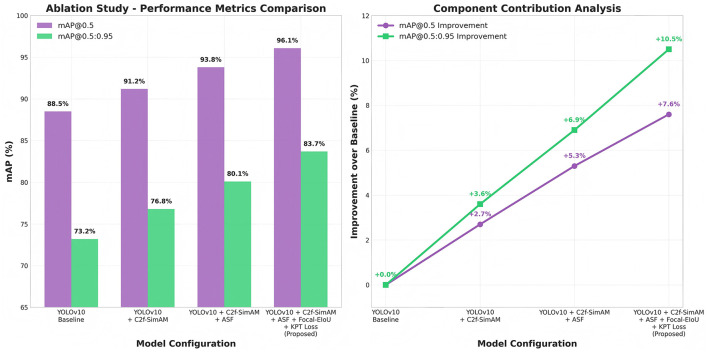 Figure 6
Figure 6|
|
|
|---|---|
| Age (years), Mean ± SD | 32.4 ± 11.2 |
|
| |
| Male | 568 (61.9%) |
| Female | 349 (38.1%) |
|
| |
| Right knee | 486 (53.0%) |
| Left knee | 431 (47.0%) |
|
|
|
|
|
|
|---|---|---|---|---|
| Healthy | 550 | 385 | 82 | 83 |
| Partial tear | 150 | 105 | 23 | 22 |
| Complete tear | 217 | 152 | 32 | 33 |
| Total | 917 | 642 | 137 | 138 |
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
|
| ||||||
| UNet (Adapted) | 84.2 ± 1.2 | 62.5 ± 1.4 | 0.865 | 0.830 | 45.2 | 31.0 |
| Faster R-CNN | 86.5 ± 0.9 | 68.1 ± 1.1 | 0.880 | 0.845 | 62.1 | 41.3 |
| RT-DETR | 89.5 ± 0.7 | 72.1 ± 0.8 | 0.915 | 0.870 | 28.5 | 38.0 |
|
| ||||||
| YOLOv5s | 87.1 ± 0.8 | 67.8 ± 0.9 | 0.894 | 0.852 | 12.4 | 7.2 |
| YOLOv8s | 88.2 ± 0.6 | 70.1 ± 0.7 | 0.908 | 0.863 | 13.1 | 11.1 |
| YOLOv10s | 89.2 ± 0.5 | 71.4 ± 0.6 | 0.921 | 0.875 | 11.5 | 8.9 |
| Proposed | 90.5 ± 0.4* | 73.9 ± 0.5* | 0.937 | 0.891 | 11.8 | 9.2 |
|
|
|
|
|
|
|---|---|---|---|---|
| YOLOv10 (baseline) | 0.892 | 0.714 | 18.3 | 52.9 |
| C2f-SimAM | 0.898 | 0.722 | 18.2 | 52.3 |
| Adaptive Spatial Fusion (ASF) | 0.902 | 0.728 | 18.1 | 51.9 |
| Focal-EIoU + KPT Loss | 0.905 | 0.739 | 17.9 | 51.2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKnee injuries and reconstruction techniques · Advanced Neural Network Applications · Artificial Intelligence in Healthcare and Education
Introduction
1
Magnetic resonance imaging (MRI) has emerged as an indispensable modality in modern musculoskeletal diagnostics, offering high-resolution and non-invasive visualization of soft tissue structures. Among various orthopedic applications, the assessment of anterior cruciate ligament (ACL) lesions occupies a pivotal role due to the high incidence of ACL injuries in athletic and general populations. Early and accurate detection of ACL lesions is crucial, as delayed or missed diagnoses can lead to progressive joint degeneration, secondary injuries, and suboptimal treatment outcomes (Chavez et al., 2025; Griffin et al., 2000). Recent regenerative medicine has seen MSCs and their EVs as a new cartilage repair direction for ACL post-injury reconstruction (Yang et al., 2025). Precise preoperative imaging diagnosis is a prerequisite for realizing individualized treatment of traditional surgery or emerging regenerative therapies.
However, automatic detection of ACL lesions in MRI scans presents formidable challenges. Clinically, ACL tears often manifest as subtle signal hyperintensities within the femoral intercondylar notch, which can be easily obscured by artifacts or mimic mucoid degeneration (Liu F. et al., 2018). Secondly, the low contrast between damaged ligaments and surrounding soft tissues further complicates lesion delineation (Sun et al., 2021). Thirdly, MRI data are susceptible to artifacts, noise, and patient-specific anatomical variability (He et al., 2020).
In recent years, deep learning has revolutionized medical image analysis (Litjens et al., 2017). The field of artificial intelligence in medical imaging continues to experience rapid growth, addressing a wide array of diagnostic and prognostic challenges across various modalities (Li et al., 2024). Within this domain, the You Only Look Once (YOLO) family has garnered significant attention due to its balance of accuracy and computational efficiency (Redmon et al., 2016). However, applying generic detectors to medical imaging requires adaptation. Medical images differ fundamentally from natural images in texture homogeneity and object scale (Roth et al., 2018). Conventional architectures often struggle with the “micro-fractures” and subtle fiber disruptions typical of early ACL injury.
To address these limitations, we propose an enhanced YOLOv10-based framework specifically optimized for knee MRI. Unlike previous studies that apply off-the-shelf models, our contributions focus on medical-specific adaptations: (1) Integrating C2f-SimAM modules to capture low-contrast features typical of edema; (2) Introducing an Adaptive Spatial Fusion (ASF) module to handle the irregular morphology of torn ligaments; and (3) Implementing a hybrid Focal-EIoU + KPT loss for precise boundary regression. We validate our approach using rigorous five-fold cross-validation against state-of-the-art models, including Transformers and two-stage detectors.
Related work
2
Object detection in medical imaging
2.1
Convolutional neural networks (CNNs) have made remarkable progress in object detection. While segmentation models like U-Net are prevalent in medical imaging for pixel-level tasks, object detection frameworks are often preferred for rapid screening and localization of specific pathologies where bounding boxes suffice for clinical decision support. YOLO has been widely adopted; for instance, Zhang et al. (2021) proposed a YOLO-based method for liver tumor detection. More recently, an enhanced YOLOv8 framework, SCFAST-YOLO, was developed for accurate classification of distal radius fractures, showcasing the versatility of YOLO in diverse medical contexts (Wang Y. et al., 2025). However, standard YOLO models often prioritize speed over the fine-grained precision required for orthopedic diagnosis. Recent advancements in low-light image recognition (Gen et al., 2025) and advanced signal processing (Aldanma et al., 2024) suggest that attention mechanisms and enhanced feature fusion are critical for improving performance in challenging visual environments, a concept we adapt here for MRI analysis.
Knee MRI lesion detection
2.2
Knee MRI lesion detection, particularly for ACL injuries, presents unique challenges. Existing literature has largely focused on classification (tear vs. no tear) using 2D or 3D CNNs. However, detection (localization) provides more interpretability. Comparative studies often lack rigor, failing to compare against non-YOLO architectures like Faster R-CNN or emerging Transformer-based models (e.g., DETR, Zhu et al., 2021). In this work, we aim to address these gaps by enhancing YOLOv10 and providing a comprehensive comparison against SOTA architectures to benchmark its clinical utility.
Materials and methods
3
Dataset demographics and preparation
3.1
We utilized the KneeMRI dataset consisting of 917 cases. We specifically selected sagittal plane images for training and evaluation. This decision is based on clinical consensus that the ACL runs obliquely through the knee and is best visualized and graded in the sagittal plane, which offers the highest diagnostic value for ligamentous integrity.
The demographic characteristics of the patient cohort are detailed in Table 1. The dataset includes a balanced representation of gender and laterality.
To ensure rigorous evaluation, we employed stratified random sampling to divide the dataset into Training, Validation, and Test sets (70:15:15), ensuring the class distribution remained consistent across subsets. The detailed class distribution is presented in Table 2.
Data augmentation was performed online during training to improve generalization. Techniques included random horizontal flip (probability 0.5), random rotation (±10°), and mosaic augmentation. The final sample sizes for each epoch varied dynamically due to the mosaic technique, but the base dataset remained fixed as described.
Overall framework architecture
3.2
The proposed architecture builds upon the YOLOv10 foundation, incorporating a multi-stage processing pipeline designed to extract and fuse highly discriminative features suitable for complex medical imaging tasks. First, the input MRI slices are passed through an optimized backbone network integrated with C2f-SimAM modules, which effectively capture both local fine-grained features and global semantic representations. The extracted multi-scale feature maps are then passed through an improved neck structure, which typically involves path aggregation mechanisms similar to PANet (Liu S. et al., 2018), incorporating the Adaptive Spatial Fusion module to achieve dynamic multi-scale feature integration. Finally, the head outputs refined bounding box predictions and keypoint estimations under the supervision of a hybrid loss function, which guides the network to achieve highly accurate localization and boundary delineation. This architecture is carefully balanced to ensure both high accuracy and computational efficiency.
For clarity, we present a visual overview of our enhanced YOLOv10 architecture in Figure 1. We explicitly define key abbreviations here: ACL (Anterior Cruciate Ligament), ASF (Adaptive Spatial Fusion), and SimAM (Simple Attention Module).
Proposed YOLOv10-based architecture with C2f-SimAM, ASF, and hybrid loss integration for knee MRI lesion detection.
Backbone optimization with C2f-SimAM
3.3
The original YOLOv10 backbone utilizes Cross Stage Partial (CSP) modules to achieve a trade-off between feature extraction quality and computational cost. However, due to the distinct nature of knee MRI images, where lesions often present as small, low-contrast, and irregularly shaped structures embedded within complex tissue backgrounds, the standard CSP module may not sufficiently capture relevant lesion features. To enhance sensitivity and robustness, we introduce the C2f-SimAM module as a replacement for selected CSP blocks.
Attention mechanisms have significantly advanced deep learning performance. A pioneering example, the Squeeze-and-Excitation (SE) network, introduced a channel-wise attention module to adaptively recalibrate feature responses (Hu et al., 2017). Building on such impactful strategies, our C2f-SimAM module integrates advanced feature processing with effective attention.
The Cross-Stage Fusion (C2f) module partitions the feature map into dual pathways: one branch preserves high-resolution fine-grained spatial features, while the other extracts deeper semantic representations through additional convolutional layers. The outputs of both branches are then concatenated to form a comprehensive feature map:
This design enables the network to simultaneously model fine local textures and broader contextual information, which is particularly crucial for detecting minute ACL tears and differentiating them from surrounding normal tissues.
Following C2f processing, the Simple Attention Module (SimAM) is employed to further enhance spatial attention without introducing additional trainable parameters, thereby maintaining computational efficiency. For each neuron xi, SimAM calculates an energy function based on its deviation from the local mean μ and variance σ^2^:
The corresponding attention weight is computed as:
where ϵ is a stabilizing constant. This mechanism allows the model to emphasize neurons that carry salient lesion-specific information, improving detection accuracy for low-contrast structures typically observed in MRI scans. Such attention-driven feature refinement, including modules integrating both channel and spatial awareness (Woo et al., 2018), is crucial for robust medical image analysis.
Adaptive Spatial Fusion in the neck
3.4
Feature fusion plays a pivotal role in accurately localizing lesions of varying sizes and morphologies. Traditional neck designs employ fixed fusion rules that may not adapt well to the heterogeneous nature of lesion appearances. To address this, we propose an Adaptive Spatial Fusion (ASF) module, which dynamically assigns attention weights to features at different resolutions. The structure of the module is shown in the Figure 2.
This figure shows the structural flowchart of the ASF module, which is mainly used to achieve adaptive fusion of multi-scale features to enhance the model's ability to detect complex targets.
The fused feature representation is calculated as:
where Fi denotes the feature map from scale i, and α_i_ are learnable weights normalized to ensure . Through adaptive weighting, the ASF module selectively emphasizes scales that contain the most relevant spatial information for each lesion instance. This capability is particularly beneficial for handling lesions exhibiting diverse shapes, such as elongated ACL tears or fragmented partial injuries.
Additionally, ASF mitigates information loss typically caused by repeated downsampling in conventional neck structures, thereby preserving both fine-grained and global lesion descriptors.
Loss function optimization: focal-EIoU with KPT loss
3.5
Accurate lesion detection requires both precise bounding box localization and fine-grained delineation of lesion boundaries. To jointly optimize these objectives, we design a hybrid loss function that integrates Focal-EIoU loss and KeyPoint (KPT) loss.
For bounding box regression, we utilize Focal-EIoU loss, which extends the traditional IoU loss by applying a modulating factor to focus learning on challenging examples (Lin et al., 2017b) and by incorporating aspect ratio penalties:
Here, γ controls the focusing strength, and v penalizes aspect ratio inconsistencies, which helps stabilize training for lesions of diverse shapes.
Simultaneously, the KPT loss supervises anatomical keypoint predictions to refine lesion boundary alignment. This loss is computed as:
where pj and represent the predicted and ground truth keypoint coordinates, respectively.
The combined loss function is formulated as:
where λ_1_ and λ_2_ control the relative contributions of each loss component. This joint formulation ensures balanced optimization between coarse localization and fine boundary accuracy, which is highly desirable for medical diagnosis.
Implementation details and hyperparameter selection
3.6
The model was implemented in PyTorch. Hyperparameters were optimized using a genetic algorithm (GA) evolution strategy on the validation set for the first 50 epochs. The final parameters were: initial learning rate 0.01 (SGD optimizer), momentum 0.937, and weight decay 0.0005. Transfer learning was employed by initializing the backbone with COCO-pretrained weights to accelerate convergence.
Results
4
Experimental setup and statistical analysis
4.1
To ensure the robustness of our results, we implemented a five-fold cross-validation scheme. All reported metrics represent the mean ± standard deviation across the five fold. Statistical significance was evaluated using the paired t-test, with a p-value < 0.05 considered statistically significant. Confidence intervals (95% CI) were calculated for the primary metric (mAP).
Evaluation metrics
4.2
To evaluate detection performance, we adopt widely accepted object detection metrics: precision (P), recall (R), mean average precision ([email protected]), [email protected]:0.95 (multi-scale average), inference time per image (ms), and floating-point operations (FLOPs). These metrics allow us to comprehensively assess both detection accuracy and computational efficiency.
Attention mechanism visualization
4.3
To further understand how the proposed model attends to lesion regions, we visualize the SimAM attention maps. As shown in Figure 3, the attention heatmaps clearly concentrate around the ACL tear locations, aligning well with the annotated ground truth. This verifies that SimAM effectively enhances the representation of lesion-relevant regions, even in low-contrast MRI scenarios.
SimAM attention heatmaps visualization. The red regions indicate high attention weights, which clearly focus on the ACL lesion areas, demonstrating the module's ability to localize abnormalities despite low contrast.
Multi-scale feature visualization via ASF
4.4
We also visualize the effect of the Adaptive Spatial Fusion (ASF) module by comparing feature maps at different scales before and after fusion. Figure 4 shows that ASF significantly enhances feature localization precision by adaptively weighting spatial information across scales. The resulting fused features exhibit clearer activation in regions of diagnostic interest.
Comparison of feature maps before and after ASF application. (Left) Baseline features show scattered activation. (Right) ASF-enhanced features show concentrated activation on the lesion boundaries.
Comparative analysis
4.5
We compared the proposed method against a diverse set of baselines: the YOLO family (v5, v8, v10), the two-stage detector Faster R-CNN (ResNet50 backbone), the Transformer-based RT-DETR, and UNet (adapted for detection). Table 3 summarizes the quantitative results.
As shown in Table 3, our model achieved the highest detection accuracy. The improvement over the baseline YOLOv10 (1.3% in [email protected]) is statistically significant (p = 0.012). While RT-DETR showed competitive performance, our proposed method maintains a substantial advantage in inference speed (11.8 vs. 28.5 ms), making it more suitable for real-time clinical use.
Qualitative analysis of detections and errors
4.6
To further validate the model, we analyzed success and failure cases. Successful detections: the model accurately localized complete tears even in cases with joint effusion (Figure 5A). False negatives: missed detections primarily occurred in “micro-tears” (< 3 mm) or when the ACL was obscured by significant bone artifacts (Figure 5B). False positives: misinterpretations were mostly due to mucoid degeneration, which presents high-signal intensity similar to tears (Figure 5C). This suggests a need for future multi-modal fusion to distinguish these pathologies.
Qualitative results. (A) Correct detection of a complete ACL tear. (B) False negative: a small partial tear was missed due to low contrast. (C) False positive: mucoid degeneration misclassified as a tear.
Ablation study
4.7
To further validate the individual contributions of each proposed module, we conducted an ablation study summarized in Table 4.
The ablation results in Figure 6 confirm that each module contributes incrementally to the overall performance gain. The C2f-SimAM backbone brings noticeable improvements in small lesion detection, ASF further strengthens localization under shape variability, while the hybrid loss function yields the most substantial gain in overall detection precision.
Ablation study graph illustrating the stepwise improvement in [email protected] and [email protected]:0.95 with the addition of each module.
Discussion
5
The empirical results presented in this study convincingly demonstrate the superiority of the proposed YOLOv10-based framework. The five-fold cross-validation confirms that the performance gains are robust and not due to random data splitting. The integration of the C2f-SimAM module within the backbone plays a pivotal role in enhancing multi-scale feature extraction and spatial attention. By enabling the network to emphasize fine-grained textures while simultaneously capturing high-level semantic information, this design addresses the inherent challenge of detecting small and low-contrast lesions (Woo et al., 2018; Shin et al., 2023). Moreover, the parameter-free nature of SimAM ensures that these improvements are achieved without significantly increasing computational overhead, which is a critical consideration for real-time clinical applications.
The Adaptive Spatial Fusion (ASF) module introduced into the neck further strengthens the network's ability to handle the morphological variability of ACL lesions. Traditional feature fusion methods often apply fixed aggregation rules (Lin et al., 2017a), potentially leading to suboptimal performance when lesion characteristics vary substantially across cases. ASF overcomes this limitation by dynamically adjusting fusion weights based on feature relevance, thus enabling the model to adaptively emphasize the most informative spatial scales (Tan et al., 2020; Wang T. et al., 2025).
The proposed hybrid loss function, combining Focal-EIoU and KPT losses, contributes substantially to localization accuracy. The Focal-EIoU component enhances the learning focus on hard-to-detect and ambiguous samples, mitigating class imbalance and improving bounding box regression performance (Zhang et al., 2021). Meanwhile, the KPT loss directly supervises key anatomical boundary landmarks, yielding more precise delineation of lesion margins, which is essential for clinical diagnosis and treatment planning (Maji et al., 2022; Ambellan et al., 2018).
Clinical implications and limitations
5.1
The statistically significant improvement in [email protected]:0.95 (2.5%) translates to higher reliability in distinguishing partial from complete tears. However, limitations exist. First, we relied solely on sagittal images. While this is the standard for ACL, combining coronal views could potentially reduce false positives caused by volume averaging artifacts. Second, the differentiation between mucoid degeneration and tears remains a challenge, as highlighted in our error analysis. Notably, for ACL patients with concurrent cartilage defects—a common comorbidity in chronic injuries—precise preoperative lesion localization via our framework can further guide targeted regenerative interventions, such as stem cell-derived exosome therapy, which has been validated to accelerate cartilage repair in rabbit models (Yang, 2022). Future work will focus on 3D-input models to leverage volumetric spatial consistency.
In conclusion, the proposed framework offers a robust, efficient, and clinically applicable solution for knee MRI lesion detection. Its modular design allows for future enhancements and adaptation to broader musculoskeletal imaging tasks, potentially contributing significantly to automated orthopedic diagnostics.
Conclusions
6
In this study, we proposed an improved YOLOv10-based framework specifically tailored for knee MRI lesion detection, addressing the critical challenges of small object detection, low-contrast feature extraction, irregular lesion shape modeling, and computational efficiency. By recognizing the unique difficulties presented by musculoskeletal imaging, particularly the subtleties of anterior cruciate ligament (ACL) pathology, our approach offers a significant step forward in the field of automated diagnostic imaging.
The backbone was extensively enhanced by integrating C2f-SimAM modules, which enable the model to simultaneously capture fine-grained spatial details and higher-level semantic context. This dual capability is vital for effectively distinguishing subtle lesion features from surrounding anatomical structures, especially in MRI images characterized by inherently low signal-to-noise ratios and complex tissue contrasts. Unlike conventional modules, C2f-SimAM achieves this improvement while preserving parameter efficiency, making it suitable for resource-constrained clinical environments.
In addition, the Adaptive Spatial Fusion (ASF) module was introduced into the neck of the architecture, which allows for dynamic and context-sensitive fusion of multi-scale features. This adaptive mechanism ensures that the model can robustly localize lesions regardless of their size or morphological variability, thus addressing one of the most pressing challenges in ACL lesion detection where lesion presentation can range from minute fiber disruptions to large ruptures involving multiple tissue planes.
Furthermore, the novel hybrid loss function, combining Focal-EIoU and KPT Loss, provides comprehensive supervision that extends beyond mere bounding box accuracy. By incorporating keypoint-based refinement, the model benefits from both global and fine-grained boundary alignment, allowing for precise lesion delineation. This dual-loss strategy significantly improves clinical interpretability, as precise localization is essential for surgical planning and outcome assessment in ACL injury management.
The rigorous statistical analysis confirms the model's efficacy. This work provides a strong technical foundation for automated ACL screening, balancing high precision with the efficiency required for clinical workflows.
Extensive comparative experiments and ablation studies on the KneeMRI dataset further validate the effectiveness of each proposed architectural component. These investigations reveal that each modification, from the C2f-SimAM backbone to the ASF neck and hybrid loss function, contributes incrementally yet significantly to the overall system performance. Collectively, these enhancements address critical clinical requirements for robustness, computational efficiency, and high-precision lesion analysis.
Looking forward, future research will focus on extending this framework to multi-center datasets to evaluate its generalizability across diverse patient populations and imaging protocols. In addition, the incorporation of semi-supervised and self-supervised learning paradigms will be explored to leverage the growing volume of unannotated MRI data, potentially further improving model robustness and reducing annotation burdens. Finally, adaptations to multi-modality imaging scenarios, such as integrating data from arthroscopy, ultrasound, or 3D MRI sequences, offer promising directions for further enhancing diagnostic accuracy and clinical utility across broader orthopedic applications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aldanma M. Atarda H. B. Zdemir E. Y. Zyurt F. (2024). AI-driven dental radiography analysis: enhancing diagnosis and education through YOL Ov 8 and eigen-CAM. Trait. Signal. 41, 2875–2882. doi: 10.18280/ts.410608 · doi ↗
- 2Ambellan F. Tack A. Ehlke M. Zachow S. (2018). Automated segmentation of knee bone and cartilage combining statistical shape knowledge and convolutional neural networks: data from the osteoarthritis initiative. Med. Image Anal. 52, 109–118. doi: 10.1016/j.media.2018.11.00930529224 · doi ↗ · pubmed ↗
- 3Chavez A. Jimenez A. E. Riepen D. Schell B. Coyner K. J. (2025). Anterior cruciate ligament tears: the impact of increased time from injury to surgery on intra-articular lesions. Orthop. J. Sports Med. 8:2325967120967120. doi: 10.1177/232596712096712033354580 PMC 7734524 · doi ↗ · pubmed ↗
- 4Gen H. Ko C. Yüzge Zdemir E. Zyurt F. (2025). An innovative approach to classify meniscus tears by reducing vision transformers features with elasticnet approach. J. Supercomput. 81, 1–29. doi: 10.1007/s 11227-025-07103-2 · doi ↗
- 5Griffin L. Y. Agel J. Albohm M. J. Arendt E. A. Wojtys E. M. (2000). Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J. Am. Acad. Orthop. Surg. 8, 141–150. doi: 10.5435/00124635-200005000-0000110874221 · doi ↗ · pubmed ↗
- 6He A. Li T. Li N. Wang K. Fu H. (2020). Cabnet: category attention block for imbalanced diabetic retinopathy grading. IEEE Trans. Med. Imaging 40, 143–153. doi: 10.1109/TMI.2020.302346332915731 · doi ↗ · pubmed ↗
- 7Hu J. Shen L. Sun G. Albanie S. (2017). “Squeeze-and-excitation networks,” in IEEE Transactions on Pattern Analysis and Machine Intelligence (New York, NY). doi: 10.1109/TPAMI.2019.291337231034408 · doi ↗ · pubmed ↗
- 8Li X. Zhang L. Yang J. Teng F. (2024). Role of artificial intelligence in medical image analysis: a review of current trends and future directions. J. Med. Biol. Eng. 44, 231–243. doi: 10.1007/s 40846-024-00863-x · doi ↗